
Are People with Obesity Attracted to Multidisciplinary Telemedicine Approach for Weight Management?

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Disease Management during Pandemic
3.2. Obesity Management and Telemedicine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A Novel Coronavirus Outbreak of Global Health Concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef]
- Gatto, M.; Bertuzzo, E.; Mari, L.; Miccoli, S.; Carraro, L.; Casagrandi, R.; Rinaldo, A. Spread and Dynamics of the COVID-19 Epidemic in Italy: Effects of Emergency Containment Measures. Proc. Natl. Acad. Sci. USA 2020, 117, 10484–10491. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of Home Confinement on Mental Health and Lifestyle Behaviours during the COVID-19 Outbreak: Insight from the ECLB-COVID19 Multicenter Study. Biol. Sport 2021, 38, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Zupo, R.; Castellana, F.; Sardone, R.; Sila, A.; Giagulli, V.A.; Triggiani, V.; Cincione, R.I.; Giannelli, G.; De Pergola, G. Preliminary Trajectories in Dietary Behaviors during the COVID-19 Pandemic: A Public Health Call to Action to Face Obesity. Int. J. Environ. Res. Public Health 2020, 17, 7073. [Google Scholar] [CrossRef]
- Branley-Bell, D.; Talbot, C.V. Exploring the Impact of the COVID-19 Pandemic and UK Lockdown on Individuals with Experience of Eating Disorders. J. Eat. Disord. 2020, 8, 44. [Google Scholar] [CrossRef]
- Giel, K.E.; Schurr, M.; Zipfel, S.; Junne, F.; Schag, K. Eating Behaviour and Symptom Trajectories in Patients with a History of Binge Eating Disorder during COVID-19 Pandemic. Eur. Eat. Disord. Rev. 2021, 29, 657–662. [Google Scholar] [CrossRef]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and Physical Activity during the Coronavirus Disease 2019 (COVID-19) Lockdown (March–May 2020): Results from the French NutriNet-Santé Cohort Study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Sanchis-Gomar, F.; Lavie, C.J.; Mehra, M.R.; Henry, B.M.; Lippi, G. Obesity and Outcomes in COVID-19: When an Epidemic and Pandemic Collide. Mayo Clin. Proc. 2020, 95, 1445–1453. [Google Scholar] [CrossRef]
- Wijesooriya, N.R.; Mishra, V.; Brand, P.L.P.; Rubin, B.K. COVID-19 and Telehealth, Education, and Research Adaptations. Paediatr. Respir. Rev. 2020, 35, 38–42. [Google Scholar] [CrossRef]
- Johnson, K.E.; Alencar, M.K.; Coakley, K.E.; Swift, D.L.; Cole, N.H.; Mermier, C.M.; Kravitz, L.; Amorim, F.T.; Gibson, A.L. Telemedicine-Based Health Coaching Is Effective for Inducing Weight Loss and Improving Metabolic Markers. Telemed. E-Health 2019, 25, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Alencar, M.K.; Johnson, K.; Mullur, R.; Gray, V.; Gutierrez, E.; Korosteleva, O. The Efficacy of a Telemedicine-Based Weight Loss Program with Video Conference Health Coaching Support. J. Telemed. Telecare 2019, 25, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Rapporto Osservasalute. 2020. Available online: https://www.Osservatoriosullasalute.It/Osservasalute/Rapporto-Osservasalute-2020 (accessed on 21 November 2021).
- Gilardini, L.; Cancello, R.; Caffetto, K.; Cottafava, R.; Gironi, I.; Invitti, C. Nutrition Knowledge Is Associated with Greater Weight Loss in Obese Patients Following a Multidisciplinary Rehabilitation Program. Minerva Endocrinol. 2021, 46, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Epicentro, ISS. PASSI e PASSI d’argento e La Pandemia COVID-19. Primo Report Nazionale Del Modulo COVID. Available online: https://www.Epicentro.Iss.It/Coronavirus/Sars-Cov-2-Flussi-Dati-Confronto-Passi-Pda (accessed on 19 February 2022).
- Bonora, B.M.; Morieri, M.L.; Avogaro, A.; Fadini, G.P. The Toll of Lockdown Against COVID-19 on Diabetes Outpatient Care: Analysis from an Outbreak Area in Northeast Italy. Diabetes Care 2021, 44, e18–e21. [Google Scholar] [CrossRef]
- Wosik, J.; Clowse, M.E.B.; Overton, R.; Adagarla, B.; Economou-Zavlanos, N.; Cavalier, J.; Henao, R.; Piccini, J.P.; Thomas, L.; Pencina, M.J.; et al. Impact of the COVID-19 Pandemic on Patterns of Outpatient Cardiovascular Care. Am. Heart J. 2021, 231, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Albury, C.; Strain, W.D.; Brocq, S.L.; Logue, J.; Lloyd, C.; Tahrani, A. The Importance of Language in Engagement between Health-Care Professionals and People Living with Obesity: A Joint Consensus Statement. Lancet Diabetes Endocrinol. 2020, 8, 447–455. [Google Scholar] [CrossRef]
- Pagoto, S.L.; Schneider, K.L.; Oleski, J.L.; Luciani, J.M.; Bodenlos, J.S.; Whited, M.C. Male Inclusion in Randomized Controlled Trials of Lifestyle Weight Loss Interventions. Obesity 2012, 20, 1234–1239. [Google Scholar] [CrossRef]
- Robertson, C.; Archibald, D.; Avenell, A.; Douglas, F.; Hoddinott, P.; van Teijlingen, E.; Boyers, D.; Stewart, F.; Boachie, C.; Fioratou, E.; et al. Systematic Reviews of and Integrated Report on the Quantitative, Qualitative and Economic Evidence Base for the Management of Obesity in Men. Health Technol. Assess. 2014, 18, 1–424. [Google Scholar] [CrossRef]
- Men’s Experiences and Perspectives Regarding Social Support after Weight Loss Surgery. J. Mens Health 2016, 12, 25. [CrossRef]
- Ventura Marra, M.; Lilly, C.; Nelson, K.; Woofter, D.; Malone, J. A Pilot Randomized Controlled Trial of a Telenutrition Weight Loss Intervention in Middle-Aged and Older Men with Multiple Risk Factors for Cardiovascular Disease. Nutrients 2019, 11, 229. [Google Scholar] [CrossRef]
- Drew, R.J.; Morgan, P.J.; Kay-Lambkin, F.; Collins, C.E.; Callister, R.; Kelly, B.J.; Hansen, V.; Young, M.D. Men’s Perceptions of a Gender-Tailored EHealth Program Targeting Physical and Mental Health: Qualitative Findings from the SHED-IT Recharge Trial. Int. J. Environ. Res. Public. Health 2021, 18, 12878. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Pletcher, S.N.; Stahl, J.E. Telemedicine and Primary Care Obesity Management in Rural Areas—Innovative Approach for Older Adults? BMC Geriatr. 2017, 17, 6. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | |
|---|---|
| Age, years | 50.2 ± 11.6 |
| Female, % | 90 |
| Educational level | |
| Primary school, % | 5.4 |
| Secondary school, % | 57 |
| University, % | 37.5 |
| BMI, kg/m2 | 38.0 ± 6.1 |
| Class of BMI | |
| Class I (BMI 30–34.9)% | 36.3 |
| Class II (BMI 35–39.9)% | 29.8 |
| Class III (BMI ≥ 40)% | 32.3 |
| Subjects with obesity related chronic diseases, % | 54.1 |
| Subjects who practise physical activity, % | 59 |
| Subjects with at least one diet attempt, % | 96 |
| Subjects with at least one electronic tool, % | 99 |
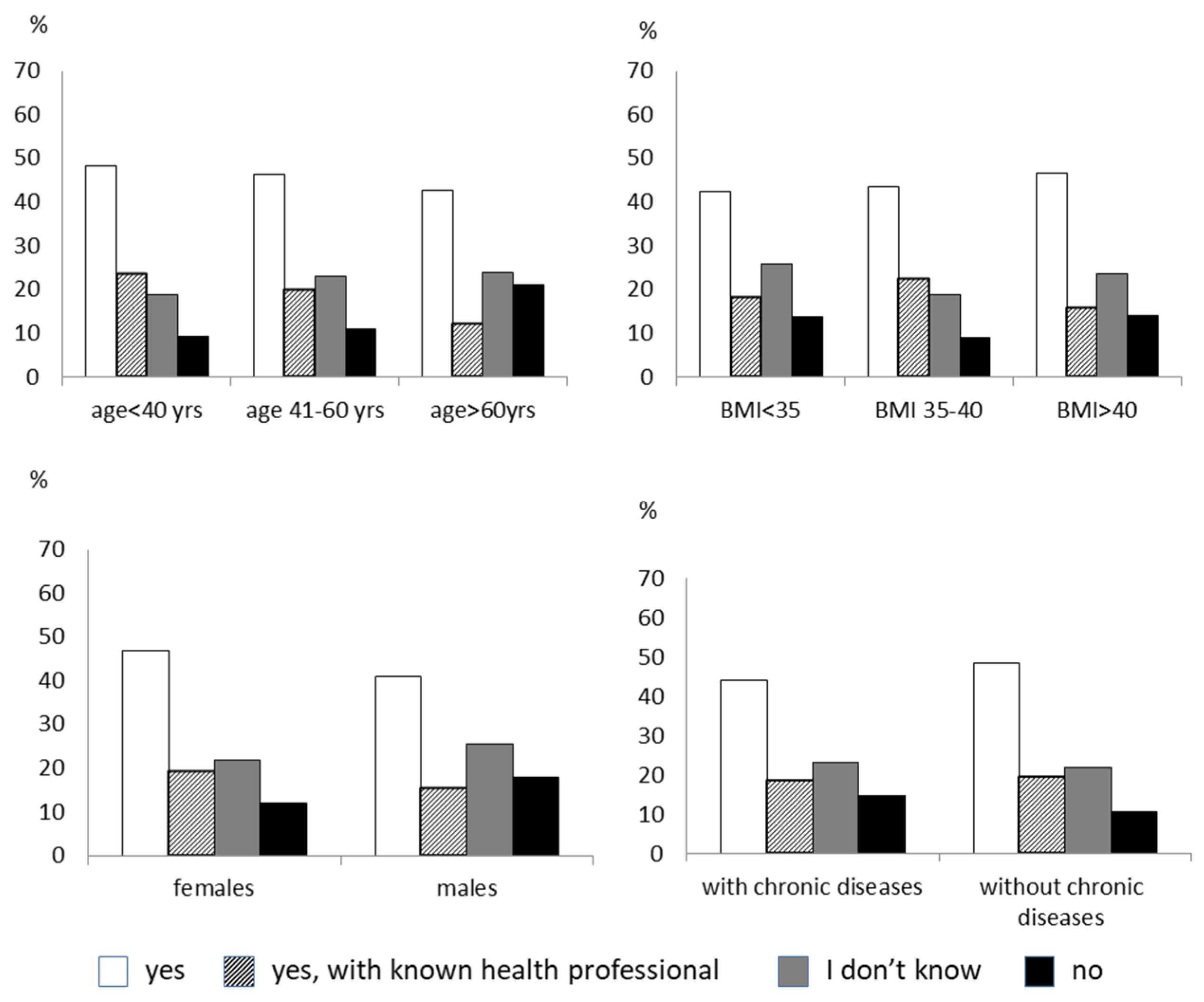
| Have you cancelled or postponed any scheduled clinical assessments during the pandemic? |
| No, 53.7% |
| Yes, 46.3% |
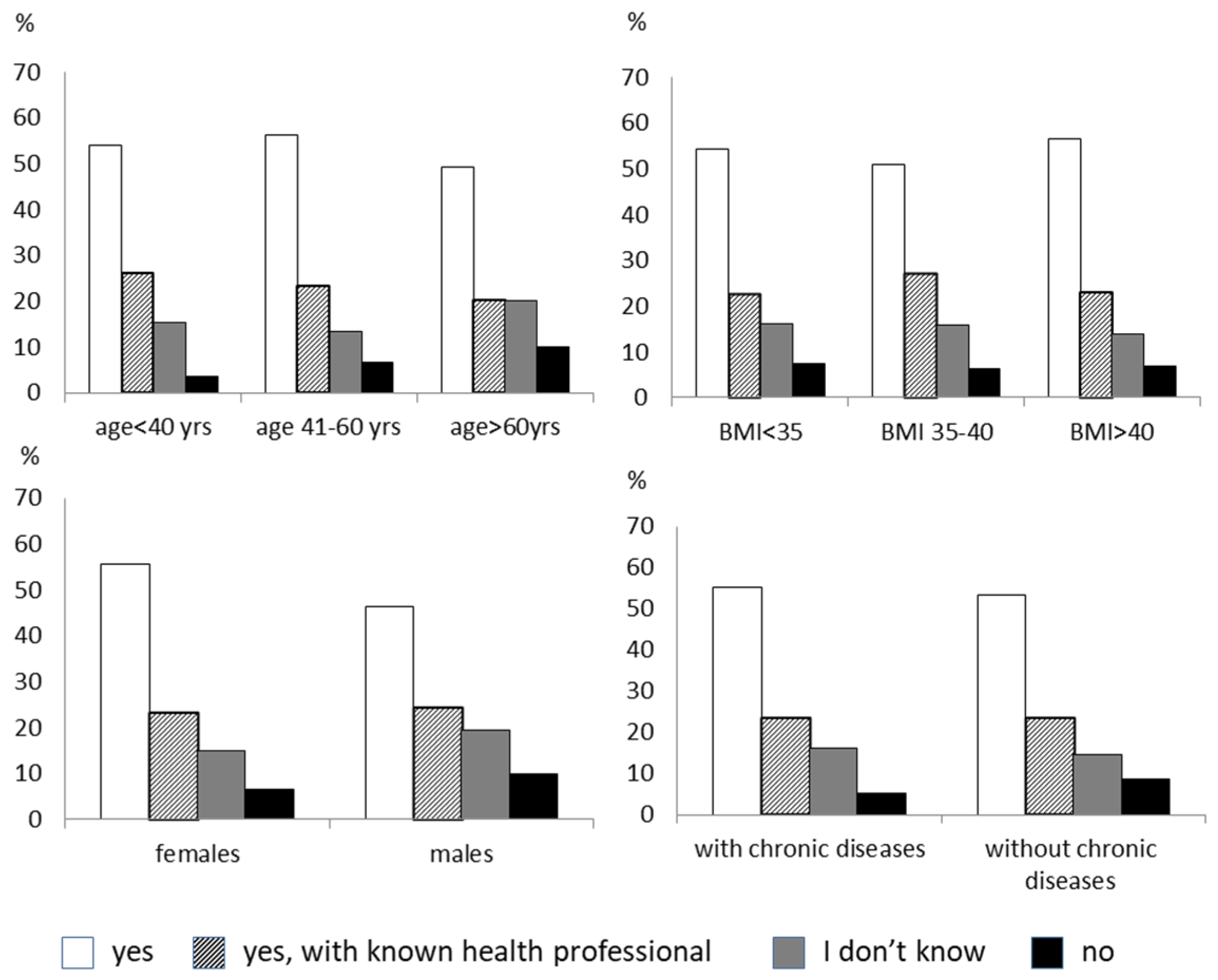
| Due to the impossibility of a visit during this period, have you contacted your doctor for the management of your complications in any other way? |
| No, never, 47.9% |
| Yes, by WhatsApp or phone message, 12.7% |
| Yes, by email, 17.1% |
| Yes, by telephone, 20.7% |
| Yes, by video consulting, 1.6% |
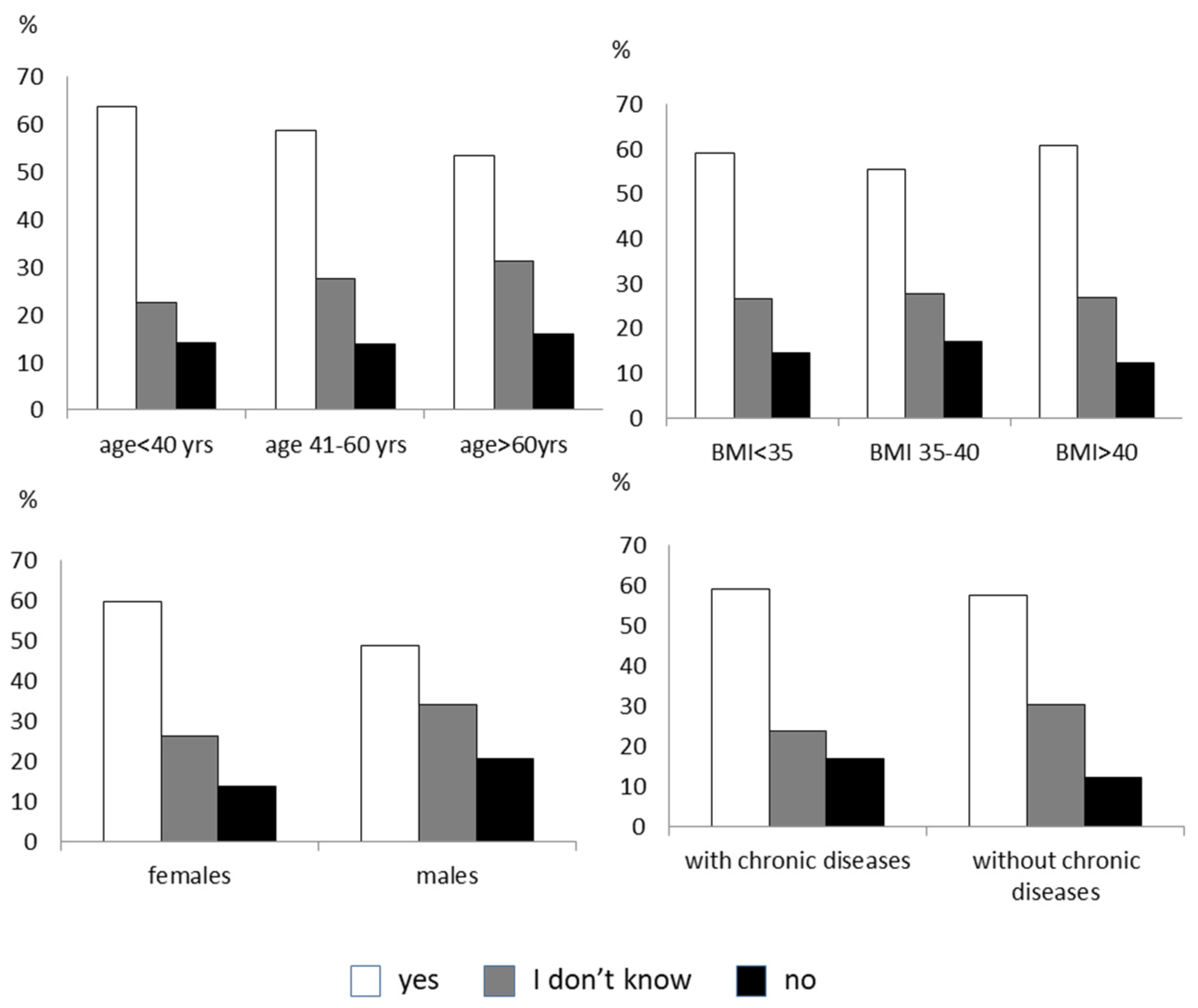
| Do you think that, during this period, a remote medical video consultation could help you have less health risks? |
| No, 12.8% |
| Yes, 59.0% |
| I don’t know, 28.1% |
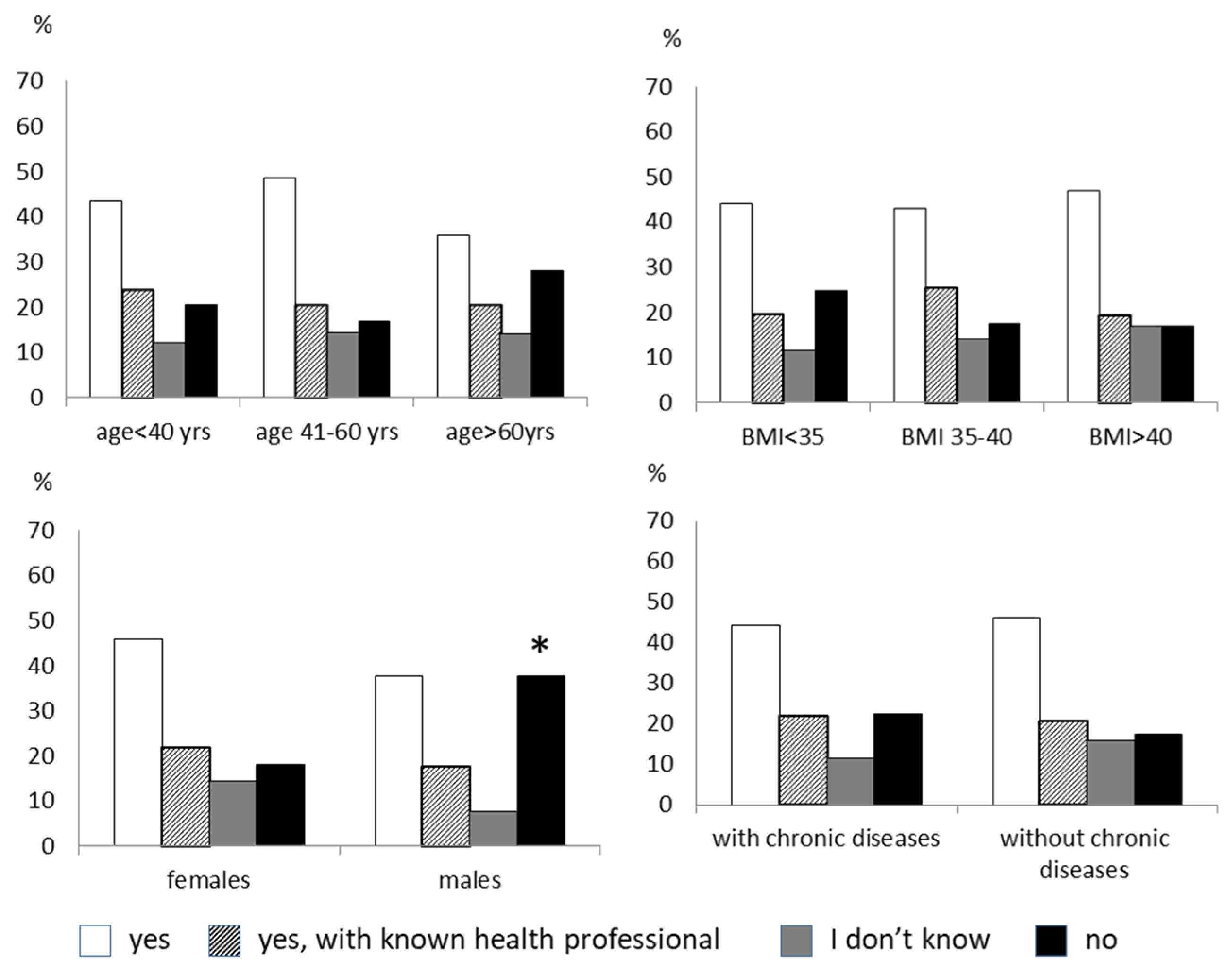
| Do you think your doctor can understand your health through a video consultation? |
| No, 12.8% |
| I don’t know, 24.5% |
| Yes, 24.4% |
| Yes, but only if he has already met me during a face-to-face visit, 37.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilardini, L.; Cancello, R.; Cavaggioni, L.; Bruno, A.; Novelli, M.; Mambrini, S.P.; Castelnuovo, G.; Bertoli, S. Are People with Obesity Attracted to Multidisciplinary Telemedicine Approach for Weight Management? Nutrients 2022, 14, 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14081579
Gilardini L, Cancello R, Cavaggioni L, Bruno A, Novelli M, Mambrini SP, Castelnuovo G, Bertoli S. Are People with Obesity Attracted to Multidisciplinary Telemedicine Approach for Weight Management? Nutrients. 2022; 14(8):1579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14081579
Chicago/Turabian StyleGilardini, Luisa, Raffaella Cancello, Luca Cavaggioni, Amalia Bruno, Margherita Novelli, Sara P. Mambrini, Gianluca Castelnuovo, and Simona Bertoli. 2022. "Are People with Obesity Attracted to Multidisciplinary Telemedicine Approach for Weight Management?" Nutrients 14, no. 8: 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14081579