
Applying Machine Learning to Determine 25(OH)D Threshold Levels Using Data from the AMATERASU Vitamin D Supplementation Trial in Patients with Digestive Tract Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
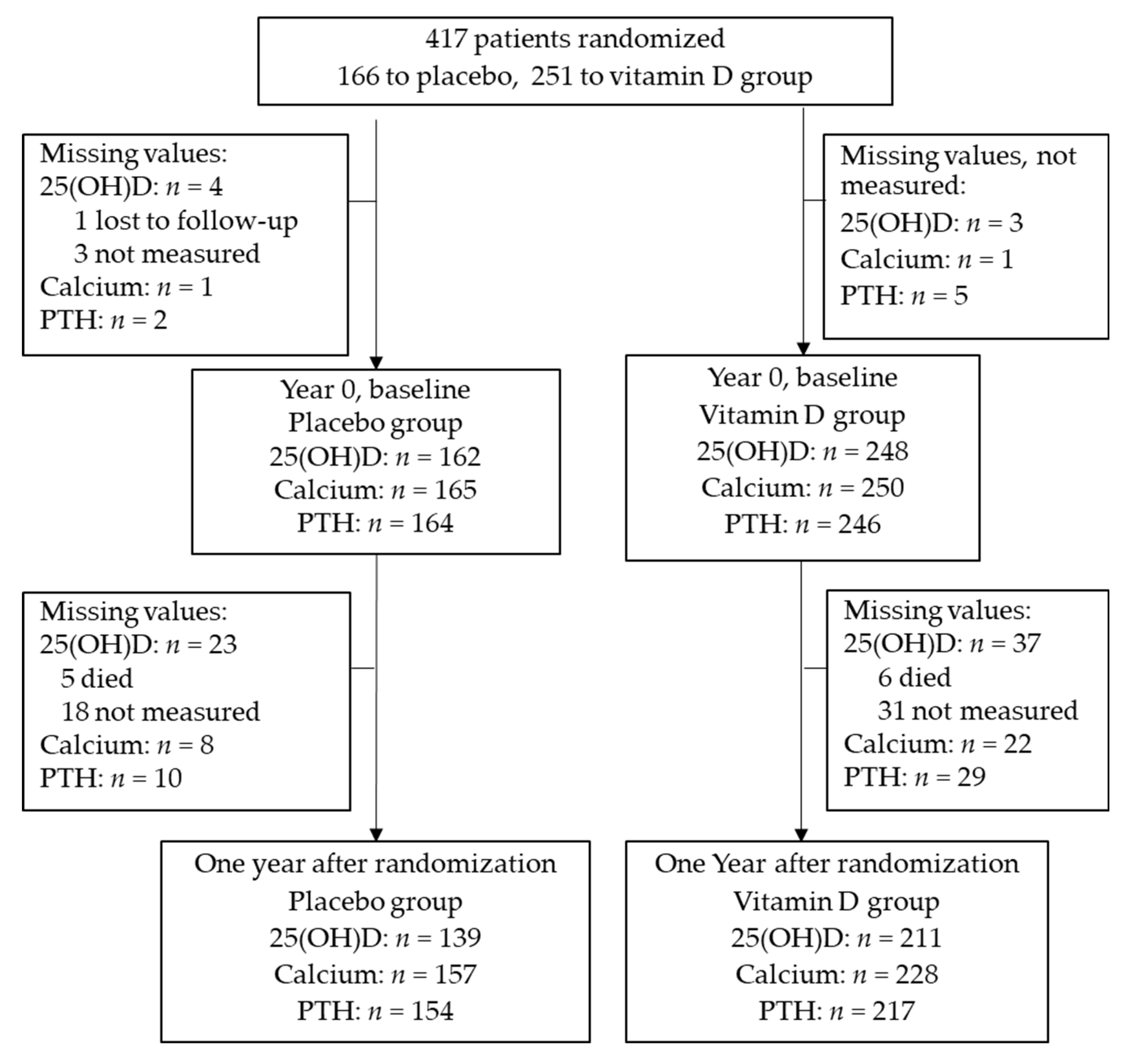
2.1. Trial Design and Participants
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
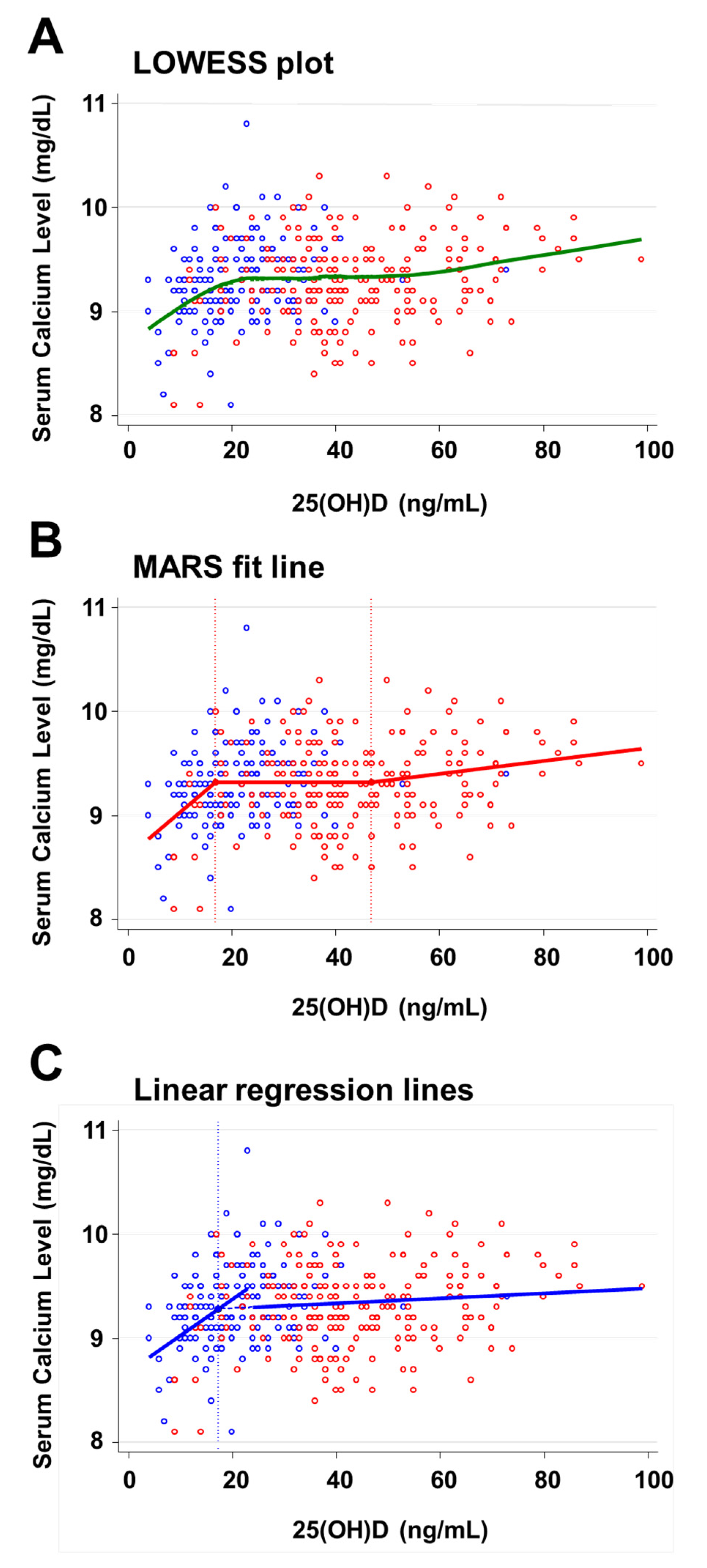
3.2. Threshold of Serum 25(OH)D Levels Relative to Calcium
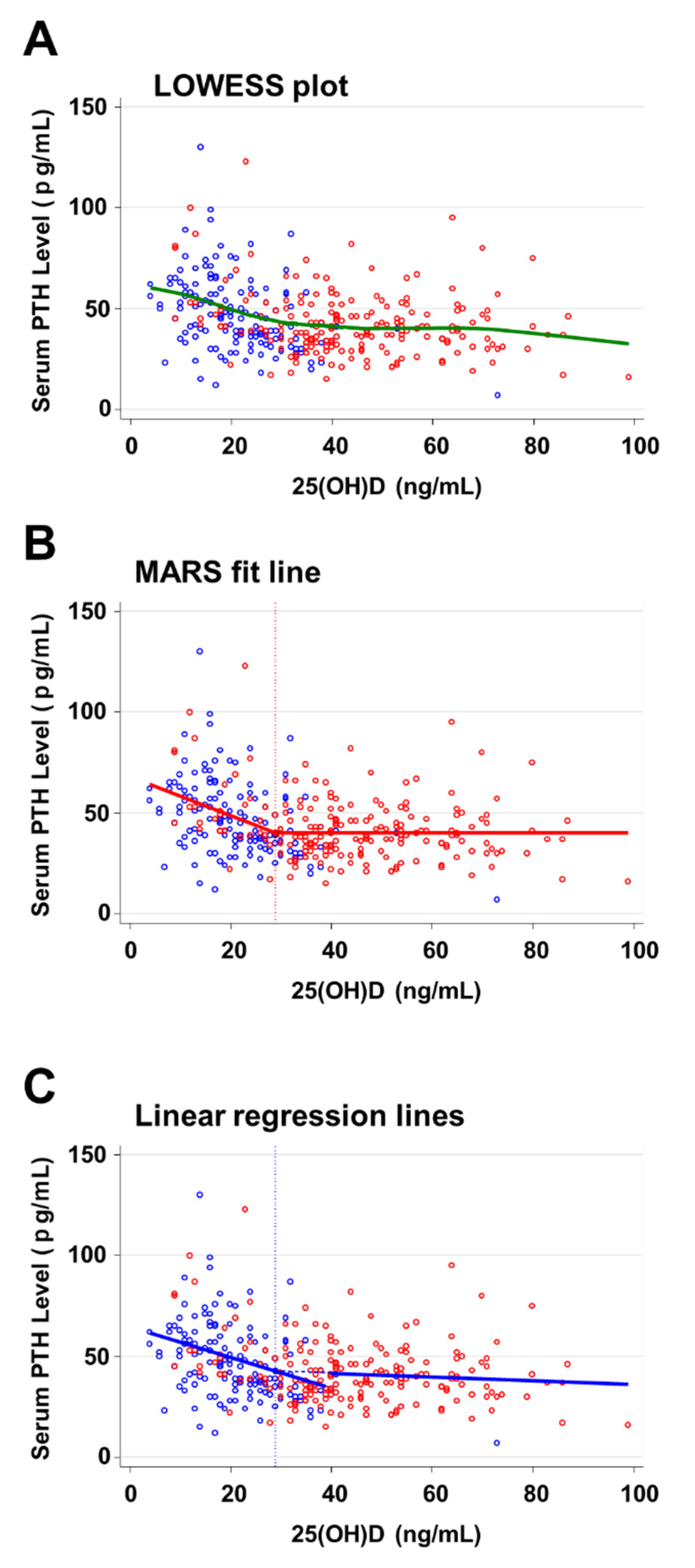
3.3. Threshold of 25(OH)D Relative to PTH
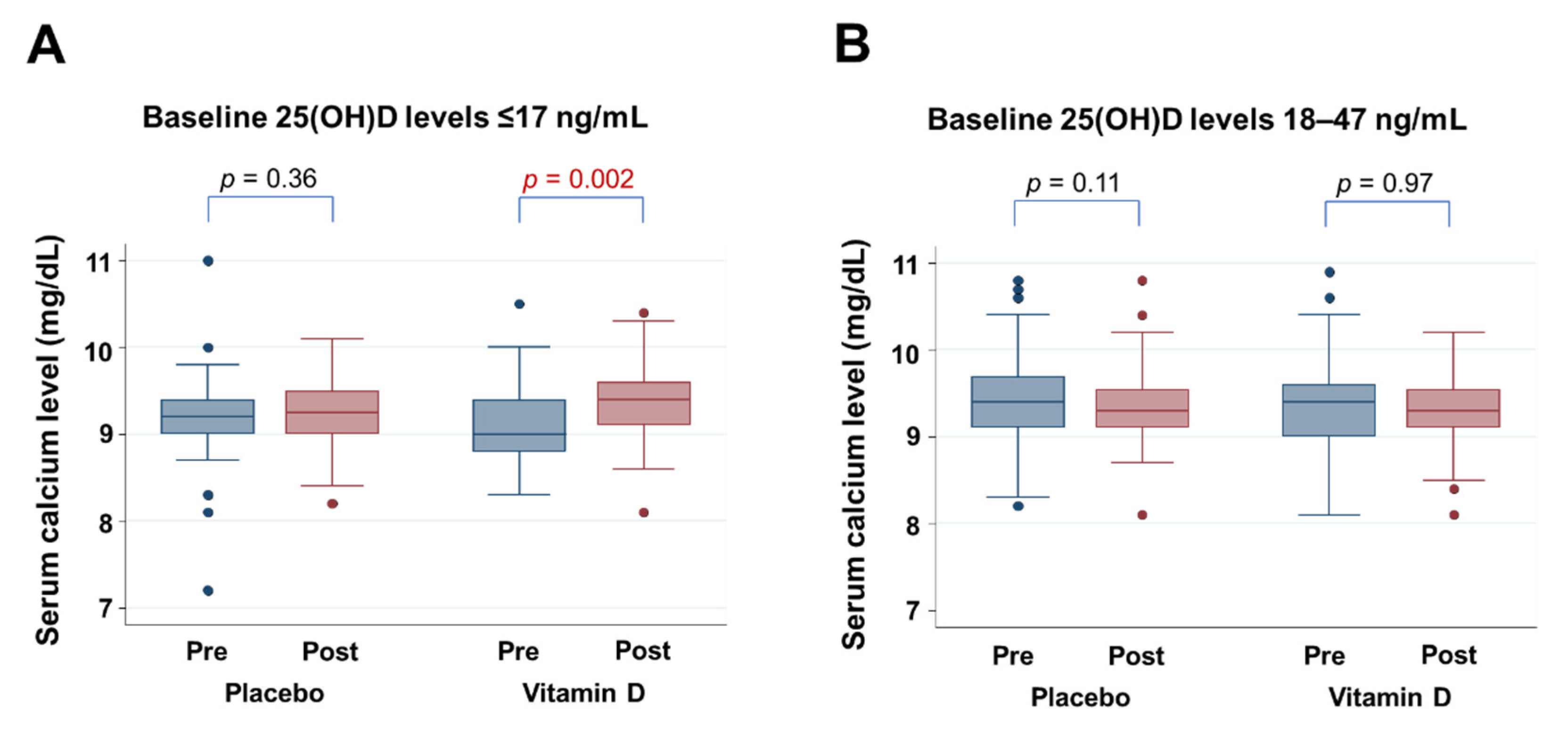
3.4. Effect of Vitamin D Supplementation on Calcium Levels
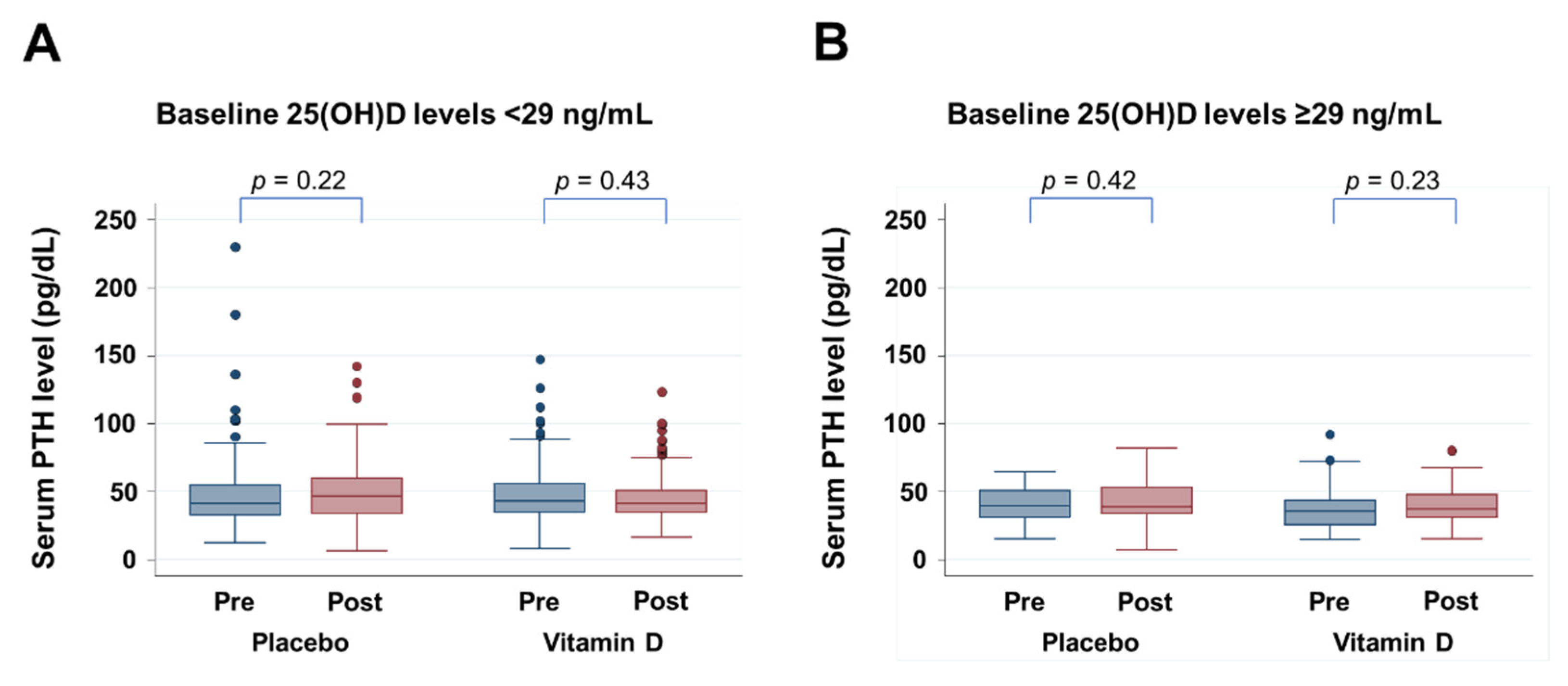
3.5. Effect of Vitamin D Supplementation on PTH Levels
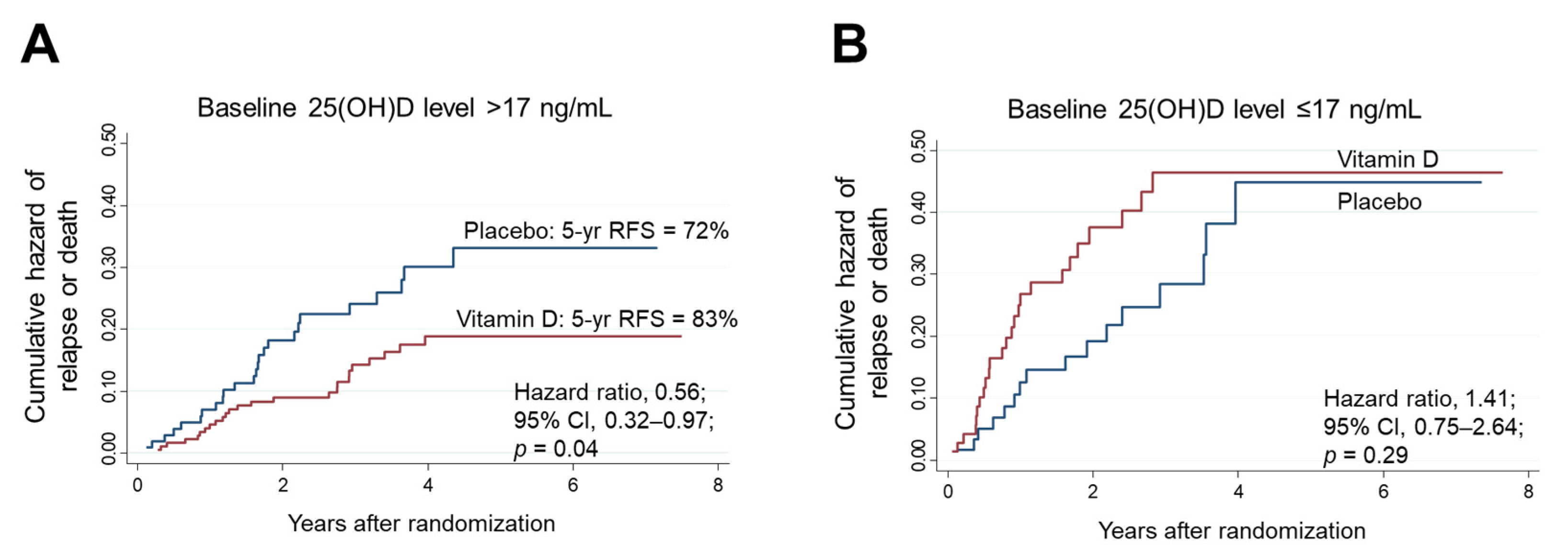
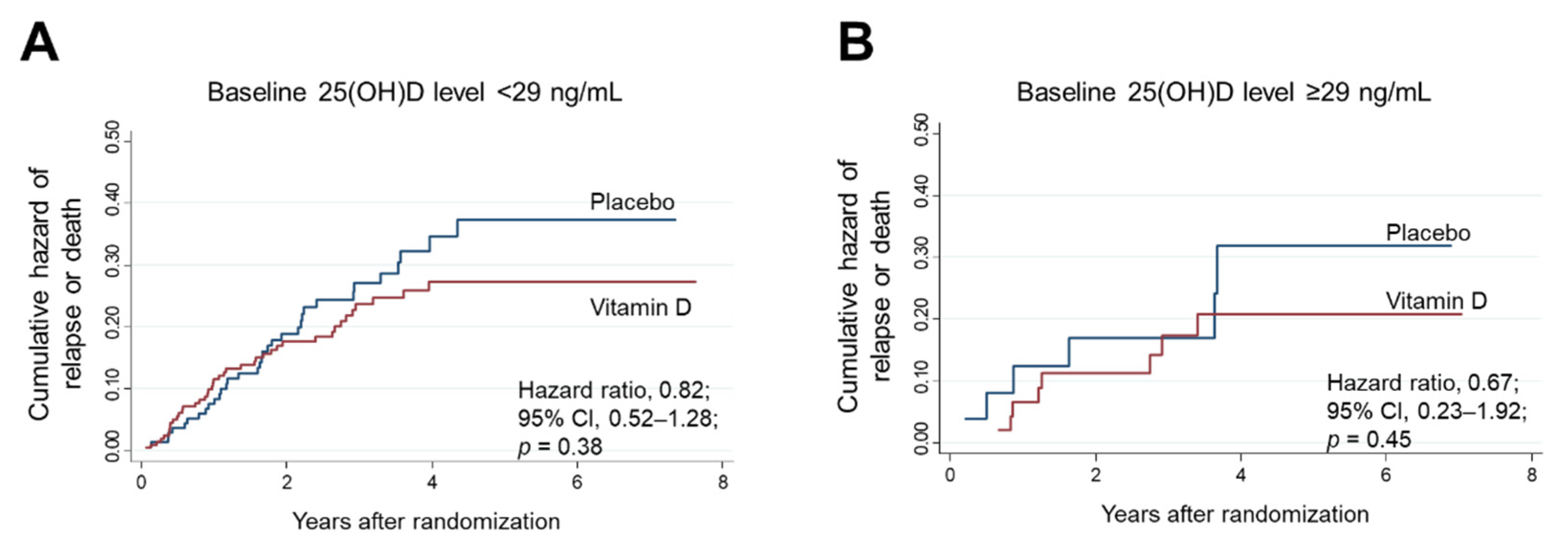
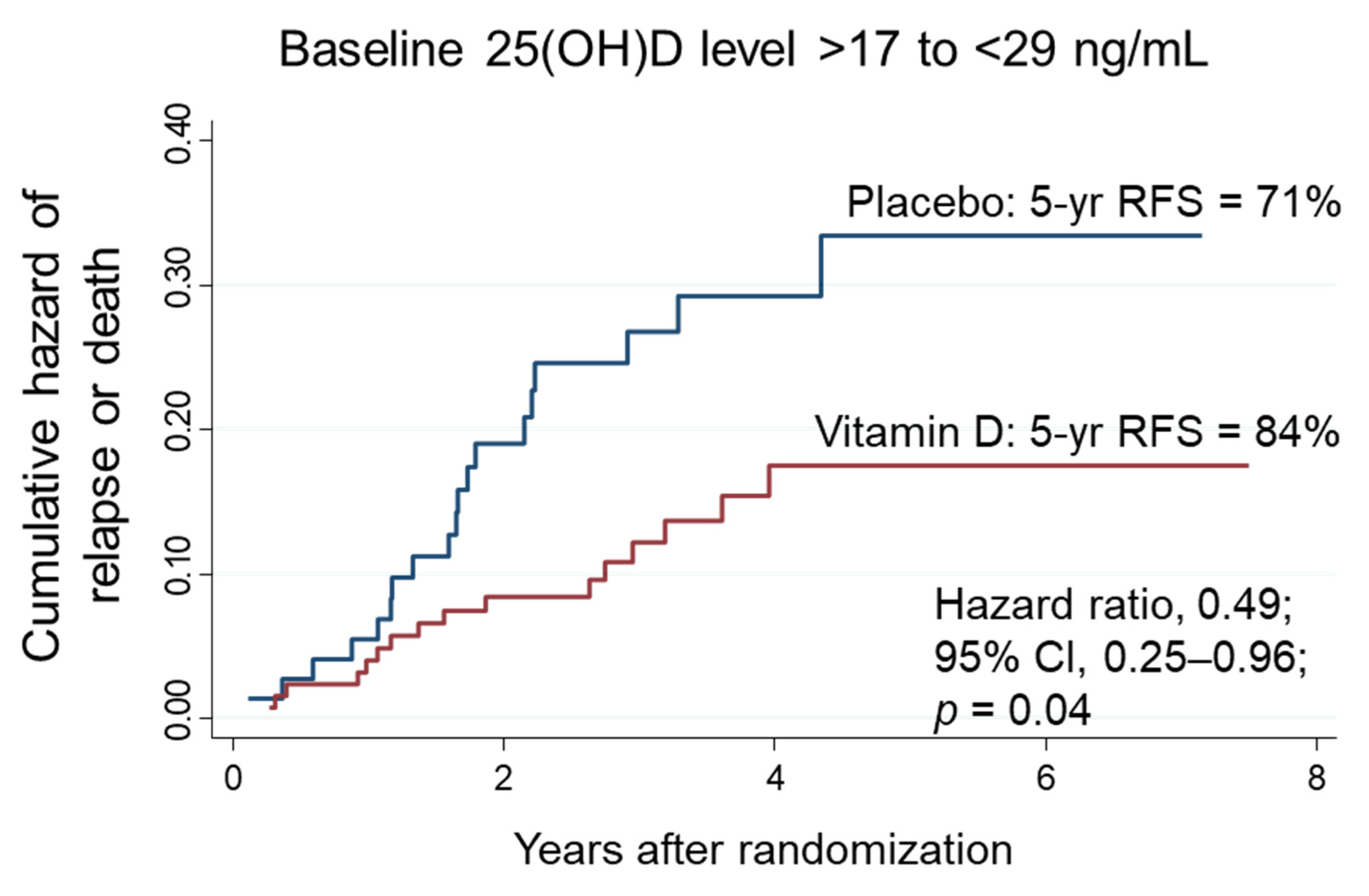
3.6. Relapse-Free Survival in Subgroups Stratified according to Thresholds Determined by MARS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bouillon, R. Comparative analysis of nutritional guidelines for vitamin D. Nat. Rev. Endocrinol. 2017, 13, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Kiely, M. Recommended dietary intakes for vitamin D: Where do they come from, what do they achieve and how can we meet them? J. Hum. Nutr. Diet 2014, 27, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Giustina, A.; Bouillon, R.; Binkley, N.; Sempos, C.; Adler, R.A.; Bollerslev, J.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Heijboer, A.; et al. Controversies in Vitamin D: A Statement From the Third International Conference. JBMR Plus 2020, 4, e10417. [Google Scholar] [CrossRef] [PubMed]
- Lips, P.; Hosking, D.; Lippuner, K.; Norquist, J.M.; Wehren, L.; Maalouf, G.; Ragi-Eis, S.; Chandler, J. The prevalence of vitamin D inadequacy amongst women with osteoporosis: An international epidemiological investigation. J. Intern. Med. 2006, 260, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Malabanan, A.; Veronikis, I.E.; Holick, M.F. Redefining vitamin D insufficiency. Lancet 1998, 351, 805–806. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J. Clin. Endocrinol. Metab. 2012, 97, 1153–1158. [Google Scholar] [CrossRef]
- van Driel, M.; van Leeuwen, J.P.T.M.; Muñoz, A.; Feldman, D. Overview of Vitamin D Actions in Cancer. In Vitamin D; Academic Press: Cambridge, MA, USA, 2018; pp. 711–742. [Google Scholar] [CrossRef]
- Urashima, M.; Ohdaira, H.; Akutsu, T.; Okada, S.; Yoshida, M.; Kitajima, M.; Suzuki, Y. Effect of Vitamin D Supplementation on Relapse-Free Survival Among Patients With Digestive Tract Cancers: The AMATERASU Randomized Clinical Trial. JAMA 2019, 321, 1361–1369. [Google Scholar] [CrossRef]
- Morita, M.; Okuyama, M.; Akutsu, T.; Ohdaira, H.; Suzuki, Y.; Urashima, M. Vitamin D Supplementation Regulates Postoperative Serum Levels of PD-L1 in Patients with Digestive Tract Cancer and Improves Survivals in the Highest Quintile of PD-L1: A Post Hoc Analysis of the AMATERASU Randomized Controlled Trial. Nutrients 2021, 13, 1987. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Valcour, A.; Blocki, F.; Hawkins, D.M.; Rao, S.D. Effects of age and serum 25-OH-vitamin D on serum parathyroid hormone levels. J. Clin. Endocrinol. Metab. 2012, 97, 3989–3995. [Google Scholar] [CrossRef] [PubMed]
- Galior, K.; Grebe, S.; Singh, R. Development of Vitamin D Toxicity from Overcorrection of Vitamin D Deficiency: A Review of Case Reports. Nutrients 2018, 10, 953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieth, R.; Holick, M.F. The IOM—Endocrine Society Controversy on Recommended Vitamin D Targets. In Vitamin D; Academic Press: Cambridge, MA, USA, 2018; pp. 1091–1107. [Google Scholar] [CrossRef]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazaretti-Castro, M.; et al. Consensus statement from 2(nd) International Conference on Controversies in Vitamin D. Rev. Endocr. Metab. Disord. 2020, 21, 89–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heaney, R.P. Guidelines for optimizing design and analysis of clinical studies of nutrient effects. Nutr. Rev. 2014, 72, 48–54. [Google Scholar] [CrossRef]
- Durazo-Arvizu, R.A.; Dawson-Hughes, B.; Sempos, C.T.; Yetley, E.A.; Looker, A.C.; Cao, G.; Harris, S.S.; Burt, V.L.; Carriquiry, A.L.; Picciano, M.F. Three-phase model harmonizes estimates of the maximal suppression of parathyroid hormone by 25-hydroxyvitamin D in persons 65 years of age and older. J. Nutr. 2010, 140, 595–599. [Google Scholar] [CrossRef] [Green Version]
- Ferrone, F.; Pepe, J.; Danese, V.C.; Fassino, V.; Cecchetti, V.; De Lucia, F.; Biamonte, F.; Colangelo, L.; Ferrazza, G.; Panzini, E.; et al. The relative influence of serum ionized calcium and 25-hydroxyvitamin D in regulating PTH secretion in healthy subjects. Bone 2019, 125, 200–206. [Google Scholar] [CrossRef]
- Breiman, L. Statistical Modeling: The Two Cultures (with comments and a rejoinder by the author). Stat. Sci. 2001, 16, 199–231. [Google Scholar] [CrossRef]
- Friedman, J.H.; Roosen, C.B. An introduction to multivariate adaptive regression splines. Stat. Methods Med. Res. 1995, 4, 197–217. [Google Scholar] [CrossRef]
- Glatzle, J.; Piert, M.; Meile, T.; Besenthal, I.; Schafer, J.F.; Konigsrainer, A.; Zittel, T.T. Prevalence of vertebral alterations and the effects of calcium and vitamin D supplementation on calcium metabolism and bone mineral density after gastrectomy. Br. J. Surg. 2005, 92, 579–585. [Google Scholar] [CrossRef]
- Zittel, T.T.; Zeeb, B.; Maier, G.W.; Kaiser, G.W.; Zwirner, M.; Liebich, H.; Starlinger, M.; Becker, H.D. High prevalence of bone disorders after gastrectomy. Am. J. Surg. 1997, 174, 431–438. [Google Scholar] [CrossRef]
- Atsumi, Y.; Rino, Y.; Wada, H.; Kitani, Y.; Ozawa, Y.; Aoyama, T.; Oshima, T.; Yukawa, N.; Yoshikawa, T.; Masuda, M. Changes in bone metabolism after gastric cancer surgery in male patients: A prospective observational study. Gastric Cancer 2019, 22, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Hollis, B.W.; Kamerud, J.Q.; Selvaag, S.R.; Lorenz, J.D.; Napoli, J.L. Determination of vitamin D status by radioimmunoassay with an 125I-labeled tracer. Clin. Chem. 1993, 39, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Curran-Everett, D. Explorations in statistics: The assumption of normality. Adv. Physiol. Educ. 2017, 41, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Levene, H. Robust tests for equality of variances. In Contributions to Probability and Statistics: Essays in Honor of Harold Hotelling; Olkin, I., Ed.; Standford University Press: Palo Alto, CA, USA, 1960; pp. 278–292. [Google Scholar]
- Cleveland, W.S. Robust Locally Weighted Regression and Smoothing Scatterplots. J. Am. Stat. Assoc. 1979, 74, 829–836. [Google Scholar] [CrossRef]
- Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual high-dose oral vitamin D and falls and fractures in older women: A randomized controlled trial. JAMA 2010, 303, 1815–1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson-Hughes, B.; Wang, J.; Barger, K.; Bischoff-Ferrari, H.A.; Sempos, C.T.; Durazo-Arvizu, R.A.; Ceglia, L. Intra-trial mean 25(OH)D and PTH levels and risk of falling in older men and women in the Boston STOP IT trial. J. Clin. Endocrinol. Metab. 2022, 107, e1932–e1937. [Google Scholar] [CrossRef] [PubMed]
- Bisballe, S.; Eriksen, E.F.; Melsen, F.; Mosekilde, L.; Sorensen, O.H.; Hessov, I. Osteopenia and osteomalacia after gastrectomy: Interrelations between biochemical markers of bone remodelling, vitamin D metabolites, and bone histomorphometry. Gut 1991, 32, 1303–1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rino, Y.; Yamamoto, Y.; Wada, N.; Yukawa, N.; Murakami, H.; Tamagawa, H.; Yamada, T.; Ohshima, T.; Masuda, M.; Imada, T. Changes in vitamin D after gastrectomy. Gastric Cancer 2007, 10, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Aloia, J.F.; Talwar, S.A.; Pollack, S.; Feuerman, M.; Yeh, J.K. Optimal vitamin D status and serum parathyroid hormone concentrations in African American women. Am. J. Clin. Nutr. 2006, 84, 602–609. [Google Scholar] [CrossRef] [Green Version]
- Sai, A.J.; Walters, R.W.; Fang, X.; Gallagher, J.C. Relationship between vitamin D, parathyroid hormone, and bone health. J. Clin. Endocrinol. Metab. 2011, 96, E436–E446. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, J.A.; Law, J.; Coakley, K.E.; Zughaier, S.M.; Hao, L.; Shahid Salles, K.; Wasse, H.; Gutierrez, O.M.; Ziegler, T.R.; Tangpricha, V. High-dose cholecalciferol reduces parathyroid hormone in patients with early chronic kidney disease: A pilot, randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2012, 96, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Oh, K.W.; Jang, E.H.; Kim, M.K.; Lim, D.J.; Kwon, H.S.; Baek, K.H.; Yoon, K.H.; Lee, W.C.; Cha, B.Y.; et al. Relationship between vitamin D, parathyroid hormone, and bone mineral density in elderly Koreans. J. Korean Med. Sci. 2012, 27, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Shapses, S.A.; Lee, E.J.; Sukumar, D.; Durazo-Arvizu, R.; Schneider, S.H. The effect of obesity on the relationship between serum parathyroid hormone and 25-hydroxyvitamin D in women. J. Clin. Endocrinol. Metab. 2013, 98, E886–E890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Lv, F.; Zhang, Z.; Deng, W.; Li, Y.; Deng, Z.; Jiang, Y.; Wang, O.; Xing, X.; Xu, L.; et al. Establishment of a normal reference value of parathyroid hormone in a large healthy Chinese population and evaluation of its relation to bone turnover and bone mineral density. Osteoporos. Int. 2016, 27, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Gannagé-Yared, M.H.; Chemali, R.; Yaacoub, N.; Halaby, G. Hypovitaminosis D in a sunny country: Relation to lifestyle and bone markers. J. Bone Min. Res 2000, 15, 1856–1862. [Google Scholar] [CrossRef]
- Kinyamu, H.K.; Gallagher, J.C.; Rafferty, K.A.; Balhorn, K.E. Dietary calcium and vitamin D intake in elderly women: Effect on serum parathyroid hormone and vitamin D metabolites. Am. J. Clin. Nutr. 1998, 67, 342–348. [Google Scholar] [CrossRef]
- Hill, K.M.; McCabe, G.P.; McCabe, L.D.; Gordon, C.M.; Abrams, S.A.; Weaver, C.M. An inflection point of serum 25-hydroxyvitamin D for maximal suppression of parathyroid hormone is not evident from multi-site pooled data in children and adolescents. J. Nutr. 2010, 140, 1983–1988. [Google Scholar] [CrossRef]
- Thomas, M.K.; Lloyd-Jones, D.M.; Thadhani, R.I.; Shaw, A.C.; Deraska, D.J.; Kitch, B.T.; Vamvakas, E.C.; Dick, I.M.; Prince, R.L.; Finkelstein, J.S. Hypovitaminosis D in medical inpatients. N. Engl. J. Med. 1998, 338, 777–783. [Google Scholar] [CrossRef]
- Holick, M.F.; Siris, E.S.; Binkley, N.; Beard, M.K.; Khan, A.; Katzer, J.T.; Petruschke, R.A.; Chen, E.; de Papp, A.E. Prevalence of Vitamin D inadequacy among postmenopausal North American women receiving osteoporosis therapy. J. Clin. Endocrinol. Metab. 2005, 90, 3215–3224. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.W.; Kweon, S.S.; Choi, J.S.; Rhee, J.A.; Lee, Y.H.; Nam, H.S.; Jeong, S.K.; Park, K.S.; Ryu, S.Y.; Song, H.R.; et al. Estimation of the cutoff value of vitamin D: The Dong-gu study. J. Physiol. Anthropol. 2015, 34, 10. [Google Scholar] [CrossRef] [Green Version]
- Chapuy, M.C.; Preziosi, P.; Maamer, M.; Arnaud, S.; Galan, P.; Hercberg, S.; Meunier, P.J. Prevalence of vitamin D insufficiency in an adult normal population. Osteoporos. Int. 1997, 7, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Guillemant, J.; Taupin, P.; Le, H.T.; Taright, N.; Allemandou, A.; Pérès, G.; Guillemant, S. Vitamin D status during puberty in French healthy male adolescents. Osteoporos. Int. 1999, 10, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Wise, S.A.; Camara, J.E.; Sempos, C.T.; Lukas, P.; Le Goff, C.; Peeters, S.; Burdette, C.Q.; Nalin, F.; Hahm, G.; Durazo-Arvizu, R.A.; et al. Vitamin D Standardization Program (VDSP) intralaboratory study for the assessment of 25-hydroxyvitamin D assay variability and bias. J. Steroid Biochem. Mol. Biol. 2021, 212, 105917. [Google Scholar] [CrossRef] [PubMed]
- Vieth, R.; Ladak, Y.; Walfish, P.G. Age-related changes in the 25-hydroxyvitamin D versus parathyroid hormone relationship suggest a different reason why older adults require more vitamin D. J. Clin. Endocrinol. Metab. 2003, 88, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Vaughan-Shaw, P.G.; Zgaga, L.; Ooi, L.Y.; Theodoratou, E.; Timofeeva, M.; Svinti, V.; Walker, M.; O’Sullivan, F.; Ewing, A.; Johnston, S.; et al. Low plasma vitamin D is associated with adverse colorectal cancer survival after surgical resection, independent of systemic inflammatory response. Gut 2020, 69, 103–111. [Google Scholar] [CrossRef]
- Reid, D.; Toole, B.J.; Knox, S.; Talwar, D.; Harten, J.; O’Reilly, D.S.; Blackwell, S.; Kinsella, J.; McMillan, D.C.; Wallace, A.M. The relation between acute changes in the systemic inflammatory response and plasma 25-hydroxyvitamin D concentrations after elective knee arthroplasty. Am. J. Clin. Nutr. 2011, 93, 1006–1011. [Google Scholar] [CrossRef] [Green Version]
- Urashima, M.; Okuyama, M.; Akutsu, T.; Ohdaira, H.; Kaji, M.; Suzuki, Y. Effect of Vitamin D Supplementation on Survival of Digestive Tract Cancer Patients with Low Bioavailable 25-Hydroxyvitamin D levels: A Post Hoc Analysis of the AMATERASU Randomized Clinical Trial. Cancers 2020, 12, 347. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker | Total | Placebo Group | Vitamin D Group | p-Value (between Groups) |
|---|---|---|---|---|
| Age at entry (year) | 66.3 ± 10.7 | 64.2 ± 10.4 | 67.6 ± 10.5 | 0.001 |
| Sex | 0.07 | |||
| Male (%) | 233 (65.3) | 85 (59.4) | 148 (69.2) | |
| Female (%) | 124 (34.7) | 58 (40.6) | 66 (30.8) | |
| BMI (kg/m2) | 22.0 ± 3.5 | 21.9 ± 3.2 | 22.1 ± 3.7 | |
| Cancer site | 0.98 | |||
| Esophagus (%) | 33 (9.2) | 14 (9.8) | 19 (8.9) | |
| Stomach (%) | 152 (42.6) | 61 (42.7) | 91 (42.5) | |
| Small intestine (%) | 2 (0.6) | 1 (0.7) | 1 (0.5) | |
| Colorectum (%) | 170 (47.6) | 67 (46.9) | 103 (48.1) | |
| Stage | 0.36 | |||
| I (%) | 162 (45.4) | 59 (41.3%) | 103 (45.4) | |
| II (%) | 96 (26.9) | 43 (30.1) | 53 (24.8) | |
| III (%) | 99 (27.7) | 41 (28.7) | 58 (27.1) | |
| 25(OH)D a (ng/mL) | 34.9 ± 18.5 | 21.3 ± 9.7 | 44.0 ± 17.3 | <0.001 |
| Ca b (mg/dL) | 9.3 ± 0.4 | 9.3 ± 0.4 | 9.3 ± 0.4 | 0.68 |
| PTH c (pg/mL) | 44.8 ± 17.8 | 47.4 ± 20.8 | 43.0 ± 16.5 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otani, K.; Kanno, K.; Akutsu, T.; Ohdaira, H.; Suzuki, Y.; Urashima, M. Applying Machine Learning to Determine 25(OH)D Threshold Levels Using Data from the AMATERASU Vitamin D Supplementation Trial in Patients with Digestive Tract Cancer. Nutrients 2022, 14, 1689. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14091689
Otani K, Kanno K, Akutsu T, Ohdaira H, Suzuki Y, Urashima M. Applying Machine Learning to Determine 25(OH)D Threshold Levels Using Data from the AMATERASU Vitamin D Supplementation Trial in Patients with Digestive Tract Cancer. Nutrients. 2022; 14(9):1689. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14091689
Chicago/Turabian StyleOtani, Katharina, Kazuki Kanno, Taisuke Akutsu, Hironori Ohdaira, Yutaka Suzuki, and Mitsuyoshi Urashima. 2022. "Applying Machine Learning to Determine 25(OH)D Threshold Levels Using Data from the AMATERASU Vitamin D Supplementation Trial in Patients with Digestive Tract Cancer" Nutrients 14, no. 9: 1689. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14091689