
Sonographic Markers Are Useful for Detection of Early Vascular Deterioration in Children with Overweight/Obesity: Effect of a 1-Year Combined Nutritional Education and Physical Exercise Program
 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Intervention
2.3. Outcome Variables
2.4. Anthropometrical and Other Clinical Parameters
2.5. Measurement of cIMT and Hepatic Steatosis
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
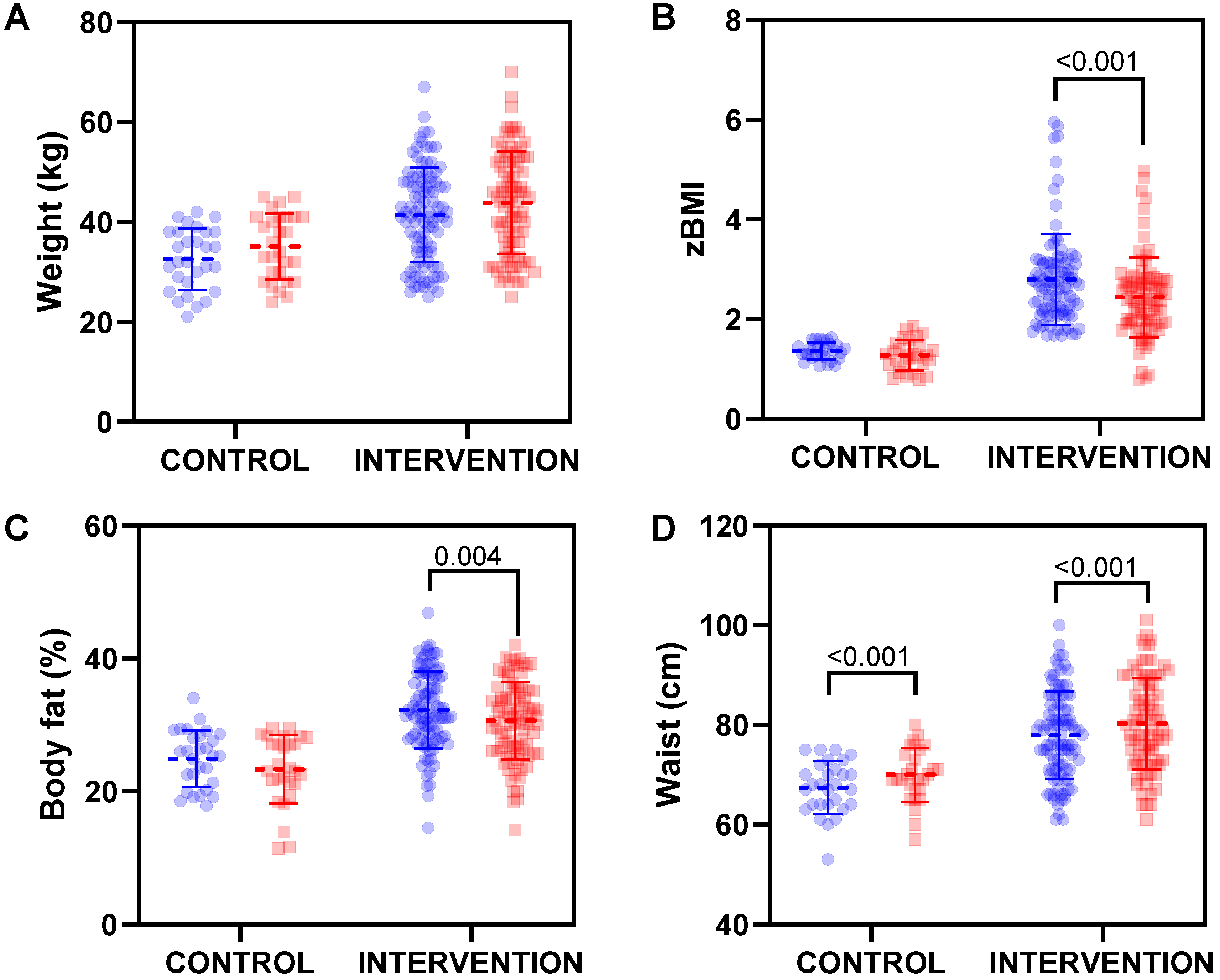
3.2. Effect of Educational Intervention on Anthropometrical Parameters
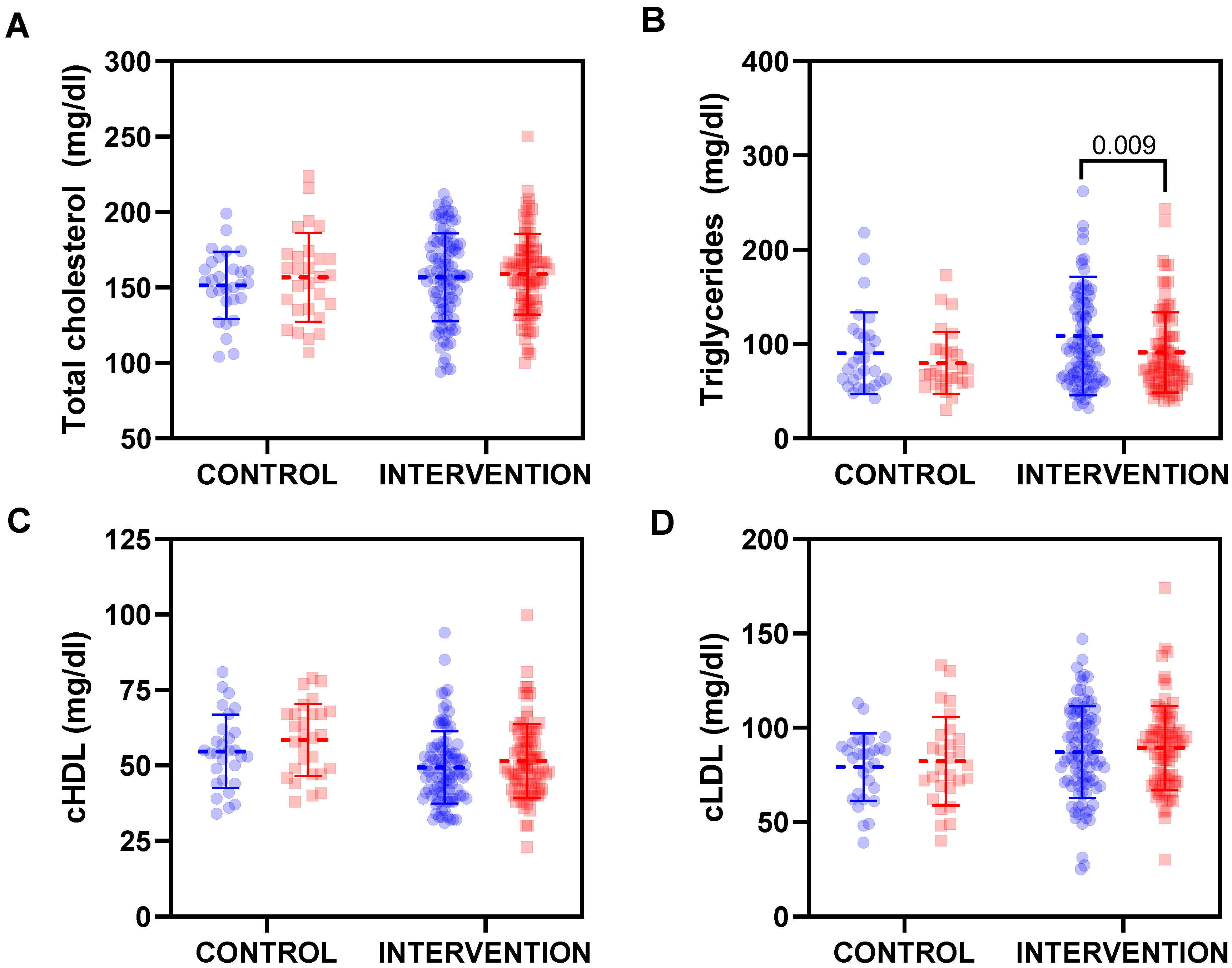
3.3. Effect of Health Educational Intervention on Clinical Parameters
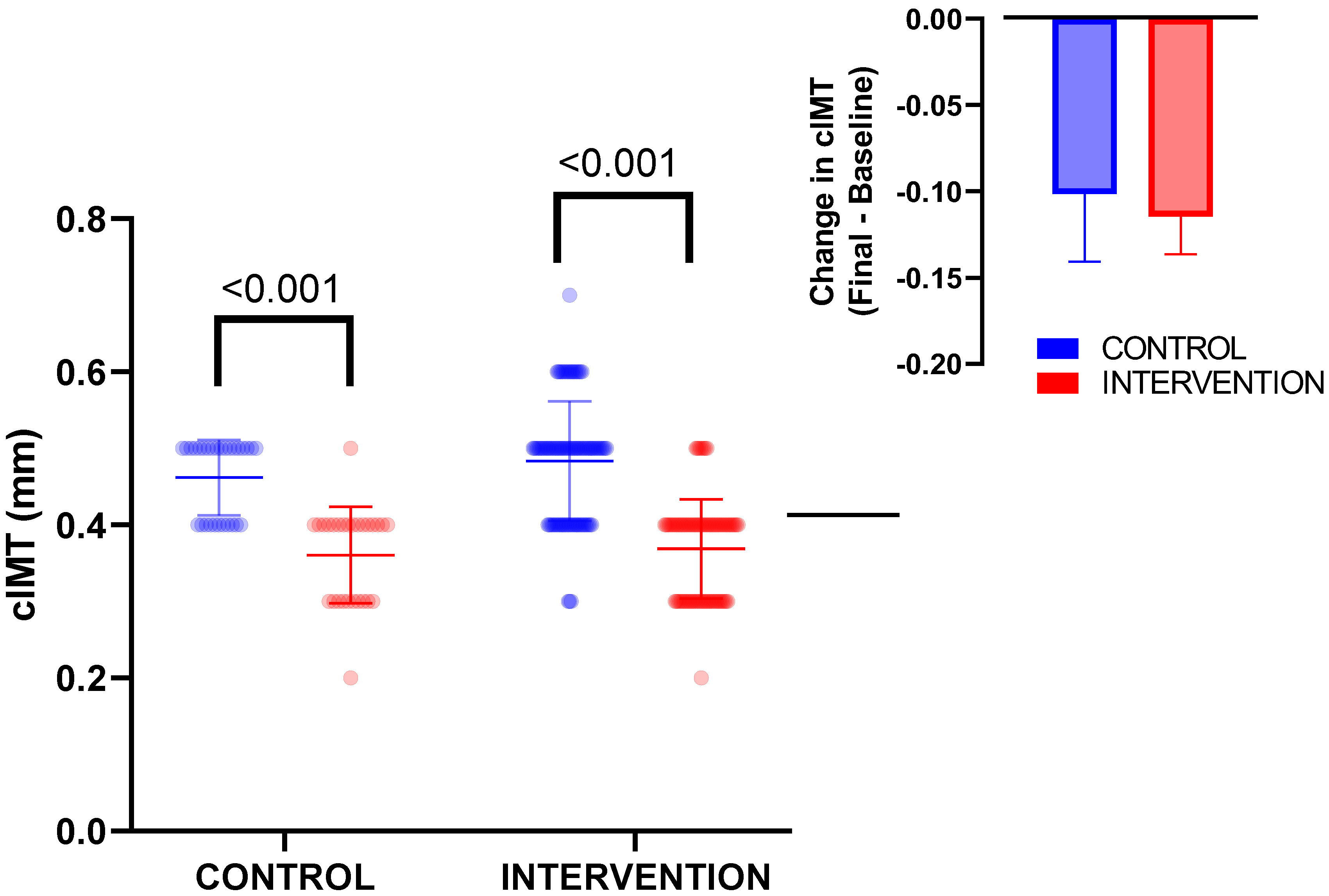
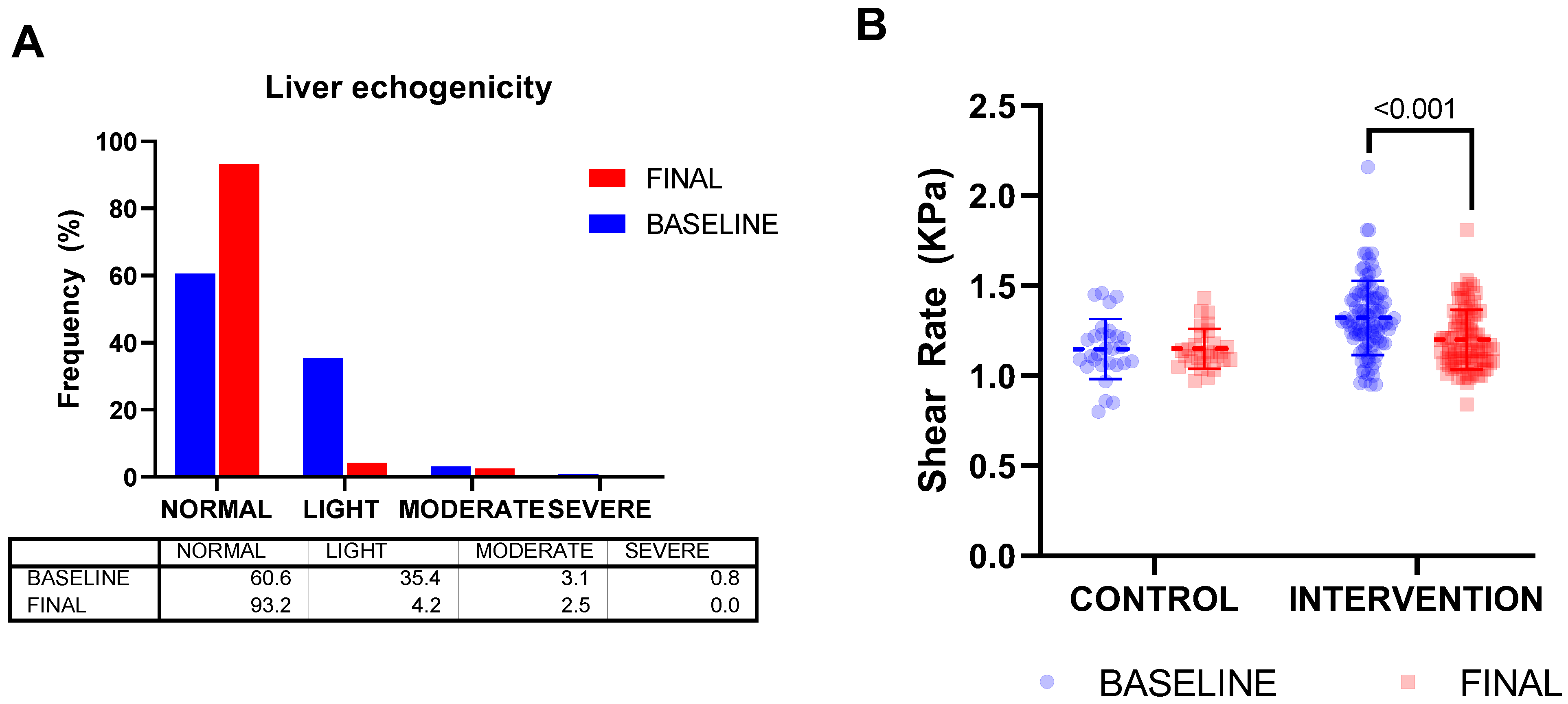
3.4. Effect of Health Educational Intervention on Echography-Related Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, F.X. The Obesity Epidemic: Pathophysiology and Consequences of Obesity. Obes. Res. 2002, 10 (Suppl. 2), 97S–104S. [Google Scholar] [CrossRef] [PubMed]
- Conway, B.; Rene, A. Obesity as a disease: No lightweight matter. Obes. Rev. 2004, 5, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Childhood Obesity Facts|Overweight & Obesity|CDC. Available online: https://www.cdc.gov/obesity/data/childhood.html (accessed on 27 January 2023).
- Estrada, E.; Eneli, I.U.; Hampl, S.; Mietus-Snyder, M.; Mirza, N.; Rhodes, E.; Sweeney, B.; Tinajero-Deck, L.; Woolford, S.J.; Pont, S.J. Children’s Hospital Association Consensus Statements for Comorbidities of Childhood Obesity. Child. Obes. 2014, 10, 304–317. [Google Scholar] [CrossRef]
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-Related Consequences of Childhood Obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef]
- Clemente, M.G.; Mandato, C.; Poeta, M.; Vajro, P. Pediatric non-alcoholic fatty liver disease: Recent solutions, unresolved issues, and future research directions. World J. Gastroenterol. 2016, 22, 8078–8093. [Google Scholar] [CrossRef]
- Torun, E.; Aydin, S.; Gökce, S.; Özgen, I.T.; Donmez, T.; Cesur, Y.; Aydın, S. Carotid intima-media thickness and flow-mediated dilation in obese children with non-alcoholic fatty liver disease. Turk. J. Gastroenterol. 2014, 25 (Suppl. 1), 92–98. [Google Scholar] [CrossRef]
- Wang, C.; Cai, Z.; Deng, X.; Li, H.; Zhao, Z.; Guo, C.; Zhang, P.; Li, L.; Gu, T.; Yang, L.; et al. Association of Hepatic Steatosis Index and Fatty Liver Index with Carotid Atherosclerosis in Type 2 Diabetes. Int. J. Med. Sci. 2021, 18, 3280–3289. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Kheniser, K.; Saxon, D.R.; Kashyap, S.R. Long-Term Weight Loss Strategies for Obesity. J. Clin. Endocrinol. Metab. 2021, 106, 1854–1866. [Google Scholar] [CrossRef]
- Kim, J.; Lim, H. Nutritional Management in Childhood Obesity. J. Obes. Metab. Syndr. 2019, 28, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Hebestreit, A.; Bogl, L.H. Dietary Behavior and Physical Activity in Children and Adolescents. Nutrients 2019, 11, 1849. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Berkel, C.; Carroll, A.J.; Fu, E.; Grimm, K.J.; Mauricio, A.M.; Rudo-Stern, J.; Winslow, E.; Dishion, T.J.; Jordan, N.; et al. Health behaviour outcomes of a family based intervention for paediatric obesity in primary care: A randomized type II hybrid effectiveness-implementation trial. Pediatr. Obes. 2021, 16, e12780. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, K.; Travers, J.; Smaldone, A. Are School Nurses an Overlooked Resource in Reducing Childhood Obesity? A Systematic Review and Meta-Analysis. J. Sch. Health 2016, 86, 309–321. [Google Scholar] [CrossRef]
- Janssen, I.; Wong, S.L.; Colley, R.; Tremblay, M.S. The fractionalization of physical activity throughout the week is associated with the cardiometabolic health of children and youth. BMC Public Health 2013, 13, 554–558. [Google Scholar] [CrossRef]
- Kelly, P.; Matthews, A.; Foster, C. Young and Physically Active: A Blueprint for Making Physical Activity Appealing to Youth; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Gargallo Fernández Manuel, M.; Breton Lesmes, I.; Basulto Marset, J.; Quiles Izquierdo, J.; Formiguera Sala, X.; Salas-Salvadó, J. Evidence-Based Nutritional Recommendations for the Prevention and Treatment of Overweight and Obesity in Adults (FESNAD-SEEDO Consensus Document). The Role of Diet in Obesity Treatment (III/III). Nutr. Hosp. 2012, 27, 833–864. [Google Scholar] [CrossRef]
- Park, M.K. Blood Pressure Tables. Pediatrics 2005, 115, 826–827. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, J.M.; Kim, J.H.; Kim, K.G.; Han, J.K.; Lee, K.H.; Park, S.H.; Yi, N.-J.; Suh, K.-S.; An, S.K.; et al. Appropriateness of a Donor Liver with Respect to Macrosteatosis: Application of Artificial Neural Networks to US Images—Initial Experience. Radiology 2005, 234, 793–803. [Google Scholar] [CrossRef]
- Amini, M.; Djazayery, A.; Majdzadeh, R.; Taghdisi, M.-H.; Sadrzadeh-Yeganeh, H.; Abdollahi, Z.; Hosseinpour-Niazi, N.; Chamari, M.; Nourmohammadi, M. A School-Based Intervention to Reduce Excess Weight in Overweight and Obese Primary School Students. Biol. Res. Nurs. 2016, 18, 531–540. [Google Scholar] [CrossRef]
- Blüher, S.; Petroff, D.; Wagner, A.; Warich, K.; Gausche, R.; Klemm, T.; Wagner, M.; Keller, A. The one year exercise and lifestyle intervention program KLAKS: Effects on anthropometric parameters, cardiometabolic risk factors and glycemic control in childhood obesity. Metabolism 2014, 63, 422–430. [Google Scholar] [CrossRef]
- Recasens, M.A.; Xicola-Coromina, E.; Manresa, J.-M.; Ullmo, P.A.; Jensen, B.B.; Franco, R.; Suarez, A.; Nadal, A.; Vila, M.; Recasens, I.; et al. Impact of school-based nutrition and physical activity intervention on body mass index eight years after cessation of randomized controlled trial (AVall study). Clin. Nutr. 2019, 38, 2592–2598. [Google Scholar] [CrossRef] [PubMed]
- van Sluijs, E.M.F.; Ekelund, U.; Crochemore-Silva, I.; Guthold, R.; Ha, A.; Lubans, D.; Oyeyemi, A.L.; Ding, D.; Katzmarzyk, P.T. Physical activity behaviours in adolescence: Current evidence and opportunities for intervention. Lancet 2021, 398, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Farpour-Lambert, N.J.; Aggoun, Y.; Marchand, L.M.; Martin, X.E.; Herrmann, F.R.; Beghetti, M. Physical Activity Reduces Systemic Blood Pressure and Improves Early Markers of Atherosclerosis in Pre-Pubertal Obese Children. J. Am. Coll. Cardiol. 2009, 54, 2396–2406. [Google Scholar] [CrossRef] [PubMed]
- Maggio, A.B.R.; Aggoun, Y.; Martin, X.E.; Marchand, L.M.; Beghetti, M.; Farpour-Lambert, N.J. Long-term follow-up of cardiovascular risk factors after exercise training in obese children. Int. J. Pediatr. Obes. 2011, 6, e603–e610. [Google Scholar] [CrossRef] [PubMed]
- Kajikawa, M.; Maruhashi, T.; Matsumoto, T.; Iwamoto, Y.; Iwamoto, A.; Oda, N.; Kishimoto, S.; Matsui, S.; Aibara, Y.; Hidaka, T.; et al. Relationship between serum triglyceride levels and endothelial function in a large community-based study. Atherosclerosis 2016, 249, 70–75. [Google Scholar] [CrossRef]
- Pacifico, L.; Arca, M.; Anania, C.; Cantisani, V.; Di Martino, M.; Chiesa, C. Arterial function and structure after a 1-year lifestyle intervention in children with nonalcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 1010–1016. [Google Scholar] [CrossRef]
- Meyer, A.A.; Kundt, G.; Lenschow, U.; Schuff-Werner, P.; Kienast, W. Improvement of Early Vascular Changes and Cardiovascular Risk Factors in Obese Children After a Six-Month Exercise Program. J. Am. Coll. Cardiol. 2006, 48, 1865–1870. [Google Scholar] [CrossRef]
- Woo, K.S.; Chook, P.; Yu, C.W.; Sung, R.Y.; Qiao, M.; Leung, S.S.; Lam, C.W.; Metreweli, C.; Celermajer, D.S. Effects of Diet and Exercise on Obesity-Related Vascular Dysfunction in Children. Circulation 2004, 109, 1981–1986. [Google Scholar] [CrossRef]
- Agbaje, A.O.; Barker, A.R.; Tuomainen, T.-P. Effects of Arterial Stiffness and Carotid Intima-Media Thickness Progression on the Risk of Overweight/Obesity and Elevated Blood Pressure/Hypertension: A Cross-Lagged Cohort Study. Hypertension 2022, 79, 159–169. [Google Scholar] [CrossRef]
- Park, J.-H.; Miyashita, M.; Kwon, Y.-C.; Park, H.-T.; Kim, E.-H.; Park, J.-K.; Park, K.-B.; Yoon, S.-R.; Chung, J.-W.; Nakamura, Y.; et al. A 12-week after-school physical activity programme improves endothelial cell function in overweight and obese children: A randomised controlled study. BMC Pediatr. 2012, 12, 111. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, L.; Calvaruso, V.; Cacopardo, B.; Alessi, N.; Attanasio, M.; Petta, S.; Fatuzzo, F.; Montineri, A.; Mazzola, A.; L’Abbate, L.; et al. Comparison of Transient Elastography and Acoustic Radiation Force Impulse for Non-Invasive Staging of Liver Fibrosis in Patients With Chronic Hepatitis, C. Am. J. Gastroenterol. 2011, 106, 2112–2120. [Google Scholar] [CrossRef]
- Palmeri, M.L.; Wang, M.H.; Rouze, N.C.; Abdelmalek, M.F.; Guy, C.D.; Moser, B.; Diehl, A.M.; Nightingale, K.R. Noninvasive evaluation of hepatic fibrosis using acoustic radiation force-based shear stiffness in patients with nonalcoholic fatty liver disease. J. Hepatol. 2011, 55, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, M.; Suzuki, K.; Kato, S.; Fujita, K.; Nozaki, Y.; Hosono, K.; Saito, S.; Nakajima, A. Nonalcoholic Fatty Liver Disease: US-based Acoustic Radiation Force Impulse Elastography. Radiology 2010, 256, 640–647. [Google Scholar] [CrossRef] [PubMed]
- El-Koofy, N.; Soliman, H.; Elbarbary, M.-A.; El Garhy, A.S.; Sheba, M.; Fouad, H. Use of Anthropometry Versus Ultrasound for the Assessment of Body Fat and Comorbidities in Children With Obesity. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 782–788. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 29) | Intervention (n = 148) | p (t) | |
|---|---|---|---|
| Age (y) | 8 ± 2 | 8 ± 2 | 0.881 |
| Weight (kg) | 32.6 ± 6.1 | 41.5 ± 9.5 | <0.001 |
| Height (cm) | 130.7 ± 9.3 | 133.2 ± 10.6 | 0.251 |
| BMI (z-score) | 1.36 ± 0.18 | 2.80 ± 0.91 | <0.001 |
| Body fat mass (kg) | 8.19 ± 2.31 | 13.61 ± 4.82 | <0.001 |
| Waist circumference (cm) | 67.4 ± 5.3 | 77.9 ± 8.7 | <0.001 |
| SBP (mmHg) | 106.6 ± 8.1 | 107.7 ± 10.8 | 0.601 |
| DBP (mmHG) | 69.6 ± 8.6 | 68.7 ± 8.7 | 0.615 |
| AST (IU/L) | 30.3 ± 5.9 | 34.1 ± 9.6 | 0.045 |
| ALT (IU/L) | 26.2 ± 6.7 | 33.0 ± 13.9 | <0.001 |
| AST/ALT ratio | 1.18 ± 0.22 | 1.12 ± 0.41 | 0.410 |
| GGT (IU/L) | 14.3 ± 5.8 | 16.9 ± 5.4 | 0.028 |
| Total cholesterol (mg/dL) | 151.4 ± 22.3 | 156.8 ± 29.1 | 0.293 |
| Triglycerides (mg/dL) | 90.1 ± 43.3 | 108.5 ± 63.1 | 0.145 |
| HDL-chol (mg/dL) | 54.6 ± 12.2 | 49.3 ± 12.0 | 0.040 |
| LDL-chol (mg/dL) | 79.2 ± 17.9 | 87.1 ± 24.3 | 0.107 |
| FPG (mg/dL) | 84.1 ± 7.1 | 86.1 ± 5.3 | 0.115 |
| Insulin (IU/mL) | 5.8 ± 2.7 | 9.9 ± 9.1 | <0.001 |
| HOMA index | 1.22 ± 0.58 | 2.15 ± 2.19 | <0.001 |
| Carotid IMT (mm) | 0.46 ± 0.05 | 0.48 ± 0.08 | 0.163 |
| Hepatic Shear Rate (KPa) | 1.15 ± 0.16 | 1.32 ± 0.21 | 0.445 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abellaneda Millán, M.; Morillas-Ruiz, J.M.; Ballester Sajardo, R.; Guillén Martínez, D.; Morales Moreno, I.; Hernández Morante, J.J. Sonographic Markers Are Useful for Detection of Early Vascular Deterioration in Children with Overweight/Obesity: Effect of a 1-Year Combined Nutritional Education and Physical Exercise Program. Nutrients 2023, 15, 894. https://0-doi-org.brum.beds.ac.uk/10.3390/nu15040894
Abellaneda Millán M, Morillas-Ruiz JM, Ballester Sajardo R, Guillén Martínez D, Morales Moreno I, Hernández Morante JJ. Sonographic Markers Are Useful for Detection of Early Vascular Deterioration in Children with Overweight/Obesity: Effect of a 1-Year Combined Nutritional Education and Physical Exercise Program. Nutrients. 2023; 15(4):894. https://0-doi-org.brum.beds.ac.uk/10.3390/nu15040894
Chicago/Turabian StyleAbellaneda Millán, María, Juan María Morillas-Ruiz, Raúl Ballester Sajardo, Daniel Guillén Martínez, Isabel Morales Moreno, and Juan José Hernández Morante. 2023. "Sonographic Markers Are Useful for Detection of Early Vascular Deterioration in Children with Overweight/Obesity: Effect of a 1-Year Combined Nutritional Education and Physical Exercise Program" Nutrients 15, no. 4: 894. https://0-doi-org.brum.beds.ac.uk/10.3390/nu15040894