
Excessive Consumption of Alcoholic Beverages and Extremely High Levels of High-Density Lipoprotein Cholesterol (HALP) in the ELSA-Brasil Cohort Baseline

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
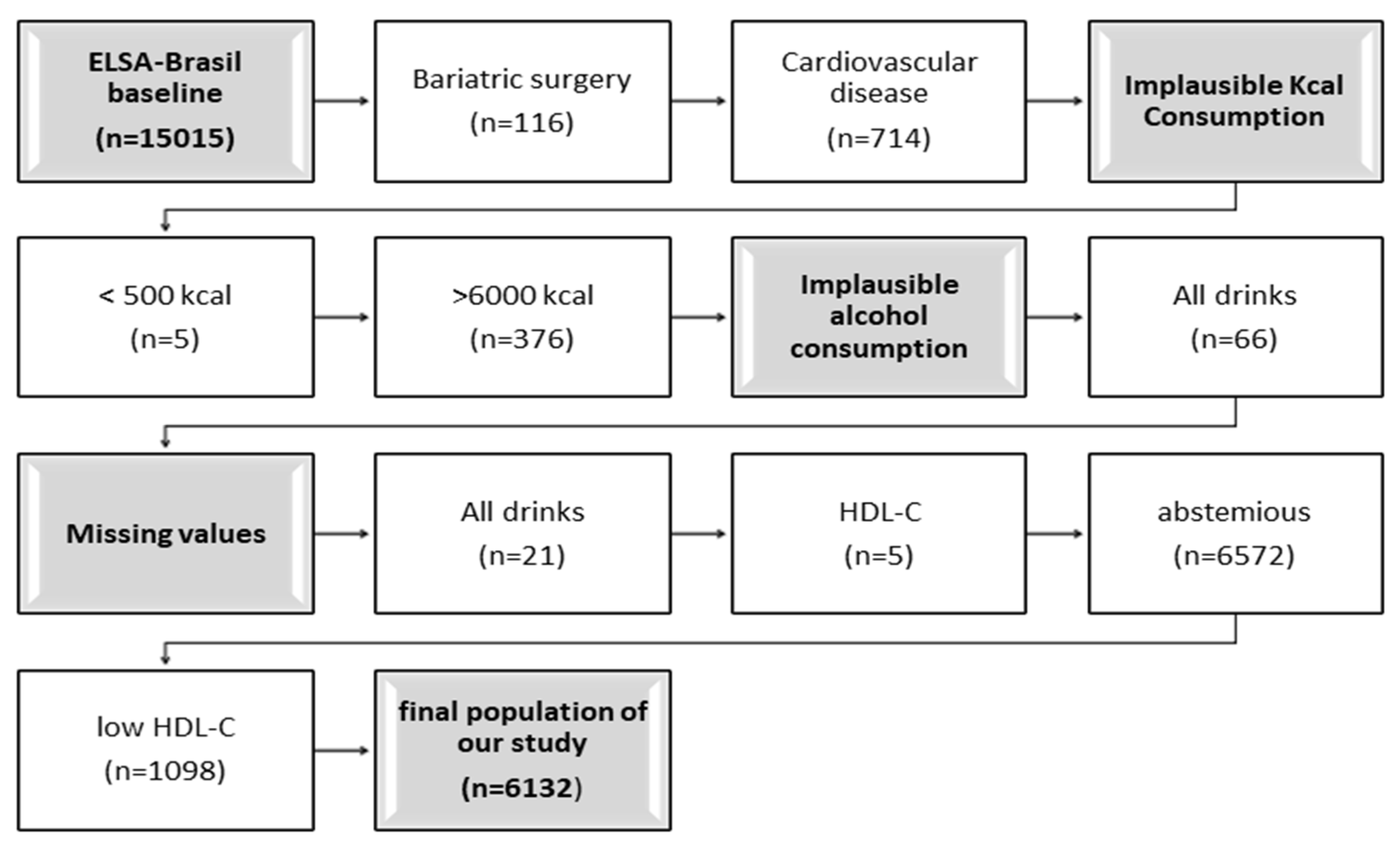
2.1. Study Design and Population
2.2. Ethical Aspects
2.3. Study Variables
2.4. Alcohol Consumption
2.5. Blood Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health 2018: Executive Summary. 2018, pp. 1–16. Available online: https://apps.who.int/iris/rest/bitstreams/1217404/retrieve#:~:text=In 2016%2C (accessed on 13 January 2023).
- Grucza, R.A.; Sher, K.J.; Kerr, W.C.; Krauss, M.J.; Lui, C.K.; McDowell, Y.E.; Hartz, S.; Virdi, G.; Bierut, L.J. Trends in Adult Alcohol Use and Binge Drinking in the Early 21st-Century United States: A Meta-Analysis of 6 National Survey Series. Alcohol. Clin. Exp. Res. 2018, 42, 1939–1950. [Google Scholar] [CrossRef]
- Manthey, J.; Shield, K.D.; Rylett, M.; Hasan, O.S.M.; Probst, C.; Rehm, J. Global alcohol exposure between 1990 and 2017 and forecasts until 2030: A modelling study. Lancet 2019, 393, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Jomard, A.; Osto, E. High Density Lipoproteins: Metabolism, Function, and Therapeutic Potential. Front. Cardiovasc. Med. 2020, 7, 39. [Google Scholar] [CrossRef]
- Julve, J.; Escolà-Gil, J.C. High-Density Lipoproteins and Cardiovascular Disease: The Good, the Bad, and the Future II. Biomedicines 2022, 10, 620. [Google Scholar] [CrossRef] [PubMed]
- Rye, K.-A.; Barter, P.J. Cardioprotective functions of HDLs. J. Lipid Res. 2014, 55, 168–179. [Google Scholar] [CrossRef] [Green Version]
- Cordero, A.; Moreno-Arribas, J.; Bertomeu-González, V.; Agudo, P.; Miralles, B.; Masiá, M.D.; López-Palop, R.; Bertomeu-Martínez, V. Low Levels of High-Density Lipoproteins Cholesterol Are Independently Associated With Acute Coronary Heart Disease in Patients Hospitalized for Chest Pain. Revista Española Cardiología 2012, 65, 319–325. [Google Scholar] [CrossRef]
- Brown, B.G.; Zhao, X.-Q.; Chait, A.; Fisher, L.D.; Cheung, M.C.; Morse, J.S.; Dowdy, A.A.; Marino, E.K.; Bolson, E.L.; Alaupovic, P.; et al. Simvastatin and Niacin, Antioxidant Vitamins, or the Combination for the Prevention of Coronary Disease. N. Engl. J. Med. 2001, 345, 1583–1592. [Google Scholar] [CrossRef] [PubMed]
- Besler, C.; Heinrich, K.; Rohrer, L.; Doerries, C.; Riwanto, M.; Shih, D.M.; Chroni, A.; Yonekawa, K.; Stein, S.; Schaefer, N.; et al. Mechanisms underlying adverse effects of HDL on eNOS-activating pathways in patients with coronary artery disease. J. Clin. Investig. 2011, 121, 2693–2708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, P.J.; Khera, A.V.; Wilensky, R.L.; Rader, D.J. Anti-oxidative and cholesterol efflux capacities of high-density lipoprotein are reduced in ischaemic cardiomyopathy. Eur. J. Heart Fail. 2013, 15, 1215–1219. [Google Scholar] [CrossRef] [Green Version]
- Hirano, K.-I.; Yamashita, S.; Nakajima, N.; Arai, T.; Maruyama, T.; Yoshida, Y.; Ishigami, M.; Sakai, N.; Kameda-Takemura, K.; Matsuzawa, Y. Genetic Cholesteryl Ester Transfer Protein Deficiency Is Extremely Frequent in the Omagari Area of Japan. Marked hyperalphalipoproteinemia caused by CETP gene mutation is not associated with longevity. Arter. Thromb. Vasc. Biol. 1997, 17, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.-W.; Park, S.-J.; Yi, J.-J.; Ohrr, H.; Kim, H. High-density lipoprotein cholesterol and all-cause mortality by sex and age: A prospective cohort study among 15.8 million adults. Int. J. Epidemiol. 2020, 50, 902–913. [Google Scholar] [CrossRef] [PubMed]
- Kontush, A.; de Faria, E.C.; Chantepie, S.; Chapman, M.J. Antioxidative activity of HDL particle subspecies is impaired in hyperalphalipoproteinemia: Relevance of enzymatic and physicochemical properties. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Hirano, K.-I.; Nagasaka, H.; Kobayashi, K.; Yamaguchi, S.; Suzuki, A.; Toda, T.; Doyu, M. Disease-associated marked hyperalphalipoproteinemia. Mol. Genet. Metab. Rep. 2014, 1, 264–268. [Google Scholar] [CrossRef]
- Borggreve, S.E.; Hillege, H.L.; Wolffenbuttel, B.H.; De Jong, P.E.; Zuurman, M.W.; Van Der Steege, G.; Van Tol, A.; Dullaart, R.P.F. An Increased Coronary Risk Is Paradoxically Associated with Common Cholesteryl Ester Transfer Protein Gene Variations That Relate to Higher High-Density Lipoprotein Cholesterol: A Population-Based Study. J. Clin. Endocrinol. Metab. 2006, 91, 3382–3388. [Google Scholar] [CrossRef]
- Laurinavicius, A.G.; Santos, I.S.; Santos, R.D.; Bensenor, I.M.; Conceição, R.D.; Lotufo, P.A. Extremely elevated HDL-cholesterol levels are not associated with increased carotid intima-media thickness: Data from ELSA Brasil. J. Clin. Lipidol. 2016, 10, 898–904.e1. [Google Scholar] [CrossRef]
- Curb, J.D.; Abbott, R.D.; Rodriguez, B.L.; Masaki, K.; Chen, R.; Sharp, D.S.; Tall, A.R. A prospective study of HDL-C and cholesteryl ester transfer protein gene mutations and the risk of coronary heart disease in the elderly. J. Lipid Res. 2004, 45, 948–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulley, S.B.; Cohen, R.; Widdowson, G. Plasma High-Density Lipoprotein Cholesterol Level: Influence of Risk Factor Intervention. JAMA 1977, 238, 2269–2271. [Google Scholar] [CrossRef]
- Bagnardi, V.; Zatonski Scotti, L.; La Vecchia, C.; Corrao, G. Does drinking pattern modify the effect of alcohol on the risk of coronary heart disease? Evidence from a meta-analysis. J. Epidemiol. Community Health 2008, 62, 615–619. [Google Scholar] [CrossRef]
- Millwood, I.Y.; Walters, R.G.; Mei, X.W.; Guo, Y.; Yang, L.; Bian, Z.; Bennett, D.A.; Chen, Y.; Dong, C.; Hu, R.; et al. Conventional and genetic evidence on alcohol and vascular disease aetiology: A prospective study of 500,000 men and women in China. Lancet 2019, 393, 1831–1842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- So-Armah, K.A.; Cheng, D.M.; Freiberg, M.S.; Gnatienko, N.; Patts, G.; Ma, Y.; White, L.; Blokhina, E.; Lioznov, D.; Doyle, M.F.; et al. Association between alcohol use and inflammatory biomarkers over time among younger adults with HIV—The Russia ARCH Observational Study. PLoS ONE 2019, 14, e0219710. [Google Scholar] [CrossRef] [Green Version]
- Castelli, W.P.; Doyle, J.T.; Gordon, T.; Hames, C.G.; Hjortland, M.C.; Hulley, S.B.; Kagan, A.; Zukel, W.J. HDL cholesterol and other lipids in coronary heart disease. The cooperative lipoprotein phenotyping study. Circulation 1977, 55, 767–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Steeg, W.A.; Holme, I.; Boekholdt, S.M.; Larsen, M.L.; Lindahl, C.; Stroes, E.S.; Tikkanen, M.J.; Wareham, N.J.; Faergeman, O.; Olsson, A.G.; et al. High-Density Lipoprotein Cholesterol, High-Density Lipoprotein Particle Size, and Apolipoprotein A-I: Significance for Cardiovascular Risk. The IDEAL and EPIC-Norfolk Studies. J. Am. Coll. Cardiol. 2008, 51, 634–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Averina, M.; Nilssen, O.; Brenn, T.; Brox, J.; Arkhipovsky, V.L.; Kalinin, A.G. Social and lifestyle determinants of depression, anxiety, sleeping disorders and self-evaluated quality of life in Russia—A population-based study in Arkhangelsk. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 511–518. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.H.; Bybee, K.A.; Lavie, C.J. Alcohol and Cardiovascular Health: The Razor-Sharp Double-Edged Sword. J. Am. Coll. Cardiol. 2007, 50, 1009–1014. [Google Scholar] [CrossRef] [Green Version]
- Hansel, B.; Thomas, F.; Pannier, B.; Bean, K.; Kontush, A.; Chapman, M.J.; Guize, L.; Bruckert, E. Relationship between alcohol intake, health and social status and cardiovascular risk factors in the Urban Paris-Ile-de-France Cohort: Is the cardioprotective action of alcohol a myth? Eur. J. Clin. Nutr. 2010, 64, 561–568. [Google Scholar] [CrossRef] [Green Version]
- Enríquez Martínez, O.G.; Luft, V.C.; Faria CP de Molina, M.D.C.B. Alcohol consumption and lipid profile in participants of the Longitudinal Study of Adult Health (ELSA-BRASIL). Nutr. Hosp. 2019, 36, 665–673. [Google Scholar]
- Nova, E.; Mauro-Martín, I.S.; Díaz-Prieto, L.E.; Marcos, A. Wine and beer within a moderate alcohol intake is associated with higher levels of HDL-c and adiponectin. Nutr. Res. 2019, 63, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.; Li, J.; Shearer, G.C.; Lichtenstein, A.H.; Zheng, X.; Wu, Y.; Jin, C.; Wu, S.; Gao, X. Longitudinal study of alcohol consumption and HDL concentrations: A community-based study. Am. J. Clin. Nutr. 2017, 105, 905–912. [Google Scholar] [CrossRef] [Green Version]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric standardization reference manual; Human Kinetics Books: Champaing, IL, USA, 1988. [Google Scholar]
- Molina, M.D.C.B.; Benseñor, I.M.; Cardoso, L.D.O.; Velasquez-Melendez, G.; Drehmer, M.; Pereira, T.S.S.; Faria, C.P.D.; Melere, C.; Manato, L.; Gomes, A.L.C.; et al. Reprodutibilidade e validaderelativa do Questionário de FrequênciaAlimentar do ELSA-Brasil Reproducibility and relative validity of the Food Frequency Questionnaire used in the ELSA-BrasilReproducibilidad y validezrelativa del Cuestionario de Frecuenc. Cadernos de SaúdePública 2013, 29, 379–389. [Google Scholar]
- Martinez, O.G.E.; Aprelini, C.M.D.O.; Moreira, T.K.B.; Alves, S.A.; Pereira, T.S.S.; Siqueira, J.H.; Ferriani, L.O.; de Faria, C.P.; Molina, M.D.C.B. Reproducibility and validity ELSA-Brasil Food Frequency Questionnaire. Revista Española Nutrición Humana y Dietética 2021, 25, 294–302. [Google Scholar] [CrossRef]
- Chor, D.; Alves, M.G.D.M.; Giatti, L.; Cade, N.V.; Nunes, M.A.; Molina, M.D.C.B.; Benseñor, I.M.; Aquino, E.M.; Passos, V.; Santos, S.M.; et al. Questionnaire development in ELSA-Brasil: Challenges of a multidimensional instrument. Rev. SaúdePublica 2013, 47 (Suppl. S2), 27–36. [Google Scholar]
- U.S. Department of Health and Human Services. Dietary Guidelines for Americans 2005. Available online: https://health.gov/sites/default/files/2020-01/DGA2005.pdf (accessed on 16 December 2022).
- Fedeli, L.G.; Vidigal, P.G.; Leite, C.M.; Castilhos, C.D.; Pimentel, R.A.; Maniero, V.C.; Mill, J.G.; A Lotufo, P.; Pereira, A.C.; Bensenor, I.M. Logistica de coleta e transporte de material biologico e organizacao do laboratorio central no ELSA-Brasil. Revista SaúdePública 2013, 47, 63–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, L.G.V.; Melo, A.P.S.; César, C.C. Prevalência do consumomoderado e excessivo de álcool e fatoresassociados entre residentes de ComunidadesQuilombolas de Vitória da Conquista, Bahia, Brasil. Ciência&SaúdeColetiva 2015, 20, 809–820. [Google Scholar] [CrossRef] [Green Version]
- Oates, C.P.; Koenig, D.; Rhyne, J.; Bogush, N.; O’Connell, J.; Mitchell, B.D.; Miller, M. Novel polymorphisms associated with hyperalphalipoproteinemia and apparent cardioprotection. J. Clin. Lipidol. 2018, 12, 110–115. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Hutchins, P.M.; Matthews, K.A.; Brooks, M.M.; Orchard, T.J.; Ronsein, G.E.; Heinecke, J.W. Cholesterol Efflux Capacity and Subclasses of HDL Particles in Healthy Women Transitioning Through Menopause. J. Clin. Endocrinol. Metab. 2016, 101, 3419–3428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, A.Z.; Dwyer, J.H. Sex differences in the relation of HDL cholesterol to progression of carotid intima-media thickness: The Los Angeles Atherosclerosis Study. Atherosclerosis 2007, 195, e191–e196. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Obesity: Preventing and Managing the Global Epidemic: Report of a Who Consultation on Obesity; World Heal Organ: Geneva, Switzerland, 1998. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/11234459 (accessed on 12 December 2022).
- Shohaimi, S.; Boekholdt, M.S.; Luben, R.; Wareham, N.J.; Khaw, K.-T. Distribution of lipid parameters according to different socio-economic indicators- the EPIC-Norfolk prospective population study. BMC Public Health 2014, 14, 782. [Google Scholar] [CrossRef] [Green Version]
- Espírito Santo, L.R.; Faria, T.O.; Silva, C.S.O.; Xavier, L.A.; Reis, V.C.; Mota, G.A.; Silveira, M.F.; Mill, J.G.; Baldo, M.P. Socioeconomic status and education level are associated with dyslipidemia in adults not taking lipid-lowering medication: A population-based study. Int. Health 2019, 14, 346–353. [Google Scholar] [CrossRef]
- Benetou, V.; Chloptsios, Y.; Zavitsanos, X.; Karalis, D.; Naska, A.; Trichopoulou, A. Total cholesterol and HDL-cholesterol in relation to socioeconomic status in a sample of 11,645 Greek adults: The EPIC study in Greece. European Prospective Investigation into Nutrition and Cancer. Scand. J. Public Health 2000, 28, 260–265. [Google Scholar] [CrossRef]
- Lara, M.; Amigo, H. Association between education and blood lipid levels as income increases over a decade: A cohort study. BMC Public Health 2018, 18, 286. [Google Scholar] [CrossRef] [Green Version]
- Wilkins, J.T.; Ning, H.; Stone, N.J.; Criqui, M.H.; Zhao, L.; Greenland, P.; Lloyd-Jones, D.M. Coronary Heart Disease Risks Associated with High Levels of HDL Cholesterol. J. Am. Heart Assoc. 2014, 3, e000519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, H.; Alsalhe, T.A.; Chalghaf, N.; Riccò, M.; Bragazzi, N.L.; Wu, J. The global burden of disease attributable to high body mass index in 195 countries and territories, 1990–2017: An analysis of the Global Burden of Disease Study. PLoS Med. 2020, 17, e1003198. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Bora, K.; Pathak, M.S.; Borah, P.; Das, D. Association of decreased high-density lipoprotein cholesterol (HDL-C) with obesity and risk estimates for decreased HDL-C attributable to obesity: Preliminary findings from a hospital-based study in a city from Northeast India. J. Prim. Care Community Health 2017, 8, 26–30. [Google Scholar] [CrossRef]
- Mandai, N.; Akazawa, K.; Hara, N.; Ide, Y.; Ide, K.; Dazai, U.; Chishaki, A.; Chishaki, H. Body Weight Reduction Results in Favorable Changes in Blood Pressure, Serum Lipids, and Blood Sugar in Middle-Aged Japanese Persons: A 5-Year Interval Observational Study of 26,824 Cases. Glob. J. Health Sci. 2015, 7, 159–170. [Google Scholar] [CrossRef] [Green Version]
- Finelli, C.; Crispino, P.; Gioia, S.; La Sala, N.; D’amico, L.; La Grotta, M.; Miro, O.; Colarusso, D. The improvement of large High-Density Lipoprotein (HDL) particle levels, and presumably HDL metabolism, depend on effects of low-carbohydrate diet and weight loss. EXCLI J. 2016, 15, 166–176. [Google Scholar]
- Ryan, D.H.; Yockey, S.R. Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over. Curr. Obes. Rep. 2017, 6, 187–194. [Google Scholar] [CrossRef]
- Bazzano, L.A.; Gu, D.; Reynolds, K.; Chen, J.; Wu, X.; Chen, C.-S.; Duan, X.; Chen, J.; He, J. Alcohol consumption and risk of coronary heart disease among Chinese men. Int. J. Cardiol. 2009, 135, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Polsky, S.; Akturk, H.K. Alcohol Consumption, Diabetes Risk, and Cardiovascular Disease Within Diabetes. Curr. Diabetes Rep. 2017, 17, 136. [Google Scholar] [CrossRef]
- Park, H.; Shin, S.K.; Joo, I.; Song, D.S.; Jang, J.W.; Park, J.-W. Systematic Review with Meta-Analysis: Low-Level Alcohol Consumption and the Risk of Liver Cancer. Gut Liver 2020, 14, 792–807. [Google Scholar] [CrossRef]
- Ma, H.; Li, X.; Zhou, T.; Sun, D.; Shai, I.; Heianza, Y.; Rimm, E.B.; Manson, J.E.; Qi, L. Alcohol Consumption Levels as Compared With Drinking Habits in Predicting All-Cause Mortality and Cause-Specific Mortality in Current Drinkers. Mayo Clin. Proc. 2021, 96, 1758–1769. [Google Scholar] [CrossRef]
- Barter, P.J.; Caulfield, M.; Eriksson, M.; Grundy, S.M.; Kastelein, J.J.P.; Komajda, M.; Lopez-Sendon, J.; Mosca, L.; Tardif, J.-C.; Waters, D.D.; et al. Effects of Torcetrapib in Patients at High Risk for Coronary Events. N. Engl. J. Med. 2007, 357, 2109–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bots, M.L.; Visseren, F.L.; Evans, G.W.; Riley, W.A.; Revkin, J.H.; Tegeler, C.H.; Shear, C.L.; Duggan, W.T.; Vicari, R.M.; Grobbee, D.E.; et al. Torcetrapib and carotid intima-media thickness in mixed dyslipidemia (RADIANCE 2 study): A randomized, double-blind trial. Lancet 2007, 370, 153–160. [Google Scholar] [CrossRef]
- Schaefer, E.J.; Asztalos, B.F. Cholesteryl ester transfer protein inhibition, high-density lipoprotein metabolism and heart disease risk reduction. Curr. Opin. Lipidol. 2006, 17, 394–398. [Google Scholar] [CrossRef]
- Swertfeger, D.K.; Rebholz, S.; Li, H.; Shah, A.S.; Davidson, W.S.; Lu, L.J. Feasibility of a plasma bioassay to assess oxidative protection of low-density lipoproteins by high-density lipoproteins. J. Clin. Lipidol. 2018, 12, 1539–1548. [Google Scholar] [CrossRef]
- Movva, R.; Rader, D.J. Laboratory Assessment of HDL Heterogeneity and Function. Clin. Chem. 2008, 54, 788–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacks, F.M.; Liang, L.; Furtado, J.D.; Cai, T.; Davidson, W.S.; He, Z.; McClelland, R.L.; Rimm, E.B.; Jensen, M.K. Protein-Defined Subspecies of HDLs (High-Density Lipoproteins) and Differential Risk of Coronary Heart Disease in 4 Prospective Studies. Arter. Thromb. Vasc. Biol. 2020, 40, 2714–2727. [Google Scholar] [CrossRef]
- Axley, P.D.; Richardson, C.T.; Singal, A.K. Epidemiology of Alcohol Consumption and Societal Burden of Alcoholism and Alcoholic Liver Disease. Clin. Liver Dis. 2019, 23, 39–50. [Google Scholar] [CrossRef]
- Brien, S.E.; Ronksley, P.E.; Turner, B.J.; Mukamal, K.J.; A Ghali, W. Effect of alcohol consumption on biological markers associated with risk of coronary heart disease: Systematic review and meta-analysis of interventional studies. BMJ 2011, 342, d636. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira e Silva, E.R.; Foster, D.; McGee Harper, M.; Seidman, C.E.; Smith, J.D.; Breslow, J.L.; Brinton, E.A. Alcohol consumption raises HDL cholesterol levels by increasing the transport rate of apolipoproteins A-I and A-II. Circulation 2000, 102 (Suppl. S19), 2347–2352. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Normal | HALP | p | |
|---|---|---|---|
| n (%) | n (%) | ||
| 5717 (93.2) | 415 (6.8) | ||
| Sex | |||
| Male | 3312 (57.9) | 100 (24.1) | <0.001 |
| Female | 2405 (42.1) | 315 (75.9) | |
| Income Tertile | |||
| 1 | 1926 (33.7) | 107 (25.8) | <0.001 |
| 2 | 1907 (33.4) | 133 (32.1) | |
| 3 | 1874 (32.8) | 174 (42.0) | |
| Education Level | |||
| Primary incomplete | 236 (4.1) | 20 (4.8) | 0.038 |
| Primary complete | 305 (5.3) | 18 (4.3) | |
| High school complete | 1722 (30.1) | 100 (24.1) | |
| University complete | 3454 (60.4) | 277 (66.7) | |
| Marital Status | |||
| Married | 3995 (69.9) | 227 (54.7) | <0.001 |
| Separated/divorced | 910 (15.9) | 78 (18.8) | |
| Single | 467 (8.2) | 68 (16.4) | |
| Widower | 155 (2.7) | 19 (4.6) | |
| Other (with previous union) | 190 (3.3) | 23 (5.5) | |
| Ethnicity | |||
| Not white | 2371 (42.0) | 171 (41.7) | 0.918 |
| White | 3269 (58.0) | 239 (58.3) | |
| lipid-lowering drugs | |||
| No | 5037 (88.1) | 390 (94.0) | <0.001 |
| Yes | 680 (11.9) | 25 (6.0) | |
| Physical activity in leisure | |||
| Low | 4144 (73.6) | 274 (66.2) | 0.005 |
| Moderate | 872 (15.5) | 84 (20.3) | |
| High | 618 (11.0) | 56 (13.5) | |
| Smoking | |||
| Never smoked | 2881 (50.4) | 204 (49.2) | 0.326 |
| Ex-smoker | 1882 (32.9) | 150 (36.1) | |
| Smoker | 953 (16.7) | 61 (14.7) | |
| Consumption of alcoholic beverages | |||
| Moderate | 5041 (88.2) | 352 (84.8) | 0.043 |
| Excessive | 676 (11.8) | 63 (15.2) | |
| Normal Median ± SD | HALP Median ± SD | p | |
|---|---|---|---|
| n (%) | 5717 (93.2) | 415 (6.8) | |
| Age (years) | 51.8 ± (8.9) | 54.0 ± (8.7) | <0.001 |
| BMI (Kg/m2) | 26.7 ± (4.4) | 24.5 ± (3.9) | <0.001 |
| Waist circumference (cm) | 91.8 ± (12.3) | 82.7 ± (10.5) | <0.001 |
| Kilocalories | 2933.1 ± (997.8) | 2671.4 ± (899.5) | <0.001 |
| Lipids | 94.3 ± (36.5) | 86.4 ± (34.7) | <0.001 |
| Carbohydrates | 374.6 ± (144.6) | 334.4 ± (125.5) | <0.001 |
| Proteins | 137.7 ± (53.1) | 130.7 ± (52.8) | 0.009 |
| Wine (mL/week) | 248.6 ± (418.1) | 283.9 ± (424.7) | 0.097 |
| Beer (mL/week) | 1380.8 ± (1736.7) | 1259.6 ± (1740.0) | 0.171 |
| spirits (mL/week) | 39.6 ± (116.6) | 49.7 ± (117.1) | 0.255 |
| Total alcohol (mL/week) | 1669.2 ± (1756.9) | 1593.4 ± (1784.9) | 0.397 |
| Total alcohol (g/week) | 91.5 ± (88.8) | 93.1 ± (103.0) | 0.722 |
| TC (mg/dL) | 218.9 ± (40.6) | 241.4 ± (40.3) | <0.001 |
| Triglycerides (mg/dL) | 145.0 ± (109.7) | 93.6 ± (67.8) | <0.001 |
| HDL-C (mg/dL) | 56.6 ± (10.6) | 93.4 ± (11.3) | <0.001 |
| LDL-C (mg/dL) | 134.3 ± (34.4) | 129.6 ± (36.3) | 0.007 |
| Normal | HALP | |||||
|---|---|---|---|---|---|---|
| n (%) | p | n (%) | p | |||
| Moderate | Excessive | Moderate | Excessive | |||
| 5041 (88.2) | 676 (11.8) | 352 (84.8) | 63 (15.2) | |||
| Sex | ||||||
| Male | 2825 (56.0) | 487 (72.0) | <0.001 | 70 (19.9) | 30 (47.6) | <0.001 |
| Female | 2216 (44.0) | 189 (28.0) | 282 (80.1) | 33 (52.4) | ||
| Income Tertile | ||||||
| 1 | 1669 (33.2) | 257 (38.0) | 0.023 | 84 (23.9) | 23 (36.5) | 0.108 |
| 2 | 1707 (33.9) | 200 (29.6) | 115 (32.8) | 18 (28.6) | ||
| 3 | 1655 (32.9) | 219 (32.4) | 152 (43.3) | 22 (34.9) | ||
| Education Level | ||||||
| Incomplete primary | 191 (3.8) | 45 (6.7) | <0.001 | 19 (5.4) | 1 (1.6) | 0.005 |
| Complete primary | 257 (5.1) | 48 (7.1) | 11 (3.1) | 7 (11.1) | ||
| High school complete | 1507 (29.9) | 215 (31.8) | 80 (22.7) | 20 (31.7) | ||
| University complete | 3086 (61.2) | 368 (54.4) | 242 (68.8) | 35 (55.6) | ||
| Marital Status | ||||||
| Married | 3453 (70.3) | 452 (66.9) | 0.007 | 187 (53.1) | 40 (63.5) | 0.332 |
| Separated/divorced | 784 (15.6) | 126 (18.6) | 70 (19.9) | 8 (12.7) | ||
| Single | 420 (8.3) | 47 (7.0) | 58 (16.5) | 10 (15.9) | ||
| Widower | 139 (2.8) | 16 (2.4) | 18 (5.1) | 1 (1.6) | ||
| Other (with previous union) | 155 (3.1) | 35 (5.2) | 18 (5.4) | 4 (6.3) | ||
| Ethnicity | ||||||
| Not white | 2069 (41.6) | 302 (45.6) | 0.047 | 139 (38.8) | 32 (52.5) | 0.065 |
| White | 2909 (58.4) | 360 (54.4) | 210 (60.2) | 29 (47.5) | ||
| lipid-lowering drugs | ||||||
| No | 4438 (88.0) | 599 (88.6) | 0.667 | 331 (94.0) | 59 (93.7) | 0.781 * |
| Yes | 603 (12.0) | 77 (11.4) | 21 (6.0) | 4 (6.3) | ||
| Body mass index | ||||||
| Thin | 35 (0.7) | 2 (0.3) | <0.001 | 7 (2.0) | 4 (6.3) | 0.051 |
| Normal | 1926 (38.2) | 182 (26.9) | 209 (59.4) | 28 (44.4) | ||
| Overweight | 2088 (41.4) | 323 (47.8) | 98 (27.8) | 24 (38.1) | ||
| Obesity | 990 (19.6) | 169 (25.0) | 38 (10.8) | 7 (11.1) | ||
| Physical activity in leisure | ||||||
| Low | 3627 (73.1) | 517 (77.3) | 229 (65.2) | 45.0 (71.4) | 0.12 | |
| Moderate | 781 (15.7) | 91 (13.6) | 0.063 | 77 (21.9) | 7.0 (11.1) | |
| High | 557 (11.2) | 61 (9.1) | 45 (12.8) | 11 (17.5) | ||
| Smoking | ||||||
| Never smoked | 2679 (53.2) | 202 (29.9) | <0.001 | 187 (53.1) | 17 (27.0) | <0.001 |
| Ex-smoker | 1604 (31.8) | 278 (41.1) | 122 (34.7) | 28 (44.4) | ||
| Smoker | 757 (15.0) | 196 (29.0) | 43 (12.2) | 18 (28.6) | ||
| Normal | HALP | |||||
|---|---|---|---|---|---|---|
| Median ± SD | p | Median ± SD | p | |||
| Moderate | Excessive | Moderate | Excessive | |||
| 5041 (88.2) | 676 (11.8) | 352 (84.8) | 63 (15.2) | |||
| Age (years) | 51.7 ± (9.0) | 52.6 (8.2) | 0.007 | 53.9 ± (8.9) | 54.8 ± (7.8) | 0.436 |
| Weight (Kg) | 74.6 ± (14.8) | 79.0 ± (14.4) | <0.001 | 63.9 ± (10.9) | 67.5 ± (13.6) | 0.023 |
| Height (Mts) | 166.9 ± (9.2) | 169.2 ± (8.6) | <0.001 | 161.5 ± (8.2) | 164.6 ± (8.0) | 0.006 |
| BMI (Kg/m2) | 26.9 ± (4.4) | 27.5 ± (4.2) | <0.001 | 24.5 ± (3.8) | 24.8 ± (4.4) | 0.542 |
| Waist circumference (cm) | 91.3 ± (12.2) | 95.9 ± (11.6) | <0.001 | 82.2 ± (10.3) | 85.8 ± (11.2) | 0.011 |
| Kilocalories | 2892.8 ± (981.6) | 3233.9 ± (1064.6) | <0.001 | 2633.1 ± (867.8) | 2885.3 ± (1041.1) | 0.04 |
| Lipids | 93.3 ± (35.9) | 102.0 ± (39.9) | <0.001 | 86.2 ± (34.0) | 87.5 ± (39.0) | 0.784 |
| Carbohydrates | 372.8 ± (143.4) | 387.7 ± (152.1) | 0.017 | 333.0 ± (122.7) | 342.1 ± (140.9) | 0.598 |
| Proteins | 136.5 ± (52.4) | 147.1 ± (57.1) | <0.001 | 129.6 ± (50.9) | 137.0 ± (62.7) | 0.304 |
| Wine (mL/week) | 210.0 ± (293.5) | 536.2 ± (862.1) | <0.001 | 243.9 ± (325.2) | 507.8 ± (738.9) | 0.007 |
| Beer (mL/week) | 972.6 ± (1029.8) | 4425.4 ± (2663.5) | <0.001 | 759.0 ± (885.7) | 4056.9 ± (2530.1) | <0.001 |
| Spirits (mL/week) | 22.6 ± (60.5) | 166.7 ± (263.6) | <0.001 | 23.0 ± (69.7) | 199.2 ± (393.9) | <0.001 |
| Total alcohol (mL/week) | 1205.3 ± (993.2) | 5128.3 ± (2276.5) | 0.017 | 1025.9 ± (854.4) | 4764.0 ± (2258.0) | <0.001 |
| Total alcohol (g/week) | 66.1 ± (47.0) | 281.0 ± (97.5) | <0.001 | 60.9 ± (44.4) | 273.1 ± (144.5) | <0.001 |
| TC (mg/dL) | 217.9 ± (40.1) | 226.4 ± (43.3) | <0.001 | 241.7 ± (40.1) | 239.6 ± (41.7) | 0.703 |
| Triglycerides (mg/dL) | 140.3 ± (102.4) | 180.0 ± (148.9) | <0.001 | 90.8 ± (41.4) | 109.4 ± (144.0) | 0.313 |
| HDL-C (mg/dL) | 56.4 ± (10.6) | 57.9 ± (11.0) | 0.001 | 93.5 ± (10.9) | 92.9 ± (13.5) | 0.66 |
| LDL-C (mg/dL) | 134.2 ± (34.3) | 134.9 ± (35.7) | 0.586 | 130.3 ± (36.9) | 125.5 ± (32.7) | 0.339 |
| OR Crude | OR Adjusted 1 * | OR Adjusted 2 ** | |
|---|---|---|---|
| OR CI 95% | OR CI 95% | OR CI 95% | |
| Moderate | 1 | 1 | 1 |
| Excessive | 1.33 (1.1–1.7) | 1.73 (1.2–2.3) | 1.92 (1.4–2.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enriquez-Martinez, O.G.; Silva Pereira, T.S.; Mill, J.G.; Fonseca, M.d.J.M.d.; Molina, M.d.C.B.; Griep, R.H. Excessive Consumption of Alcoholic Beverages and Extremely High Levels of High-Density Lipoprotein Cholesterol (HALP) in the ELSA-Brasil Cohort Baseline. Nutrients 2023, 15, 1221. https://0-doi-org.brum.beds.ac.uk/10.3390/nu15051221
Enriquez-Martinez OG, Silva Pereira TS, Mill JG, Fonseca MdJMd, Molina MdCB, Griep RH. Excessive Consumption of Alcoholic Beverages and Extremely High Levels of High-Density Lipoprotein Cholesterol (HALP) in the ELSA-Brasil Cohort Baseline. Nutrients. 2023; 15(5):1221. https://0-doi-org.brum.beds.ac.uk/10.3390/nu15051221
Chicago/Turabian StyleEnriquez-Martinez, Oscar Geovanny, Taísa Sabrina Silva Pereira, Jose Geraldo Mill, Maria de Jesus Mendes da Fonseca, Maria del Carmen Bisi Molina, and Rosane Harter Griep. 2023. "Excessive Consumption of Alcoholic Beverages and Extremely High Levels of High-Density Lipoprotein Cholesterol (HALP) in the ELSA-Brasil Cohort Baseline" Nutrients 15, no. 5: 1221. https://0-doi-org.brum.beds.ac.uk/10.3390/nu15051221