
Tolerance and Safety of an Anti-Regurgitation Formula Containing Locust Bean Gum, Pre-, and Postbiotics: A Multi-Country Multi-Center Prospective Randomized Controlled Study in Infants with Regurgitation
 , , , , , ,
, , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Subjects
2.3. Intervention
2.4. Outcome Measures
2.5. Statistical Analyses
3. Results
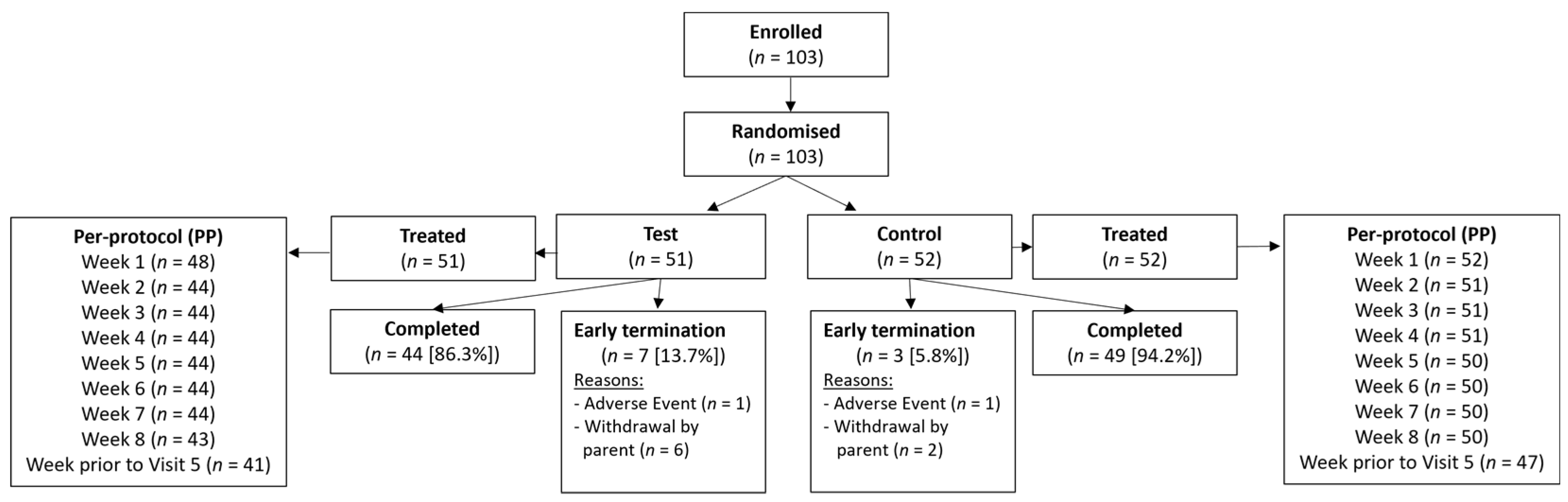
3.1. Subjects
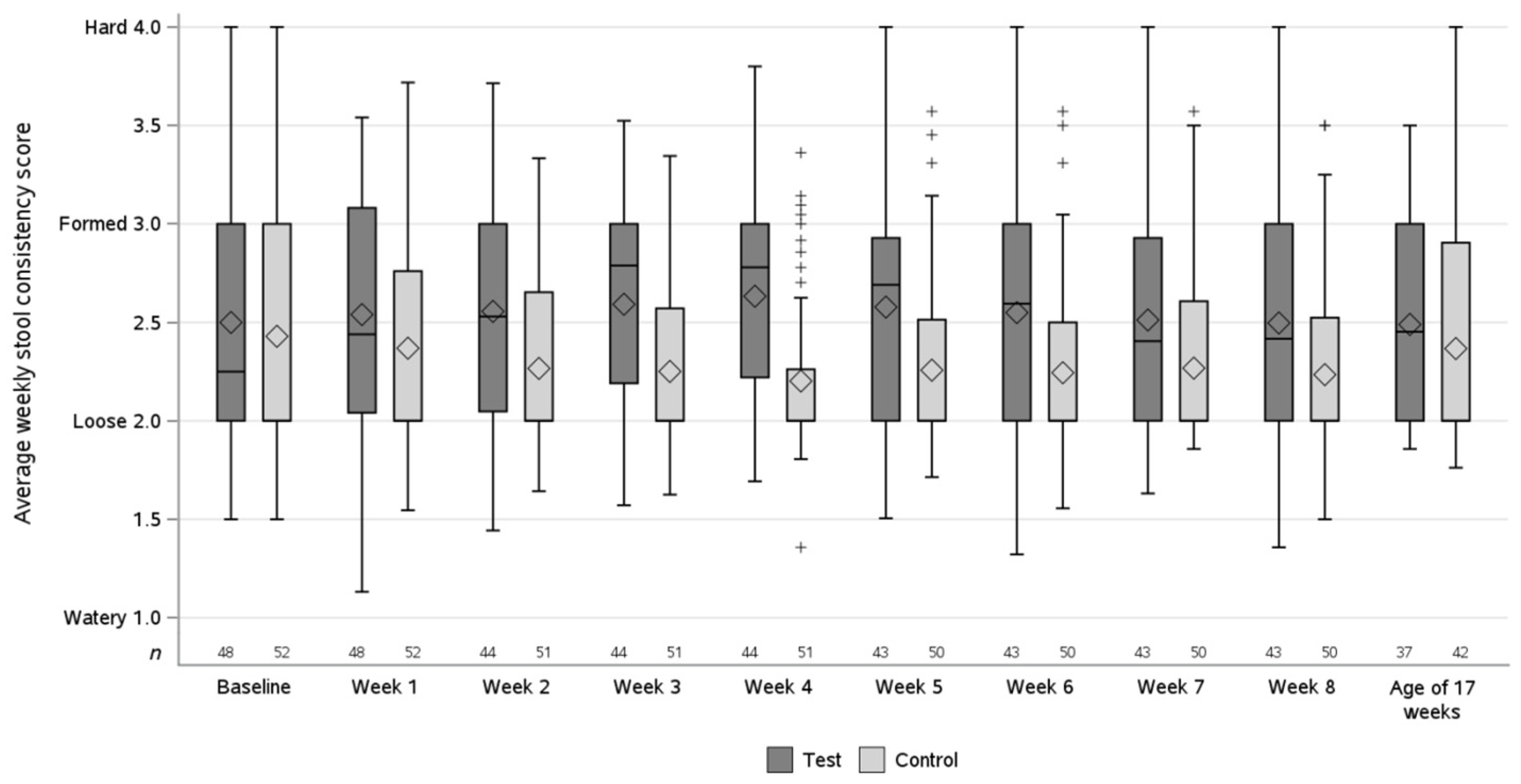
3.2. Primary Outcome Results
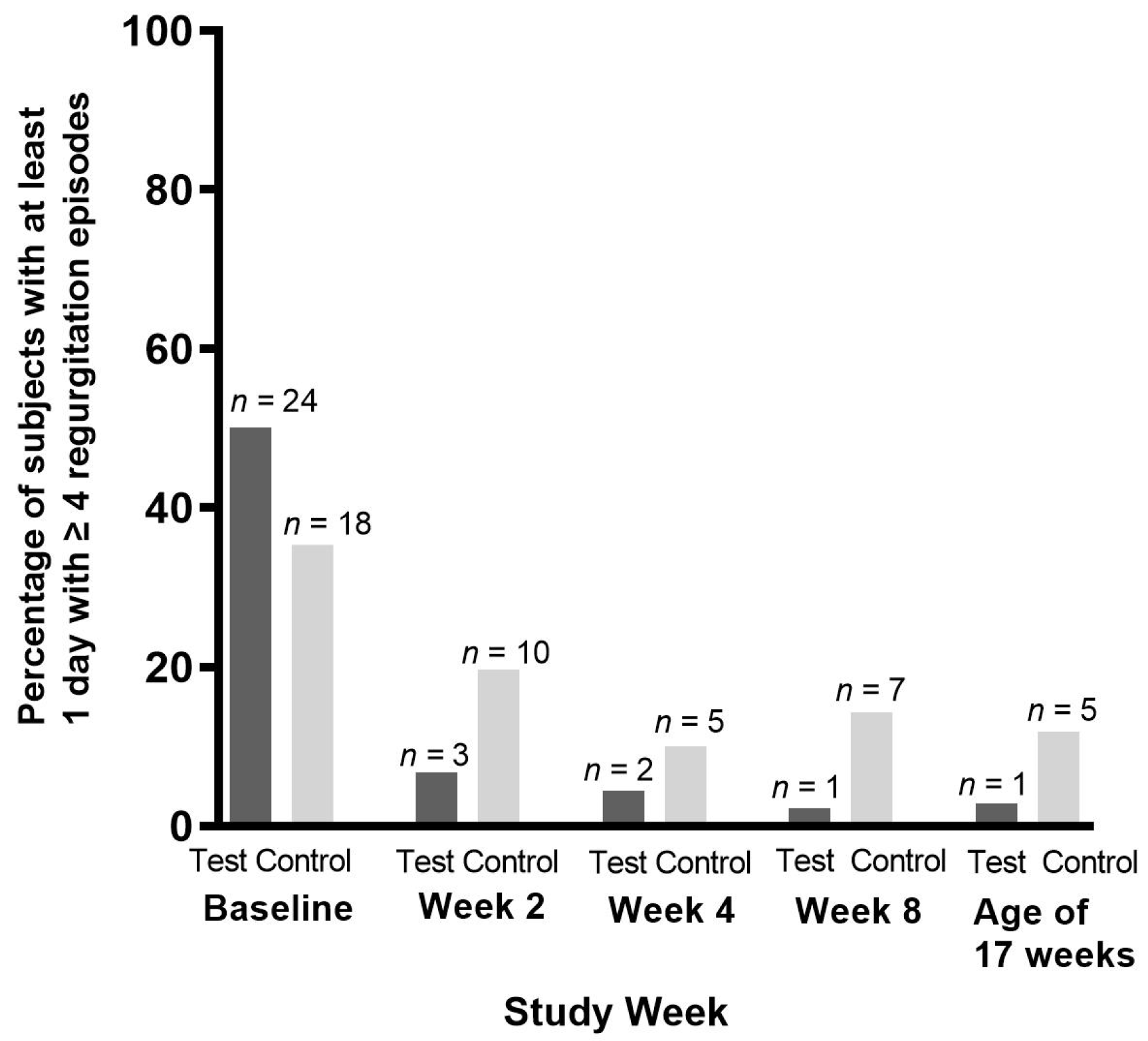
3.3. Secondary Outcome Results
3.4. Adverse Events and Concomitant Medication
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahon, J.; Lifschitz, C.; Ludwig, T.; Thapar, N.; Glanville, J.; Miqdady, M.; Saps, M.; Quak, S.H.; Wijnkoop, I.L.; Edwards, M.; et al. The costs of functional gastrointestinal disorders and related signs and symptoms in infants: A systematic literature review and cost calculation for England. BMJ Open 2017, 7, e015594. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, S.; Savino, F.; Singendonk, M.; Tabbers, M.; Benninga, M.A.; Staiano, A.; Vandenplas, Y. Thickened infant formula: What to know. Nutrition 2018, 49, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Muhardi, L.; Aw, M.M.; Hasosah, M.; Ng, R.T.; Chong, S.Y.; Hegar, B.; Toro-Monjaraz, E.; Darma, A.; Cetinkaya, M.; Chow, C.M.; et al. A Narrative Review on the Update in the Prevalence of Infantile Colic, Regurgitation, and Constipation in Young Children: Implications of the ROME IV Criteria. Front. Pediatr. 2021, 9, 778747. [Google Scholar] [CrossRef] [PubMed]
- Bellaiche, M.; Oozeer, R.; Gerardi-Temporel, G.; Faure, C.; Vandenplas, Y. Multiple functional gastrointestinal disorders are frequent in formula-fed infants and decrease their quality of life. Acta Paediatr. 2018, 107, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Benítez, C.A.; Collazos-Saa, L.I.; García-Perdomo, H.A. Functional Gastrointestinal Disorders in Neonates and Toddlers According to the Rome IV Criteria: A Systematic Review and Meta-Analysis. Pediatr. Gastroenterol. Hepatol. Nutr. 2022, 25, 376–386. [Google Scholar] [CrossRef]
- Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.P. Epidemiology of functional gastrointestinal disorders in infants and toddlers: A systematic review. World J. Gastroenterol. 2016, 22, 6547–6558. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, S.W.; Kwon, Y.; Ha, E.K.; An, J.; Cha, H.R.; Jeong, S.J.; Han, M.Y. Infantile Colic and the Subsequent Development of the Irritable Bowel Syndrome. J. Neurogastroenterol. Motil. 2022, 28, 618–629. [Google Scholar] [CrossRef]
- Lenglart, L.; Raieli, V.; Sciruicchio, V.; Caula, C.; Vitali, G.; Guedj, R.; Quatrosi, G.; D’agnano, D.; D’alonzo, R.; Moulding, T.; et al. The association between gastro-oesophageal reflux and migraine in the paediatric population: A multicentre case-control study. Eur. J. Pediatr. 2022, 181, 1679–1687. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.; Vandenplas, Y.; Singendonk, M.; Cabana, M.; DiLorenzo, C.; Gottrand, F.; Gupta, S.; Langendam, M.; Staiano, A.; Thapar, N.; et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 516–554. [Google Scholar] [CrossRef]
- Salvatore, S.; Abkari, A.; Cai, W.; Catto-Smith, A.; Cruchet, S.; Gottrand, F.; Hegar, B.; Lifschitz, C.; Ludwig, T.; Shah, N.; et al. Review shows that parental reassurance and nutritional advice help to optimise the management of functional gastrointestinal disorders in infants. Acta Paediatr. 2018, 107, 1512–1520. [Google Scholar] [CrossRef]
- Lightdale, J.R.; Gremse, D.A. Section on Gastroenterology, Hepatology and Nutrition Gastroesophageal reflux: Management guidance for the pediatrician. Pediatrics 2013, 131, e1684–e1695. [Google Scholar] [CrossRef] [PubMed]
- Puntis, J.W. Gastro-oesophageal reflux in young babies: Who should be treated? Arch. Dis. Child. 2015, 100, 989–993. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Hachimi-Idrissi, S.; Casteels, A.; Mahler, T.; Loeb, H. A clinical trial with an “anti-regurgitation” formula. Eur. J. Pediatr. 1994, 153, 419–423. [Google Scholar]
- Tounian, P.; Meunier, L.; Speijers, G.; Oozeer, R.; Vandenplas, Y. Effectiveness and tolerance of a locust bean gum thickened formula: A real-life study. Pediatr. Gastroenterol. Hepatol. Nutr. 2020, 23, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, R.; Tomomasa, T.; Kaneko, H.; Arakawa, H.; Morikawa, A. Effect of formula thickened with reduced concentration of locust bean gum on gastroesophageal reflux. Acta Paediatr. 2007, 96, 910–914. [Google Scholar] [CrossRef] [PubMed]
- Horvath, A.; Dziechciarz, P.; Szajewska, H. The effect of thickened-feed interventions on gastroesophageal reflux in infants: Systematic review and meta-analysis of randomized, controlled trials. Pediatrics 2008, 122, e1268–e1277. [Google Scholar] [CrossRef]
- Bellaiche, M.; Ludwig, T.; Arciszewska, M.; Bongers, A.; Gomes, C.; Świat, A.; Dakhlia, F.; Piollet, A.; Oozeer, R.; Vandenplas, Y. Safety and Tolerance of a Novel Anti-Regurgitation Formula: A Double-Blind, Randomised, Controlled Trial. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Bellaiche, M.; Tounian, P.; Oozeer, R.; Rocher, E.; Vandenplas, Y. Digestive Tolerance and Safety of an Anti-Regurgitation Formula Containing Locust Bean Gum, Prebiotics and Postbiotics: A Real-World Study. Pediatr. Gastroenterol. Hepatol. Nutr. 2023, 26, 249–265. [Google Scholar] [CrossRef]
- Meunier, L.; Garthoff, J.A.; Schaafsma, A.; Krul, L.; Schrijver, J.; van Goudoever, J.B.; Speijers, G.; Vandenplas, Y. Locust bean gum safety in neonates and young infants: An integrated review of the toxicological database and clinical evidence. Regul. Toxicol. Pharmacol. 2014, 70, 155–169. [Google Scholar] [CrossRef]
- EFSA Panel on Food Additives Nutrient Sources added to Food (ANS); Mortensen, A.; Aguilar, F.; Crebelli, R.; Di Domenico, A.; Frutos, M.J.; Galtier, P.; Gott, D.; Gundert-Remy, U.; Lambré, C.; et al. Re-evaluation of locust bean gum (E410) as food additive. EFSA J. 2017, 15, 4646. [Google Scholar]
- Benninga, M.A.; Nurko, S.; Faure, C.; Hyman, P.E.; Roberts, I.S.J.; Schechter, N.L. Childhood Functional Gastrointestinal Disorders: Neonate/Toddler. Gastroenterology 2016, 150, 1443–1455. [Google Scholar] [CrossRef] [PubMed]
- Zeevenhooven, J.; Koppen, I.J.N.; Benninga, M.A. The New Rome IV Criteria for Functional Gastrointestinal Disorders in Infants and Toddlers. Pediatr. Gastroenterol. Hepatol. Nutr. 2017, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ismail, L.C.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; Szajewska, H.; Benninga, M.; Di Lorenzo, C.; Dupont, C.; Faure, C.; Miqdadi, M.; Osatakul, S.; Ribes-Konickx, C.; Saps, M.; et al. Development of the Brussels Infant and Toddler Stool Scale (‘BITSS’): Protocol of the study. BMJ Open 2017, 7, e014620. [Google Scholar] [CrossRef] [PubMed]
- Huysentruyt, K.; Koppen, I.; Benninga, M.; Cattaert, T.; Cheng, J.; De Geyter, C.; Faure, C.; Gottrand, F.; Hegar, B.; Hojsak, I.; et al. The Brussels Infant and Toddler Stool Scale: A Study on Interobserver Reliability. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Riley, A.W.; Trabulsi, J.; Yao, M.; Bevans, K.B.; DeRusso, P.A. Validation of a Parent Report Questionnaire: The Infant Gastrointestinal Symptom Questionnaire. Clin. Pediatr. 2015, 54, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Gosho, M.; Maruo, K. Effect of heteroscedasticity between treatment groups on mixed-effects models for repeated measures. Pharm. Stat. 2018, 17, 578–592. [Google Scholar] [CrossRef]
- Training Course on Child Growth Assessment; WHO: Geneva, Switzerland, 2008; Available online: https://apps.who.int/iris/bitstream/handle/10665/43601/9789241595070_C_eng.pdf?sequence=3&isAllowed=y (accessed on 26 September 2023).
- Moro, G.; Minoli, I.; Mosca, M.; Fanaro, S.; Jelinek, J.; Stahl, B.; Boehm, G. Dosage-related bifidogenic effects of galacto- and fructooligosaccharides in formula-fed term infants. J. Pediatr. Gastroenterol. Nutr. 2002, 34, 291–295. [Google Scholar]
- Rodriguez-Herrera, A.; Mulder, K.; Bouritius, H.; Rubio, R.; Muñoz, A.; Agosti, M.; Lista, G.; Corvaglia, L.; Ludwig, T.; Abrahamse-Berkeveld, M.; et al. Gastrointestinal Tolerance, Growth and Safety of a Partly Fermented Formula with Specific Prebiotics in Healthy Infants: A Double-Blind, Randomized, Controlled Trial. Nutrients 2019, 11, 1530. [Google Scholar] [CrossRef]
- Parschat, K.; Melsaether, C.; Jäpelt, K.R.; Jennewein, S. Clinical Evaluation of 16-Week Supplementation with 5HMO-Mix in Healthy-Term Human Infants to Determine Tolerability, Safety, and Effect on Growth. Nutrients 2021, 13, 2871. [Google Scholar] [CrossRef]
- Scholtens, P.A.; Goossens, D.A.; Staiano, A. Stool characteristics of infants receiving short-chain galacto-oligosaccharides and long-chain fructo-oligosaccharides: A review. World J. Gastroenterol. 2014, 20, 13446–13452. [Google Scholar] [CrossRef]
- Storm, H.M.; Shepard, J.; Czerkies, L.M.; Kineman, B.; Cohen, S.S.; Reichert, H.; Carvalho, R. 2′-Fucosyllactose Is Well Tolerated in a 100% Whey, Partially Hydrolyzed Infant Formula with Bifidobacterium lactis: A Randomized Controlled Trial. Glob. Pediatr. Health 2019, 6, 1–10. [Google Scholar] [CrossRef]
- Vivatvakin, B.; Volger, S.; Sintusek, P.; Leewiboonsilp, W.; Lebumfacil, J.; Northington, R. Clinical characteristics of Thai infants experiencing minor gastrointestional discomfort. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 346. [Google Scholar]
- Yao, M.; Lien, E.L.; Capeding, M.R.Z.; Fitzgerald, M.; Ramanujam, K.; Yuhas, R.; Northington, R.; Lebumfacil, J.; Wang, L.; DeRusso, P.A. Effects of Term Infant Formulas Containing High sn-2 Palmitate with and without Oligofructose on Stool Composition, Stool Characteristics, and Bifidogenicity. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 440–448. [Google Scholar] [CrossRef]
- Mao, M.; Zhang, L.; Ge, J.; Yan, J.; Northington, R.; Yao, M.; Nowacki, J.; Hays, N.P. Infant Feeding Regimens and Gastrointestinal Tolerance: A Multicenter, Prospective, Observational Cohort Study in China. Glob. Pediatr. Health 2018, 5, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nowacki, J.; Lee, H.-C.; Lien, R.; Cheng, S.-W.; Li, S.-T.; Yao, M.; Northington, R.; Jan, I.; Mutungi, G. Stool fatty acid soaps, stool consistency and gastrointestinal tolerance in term infants fed infant formulas containing high sn-2 palmitate with or without oligofructose: A double-blind, randomized clinical trial. Nutr. J. 2014, 13, 105. [Google Scholar] [CrossRef] [PubMed]
- Wegh, C.A.M.; Geerlings, S.Y.; Knol, J.; Roeselers, G.; Belzer, C. Postbiotics and Their Potential Applications in Early Life Nutrition and Beyond. Int. J. Mol. Sci. 2019, 20, 4673. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, V.; Indrio, F.; Verduci, E.; Calcaterra, V.; Pop, T.L.; Mari, A.; Zuccotti, G.V.; Cokugras, F.C.; Pettoello-Mantovani, M.; Goulet, O. Term Infant Formulas Influencing Gut Microbiota: An Overview. Nutrients 2021, 13, 4200. [Google Scholar] [CrossRef] [PubMed]
- Chao, H.C.; Vandenplas, Y. Effect of cereal-thickened formula and upright positioning on regurgitation, gastric emptying, and weight gain in infants with regurgitation. Nutrition 2007, 23, 23–28. [Google Scholar] [CrossRef]
- Hegar, B.; Boediarso, A.; Firmansyah, A.; Vandenplas, Y. Investigation of regurgitation and other symptoms of gastroesophageal reflux in Indonesian infants. World J. Gastroenterol. 2004, 10, 1795–1797. [Google Scholar] [CrossRef]
- Nelson, S.P.; Chen, E.H.; Syniar, G.M.; Christoffel, K.K. Prevalence of symptoms of gastroesophageal reflux during infancy. A pediatric practice-based survey. Arch. Pediatr. Adolesc. Med. 1997, 151, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Hua, S.; Peters, R.L.; Allen, K.J.; Dharmage, S.C.; Tang, M.L.; Wake, M.; Foskey, R.; Heine, R.G.; HealthNuts Study Investigators. Medical intervention in parent-reported infant gastro-oesophageal reflux: A population-based study. J. Paediatr. Child. Health 2015, 51, 515–523. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvatore, S.; Klymenko, V.; Karpushenko, Y.; Durczak-Hilleman, M.; Loboda, A.; Petrashenko, V.; Olechowski, W.; Lista, G.; Meneghin, F.; Amodio, S.; et al. Tolerance and Safety of an Anti-Regurgitation Formula Containing Locust Bean Gum, Pre-, and Postbiotics: A Multi-Country Multi-Center Prospective Randomized Controlled Study in Infants with Regurgitation. Nutrients 2024, 16, 899. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16060899
Salvatore S, Klymenko V, Karpushenko Y, Durczak-Hilleman M, Loboda A, Petrashenko V, Olechowski W, Lista G, Meneghin F, Amodio S, et al. Tolerance and Safety of an Anti-Regurgitation Formula Containing Locust Bean Gum, Pre-, and Postbiotics: A Multi-Country Multi-Center Prospective Randomized Controlled Study in Infants with Regurgitation. Nutrients. 2024; 16(6):899. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16060899
Chicago/Turabian StyleSalvatore, Silvia, Viktoriia Klymenko, Yuliia Karpushenko, Maria Durczak-Hilleman, Andrii Loboda, Viktoriia Petrashenko, Wiesław Olechowski, Gianluca Lista, Fabio Meneghin, Sonia Amodio, and et al. 2024. "Tolerance and Safety of an Anti-Regurgitation Formula Containing Locust Bean Gum, Pre-, and Postbiotics: A Multi-Country Multi-Center Prospective Randomized Controlled Study in Infants with Regurgitation" Nutrients 16, no. 6: 899. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16060899