Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources


Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Calculation of Dietary Protein Intake
2.3. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| Subject Characteristics | Community-Dwelling Elderly (n = 739) | Frail Elderly (n = 321) | Institutionalized Elderly (n = 219) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age (year) | 77.2 | 5.2 | 78.5 | 6.5 | 80.2 | 7.7 |
| Women | 77.6 | 5.4 | 77.9 | 6.1 | 81.2 | 7.9 |
| Men | 76.7 | 5.0 | 79.8 | 7.1 | 78.8 | 7.1 |
| Sex, women % | 50 | - | 45 | - | 62 | - |
| Weight (kg) | 77.2 | 12.4 | 70.1 | 12.4 | 72.0 | 18.3 |
| Women | 71.6 | 11.3 | 66.9 | 11.6 | 71.5 | 17.3 |
| Men | 82.7 | 10.9 | 77.2 | 11.2 | 72.8 | 20.0 |
| Height (m) | 1.67 | 0.09 | 1.65 | 0.09 | 1.62 | 0.11 |
| Women | 1.61 | 0.06 | 1.61 | 0.06 | 1.57 | 0.09 |
| Men | 1.74 | 0.06 | 1.73 | 0.07 | 1.69 | 0.09 |
| BMI (kg/m2) | 27.4 | 3.8 | 25.7 | 3.8 | 27.9 | 5.7 |
| Women | 27.6 | 4.3 | 25.7 | 4.0 | 28.8 | 6.3 |
| Men | 27.2 | 3.2 | 25.5 | 3.1 | 26.2 | 4.0 |
| Nutritional intake | ||||||
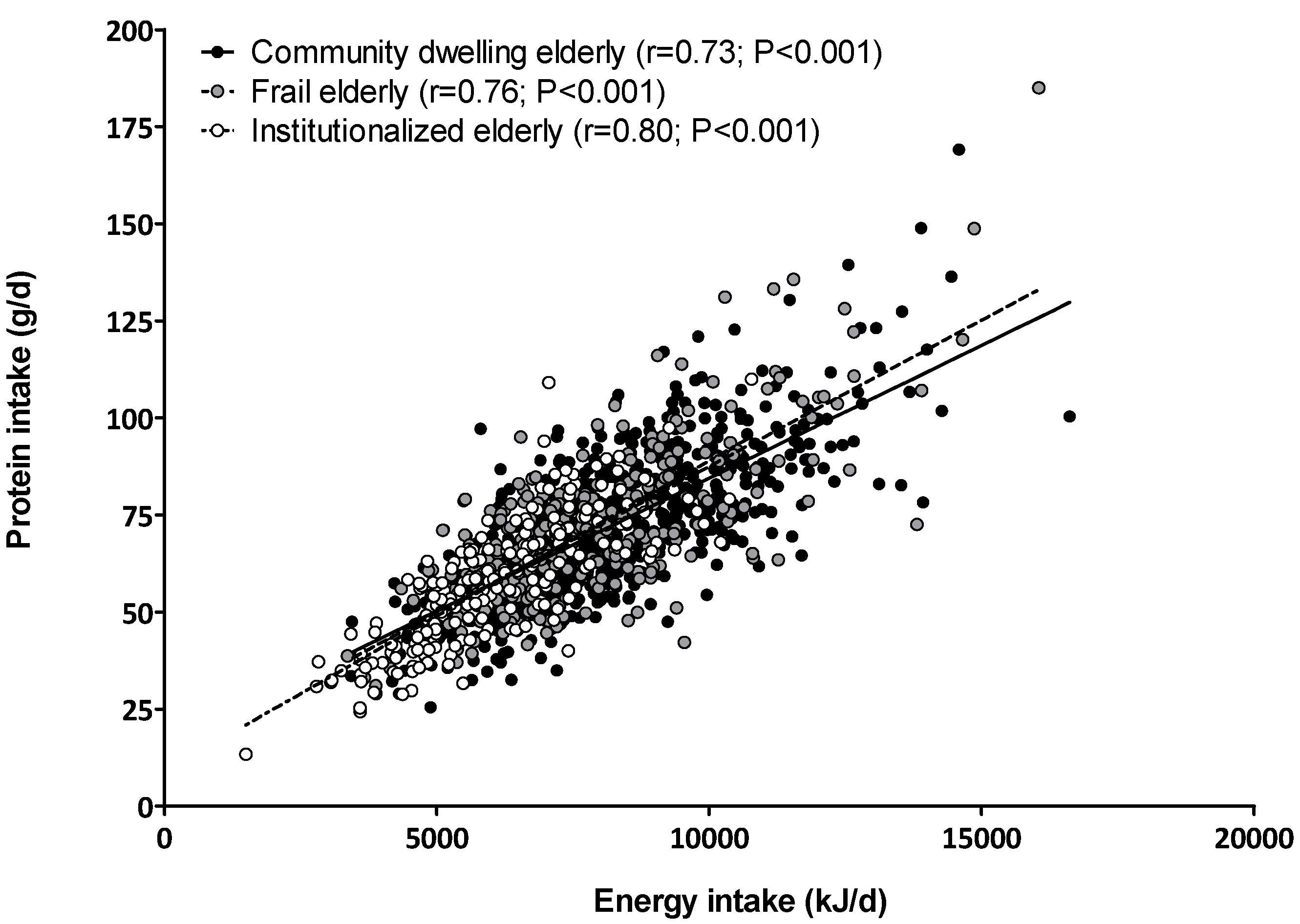
| Energy intake (kJ/day) | 8089 | 1944 | 7749 | 2010 | 6148 | 1635 |
| Women | 7230 | 1646 | 7178 | 1654 | 5943 | 1604 |
| Men | 8932 | 1844 | 8992 | 2159 | 6471 | 1640 |
| Protein intake (g/day) | 71 | 18 | 71 | 20 | 58 | 16 |
| Women | 65 | 16 | 66 | 16 | 55 | 15 |
| Men | 78 | 18 | 80 | 24 | 63 | 18 |
| Protein intake (en%) | 15 | 3 | 16 | 3 | 16 | 3 |
| Women | 15 | 3 | 16 | 3 | 16 | 3 |
| Men | 15 | 3 | 15 | 3 | 16 | 3 |
| Protein intake (g/kg-bw/day) | 0.9 | 0.3 | 1.0 | 0.3 | 0.8 | 0.3 |
| Women | 0.9 | 0.3 | 1.0 | 0.3 | 0.8 | 0.3 |
| Men | 0.9 | 0.2 | 1.0 | 0.3 | 0.9 | 0.3 |
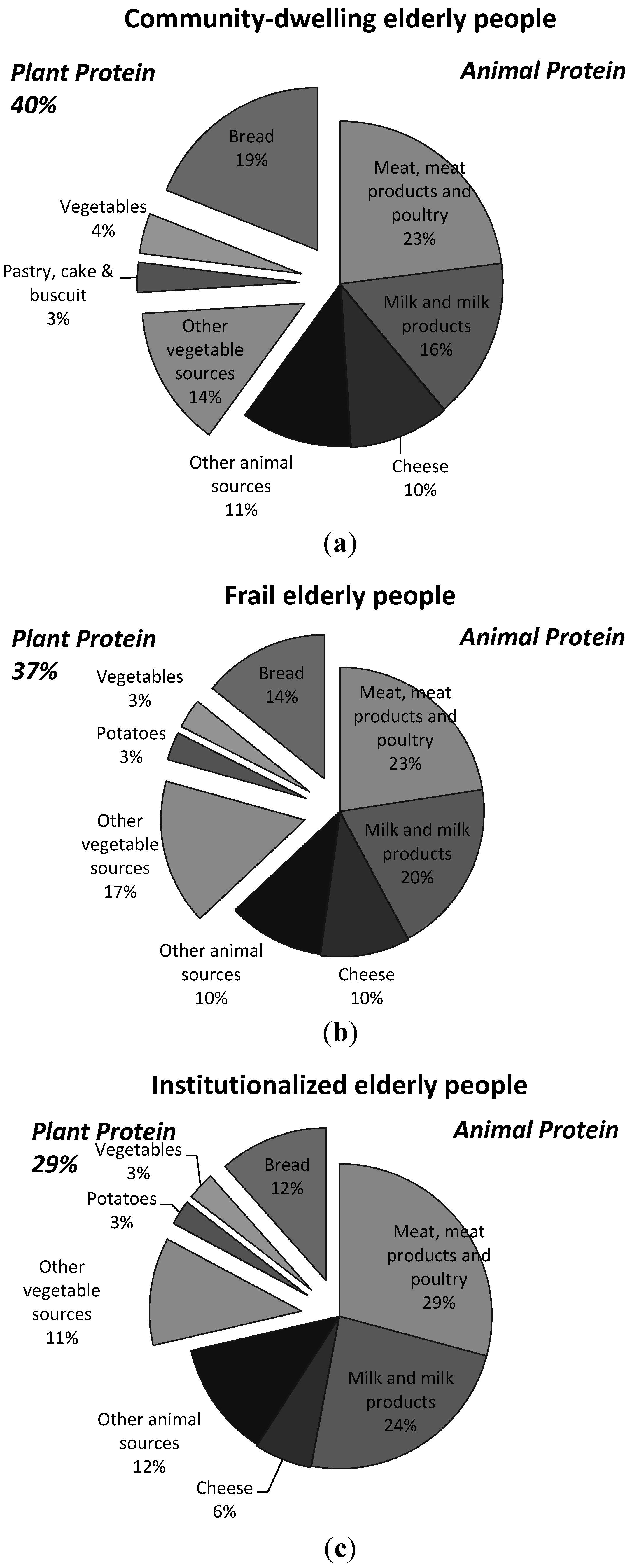
| Plant protein (g) | 28 | 9 | 25 | 7 | 16 | 6 |
| Women | 25 | 7 | 23 | 6 | 15 | 5 |
| Men | 30 | 9 | 29 | 9 | 17 | 6 |
| Plant protein (%) | 40 | 10 | 37 | 9 | 28 | 8 |
| Women | 40 | 10 | 37 | 9 | 28 | 9 |
| Men | 40 | 9 | 37 | 9 | 29 | 8 |
| Animal protein (g) | 44 | 14 | 46 | 17 | 42 | 14 |
| Women | 40 | 13 | 43 | 14 | 40 | 12 |
| Men | 47 | 14 | 52 | 20 | 45 | 16 |
| Animal protein (%) | 60 | 10 | 63 | 9 | 71 | 9 |
| Women | 60 | 10 | 63 | 9 | 72 | 8 |
| Men | 60 | 9 | 63 | 9 | 70 | 10 |

| Protein Intake | Breakfast | Morning Snack | Lunch | Afternoon Snack | Dinner | Evening Snack | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD | Frail | INST | CD | Frail | INST | CD | Frail | INST | CD | Frail | INST | CD | Frail | INST | CD | Frail | INST | |
| Protein intake (g/day) | 11 (7) | 10 (7) | 12 (7) | 3 (4) | 3 (4) | 2 (3) | 22 (13) | 18 (10) | 15 (8) | 4 (6) | 4 (6) | 3 (4) | 27 (13) | 31 (15) | 24 (12) | 5 (6) | 5 (7) | 2 (4) |
| Protein intake (% of total protein intake) | 16% | 14% | 21% | 4% | 5% | 3% | 31% | 26% | 25% | 5% | 5% | 6% | 38% | 43% | 41% | 7% | 7% | 4% |
| Plant-based protein (g/day) | 6 (4) | 5 (3) | 4 (2) | 1 (2) | 1 (2) | 1 (2) | 8 (4) | 7 (4) | 5 (3) | 2 (2) | 2 (3) | 1 (1) | 8 (5) | 8 (4) | 5 (3) | 2 (3) | 2 (3) | 1 (1) |
| Animal protein (g/day) | 5 (5) | 5 (6) | 8 (6) | 1 (2) | 2 (3) | 1 (2) | 14 (11) | 11 (9) | 10 (7) | 2 (5) | 2 (5) | 2 (4) | 19 (13) | 23 (14) | 19 (11) | 3 (5) | 3 (5) | 1 (3) |
| Breakfast | Morning Snack | Lunch | Afternoon Snack | Dinner | Evening Snack | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD | Frail | INST | CD | Frail | INST | CD | Frail | INST | CD | Frail | INST | CD | Frail | INST | CD | Frail | INST |
| Bread (44%) | Bread (38%) | Milk and milk products (40%) | Milk and milk products (29%) | Milk and milk products (49%) | Milk and milk products (50%) | Meat, meat products and poultry (25%) | Bread (30%) | Milk and milk products (31%) | Pastry, cake and biscuits (19%) | Milk and milk products (27%) | Milk and milk products (38%) | Meat, meat products and poultry (36%) | Meat, meat products and poultry (44%) | Meat, meat products and poultry (44%) | Milk and milk products (30%) | Milk and milk products (37%) | Milk and milk products (53%) |
| Cheese (18%) | Milk and milk products (21%) | Bread (25%) | Pastry, cake and biscuits (28%) | Pastry, cake and biscuits (24%) | Pastry, cake and biscuits (18%) | Bread (23%) | Milk and milk products (21%) | Bread (26%) | Milk and milk products (17.%) | Pastry, cake and biscuits (21%) | Foods for specific dietetic use (21%) | Milk and milk products (12%) | Milk and milk products (12%) | Milk and milk products (20%) | Cheese (14%) | Pastry, cake and biscuits (13%) | Beverages (13%) |
| Milk and milk products (17%) | Cheese (20%) | Cheese (14%) | Beverages (17%) | Beverages (10%) | Beverages (13%) | Milk and milk products (16%) | Cheese (20%) | Meat, meat products and poultry (16%) | Cheese (10%) | Nuts, seeds and snacks (14%) | Pastry, cake and biscuits (13%) | Bread (11%) | Fish (9%) | Vegetables (7%) | Pastry, cake and biscuits (13%) | Nuts, seeds and snacks (12%) | Pastry, cake and biscuits (13%) |
| Meat, meat products and poultry (5%) | Eggs (4%) | Meat, meat products and poultry (9%) | Bread (9%) | Nuts, seeds and snacks (5%) | Foods for specific dietetic use (10%) | Cheese (11%) | Meat, meat products and poultry (11%) | Cheese (13%) | Nuts, seeds and snacks (10%) | Cheese (7%) | Beverages (8%) | Fish (10%) | Potatoes (8%) | Potatoes (7%) | Nuts, seeds and snacks (12%) | Cheese (10%) | Foods for specific dietetic use (12%) |
| Eggs (4%) | Cereal products (4%) | Eggs (5%) | Cheese (5%) | Fruit (3%) | Sugar, sweet fillings and sweet sauces (6%) | Fish (7%) | Fish (5%) | Soups (4%) | Beverages (9%) | Beverages (6%) | Fruit (7%) | Cheese (6%) | Vegetables (7%) | Fish (6%) | Beverages (8%) | Beverages (6%) | Fish (3%) |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Koopman, R.; van Loon, L.J. Aging, exercise and muscle protein metabolism. J. Appl. Physiol. 2009, 106, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Czerwinski, S.; Abellan-Van-Kan, G.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Bohe, J.; Low, A.; Wolfe, R.R.; Rennie, M.J. Human muscle protein synthesis is modulated by extracellular, not intramuscular amino acid availability: A dose-response study. J. Physiol. 2003, 552, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, C.S.; Chinkes, D.L.; Paddon-Jones, D.; Zhang, X.J.; Aarsland, A.; Wolfe, R.R. Whey protein ingestion in elderly persons results in greater muscle protein accrual than ingestion of its constituent essential amino acid content. Nutr. Res. 2008, 28, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Pennings, B.; Boirie, Y.; Senden, J.M.; Gijsen, A.P.; Kuipers, H.; van Loon, L.J. Whey protein stimulates postprandial muscle protein accretion more effectively than do casein and casein hydrolysate in older men. Am. J. Clin. Nutr. 2011, 93, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Koopman, R.; Verdijk, L.; Manders, R.J.; Gijsen, A.P.; Gorselink, M.; Pijpers, E.; Wagenmakers, A.J.; van Loon, L.J. Co-ingestion of protein and leucine stimulates muscle protein synthesis rates to the same extent in young and elderly lean men. Am. J. Clin. Nutr. 2006, 84, 623–632. [Google Scholar] [PubMed]
- Paddon-Jones, D.; Sheffield-Moore, M.; Katsanos, C.S.; Zhang, X.J.; Wolfe, R.R. Differential stimulation of muscle protein synthesis in elderly humans following isocaloric ingestion of amino acids or whey protein. Exp. Gerontol. 2006, 41, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.M.; Tang, J.E.; Moore, D.R. The role of milk- and soy-based protein in support of muscle protein synthesis and muscle protein accretion in young and elderly persons. J. Am. Coll. Nutr. 2009, 28, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Rennie, M.J.; Tipton, K.D. Protein and amino acid metabolism during and after exercise and the effects of nutrition. Annu. Rev. Nutr. 2000, 20, 457–483. [Google Scholar] [CrossRef] [PubMed]
- Tipton, K.D.; Rasmussen, B.B.; Miller, S.L.; Wolf, S.E.; Owens-Stovall, S.K.; Petrini, B.E.; Wolfe, R.R. Timing of amino acid-carbohydrate ingestion alters anabolic response of muscle to resistance exercise. Am. J. Physiol. Endocrinol. Metab. 2001, 281, E197–E206. [Google Scholar] [PubMed]
- Katsanos, C.S.; Kobayashi, H.; Sheffield-Moore, M.; Aarsland, A.; Wolfe, R.R. Aging is associated with diminished accretion of muscle proteins after the ingestion of a small bolus of essential amino acids. Am. J. Clin. Nutr. 2005, 82, 1065–1073. [Google Scholar] [PubMed]
- Cuthbertson, D.; Smith, K.; Babraj, J.; Leese, G.; Waddell, T.; Atherton, P.; Wackerhage, H.; Taylor, P.M.; Rennie, M.J. Anabolic signaling deficits underlie amino acid resistance of wasting, aging muscle. FASEB J. 2005, 19, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Gorissen, S.H.; Remond, D.; van Loon, L.J. The muscle protein synthetic response to food ingestion. Meat Sci. 2015, 109, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Van Rossum, C.T.M.; Fransen, H.P.; Verkaik-Kloosterman, J.; Buurma-Rethans, E.J.M.; Ocke, M.C. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years; National Institute for Public Health and the Environment (RIVM): Bilthoven, The Netherlands, 2011. [Google Scholar]
- Tieland, M.; Dirks, M.L.; van der Zwaluw, N.; Verdijk, L.B.; van de Rest, O.; de Groot, L.C.P.G.M.; van Loon, L.J.C. Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.; de Groot, L.C. Protein supplementation improves physical performance in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Paw, M.J.M.C.A.; Jong, N.D.; Schouten, E.G.; Staveren, W.A.V.; Kok, F.J. Physical exercise or micronutrient supplementation for the wellbeing of the frail elderly? A randomised controlled trial. Br. J. Sports Med. 2002, 36, 126–131. [Google Scholar] [CrossRef]
- Chin, A.P.M.J.; de Groot, L.C.; van Gend, S.V.; Schoterman, M.H.; Schouten, E.G.; Schroll, M.; van Staveren, W.A. Inactivity and weight loss: Effective criteria to identify frailty. J. Nutr. Health Aging 2003, 7, 55–60. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Nijs, K.A.; Graaf, C.D.; Siebelink, E.; Blauw, Y.H.; Vanneste, V.; Kok, F.J.; van Staveren, W.A. Effect of family-style meals on energy intake and risk of malnutrition in Dutch nursing home Residents: A randomized controlled trial. J. Gerontol. 2006, 61A, 935–942. [Google Scholar] [CrossRef]
- Paddon-Jones, D.; Campbell, W.W.; Jacques, P.F.; Kritchevsky, S.B.; Moore, L.L.; Rodriguez, N.R.; van Loon, L.J. Protein and healthy aging. Am. J. Clin. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; Food and Agriculture Organization of the United Nations; United Nations University. Protein and Amino Acid Requirements in Human Nutrition; Report of a Joint FAO/WHO/UNU Expert Consultation (WHO Technical Report Series 935); WHO: Geneva, Switserland, 2007. [Google Scholar]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.R.; Miller, S.L.; Miller, K.B. Optimal protein intake in the elderly. Clin. Nutr. 2008, 27, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Mamerow, M.M.; Mettler, J.A.; English, K.L.; Casperson, S.L.; Arentson-Lantz, E.; Sheffield-Moore, M.; Layman, D.K.; Paddon-Jones, D. Dietary protein distribution positively influences 24-h muscle protein synthesis in healthy adults. J. Nutr. 2014, 144, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Areta, J.L.; Burke, L.M.; Ross, M.L.; Camera, D.M.; West, D.W.; Broad, E.M.; Jeacocke, N.A.; Moore, D.R.; Stellingwerff, T.; Phillips, S.M.; et al. Timing and distribution of protein ingestion during prolonged recovery from resistance exercise alters myofibrillar protein synthesis. J. Physiol. 2013, 591, 2319–2331. [Google Scholar] [CrossRef] [PubMed]
- Schaafsma, G. The protein digestibility-corrected amino acid score (PDCAAS)—A concept for describing protein quality in foods and food ingredients: A critical review. J. AOAC Int. 2005, 88, 988–994. [Google Scholar] [PubMed]
- Van Vliet, S.; Burd, N.A.; van Loon, L.J. The skeletal muscle anabolic response to plant- versus animal-based protein consumption. J. Nutr. 2015, 145, 1981–1991. [Google Scholar] [CrossRef] [PubMed]
- Schaafsma, G. The protein digestibility-corrected amino acid score. J. Nutr. 2000, 130, 1865S–1867S. [Google Scholar] [PubMed]
- Norton, L.E.; Wilson, G.J.; Layman, D.K.; Moulton, C.J.; Garlick, P.J. Leucine content of dietary proteins is a determinant of postprandial skeletal muscle protein synthesis in adult rats. Nutr. Metab. 2012, 9, 67. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tieland, M.; Borgonjen-Van den Berg, K.J.; Van Loon, L.J.C.; De Groot, L.C.P.G.M. Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources. Nutrients 2015, 7, 9697-9706. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7125496
Tieland M, Borgonjen-Van den Berg KJ, Van Loon LJC, De Groot LCPGM. Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources. Nutrients. 2015; 7(12):9697-9706. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7125496
Chicago/Turabian StyleTieland, Michael, Karin J. Borgonjen-Van den Berg, Luc J. C. Van Loon, and Lisette C. P. G. M. De Groot. 2015. "Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources" Nutrients 7, no. 12: 9697-9706. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7125496