Nutrient Patterns and Their Association with Socio-Demographic, Lifestyle Factors and Obesity Risk in Rural South African Adolescents

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Ethical Approval
2.3. Measurement of Diet, Lifestyle Factors, Anthropometric Indicators and Socio-Demographic Information
2.4. Data Analysis


3. Results
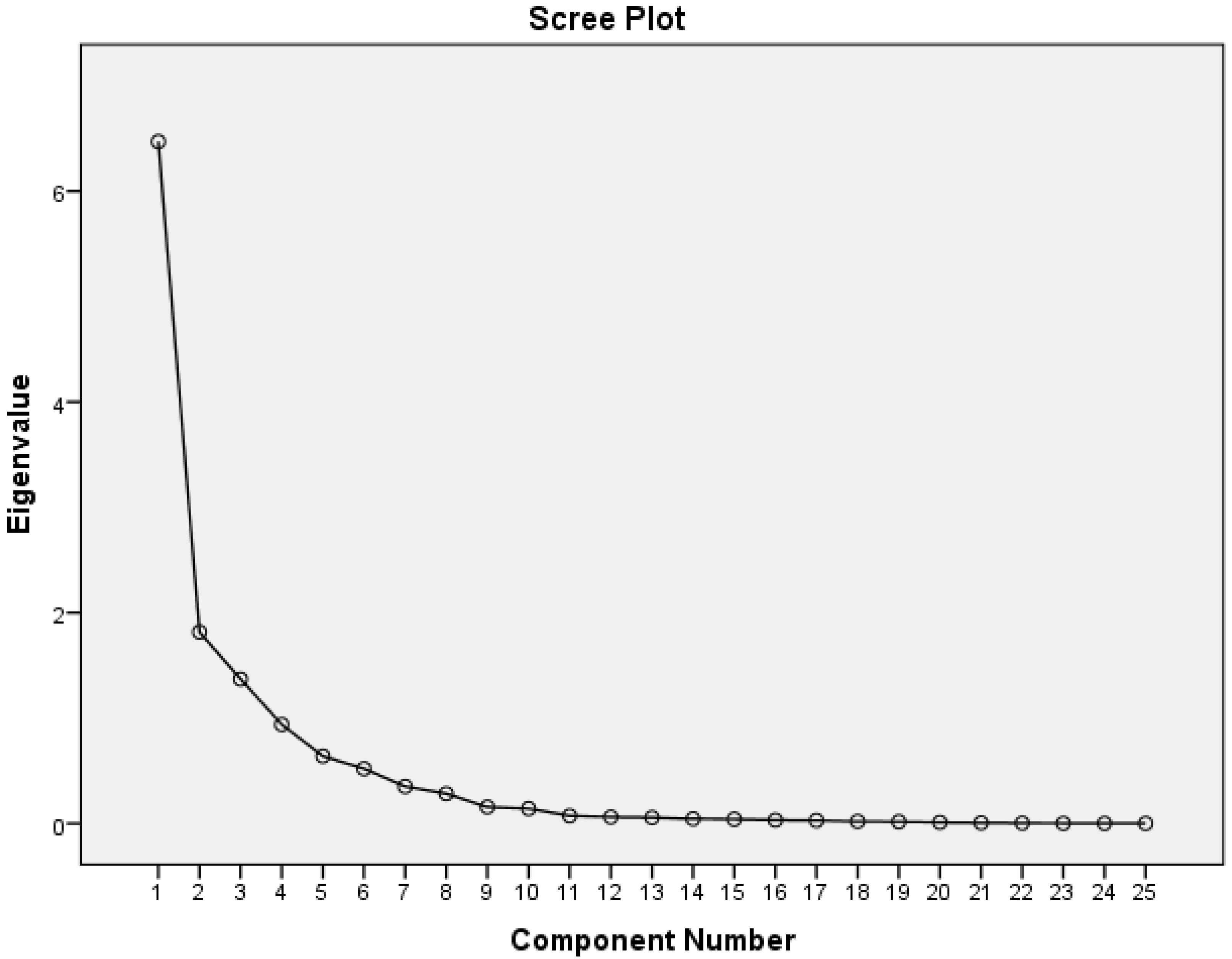
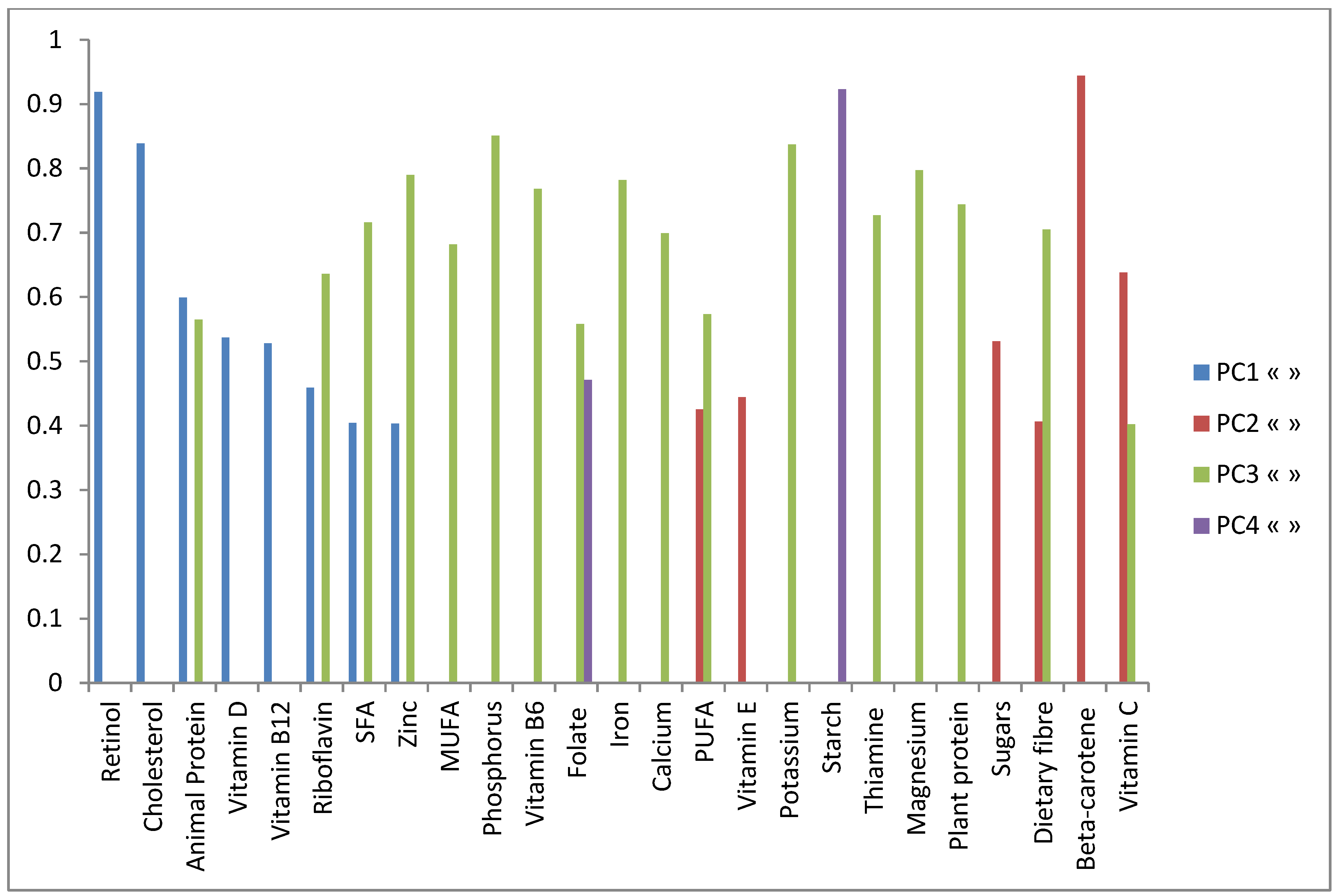
3.1. Identification and Description of Depicted Nutrient Patterns (PC)

{kind=link}
{kind=link}
| Nutrients | PC1 (Animal Driven Nutrients) | PC2 (Vitamins, Fibre and Vegetable Oil Nutrients) | PC3 (Mixed Diet Driven Nutrients) | PC4 (Starch and Folate Driven) |
|---|---|---|---|---|
| Animal Protein | 0.599 | −0.032 | 0.565 | −0.019 |
| Plant protein | 0.127 | 0.255 | 0.744 | 0.249 |
| SFA | 0.404 | 0.205 | 0.716 | 0.179 |
| MUFA | 0.356 | 0.326 | 0.682 | 0.191 |
| PUFA | 0.298 | 0.425 | 0.573 | 0.25 |
| Cholesterol | 0.839 | −0.005 | 0.371 | 0.115 |
| Starch | 0.207 | 0.235 | 0.165 | 0.923 |
| Sugars | 0.12 | 0.531 | 0.276 | 0.364 |
| Dietary fibre | 0.115 | 0.406 | 0.705 | 0.152 |
| Thiamine | 0.184 | 0.053 | 0.727 | 0.002 |
| Riboflavin | 0.459 | 0.105 | 0.636 | 0.058 |
| Vitamin B6 | 0.344 | 0.261 | 0.768 | 0.174 |
| Folate | 0.316 | 0.329 | 0.558 | 0.471 |
| Vitamin B12 | 0.528 | 0.059 | 0.27 | 0.089 |
| Vitamin C | 0.04 | 0.638 | 0.402 | 0.089 |
| Beta-carotene | 0.083 | 0.944 | 0.136 | 0.081 |
| Retinol | 0.919 | 0.211 | -0.007 | 0.157 |
| Vitamin E | 0.243 | 0.444 | 0.381 | 0.277 |
| Vitamin D | 0.537 | 0.205 | 0.359 | 0.148 |
| Calcium | 0.307 | 0.33 | 0.699 | 0.118 |
| Phosphorus | 0.349 | 0.163 | 0.851 | 0.092 |
| Iron | 0.31 | 0.253 | 0.782 | 0.116 |
| Potassium | 0.239 | 0.323 | 0.837 | 0.172 |
| Magnesium | 0.128 | 0.308 | 0.797 | 0.043 |
| Zinc | 0.403 | 0.172 | 0.79 | 0.129 |
| Explained variance (%) | 26 | 21 | 19 | 13 |
| Cumulative explained variance (%) | 26 | 47 | 66 | 79 |
3.2. Dietary, Lifestyle, Anthropometric and Socio-Demographic Variables Associated with Identified Nutrient Patterns
| Variables | PC1 (Animal Driven Nutrients) | PC2 (Vitamins, Fibre and Vegetable Oil Nutrients) | PC3 (Mixed Diet Driven Nutrients) | PC4 (Starch and Folate Driven) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | β | SE | p-Value | |
| Age (years) of adolescent | −0.027 | 0.036 | 0.46 | −0.046 | 0.036 | 0.21 | 0.033 | 0.022 | 0.14 | 0.007 | 0.037 | 0.84 |
| BMI | 0.024 | 0.016 | 0.15 | −0.009 | 0.016 | 0.58 | −0.005 | 0.1 | 0.64 | 0.001 | 0.017 | 0.98 |
| Log (Energy) | 0.607 | 0.132 | <0.0001 | 0.601 | 0.132 | <0.0001 | 2.127 | 0.08 | <0.0001 | 0.665 | 0.135 | <0.0001 |
| Sex | ||||||||||||
| Female | 0.235 | 0.11 | 0.03 | −0.052 | 0.11 | 0.64 | −0.046 | 0.067 | 0.5 | 0.147 | 0.112 | 0.19 |
| Male (Ref) | ||||||||||||
| Maternal Education level | ||||||||||||
| Primary school | −0.041 | 0.13 | 0.75 | 0.09 | 0.131 | 0.49 | −0.07 | 0.079 | 0.38 | −0.16 | 0.133 | 0.24 |
| Secondary and higher education | −0.147 | 0.138 | 0.29 | 0.171 | 0.138 | 0.22 | −0.109 | 0.084 | 0.2 | −0.57 | 0.141 | 0.69 |
| None (Ref) | ||||||||||||
| Physical activity of adolescent | ||||||||||||
| Walking to and from school (min week−1) | <0.0001 | <0.0001 | 0.62 | <0.0001 | <0.0001 | 0.74 | 0.001 | 0.001 | 0.01 | −0.001 | 0.001 | 0.05 |
| Tanner stage | ||||||||||||
| Mid | −0.067 | 0.151 | 0.66 | 0.343 | 0.151 | 0.02 | −0.045 | 0.092 | 0.62 | 0.014 | 0.154 | 0.93 |
| Early (Ref) | ||||||||||||
| Marital Status of mother | ||||||||||||
| Never in union | 0.231 | 0.121 | 0.05 | 0.196 | 0.121 | 0.11 | −0.108 | 0.703 | 0.14 | 0.106 | 0.124 | 0.4 |
| Ever in union ended | 0.017 | 0.183 | 0.93 | 0.104 | 0.183 | 0.57 | 0.051 | 0.11 | 0.65 | 0.001 | 0.187 | 0.99 |
| Ever in union current (Ref) | ||||||||||||
| Maternal age (years) | ||||||||||||
| 15–24 | 0.289 | 0.975 | 0.77 | 0.966 | 0.978 | 0.32 | −0.257 | 0.59 | 0.66 | 0.406 | 0.996 | 0.68 |
| 25–34 (Ref) | ||||||||||||
| 35–49 | 0.264 | 0.115 | 0.02 | 0.007 | 0.115 | 0.95 | −0.09 | 0.07 | 0.2 | 0.048 | 0.117 | 0.68 |
| >50 | −0.251 | 0.178 | 0.161 | 0.188 | 0.179 | 0.29 | 0.117 | 0.108 | 0.28 | 0.076 | 0.182 | 0.68 |
| SES status of mother (based on SES Wealth Index) | ||||||||||||
| lowest tertile | −0.336 | 0.134 | 0.01 | −0.098 | 0.134 | 0.46 | 0.166 | 0.081 | 0.04 | −0.06 | 0.136 | 0.67 |
| middle tertile | −0.11 | 0.132 | 0.4 | −0.207 | 0.133 | 0.12 | 0.071 | 0.08 | 0.39 | −0.07 | 0.135 | 0.62 |
| highest tertile (Ref) | ||||||||||||
| Variable | DF# | PC1 (Animal Driven Nutrients) | PC2 (Vitamins, Fibre and Vegetable Oil Nutrients) | PC3 (Mixed Diet Driven Nutrients) | PC4 (Starch and Folate Driven) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Partial R2 | % | p-value | Partial R2 | % | p-value | Partial R2 | % | p-value | Partial R2 | % | p-value | ||
| Age | 1 | 0.001 | 0.1 | 0.57 | 0.001 | 0.1 | 0.48 | 0.009 | 0.9 | 0.06 | 0.001 | 0.1 | 0.51 |
| BMI | 1 | 0.013 | 1.3 | 0.03 | 0.001 | 0.1 | 0.64 | 0.003 | 0.3 | 0.28 | 0.006 | 0.6 | 0.12 |
| Log(Energy) | 1 | 0.065 | 6.5 | <0.0001 | 0.06 | 6 | <0.0001 | 0.666 | 66.6 | <0.0001 | 0.067 | 6.7 | <0.0001 |
| Sex | 1 | 0.026 | 2.6 | <0.0001 | 0 | 0 | 0.85 | 0.005 | 0.5 | 0.17 | 0.004 | 0.4 | 0.23 |
| Maternal education | 2 | 0.059 | 5.9 | <0.0001 | 0.006 | 0.6 | 0.2 | 0.002 | 0.2 | 0.51 | 0 | 0 | 0.84 |
| Physical activity (Walking to and from school (min week−1) | 1 | 0.005 | 0.5 | 0.17 | 0.001 | 0.1 | 0.5 | 0 | 0 | 0.96 | 0.013 | 1.3 | 0.02 |
| Tanner Stage | 1 | 0.001 | 0.1 | 0.65 | 0.011 | 1.1 | 0.04 | 0.002 | 0.2 | 0.33 | 0.002 | 0.2 | 0.41 |
| Marital status of mother | 2 | 0.001 | 0.1 | 0.51 | 0.008 | 0.8 | 0.1 | 0.001 | 0.1 | 0.57 | 0.001 | 0.1 | 0.61 |
| Maternal age | 3 | 0.002 | 0.2 | 0.4 | 0.001 | 0.1 | 0.55 | 0.001 | 0.1 | 0.59 | 0.001 | 0.1 | 0.6 |
| SES status of mother (based on SES Wealth Index) | 2 | 0.013 | 1.3 | 0.04 | 0.01 | 1 | 0.07 | 0 | 0 | 0.84 | 0.005 | 0.5 | 0.23 |
| Nutrient pattern | M1 | M2 | M3 | M4 | ||||
|---|---|---|---|---|---|---|---|---|
| B (95% CI) | p value | B (95% CI) | p value | B (95% CI) | p value | B (95% CI) | p value | |
| PCI | 0.129 (0.018–0.239) | 0.02 | 0.137 (0.025; 0.248) | 0.02 | 0.118 (0.005; 0.230) | 0.04 | 0.120 (−0.005; 0.245) | 0.06 |
| Physical activity | 2.191×10−5 (−0.001; 0.001) | 0.95 | 0.0 (−0.001; 0.001) | 0.78 | 6.67×10−5 (−0.001; 0.001) | 0.87 | ||
| Socio-economic status | ||||||||
| low tertile | −0.331 (−0.601; −0.060) | 0.02 | −0.346 (−0.672; −0.020) | 0.04 | ||||
| middle tertile | 0.009 (−0.262; 0.280) | 0.95 | 0.144 (−0.172; 0.46) | 0.37 | ||||
| highest tertile (ref) | ||||||||
| Maternal education | ||||||||
| Total number of years of schooling | 0.026 (0.0; 0.053) | 0.05 | ||||||
| PC4 | 0.103 (−0.008; 0.213) | 0.05 | 0.092 (−0.022; 0.206) | 0.12 | 0.087 (−0.026; 0.201) | 0.13 | 0.011 (−0.117;0.138) | 0.87 |
| Physical activity | 2.74× 10−5 (−0.001; 0.001) | 0.94 | 0.0 (−0.001; 0.001) | 0.75 | 7.59×10−6 (−0.001; 0.001) | 0.99 | ||
| Socio-economic status | ||||||||
| low tertile | −0.361 (−0.629; −0.092) | 0.01 | −0.407 (−0.729; −0.085) | 0.01 | ||||
| middle tertile | 0.002 (−0.269; 0.273) | 0.98 | 0.103 (−0.212; 0.418) | 0.52 | ||||
| highest tertile (ref) | ||||||||
| Maternal education | ||||||||
| Total number of years of schooling | 0.028 (0.002; 0.05) | 0.04 | ||||||
| R2 values of each model | 0.009 | 0.007 | 0.029 | 0.063 | ||||
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgements
Author Contributions
Conflicts of Interest
References
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Freisling, H.; Fahey, M.T.; Moskal, A.; Ocke, M.C.; Ferrari, P.; Jenab, M.; Norat, T.; Naska, A.; Welch, A.A.; Navarro, C.; et al. Region-specific nutrient intake patterns exhibit a geographical gradient within and between European countries. J. Nutr. 2010, 140, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Moskal, A.; Pisa, P.T.; Ferrari, P.; Byrnes, G.; Freisling, H.; Boutron-Ruault, M.C.; Cadeau, C.; Nailler, L.; Wendt, A.; Kuhn, T.; et al. Nutrient patterns and their food sources in an International Study Setting: Report from the EPIC study. PLoS ONE 2014, 9, e98647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Kipnis, V.; Schatzkin, A.; Tasevska, N.; Potischman, N. Can we use biomarkers in combination with self-reports to strengthen the analysis of nutritional epidemiologic studies? Epidemiol. Perspect. Innov. 2010, 7, 2–7. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, A.; Gibney, M.J.; Brennan, L. Dietary intake patterns are reflected in metabolomic profiles: Potential role in dietary assessment studies. Am. J. Clin. Nutr. 2011, 93, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, R.M. New approaches to the study of dietary patterns. Br. J. Nutr. 2005, 93, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Bertuccio, P.; Edefonti, V.; Bravi, F.; Ferraroni, M.; Pelucchi, C.; Negri, E.; Decarli, A.; La, V.C. Nutrient dietary patterns and gastric cancer risk in Italy. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2882–2886. [Google Scholar] [CrossRef]
- Bosetti, C.; Bravi, F.; Turati, F.; Edefonti, V.; Polesel, J.; Decarli, A.; Negri, E.; Talamini, R.; Franceschi, S.; La, V.C.; et al. Nutrient-based dietary patterns and pancreatic cancer risk. Ann. Epidemiol. 2013, 23, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Bravi, F.; Edefonti, V.; Bosetti, C.; Talamini, R.; Montella, M.; Giacosa, A.; Franceschi, S.; Negri, E.; Ferraroni, M.; La, V.C.; Decarli, A. Nutrient dietary patterns and the risk of colorectal cancer: A case-control study from Italy. Cancer Causes Control 2010, 21, 1911–1918. [Google Scholar] [CrossRef] [PubMed]
- Bravi, F.; Edefonti, V.; Randi, G.; Garavello, W.; La, V.C.; Ferraroni, M.; Talamini, R.; Franceschi, S.; Decarli, A. Dietary patterns and the risk of esophageal cancer. Ann. Oncol. 2012, 23, 765–770. [Google Scholar] [CrossRef] [PubMed]
- De, S.E.; Boffetta, P.; Ronco, A.L.; Deneo-Pellegrini, H.; Acosta, G.; Gutierrez, L.P.; Mendilaharsu, M. Nutrient patterns and risk of lung cancer: A factor analysis in Uruguayan men. Lung Cancer 2008, 61, 283–291. [Google Scholar] [CrossRef] [PubMed]
- De, S.E.; Boffetta, P.; Fagundes, R.B.; Deneo-Pellegrini, H.; Ronco, A.L.; Acosta, G.; Mendilaharsu, M. Nutrient patterns and risk of squamous cell carcinoma of the esophagus: A factor analysis in uruguay. Anticancer Res. 2008, 28, 2499–2506. [Google Scholar] [PubMed]
- De, S.E.; Ronco, A.L.; Boffetta, P.; Deneo-Pellegrini, H.; Correa, P.; Acosta, G.; Mendilaharsu, M. Nutrient-derived dietary patterns and risk of colorectal cancer: A factor analysis in Uruguay. Asian Pac. J. Cancer Prev. 2012, 13, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Deneo-Pellegrini, H.; Boffetta, P.; De, S.E.; Correa, P.; Ronco, A.L.; Acosta, G.; Mendilaharsu, M.; Silva, C.; Luaces, M.E. Nutrient-based dietary patterns of head and neck squamous cell cancer: A factor analysis in Uruguay. Cancer Causes Control 2013, 24, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Edefonti, V.; Bravi, F.; La, V.C.; Randi, G.; Ferraroni, M.; Garavello, W.; Franceschi, S.; Talamini, R.; Boffetta, P.; Decarli, A. Nutrient-based dietary patterns and the risk of oral and pharyngeal cancer. Oral Oncol. 2010, 46, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Edefonti, V.; Hashibe, M.; Ambrogi, F.; Parpinel, M.; Bravi, F.; Talamini, R.; Levi, F.; Yu, G.; Morgenstern, H.; Kelsey, K.; et al. Nutrient-based dietary patterns and the risk of head and neck cancer: A pooled analysis in the International Head and Neck Cancer Epidemiology consortium. Ann. Oncol. 2012, 23, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Ganganna, P.; Johnson, A.A. A new nutrient index for measuring nutritional well-being of Indian states. Int. J. Vitam. Nutr. Res. 1985, 55, 315–322. [Google Scholar] [PubMed]
- Ishimoto, H.; Nakamura, H.; Miyoshi, T. Epidemiological study on relationship between breast cancer mortality and dietary factors. Tokushima J. Exp. Med. 1994, 41, 103–114. [Google Scholar] [PubMed]
- Palli, D.; Russo, A.; Decarli, A. Dietary patterns, nutrient intake and gastric cancer in a high-risk area of Italy. Cancer Causes Control 2001, 12, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Ronco, A.L.; De, S.E.; Aune, D.; Boffetta, P.; Deneo-Pellegrini, H.; Acosta, G.; Mendilaharsu, M. Nutrient patterns and risk of breast cancer in Uruguay. Asian Pac. J. Cancer Prev. 2010, 11, 519–524. [Google Scholar] [PubMed]
- Turati, F.; Edefonti, V.; Bravi, F.; Ferraroni, M.; Franceschi, S.; La, V.C.; Montella, M.; Talamini, R.; Decarli, A. Nutrient-based dietary patterns, family history, and colorectal cancer. Eur. J. Cancer Prev. 2011, 20, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Pisa, P.T.; Vorster, H.H.; Nishida, C. Cardiovascular disease and nutrition: The use of food-based dietary guidelines for prevention in Africa. South Afr. Heart J. 2011, 8, 38–47. [Google Scholar]
- Pisa, P.T.; Behanan, R.; Vorster, H.H.; Kruger, A. Social drift of cardiovascular disease risk factors in Africans from the North West Province of South Africa: The PURE study. Cardiovasc. J. Afr. 2012, 23, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Vorster, H.H. The emergence of cardiovascular disease during urbanisation of Africans. Public Health Nutr. 2002, 5, 239–243. [Google Scholar] [PubMed]
- Popkin, B.M. Nutrition in transition: The changing global nutrition challenge. Asia Pac. J. Clin. Nutr. 2001, 10, S13–S18. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Dynamics of the nutrition transition and its implications for the developing world. Forum Nutr. 2003, 56, 262–264. [Google Scholar] [PubMed]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Bosman, L.; Herselman, M.G.; Kruger, H.S.; Labadarios, D. Secondary analysis of anthropometric data from a South African national food consumption survey, using different growth reference standards. Matern. Child Health J. 2011, 15, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Jinabhai, C.C.; Reddy, P.; Taylor, M.; Monyeki, D.; Kamabaran, N.; Omardien, R.; Sullivan, K.R. Sex differences in under and over nutrition among school-going Black teenagers in South Africa: An uneven nutrition trajectory. Trop. Med. Int. Health 2007, 12, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Kimani-Murage, E.W.; Kahn, K.; Pettifor, J.M.; Tollman, S.M.; Dunger, D.B.; Gomez-Olive, X.F.; Norris, S.A. The prevalence of stunting, overweight and obesity, and metabolic disease risk in rural South African children. BMC Public Health 2010, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.J.; Jones, R.M.; Levita, L.; Libby, V.; Pattwell, S.S.; Ruberry, E.J.; Soliman, F.; Somerville, L.H. The storm and stress of adolescence: Insights from human imaging and mouse genetics. Dev. Psychobiol. 2010, 52, 225–235. [Google Scholar] [PubMed]
- Huybrechts, I.; de Vriendt, T.; Breidenassel, C.; Rogiers, J.; Vanaelst, B.; Cuenca-Garcia, M.; Moreno, L.A.; Gonzalez-Gross, M.; Roccaldo, R.; Kafatos, A.; et al. Mechanisms of stress, energy homeostasis and insulin resistance in European adolescents—The HELENA study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1082–1089. [Google Scholar] [CrossRef] [PubMed]
- Kahn, K.; Tollman, S.M.; Collinson, M.A.; Clark, S.J.; Twine, R.; Clark, B.D.; Shabangu, M.; Gomez-Olive, F.X.; Mokoena, O.; Garenne, M.L. Research into health, population and social transitions in rural South Africa: Data and methods of the Agincourt Health and Demographic Surveillance System. Scand. J. Public Health Suppl. 2007, 69, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Kahn, K.; Collinson, M.A.; Gomez-Olive, F.X.; Mokoena, O.; Twine, R.; Mee, P.; Afolabi, S.A.; Clark, B.D.; Kabudula, C.W.; Khosa, A.; et al. Profile: Agincourt health and socio-demographic surveillance system. Int. J. Epidemiol. 2012, 41, 988–1001. [Google Scholar] [CrossRef] [PubMed]
- Kimani-Murage, E.W.; Kahn, K.; Pettifor, J.M.; Tollman, S.M.; Klipstein-Grobusch, K.; Norris, S.A. Predictors of adolescent weight status and central obesity in rural South Africa. Public Health Nutr. 2011, 14, 1114–1122. [Google Scholar] [CrossRef] [PubMed]
- Wrottesley, S.V.; Micklesfield, L.K.; Hamill, M.M.; Goldberg, G.R.; Prentice, A.; Pettifor, J.M.; Norris, S.A.; Feeley, A.B. Dietary intake and body composition in HIV-positive and -negative South African women. Public Health Nutr. 2014, 17, 1603–1613. [Google Scholar] [CrossRef] [PubMed]
- Nel, J.; Steyn, J.P. Report on South African Food Consumption Studies Undertaken among Diffirent Population Groups (1983–2000): Average Intakes of Foods Most Commonly Consumed; Department of Health of Directorate: Pretoria, South Africa, 2002.
- Steyn, N.; Senekal, M. A Guide for the use of Dietary Assessment and Education Kit (DAEK); Medical Research Council: Cape Town, South Africa, 2005. [Google Scholar]
- Steyn, N.P.; Senekal, M.; Norris, S.A.; Whati, L.; Mackeown, J.M.; Nel, J.H. How well do adolescents determine portion sizes of foods and beverages? Asia Pac. J. Clin. Nutr. 2006, 15, 35–42. [Google Scholar] [PubMed]
- Langenhoven, M.L.; Kruger, M.; Gouws, E. MRC Food Composition Tables, 3rd ed.; Medical Research Council: Cape Town, South Africa, 1991. [Google Scholar]
- World Health Organization. WHO Anthro Plus for Personal Computers, Manual. Software for Assessing Growth of the World’s Children and Adolescents; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Norris, S.; Ritcher, L. Usefulness and realibility of tanner pubertal self rating to urban black adolescents in South Africa. J. Res. Adolesc. 2005, 15, 609–624. [Google Scholar] [CrossRef]
- McVeigh, J.A.; Norris, S.A.; Cameron, N.; Pettifor, J.M. Associations between physical activity and bone mass in black and white South African children at age 9 year. J. Appl. Physiol. 2004, 97, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- McVeigh, J.A.; Norris, S.A. Criterion validity and test-retest realibility of a physical activity questionnaire in South African primary school-aged children. South Afr. J. Sports Med. 2012, 24, 43–48. [Google Scholar]
- Micklesfield, L.K.; Pedro, T.M.; Kahn, K.; Kinsman, J.; Pettifor, J.M.; Tollman, S.; Norris, S.A. Physical activity and sedentary behavior among adolescents in rural South Africa: Levels, patterns and correlates. BMC Public Health 2014, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.A.; Wichern, D.W. Applied Multivariate Statistical Analysis, 5th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2007. [Google Scholar]
- Willet, W.C. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Tucker, K.L. Dietary patterns, approaches, and multicultural perspective. Appl. Physiol. Nutr. Metab. 2010, 35, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Edefonti, V.; Decarli, A.; La, V.C.; Bosetti, C.; Randi, G.; Franceschi, S.; Dal, M.L.; Ferraroni, M. Nutrient dietary patterns and the risk of breast and ovarian cancers. Int. J. Cancer 2008, 122, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Edefonti, V.; Bravi, F.; Garavello, W.; La, V.C.; Parpinel, M.; Franceschi, S.; Dal, M.L.; Bosetti, C.; Boffetta, P.; Ferraroni, M.; et al. Nutrient-based dietary patterns and laryngeal cancer: Evidence from an exploratory factor analysis. Cancer Epidemiol. Biomark. Prev. 2010, 19, 18–27. [Google Scholar] [CrossRef]
- Slimani, N.; Fahey, M.; Welch, A.A.; Wirfalt, E.; Stripp, C.; Bergstrom, E.; Linseisen, J.; Schulze, M.B.; Bamia, C.; Chloptsios, Y.; et al. Diversity of dietary patterns observed in the European Prospective Investigation into Cancer and Nutrition (EPIC) project. Public Health Nutr. 2002, 5, 1311–1328. [Google Scholar] [CrossRef] [PubMed]
- Dugee, O.; Khor, G.L.; Lye, M.S.; Luvsannyam, L.; Janchiv, O.; Jamyan, B.; Esa, N. Association of major dietary patterns with obesity risk among Mongolian men and women. Asia Pac. J. Clin. Nutr. 2009, 18, 433–440. [Google Scholar] [PubMed]
- Esmaillzadeh, A.; Kimiagar, M.; Mehrabi, Y.; Azadbakht, L.; Hu, F.B.; Willett, W.C. Dietary patterns, insulin resistance, and prevalence of the metabolic syndrome in women. Am. J. Clin. Nutr. 2007, 85, 910–918. [Google Scholar] [PubMed]
- Murtaugh, M.A.; Herrick, J.S.; Sweeney, C.; Baumgartner, K.B.; Guiliano, A.R.; Byers, T.; Slattery, M.L. Diet composition and risk of overweight and obesity in women living in the southwestern United States. J. Am. Diet. Assoc. 2007, 107, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Paradis, A.M.; Godin, G.; Perusse, L.; Vohl, M.C. Associations between dietary patterns and obesity phenotypes. Int. J. Obes. 2009, 33, 1419–1426. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisa, P.T.; Pedro, T.M.; Kahn, K.; Tollman, S.M.; Pettifor, J.M.; Norris, S.A. Nutrient Patterns and Their Association with Socio-Demographic, Lifestyle Factors and Obesity Risk in Rural South African Adolescents. Nutrients 2015, 7, 3464-3482. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053464
Pisa PT, Pedro TM, Kahn K, Tollman SM, Pettifor JM, Norris SA. Nutrient Patterns and Their Association with Socio-Demographic, Lifestyle Factors and Obesity Risk in Rural South African Adolescents. Nutrients. 2015; 7(5):3464-3482. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053464
Chicago/Turabian StylePisa, Pedro T., Titilola M. Pedro, Kathleen Kahn, Stephen M. Tollman, John M. Pettifor, and Shane A. Norris. 2015. "Nutrient Patterns and Their Association with Socio-Demographic, Lifestyle Factors and Obesity Risk in Rural South African Adolescents" Nutrients 7, no. 5: 3464-3482. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7053464