The Potential for Zinc Stable Isotope Techniques and Modelling to Determine Optimal Zinc Supplementation

Abstract
:1. Introduction
2. Techniques for Measuring Zinc Physiology
3. Assessment of Zinc Physiology Using Zinc Stable Isotopes
3.1. Intestinal Regulation of Zinc Homeostasis
3.2. Zinc Bioavailability and Phytic Acid
3.3. Measurement of Zinc Absorption
- (i)
- That both isotopes (oral and intravenous) enter the plasma at the same time.
- (ii)
- That the isotope enrichment in plasma and urine are the same after 40 hrs (enough time has elapsed since isotope administration so that the intravenous and oral tracer enrichments are decaying proportionally).
- (iii)
- That urine enrichments of both isotopes are similar for plasma.
- (iv)
- That the extrinsic label isotope reflects that of the intrinsic zinc in the diet.
3.4. Measurement of Endogenous Faecal Zinc (EFZ) Excretion
- (i)
- That the endogenous zinc excreted in the faeces is derived from a pool of zinc that exchanges rapidly with zinc in plasma and in certain solid tissues.
- (ii)
- That there will be some unabsorbed label in the faeces compared to label that has been absorbed and then secreted into the intestine and excreted with the faeces.
- (iii)
- That there will be no unabsorbed quantity of the same tracer used to label the urine in the faeces during the metabolic period.
3.5. Assessment of Readily Exchangeable Zinc Pools (EZP)
- (i)
- That the EZP accounting for 10% of total body zinc in adults is considered to be particularly important for zinc-dependent biological processes.
- (ii)
- That estimates of EZP size can be obtained from plasma or urine enrichment data after intravenous administration of a zinc stable isotope tracer.
3.6. Limitations of Zinc Stable Isotope Techniques
4. Utilisation of Zinc Stable Isotope to Model Zinc Kinetics
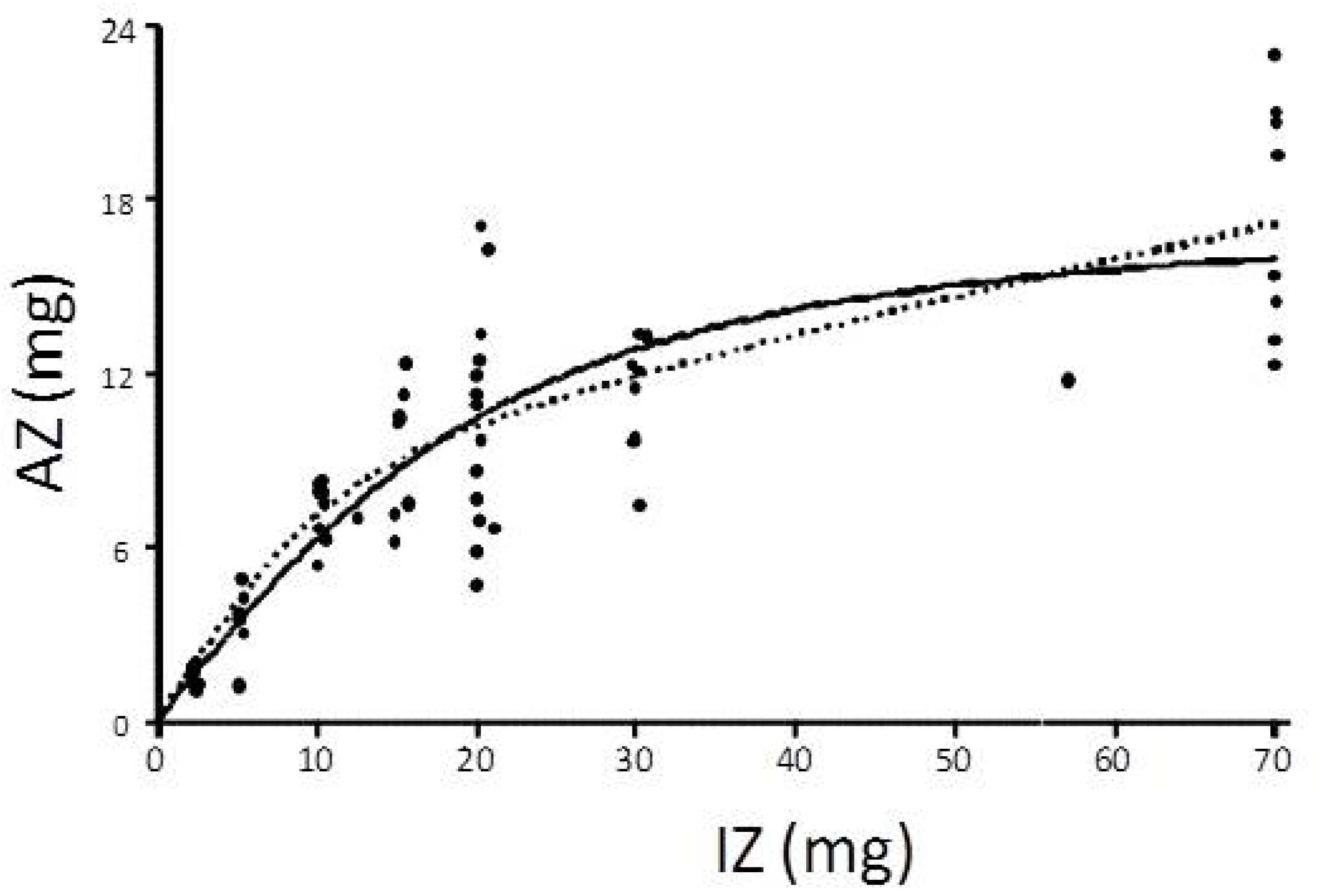
4.1. Saturation Response Kinetic Modelling

- (i)
- That the saturation response model fits a Michaelis-Menten kinetics curve
4.2. Compartmental Modelling
5. Implications for Zinc Supplementation
5.1. Zinc Dose and Amount Absorbed
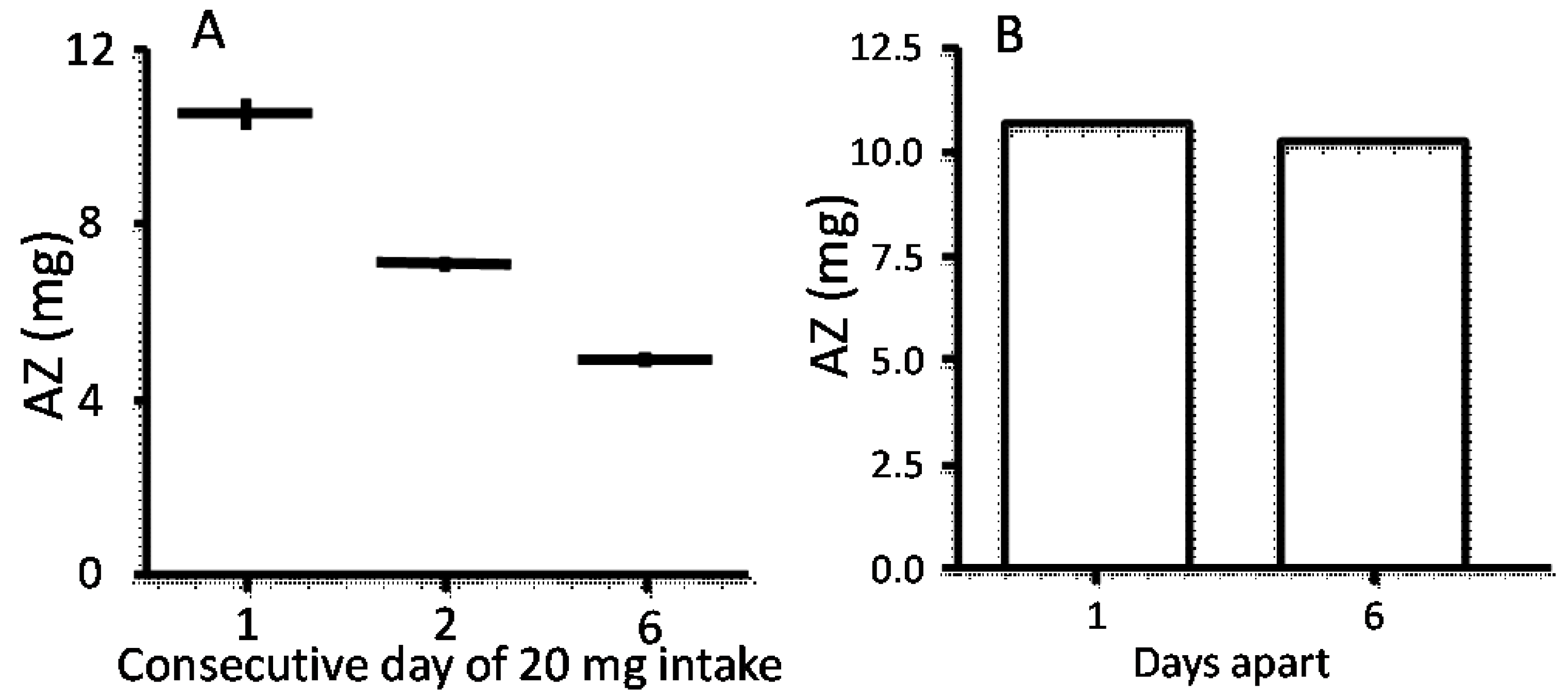
5.2. Frequency and Duration of Administration?

5.3. The Optimal Zinc Salt?
5.4. Zinc Supplementation and Its Relationship to Markers of Zinc Deficiency
5.5. Zinc Supplementation and Its Relationship to Intestinal Disease

{kind=link}
{kind=link}
| Reference | Context | Zinc Intake | Zinc Status Parameters Using DITR Technique | Key Findings | ||
|---|---|---|---|---|---|---|
| FAZ/AZ/TAZ | EZP | EFZ | ||||
| Ariff et al., 2014 [146] | Pakistan; healthy breastfed infants (6 months) | 10 mg/day for 6 month | √ | √ | ↑ AZ, EZP | |
| Esami et al., 2014 [147] | Kenya; healthy breastfed infants (9 months) | 5 mg/day for 3 month | √ | ↔ AZ | ||
| Hambidge et al., 2007 [36] | Guatemala; healthy children (8.9 ±1.3 years) | low-, isohybrid- and control-phyate maize | √ | ↔ EFZ | ||
| Herman et al., 2002 [132] | Indonesia; healthy children (4–8 years) | fortified flour meal 60 mg Zn/kg (as ZnO or ZnSO4) | √ | ↔ AZ between ZnO or ZnSO4 | ||
| Hettiarachchi et al., 2004 [149] | Sri Lanka; healthy children (7–10 years) | fortified rice flour 60 mg/kg (ZnO) for 2 weeks | √ | addition of Na2EDTA improve zinc absorption | ||
| Hettiarachchi et al., 2010 [153] | Sri Lanka; healthy children (4–7 years) | meal 1.5 mg Zn (ZnSO4) | √ | ↔ AZ | ||
| Islam et al., 2013 [154] | Bangladesh; healthy non breastfed children (36–59 months) | high-zinc rice (HZnR), conventional rice (CR), or CR+zinc for 1 day | √ | ↔ TAZ between CR and HZnR ↑ TAZ for CR+Zn | ||
| Kennedy et al., 2010 [150] | Malawi; healthy children (2–5 years) | maize high-phytate or maize reduced-phytate diets for 40 days | √ | ↔ EZP | ||
| Kodkany et al., 2013 [155] | India; healthy children (22–35 months) | zinc-rich dry pearl millet flour for 1 day | √ | zinc biofortified pearl millet adequately meet the physiological requirements | ||
| Li et al., 2015 [156] | China; healthy children (13 ± 1.1 years) | 3 mg Zn for 10 days +NaFeEDTA-fortified soy sauce | √ | ↔ FAZ | ||
| Lopez de Romana et al., 2005 [66] | Peru; children at risk of zinc deficiency (3–4 years) | 0, 3, 9 mg Zn/100 g flour for 7 weeks | √ | ↔ AZ before and after | ||
| Manary et al., 2010 [43] | Malawi; children with tropical enteropathy (3–5 years) | habitual diet | √ | √ | ↑ EFZ compared to healthy | |
| Manary et al., 2002 [73] | Malawi; healthy children (2–5 years) | maize-based diet + 1.5–2 mg Zn for 1 day | √ | √ | ↑ EFZ compared to previous studies | |
| Manary et al., 2000 [151] | Malawi; children hospitalised for tuberculosis (3–13 years) | corn+soy porridge (low or high phytate) for 3–7 days | √ | √ | low phytate ↑ FAZ, TAZ | |
| Mazariegos et al., 2006 [152] | Guatemala; healthy children (6–11 years) | low-phytate, isohybrid wild-type or a local maize for 10 weeks | √ | ↔ FAZ, TAZ | ||
| Nair et al., 2013 [157] | India; healthy adolescent (13–15 years) | standardized rice meal or the same meal with 100 g of guava fruit (2.7 mg Zn) for 2 days | √ | ↔ FAZ | ||
| Sheng et al., 2006 [37] | China; healthy children (19–25 months) | habitual diet | √ | √ | mean intake and absorption of zinc are low compared to average dietary requirements | |
| Zlotkin et al., 2006 [148] | Ghana; healthy children (12–24 months) | 5 or 10 mg Zn for 14 days | √ | ↑ TAZ for high zinc | ||
6. Summary and Conclusions
- Proof of concept demonstrating relationship of a clinical response to a pharmacodynamics or pharmacokinetic marker. At this stage, there has been very little work relating stable isotope measurements such as FAZ, TAZ, EZP and so on to zinc administration and clinical benefit.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bhutta, Z.A.; Black, R.E.; Brown, K.H.; Gardner, J.M. Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: Pooled analysis of randomized controlled trials. J. Pediatr. 1999, 135, 689–697. [Google Scholar] [CrossRef]
- Cousins, R.J. A role of zinc in the regulation of gene expression. Proc. Nutr. Soc. 1998, 57, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lonnerdal, B.; Ruel, M.T.; Sandtrom, B.; Wasantwisut, E.; Hotz, C. International zinc nutrition consultative group (izincg) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar] [PubMed]
- Chasapis, C.; Loutsidou, A.; Spiliopoulou, C.; Stefanidou, M. Zinc and human health: An update. Arch. Toxicol. 2012, 86, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Scrimgeour, A.G.; Lukaski, H.C. Zinc and diarrheal disease: Current status and future perspectives. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Scrimgeour, A.; Condlin, M.; Otieno, L.; Bovill, M. Zinc intervention strategies: Costs and health benefits. In Nutrients, Dietary Supplements, and Nutriceuticals; Gerald, J.K., Watson, R.R., Preedy, V.R., Eds.; Humana Press, 2011; pp. 189–214. [Google Scholar]
- Aggarwal, R.; Sentz, J.; Miller, M.A. Role of zinc administration in prevention of childhood diarrhea and respiratory illnesses: A meta-analysis. Pediatrics 2007, 119, 1120–1130. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Nizami, S.Q.; Isani, Z. Zinc supplementation in malnourished children with persistent diarrhea in pakistan. Pediatrics 1999, 103, e42. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Peerson, J.M.; Baker, S.K.; Hess, S.Y. Preventive zinc supplementation among infants, preschoolers, and older prepubertal children. Food Nutr. Bull. 2009, 30, S12–S40. [Google Scholar] [PubMed]
- Baqui, A.H.; Black, R.E.; El Arifeen, S.; Yunus, M.; Chakraborty, J.; Ahmed, S.; Vaughan, J.P. Effect of zinc supplementation started during diarrhoea on morbidity and mortality in bangladeshi children: Community randomised trial. BMJ 2002, 325, 1059. [Google Scholar] [CrossRef] [PubMed]
- Muller, O.; Becher, H.; van Zweeden, A.B.; Ye, Y.; Diallo, D.A.; Konate, A.T.; Gbangou, A.; Kouyate, B.; Garenne, M. Effect of zinc supplementation on malaria and other causes of morbidity in west african children: Randomised double blind placebo controlled trial. BMJ 2001, 322, 1567. [Google Scholar] [CrossRef] [PubMed]
- Sazawal, S.; Black, R.E.; Menon, V.P.; Dinghra, P.; Caulfield, L.E.; Dhingra, U.; Bagati, A. Zinc supplementation in infants born small for gestational age reduces mortality: A prospective, randomized, controlled trial. Pediatrics 2001, 108, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.B.; Dhande, L.A.; Rawat, M.S. Therapeutic evaluation of zinc and copper supplementation in acute diarrhea in children: Double blind randomized trial. Indian Pediatr. 2005, 42, 433–442. [Google Scholar] [PubMed]
- Brooks, W.A.; Santosham, M.; Naheed, A.; Goswami, D.; Wahed, M.A.; Diener-West, M.; Faruque, A.S.; Black, R.E. Effect of weekly zinc supplements on incidence of pneumonia and diarrhoea in children younger than 2 years in an urban, low-income population in bangladesh: Randomised controlled trial. Lancet 2005, 366, 999–1004. [Google Scholar] [CrossRef]
- Brown, K.H.; Peerson, J.M.; Rivera, J.; Allen, L.H. Effect of supplemental zinc on the growth and serum zinc concentrations of prepubertal children: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2002, 75, 1062–1071. [Google Scholar] [PubMed]
- Black, R.E. Therapeutic and preventive effects of zinc on serious childhood infectious diseases in developing countries. Am. J. Clin. Nutr. 1998, 68, 476S–479S. [Google Scholar] [PubMed]
- Black, R.E.; Sazawal, S. Zinc and childhood infectious disease morbidity and mortality. Br. J. Nutr. 2001, 85 (Suppl. 2), S125–S129. [Google Scholar] [CrossRef] [PubMed]
- Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; The National Academies Press: Washington, DC, USA, 2001.
- Horton, S.A.H.; Rivera, J.A. Hunger and malnutrition. In Global Crises, Global Solutions, 2nd ed.; Lomborg, B., Ed.; Cambridge University Press: The Edinburgh Building, Cambridge, UK, 2009; pp. 305–333. [Google Scholar]
- WHO/UNICEF, Joint Statement on the Clinical Management of Acute Diarrhoea; UNICEF, 2004.
- Patro, B.; Golicki, D.; Szajewska, H. Meta-analysis: Zinc supplementation for acute gastroenteritis in children. Aliment. Pharmacol. Ther. 2008, 28, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.B.; Mamtani, M.; Badhoniya, N.; Kulkarni, H. What zinc supplementation does and does not achieve in diarrhea prevention: A systematic review and meta-analysis. BMC Infect. Dis. 2011, 11, 122. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Mamtani, M.; Dibley, M.J.; Badhoniya, N.; Kulkarni, H. Therapeutic value of zinc supplementation in acute and persistent diarrhea: A systematic review. PLoS ONE 2010, 5, e10386. [Google Scholar] [CrossRef] [PubMed]
- Wastney, M.E.; Henkin, R.I. Development and application of a model for zinc metabolism in humans. Prog. Food Nutr. Sci. 1988, 12, 243–254. [Google Scholar] [PubMed]
- Wastney, M.E.; Henkin, R.I. Calculation of zinc absorption in humans using tracers by fecal monitoring and a compartmental approach. J. Nutr. 1989, 119, 1438–1443. [Google Scholar] [PubMed]
- Sandström, B.; Cederblad, A. Zinc absorption from composite meals. Ιι. Influence of the main protein source. Am. J. Clin. Nutr. 1980, 33, 1778–1783. [Google Scholar] [PubMed]
- Wastney, M.E.; Aamodt, R.L.; Rumble, W.F.; Henkin, R.I. Kinetic analysis of zinc metabolism and its regulation in normal humans. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 1986, 251, R398–R408. [Google Scholar]
- Sandström, B.; Almgren, A.; Kivistö, B.; Cederblad, A. Zinc absorption in humans from meals based on rye, barley, oatmeal, triticale and whole wheat. J. Nutr. 1987, 117, 1898–1902. [Google Scholar] [PubMed]
- Sandström, B.; Kivistö, B.; Cederblad, A. Absorption of zinc from soy protein meals in humans. J. Nutr. 1987, 117, 321–327. [Google Scholar] [PubMed]
- Johnson, P.E. A mass spectrometric method for use of stable isotopes as tracers in studies of iron, zinc, and copper absorption in human subjects. J. Nutr. 1982, 112, 1414–1424. [Google Scholar] [PubMed]
- Turnlund, J.R.; Durkin, N.; Costa, F.; Margen, S. Stable isotope studies of zinc absorption and retention in young and elderly men. J. Nutr. 1986, 116, 1239–1247. [Google Scholar] [PubMed]
- Friel, J.K.; Naake, V.L.; Miller, L.V.; Fennessey, P.V. The analysis of stable isotopes in urine to determine the fractional absorption of zinc. Am. J. Clin. Nutr. 1992, 55, 473–477. [Google Scholar] [PubMed]
- Janghorbani, M.; Young, V.R. Use of stable isotopes to determine bioavailability of minerals in human diets using the method of fecal monitoring. Am. J. Clin. Nutr. 1980, 33, 2021–2030. [Google Scholar] [PubMed]
- Shames, D.M.; Woodhouse, L.R.; Lowe, N.M.; King, J.C. Accuracy of simple techniques for estimating fractional zinc absorption in humans. J. Nutr. 2001, 131, 1854–1861. [Google Scholar] [PubMed]
- Griffin, I.J.; Lynch, M.F.; Hawthorne, K.M.; Chen, Z. Zinc homeostasis in 1–4 year olds consuming diets typical of us children. Br. J. Nutr. 2007, 98, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Hambidge, K.M.; Mazariegos, M.; Solomons, N.W.; Westcott, J.E.; Lei, S.; Raboy, V.; Grunwald, G.; Miller, L.V.; Sheng, X.; Krebs, N.F. Intestinal excretion of endogenous zinc in guatemalan school children. J. Nutr. 2007, 137, 1747–1749. [Google Scholar] [PubMed]
- Sheng, X.; Hambidge, K.M.; Zhu, X.; Ni, J.; Bailey, K.B.; Gibson, R.S.; Krebs, N.F. Major variables of zinc homeostasis in chinese toddlers1–. Am. J. Clin. Nutr. 2006, 84, 389–394. [Google Scholar] [PubMed]
- Griffin, I.J.; Hicks, P.D.; Liang, L.K.; Abrams, S.A. Metabolic adaptations to low zinc intakes in premenarcheal girls. Am. J. Clin. Nutr. 2004, 80, 385–390. [Google Scholar] [PubMed]
- Hambidge, K.M.; Krebs, N.F.; Miller, L. Evaluation of zinc metabolism with use of stable-isotope techniques: Implications for the assessment of zinc status. Am. J. Clin. Nutr. 1998, 68, 410S–413S. [Google Scholar] [PubMed]
- Krebs, N.; Hambidge, K.; Westcott, J.; Miller, L.; Grunwald, G.K. Exchangeable zinc pool size in infants is related to key variables of zinc homeostasis. J. Nutr. 2003, 133, 1498. [Google Scholar]
- Krebs, N.; Hambidge, K.M. Zinc metabolism and homeostasis: The application of tracer techniques to human zinc physiology. Biometals 2001, 14, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Krebs, N.F. Overview of zinc absorption and excretion in the human gastrointestinal tract. J. Nutr. 2000, 130, 1374–1377. [Google Scholar]
- Manary, M.J.; Abrams, S.A.; Griffin, I.J.; Quimper, M.M.; Shulman, R.J.; Hamzo, M.G.; Chen, Z.; Maleta, K.; Manary, M.J. Perturbed zinc homeostasis in rural 3–5-y-old malawian children is associated with abnormalities in intestinal permeability attributed to tropical enteropathy. Pediatr. Res. 2010, 67, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Plum, L.; Rink, L.; Haase, H. The essential toxin: Impact of zinc on human health. Int. J. Environ. Res. Public Health 2010, 7, 1342–1365. [Google Scholar] [CrossRef] [PubMed]
- Walter, A.; Krämer, K.; Most, E.; Pallauf, J. Zinc availability from zinc lipoate and zinc sulfate in growing rats. J. Trace Elem. Med. Biol. 2002, 16, 169–174. [Google Scholar] [CrossRef]
- Wolffram, S.; Bisang, B.; Grenacher, B.; Scharrer, E. Transport of tri- and dicarboxylic acids across the intestinal brush border membrane of calves. J. Nutr. 1990, 120, 767–774. [Google Scholar] [PubMed]
- Walter, A.; Rimbach, G.; Most, E.; Pallauf, J. Effect of citric acid supplements to a maize-soya diet on the in vitro availability of minerals, trace elements, and heavy metals. Zentralbl Veterinarmed. A 1998, 45, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Nävert, B.; Sandström, B.; Cederblad, A. Reduction of the phytate content of bran by leavening in bread and its effect on zinc absorption in man. Br. J. Nutr. 1985, 53, 47–53. [Google Scholar] [PubMed]
- Sandström, B.; Almgren, A.; Kivistö, B.; Cederblad, A. Effect of protein level and protein source on zinc absorption in humans. J. Nutr. 1989, 119, 48–53. [Google Scholar] [PubMed]
- Wise, A. Phytate and zinc bioavailability. Int. J. Food Sci. Nutr. 1995, 46, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Afify, A.-M.; El-Beltagi, H.S.; El-Salam, S.M.; Omran, A.A. Bioavailability of iron, zinc, phytate and phytase activity during soaking and germination of white sorghum varieties. PLoS ONE 2011, 6, e25512. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, A.S. The effect of food processing on phytate hydrolysis and availability of iron and zinc. Adv. Exp. Med. Biol. 1991, 289, 499–508. [Google Scholar] [PubMed]
- Hotz, C.; Gibson, R.S. Assessment of home-based processing methods to reduce the phytate content and phytate/zinc molar ratio of white maize (zea mays). J. Agric. Food Chem. 2001, 49, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Hotz, C.; Gibson, R.S. Traditional food-processing and preparation practices to enhance the bioavailability of micronutrients in plant-based diets. J. Nutr. 2007, 137, 1097–1100. [Google Scholar] [PubMed]
- Krebs, N.F.; Miller, L.V.; Naake, V.L.; Lei, S. The use of stable isotope techniques to assess zinc metabolism. J. Nutr. Biochem. 1995, 6, 292–301. [Google Scholar] [CrossRef]
- Griffin, I.J.; Kim, S.C.; Hicks, P.D.; Liang, L.K.; Abrams, S.A. Zinc metabolism in adolescents with crohn’s disease. Pediatr. Res. 2004, 56, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Yang, X.; Piao, J.; Tian, Y.; Wang, Y.; Wang, J. Studies on zinc bioavailability from a representative diet in chinese urban women. J. Trace Elem. Med. Biol. 2005, 19, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Tran, C.D.; Katsikeros, R.; Manton, N.; Krebs, N.F.; Hambidge, K.M.; Butler, R.N.; Davidson, G.P. Zinc homeostasis and gut function in children with celiac disease. Am. J. Clin. Nutr. 2011, 94, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Hambidge, K.M.; Abebe, Y.; Gibson, R.S.; Westcott, J.E. Zinc absorption during late pregnancy in rural southern ethiopia. Am. J. Clin. Nutr. 2006, 84, 1102–1106. [Google Scholar] [PubMed]
- Lee, D.Y.; Prasad, A.S.; Hydrickadair, C.; Brewer, G.; Johnson, P.E. Homeostasis of zinc in marginal human zinc-deficiency - role of absorption and endogenous excretion of zinc. J. Lab. Clin. Med. 1993, 122, 549–556. [Google Scholar] [PubMed]
- Turnlund, J.R.; Michel, M.C.; Keyes, W.R.; King, J.C. Use of enriched stable isotopes to determine zinc and iron absorption in elderly men. Am. J. Clin. Nutr. 1982, 35, 1033–1040. [Google Scholar] [PubMed]
- Wada, L.; Turnlund, J.R.; King, J.C. Zinc utilization in young men fed adequate and low zinc intakes. J. Nutr. 1985, 115, 1345–1354. [Google Scholar] [PubMed]
- Taylor, C.M.; Bacon, J.R.; Aggett, P.J.; Bremner, I. Homeostatic regulation of zinc absorption and endogenous losses in zinc-deprived men. Am. J. Clin. Nutr. 1991, 53, 755–763. [Google Scholar] [PubMed]
- Chung, C. Current dietary zinc intake has a greater effect on fractional zinc absorption than does longer term inc consumption in helathy adult men. Am. J. Clin. Nutr. 2008, 87, 1224–1229. [Google Scholar] [PubMed]
- Sandström, B. Dose dependence of zinc and manganese absorption in man. Proc. Nutr. Soc. 1992, 51, 211–218. [Google Scholar] [CrossRef] [PubMed]
- López de Romaña, D.; Salazar, M.; Hambidge, K.M.; Penny, M.E. Longitudinal measurements of zinc absorption in peruvian children consuming wheat products fortified with iron only or iron and 1 of 2 amounts of zinc. Am. J. Clin. Nutr. 2005, 81, 637–647. [Google Scholar] [PubMed]
- Sian, L.; Mingyan, X.; Miller, L.V.; Tong, L.; Krebs, N.F.; Hambidge, K.M. Zinc absorption and intestinal losses of endogenous zinc in young chinese women with marginal zinc intakes. Am. J. Clin. Nutr. 1996, 63, 348. [Google Scholar] [PubMed]
- King, J.C.; Shames, D.; Woodhouse, L. Zinc homeostasis in humans. J. Nutr. 2000, 130, 1360S–1366S. [Google Scholar] [PubMed]
- Johnson, P.E.; Hunt, C.D.; Milne, D.B.; Mullen, L.K. Homeostatic control of zinc metabolism in men: Zinc excretion and balance in men fed diets low in zinc. Am. J. Clin. Nutr. 1993, 57, 557–565. [Google Scholar] [PubMed]
- Hambidge, M.; Krebs, N.F. Interrelationships of key variables of human zinc homeostasis: Relevance to dietary zinc requirements. Annu. Rev. Nutr. 2001, 21, 429–452. [Google Scholar] [CrossRef] [PubMed]
- Cousins, R.; Liuzzi, J.; Lichten, L. Mammalian zinc transport, trafficking, and signals. J. Biol. Chem. 2006, 281, 24085–24089. [Google Scholar] [CrossRef] [PubMed]
- Cousins, R.J. Gastrointestinal factors influencing zinc absorption and homeostasis. Int. J. Vitam. Nutr. Res. 2010, 80, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Manary, M.; Hotz, C.; Krebs, N.F.; Gibson, R.S.; Westcott, J.E.; Broadhead, R.L.; Hambidge, K.M. Zinc homeostasis in malawian children consuming a high-phytate, maize-based diet. Am. J. Clin. Nutr. 2002, 75, 1057–1061. [Google Scholar] [PubMed]
- Folwaczny, C. Zinc and diarrhea in infants. J. Trace Elem. Med. Biol. 1997, 11, 116–122. [Google Scholar] [CrossRef]
- Hambidge, K.M. Zinc and diarrhea. Acta Paediatr. Suppl. 1992, 381, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Baer, M.T.; King, J.C. Tissue zinc levels and zinc excretion during experimental zinc depletion in young men. Am. J. Clin. Nutr. 1984, 39, 556–570. [Google Scholar] [PubMed]
- Jackson, M.J.; Jones, D.A.; Edwards, R.H.; Swainbank, I.G.; Coleman, M.L. Zinc homeostasis in man: Studies using a new stable isotope-dilution technique. Br. J. Nutr. 1984, 51, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Turnlund, J.R.; King, J.C.; Keyes, W.R.; Gong, B.; Michel, M.C. A stable isotope study of zinc absorption in young men: Effects of phytate and alpha-cellulose. Am. J. Clin. Nutr. 1984, 40, 1071–1077. [Google Scholar] [PubMed]
- Lowe, N.; Nicola, M.L.; David, M.S.; Leslie, R.W.; Julie, S.M. A compartmental model of zinc metabolism in healthy women using oral and intravenous stable isotope tracers. Am. J. Clin. Nutr. 1997, 65, 1810. [Google Scholar] [PubMed]
- Miller, L.V.; Krebs, N.F.; Hambidge, K.M. Development of a compartmental model of human zinc metabolism: Identifiability and multiple studies analyses. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, 1671–1684. [Google Scholar]
- Berman, M. Kinetic analysis and modeling: Theory and applications to lipoproteins. In Lipoprotein Kinetics and Modeling; Berman, M.G.S., Howard, B.V., Eds.; Academic: New York, NY, USA, 1982; pp. 3–36. [Google Scholar]
- Stefanidou, M.; Maravelias, C.; Dona, A.; Spiliopoulou, C. Zinc: A multipurpose trace element. Arch. Toxicol. 2006, 80, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.V.; Hambidge, K.M.; Naake, V.L.; Hong, Z.Y. Size of the zinc pools that exchange rapidly with plasma zinc in humans—Alternative techniques for measuring and relation to dietary zinc intake. J. Nutr. 1994, 124, 268–276. [Google Scholar] [PubMed]
- Abrams, S.A. Assessing mineral metabolism in children using stable isotopes. Pediatr. Blood Cancer 2008, 50, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Condomina, J.; Zornoza-Sabina, T.; Granero, L.; Polache, A. Kinetics of zinc transport in vitro in rat small intestine and colon: Interaction with copper. Eur. J. Pharm. Sci 2002, 16, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Chiplonkar, S.; Agte, V. Predicting bioavailable zinc from lower phytate forms, folic acid and their interactions with zinc in vegetarian meals. J. Am. Coll. Nutr. 2006, 25, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Tran, C.; Miller, L.; Krebs, N.; Hambidge, K. Zinc absorption as a function of the dose of zinc sulfate in aqueous solution. Am. J. Clin. Nutr. 2004, 80, 1570–1573. [Google Scholar] [PubMed]
- Istfan, N.W.; Janghorbani, M.; Young, V.R. Absorption of stable70 zn in healthy young men in relation to zinc intake. Am. J. Clin. Nutr. 1983, 38, 187–194. [Google Scholar] [PubMed]
- Dunn, M.A.; Cousins, R.J. Kinetics of zinc-metabolism in the rat—Effect of dibutyryl camp. Am. J. Physiol. 1989, 256, E420–E430. [Google Scholar] [PubMed]
- Miller, L.V.; Krebs, N.F.; Hambidge, K.M. Human Zinc Metabolism: Advances in the Modeling of Stable Isotope Data; Plenum Press Div Plenum Publishing Corp: New York, NY, USA, 1998; Volume 445, pp. 253–269. [Google Scholar]
- Wastney, M.E.; Gokmen, I.G.; Aamodt, R.L.; Rumble, W.F.; Gordon, G.E.; Henkin, R.I. Kinetic-analysis of zinc-metabolism in humans after simultaneous administration of zn-65 and zn-70. Am. J. Physiol. 1991, 260, R134–R141. [Google Scholar] [PubMed]
- Wastney, M.E.; Angelus, P.; Barnes, R.M.; Subramanian, K.N.S. Zinc kinetics in preterm infants: A compartmental model based on stable isotope data. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 1996, 271, R1452–R1459. [Google Scholar]
- Wastney, M. Zinc absorption in humans determined using in vivo tracer studies and kinetic analysis. In Mineral Absorption in the Monogastric GI Tract; Dintzis, F., Laszlo, J., Eds.; Springer US: New York, NY, USA, 1989; volume 249, pp. 13–25. [Google Scholar]
- House, W.A.; Wastney, M.E. Compartmental analysis of zinc kinetics in mature male rats. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 1997, 42, R1117–R1125. [Google Scholar]
- Lönnerdal, B.; Bell, J.G.; Hendrickx, A.G.; Burns, R.A. Effect of phytate removal on zinc absorption from soy formula. Am. J. Clin. Nutr. 1988, 48, 1301–1306. [Google Scholar] [PubMed]
- Hambidge, K.M.; Huffer, J.W.; Raboy, V.; Grunwald, G.K. Zinc absorption from low-phytate hybrids of maize and their wild-type isohybrids. Am. J. Clin. Nutr. 2004, 79, 1053–1059. [Google Scholar] [PubMed]
- Fredlund, K.; Isaksson, M.; Rossander-Hulthén, L.; Almgren, A. Absorption of zinc and retention of calcium: Dose-dependent inhibition by phytate. J. Trace Elem. Med. Biol. 2006, 20, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Hambidge, K.; Krebs, N.; Westcott, J.; Miller, L. Changes in zinc absorption during development. J. Pediatr. 2006, 149, S64–S68. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.; Krebs, N.F.; Hambidge, K.M. A mathematical model of zinc absorption in humans as a function of dietary zinc. J. Nutr. 2007, 137, 135–141. [Google Scholar] [PubMed]
- Hambidge, K.; Miller, L.; Tran, C.; Krebs, N. Measurements of zinc absorption: Application and interpretation in research designed to improve human zinc nutriture. Int. J. Vitam. Nutr. Res. 2005, 75, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Bird, S.M.; Black, R.E.; Brown, K.H.; Gardner, J.M.; Hidayat, A.; Khatun, F.; Martorell, R.; Ninh, N.X.; Penny, M.E.; et al. Therapeutic effects of oral zinc in acute and persistent diarrhea in children in developing countries: Pooled analysis of randomized controlled trials. Am. J. Clin. Nutr. 2000, 72, 1516–1522. [Google Scholar] [PubMed]
- Black, R.E. Zinc deficiency, infectious disease and mortality in the developing world. J. Nutr. 2003, 133, 1485S–1489S. [Google Scholar] [PubMed]
- Brown, K.H.; Peerson, J.M.; Allen, L.H. Effect of Zinc Supplementation on Children’s Growth: A Meta-Analysis of Intervention Trials; Karger: Basel, Switzerland, 1998; pp. 76–83. [Google Scholar]
- Rahman, M.M.; Vermund, S.H.; Wahed, M.A.; Fuchs, G.J.; Baqui, A.H.; Alvarez, J.O. Simultaneous zinc and vitamin a supplementation in bangladeshi children: Randomised double blind controlled trial. BMJ 2001, 323, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.J.; Bates, P.H.; Dardenne, M.; Prentice, A.; Lunn, P.G.; Northrop-Clewes, C.A.; Hoare, S.; Cole, T.J.; Horan, S.J.; Longman, S.C.; et al. A trial of zinc supplementation in young rural gambian children. Br. J. Nutr. 1993, 69, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Valberg, L.S.; Flanagan, P.R.; Chamberlain, M.J. Effects of iron, tin, and copper on zinc absorption in humans. Am. J. Clin. Nutr. 1984, 40, 536–541. [Google Scholar] [PubMed]
- Sandström, B.; Davidsson, L.; Cederblad, A.; Lönnerdal, B. Oral iron, dietary ligands and zinc absorption. J .Nutr. 1985, 115, 411–414. [Google Scholar] [PubMed]
- Imdad, A.; Bhutta, Z. Effect of preventive zinc supplementation on linear growth in children under 5 years of age in developing countries: A meta-analysis of studies for input to the lives saved tool. BMC Public Health 2011, 11, S22. [Google Scholar] [CrossRef] [PubMed]
- Lind, T.; Lönnerdal, B.; Stenlund, H.; Gamayanti, I.L. A community-based randomized controlled trial of iron and zinc supplementation in indonesian infants. Am. J. Clin. Nutr. 2004, 80, 729–736. [Google Scholar] [PubMed]
- Sheikh, A.; Shamsuzzaman, S.; Ahmad, S.M.; Nasrin, D.; Nahar, S.; Alam, M.M.; Al Tarique, A.; Begum, Y.A.; Qadri, S.S.; Chowdhury, M.I.; et al. Zinc influences innate immune responses in children with enterotoxigenic escherichia coli-induced diarrhea. J. Nutr. 2010, 140, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Wuehler, S.E.; Sempertegui, F.; Brown, K.H. Dose-response trial of prophylactic zinc supplements, with or without copper, in young ecuadorian children at risk of zinc deficiency. Am. J. Clin. Nutr. 2008, 87, 723–733. [Google Scholar] [PubMed]
- Boran, P.; Tokuc, G.; Vagas, E.; Oktem, S.; Gokduman, M. Impact of zinc supplementation in children with acute diarrhoea in turkey. Arch. Dis. Child. 2006, 91, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Sandström, B.; Arvidsson, B.; Cederblad, A.; Björn-Rasmussen, E. Zinc absorption from composite meals. I. The significance of wheat extraction rate, zinc, calcium, and protein content in meals based on bread. Am. J. Clin. Nutr. 1980, 33, 739–745. [Google Scholar] [PubMed]
- Hunt, J.; Beiseigel, M.; Johnson, L.K. Adaptation in human zinc absorption as influenced by dietary zinc and bioavailability. Am. J. Clin. Nutr. 2008, 2008, 1336–1345. [Google Scholar]
- August, D.; Janghorbani, M.; Young, V.R. Determination of zinc and copper absorption at three dietary zn-cu ratios by using stable isotope methods in young adult and elderly subjects. Am. J. Clin. Nutr. 1989, 50, 1457–1463. [Google Scholar] [PubMed]
- Baqui, A.H.; Zaman, K.; Persson, L.A.; El Arifeen, S.; Yunus, M.; Begum, N.; Black, R.E. Simultaneous weekly supplementation of iron and zinc is associated with lower morbidity due to diarrhea and acute lower respiratory infection in bangladeshi infants. J. Nutr. 2003, 133, 4150–4157. [Google Scholar] [PubMed]
- Bhandari, N.; Bahl, R.; Taneja, S.; Strand, T.; Molbak, K.; Ulvik, R.J.; Sommerfelt, H.; Bhan, M.K. Substantial reduction in severe diarrheal morbidity by daily zinc supplementation in young north indian children. Pediatrics 2002, 109, e86. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.N.; Rajendran, K.; Mondal, S.K.; Ghosh, S.; Bhattacharya, S.K. Operational feasibility of implementing community-based zinc supplementation: Impact on childhood diarrheal morbidity. Pediatr. Infect. Dis. J. 2007, 26, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Ninh, N.X.; Thissen, J.P.; Collette, L.; Gerard, G.; Khoi, H.H.; Ketelslegers, J.M. Zinc supplementation increases growth and circulating insulin-like growth factor i (igf-i) in growth-retarded vietnamese children. Am. J. Clin. Nutr. 1996, 63, 514–519. [Google Scholar] [PubMed]
- Penny, M.E.; Marin, R.M.; Duran, A.; Peerson, J.M.; Lanata, C.F.; Lonnerdal, B.; Black, R.E.; Brown, K.H. Randomized controlled trial of the effect of daily supplementation with zinc or multiple micronutrients on the morbidity, growth, and micronutrient status of young peruvian children. Am. J. Clin. Nutr. 2004, 79, 457–465. [Google Scholar] [PubMed]
- Umeta, M.; West, C.E.; Haidar, J.; Deurenberg, P.; Hautvast, J.G. Zinc supplementation and stunted infants in ethiopia: A randomised controlled trial. Lancet 2000, 355, 2021–2026. [Google Scholar] [CrossRef]
- Walker, C.L.; Bhutta, Z.A.; Bhandari, N.; Teka, T.; Shahid, F.; Taneja, S.; Black, R.E. Zinc during and in convalescence from diarrhea has no demonstrable effect on subsequent morbidity and anthropometric status among infants <6 mo of age. Am. J. Clin. Nutr. 2007, 85, 887–894. [Google Scholar]
- Luabeya, K.K.; Mpontshane, N.; Mackay, M.; Ward, H.; Elson, I.; Chhagan, M.; Tomkins, A.; Van den Broeck, J.; Bennish, M.L. Zinc or multiple micronutrient supplementation to reduce diarrhea and respiratory disease in south african children: A randomized controlled trial. PLoS ONE 2007, 2, e541. [Google Scholar] [CrossRef] [PubMed]
- Taneja, S.; Bhandari, N.; Rongsen-Chandola, T.; Mahalanabis, D.; Fontaine, O.; Bhan, M.K. Effect of zinc supplementation on morbidity and growth in hospital-born, low-birth-weight infants. Am. J. Clin. Nutr. 2009, 90, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Rosado, J.L.; Lopez, P.; Munoz, E.; Martinez, H.; Allen, L.H. Zinc supplementation reduced morbidity, but neither zinc nor iron supplementation affected growth or body composition of mexican preschoolers. Am. J. Clin. Nutr. 1997, 65, 13–19. [Google Scholar] [PubMed]
- Sur, D.; Gupta, D.; Mondal, S.; Ghosh, S.; Manna, B.; Rajendran, K.; Bhattacharya, S.K. Impact of zinc supplementation on diarrheal morbidity and growth pattern of low birth weight infants in kolkata, india: A randomized, double-blind, placebo-controlled, community-based study. Pediatrics 2003, 112, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Tielsch, J.; Khatry, S.K.; Stolzfus, R.J.; Katz, J.; Black, R. Effect of daily zinc supplementation on child mortality in southern nepal: A community-based, cluster randomised, placebo-controlled trial. Lancet 2007, 370, 1230–1239. [Google Scholar] [CrossRef]
- Brown, K.H.; Wessells, K.R.; Hess, S.Y. Zinc bioavailability from zinc-fortified foods. Int. J. Vitam. Nutr. Res. 2007, 77, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Hess, S.Y.; Brown, K.H. Impact of zinc fortification on zinc nutrition. Food Nutr. Bull. 2009, 30, S79–S107. [Google Scholar] [PubMed]
- Hotz, C.; DeHaene, J.; Woodhouse, L.; Villapando, S.; Rivera, A.; King, J. Zinc absorption from zinc oxide, zinc sulfate, zinc oxide + edta, or sodium-zinc edta does not differ when added as fortificants to maize tortillas. J. Nutr. 2005, 135, 1102–1105. [Google Scholar] [PubMed]
- Lopez de Romana, D.; Lonnerdal, B.; Brown, K.H. Absorption of zinc from wheat products fortified with iron and either zinc. Am. J. Clin. Nutr. 2003, 78, 279–283. [Google Scholar] [PubMed]
- Herman, S.; Griffin, I.J.; Suwarti, S.; Ernawati, F.; Permaesih, D.; Pambudi, D.; Abrams, S.A. Cofortification of iron-fortified flour with zinc sulfate, but not zinc oxide, decreases iron absorption in indonesian children. Am. J. Clin. Nutr. 2002, 76, 813–817. [Google Scholar] [PubMed]
- Davidsson, L.; Ziegler, E.; Zeder, C.; Walczyk, T.; Hurrell, R. Sodium iron edta [nafe(iii)edta] as a food fortificant: Erythrocyte incorporation of iron and apparent absorption of zinc, copper, calcium, and magnesium from a complementary food based on wheat and soy in healthy infants. J. Nutr. 2005, 81, 104–109. [Google Scholar]
- Lowe, N.M.; Fekete, K.; Decsi, T. Methods of assessment of zinc status in humans: A systematic review. Am. J. Clin. Nutr. 2009, 89, 2040S–2051S. [Google Scholar] [CrossRef] [PubMed]
- Ryu, M.S.; Guthrie, G.J.; Maki, A.B.; Aydemir, T.B.; Cousins, R.J. Proteomic analysis shows the upregulation of erythrocyte dematin in zinc-restricted human subjects. Am. J. Clin. Nutr. 2012, 95, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.B.; Aydemir, T.B.; Guthrie, G.J.; Samuelson, D.A.; Chang, S.M.; Cousins, R.J. Gastric and colonic zinc transporter zip11 (slc39a11) in mice responds to dietary zinc and exhibits nuclear localization. J. Nutr. 2013, 143, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Liuzzi, J.P.; Bobo, J.A.; Lichten, L.A.; Samuelson, D.A.; Cousins, R.J. Responsive transporter genes within the murine intestinal-pancreatic axis form a basis of zinc homeostasis. Proc. Natl. Acad. Sci. USA 2004, 101, 14355–14360. [Google Scholar] [CrossRef] [PubMed]
- Bales, C.W.; DiSilvestro, R.A.; Currie, K.L.; Plaisted, C.S.; Joung, H.; Galanos, A.N.; Lin, P.H. Marginal zinc deficiency in older adults: Responsiveness of zinc status indicators. J. Am. Coll. Nutr. 1994, 13, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Milne, D.B.; Davis, C.D.; Nielsen, F.H. Low dietary zinc alters indices of copper function and status in postmenopausal women. Nutrition 2001, 17, 701–708. [Google Scholar] [CrossRef]
- Grider, A.; Wickwire, K.; Ho, E.; Chung, C.S.; King, J. Dietary zinc depletion and repletion affects plasma proteins: An analysis of the plasma proteome. Biometals 2013, 26, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, M.S.; Langkamp-Henken, B.; Chang, S.M.; Shankar, M.N.; Cousins, R.J. Genomic analysis, cytokine expression, and microrna profiling reveal biomarkers of human dietary zinc depletion and homeostasis. Proc. Natl. Acad. Sci. USA 2011, 108, 20970–20975. [Google Scholar] [CrossRef] [PubMed]
- Reed, S.; Qin, X.; Ran-Ressler, R.; Brenna, J.T.; Glahn, R.P.; Tako, E. Dietary zinc deficiency affects blood linoleic acid: Dihomo-gamma-linolenic acid (la:Dgla) ratio; a sensitive physiological marker of zinc status in vivo (gallus gallus). Nutrients 2014, 6, 1164–1180. [Google Scholar] [CrossRef] [PubMed]
- Faure, P.; Ducros, V.; Couzy, F.; Favier, A.; Ferry, M. Rapidly exchangeable pool study of zinc in free-living or institutionalized elderly women. Nutrition 2005, 21, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Lowe, N.M. In search of a reliable marker of zinc status-are we nearly there yet? Nutrition 2005, 21, 883–884. [Google Scholar] [CrossRef] [PubMed]
- Sturniolo, G.C.; Molokhia, M.M.; Shields, R.; Turnberg, L.A. Zinc absorption in crohn’s disease. Gut 1980, 21, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Ariff, S.; Krebs, N.F.; Soofi, S.; Westcott, J.; Bhatti, Z.; Tabassum, F.; Bhutta, Z.A. Absorbed zinc and exchangeable zinc pool size are greater in pakistani infants receiving traditional complementary foods with zinc-fortified micronutrient powder. J. Nutr. 2014, 144, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Esamai, F.; Liechty, E.; Ikemeri, J.; Westcott, J.; Kemp, J.; Culbertson, D.; Miller, L.V.; Hambidge, K.M.; Krebs, N.F. Zinc absorption from micronutrient powder is low but is not affected by iron in kenyan infants. Nutrients 2014, 6, 5636–5651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zlotkin, S.H.; Schauer, C.; Owusu Agyei, S.; Wolfson, J.; Tondeur, M.C.; Asante, K.P.; Newton, S.; Serfass, R.E.; Sharieff, W. Demonstrating zinc and iron bioavailability from intrinsically labeled microencapsulated ferrous fumarate and zinc gluconate sprinkles in young children. J. Nutr. 2006, 136, 920–925. [Google Scholar] [PubMed]
- Hettiarachchi, M.; Hilmers, D.; Liyanage, C.; Abrams, S. Na2edta enhances the absorption of iron and zinc from fortified rice flour in srilankan children. J. Nutr. 2004, 134, 3031–3036. [Google Scholar] [PubMed]
- Kennedy, G.; Hambidge, K.M.; Manary, M. A reduced phytate diet does not reduce endogenous fecal zinc in children on a habitual high-phytate diet. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 678–679. [Google Scholar] [CrossRef] [PubMed]
- Manary, M.; Hotz, C.; Krebs, N.F.; Gibson, R.S.; Hambidge, K.M.; Westcott, J.E.; Broadhead, R.L. Dietary phytate reduction improves zinc absorption in malawian children recovering from tuberculosis but not in well children. J. Nutr. 2000, 130, 2959–2964. [Google Scholar] [PubMed]
- Mazariegos, M.; Hambidge, K.M.; Krebs, N.F.; Westcott, J.E.; Sian, L.; Grunwald, G.K.; Campos, R.; Barahona, B.; Raboy, V.; Solomons, N. Zinc absorption in guatemalan schoolchildren fed normal or low-phytate maize. Am. J. Clin. Nutr. 2006, 83, 59–64. [Google Scholar] [PubMed]
- Hettiarachchi, M.; Liyanage, C.; Hilmers, D.; Griffin, I.; Abrams, S.A. Changing the zinc:Iron ratio in a cereal-based nutritional supplement has no effect on percent absorption of iron and zinc in sri lankan children. Br. J. Nutr. 2010, 103, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Woodhouse, L.R.; Hossain, M.B.; Ahmed, T.; Huda, M.N.; Ahmed, T.; Peerson, J.M.; Hotz, C.; Brown, K.H. Total zinc absorption from a diet containing either conventional rice or higher-zinc rice does not differ among bangladeshi preschool children. J. Nutr. 2013, 143, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Kodkany, B.S.; Bellad, R.M.; Mahantshetti, N.S.; Westcott, J.E.; Krebs, N.F.; Kemp, J.F.; Hambidge, K.M. Biofortification of pearl millet with iron and zinc in a randomized controlled trial increases absorption of these minerals above physiologic requirements in young children. J. Nutr. 2013, 143, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wu, J.; Ren, T.; Wang, R.; Li, W.; Piao, J.; Wang, J.; Yang, X. Effect of nafeedta-fortified soy sauce on zinc absorption in children. Food Funct. 2015, 6, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Nair, K.M.; Brahmam, G.N.; Radhika, M.S.; Dripta, R.C.; Ravinder, P.; Balakrishna, N.; Chen, Z.; Hawthorne, K.M.; Abrams, S.A. Inclusion of guava enhances non-heme iron bioavailability but not fractional zinc absorption from a rice-based meal in adolescents. J. Nutr. 2013, 143, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Chassard, D.; Kanis, R.; Namour, F.; Evene, E.; Ntssikoussalabongui, B.; Schmitz, V. A single centre, open-label, cross-over study of pharmacokinetics comparing topical zinc/clindamycin gel (zindaclin) and topical clindamycin lotion (dalacin T) in subjects with mild to moderate acne. J. Dermatol. Treat. 2006, 17, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Jia, Y.Y.; Li, F.; Liu, W.X.; Lu, C.T.; Zhu, Y.R.; Yang, J.; Ding, L.K.; Yang, L.; Wen, A.D. The effect of staggered administration of zinc sulfate on the pharmacokinetics of oral cephalexin. Br. J. Clin. Pharmacol. 2012, 73, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Lowe, N.M.; Woodhouse, L.R.; King, J.C. A comparison of the short-term kinetics of zinc metabolism in women during fasting and following a breakfast meal. Br. J. Nutr. 1998, 80, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, K.; Egger, N.G.; Ramanujam, V.M.; Alcock, N.W.; Dayal, H.H.; Penland, J.G.; Sandstead, H.H. Association between plasma zinc concentration and zinc kinetic parameters in premenopausal women. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E1010–E1020. [Google Scholar] [CrossRef] [PubMed]
- Feillet-Coudray, C.; Meunier, N.; Rambeau, M.; Brandolini-Bunlon, M.; Tressol, J.C.; Andriollo, M.; Mazur, A.; Cashman, K.D.; Coudray, C. Long-term moderate zinc supplementation increases exchangeable zinc pool masses in late-middle-aged men: The zenith study. Am. J. Clin. Nutr. 2005, 82, 103–110. [Google Scholar] [PubMed]
- Vale, S.H.; Leite, L.D.; Alves, C.X.; Dantas, M.M.; Costa, J.B.; Marchini, J.S.; Franca, M.C.; Brandao-Neto, J. Zinc pharmacokinetic parameters in the determination of body zinc status in children. Eur. J. Clin. Nutr. 2014, 68, 203–208. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, C.D.; Gopalsamy, G.L.; Mortimer, E.K.; Young, G.P. The Potential for Zinc Stable Isotope Techniques and Modelling to Determine Optimal Zinc Supplementation. Nutrients 2015, 7, 4271-4295. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7064271
Tran CD, Gopalsamy GL, Mortimer EK, Young GP. The Potential for Zinc Stable Isotope Techniques and Modelling to Determine Optimal Zinc Supplementation. Nutrients. 2015; 7(6):4271-4295. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7064271
Chicago/Turabian StyleTran, Cuong D., Geetha L. Gopalsamy, Elissa K. Mortimer, and Graeme P. Young. 2015. "The Potential for Zinc Stable Isotope Techniques and Modelling to Determine Optimal Zinc Supplementation" Nutrients 7, no. 6: 4271-4295. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7064271