Efficacy of Aloe Vera Supplementation on Prediabetes and Early Non-Treated Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
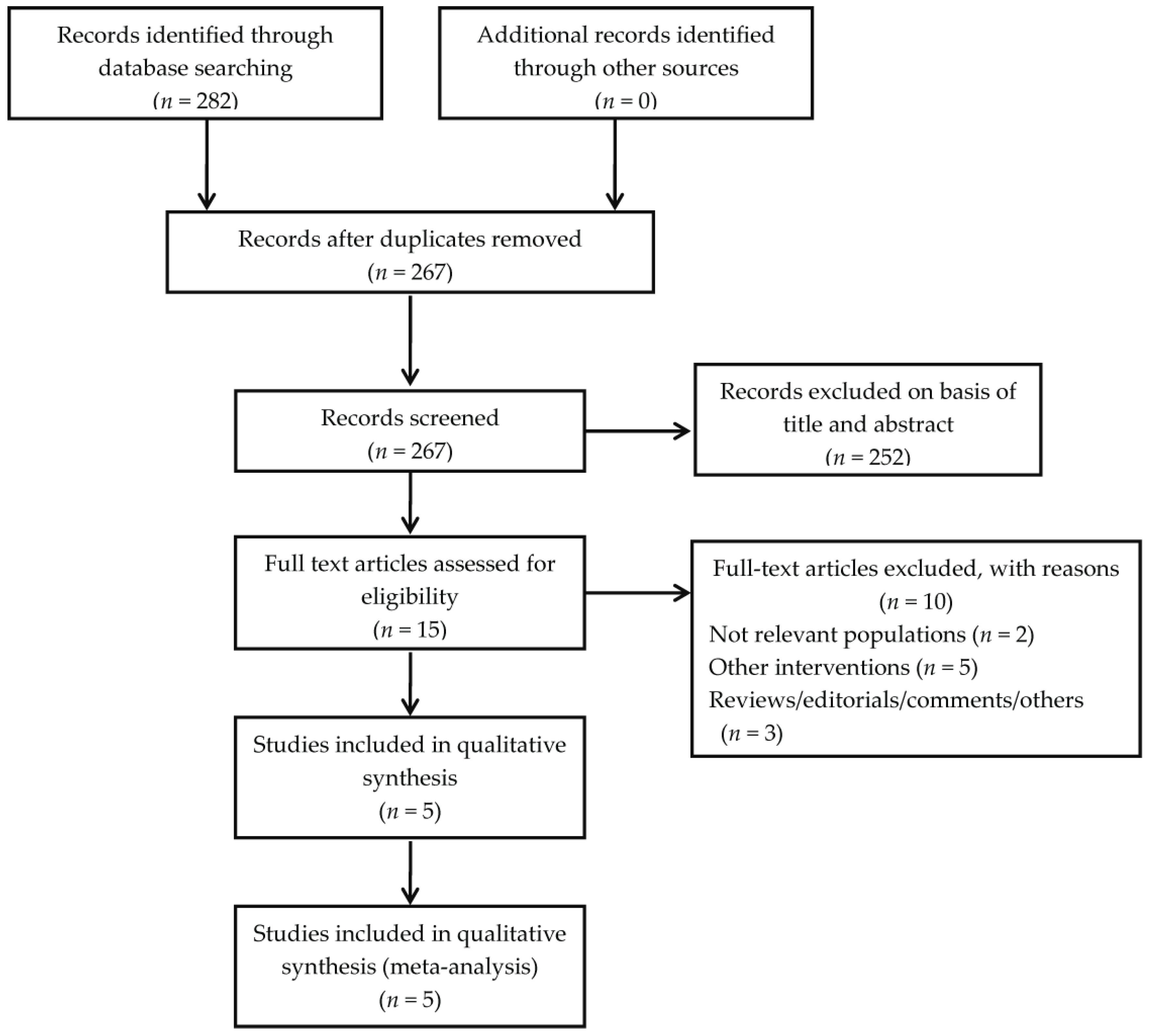
3.1. Eligible Studies and Baseline Characteristics
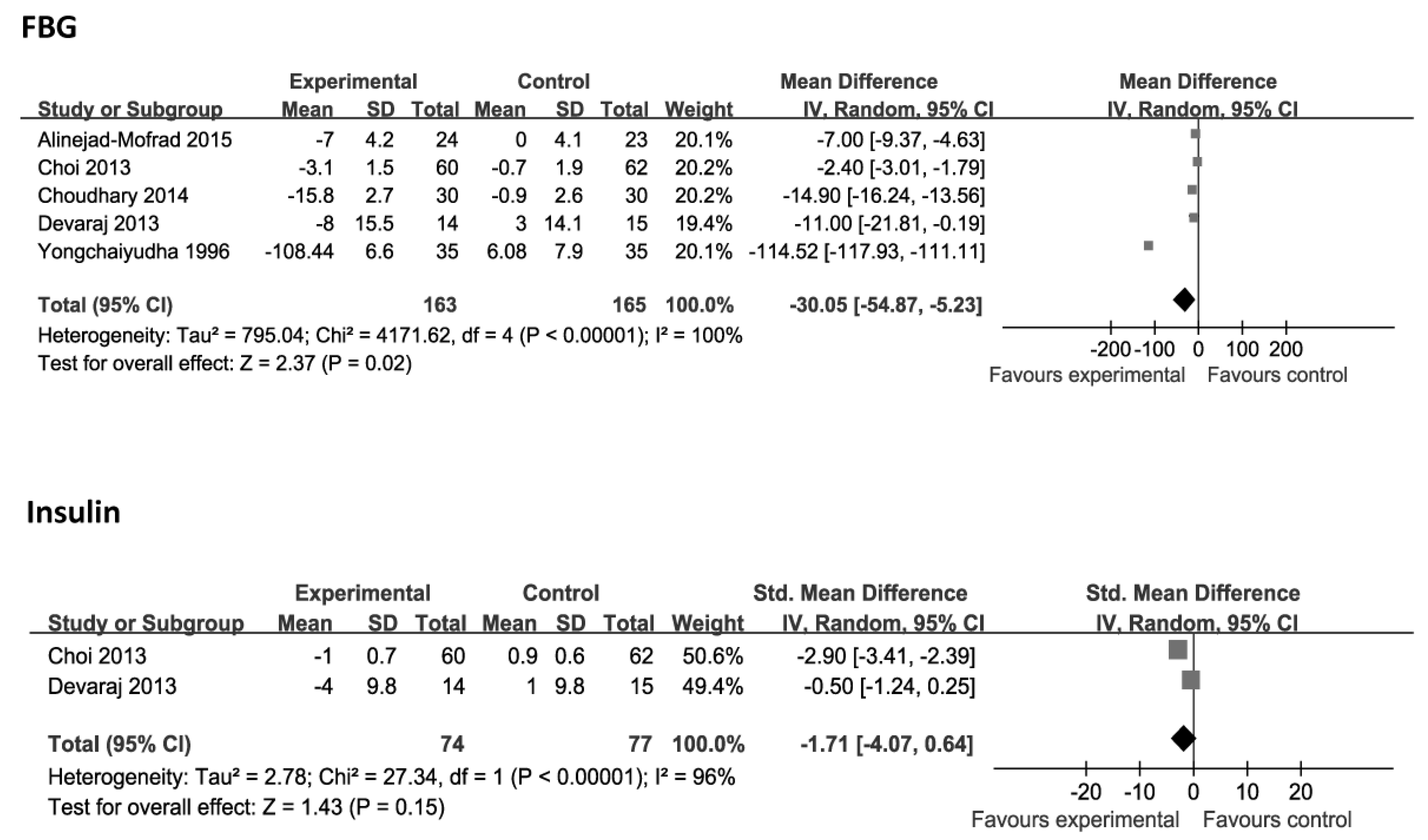
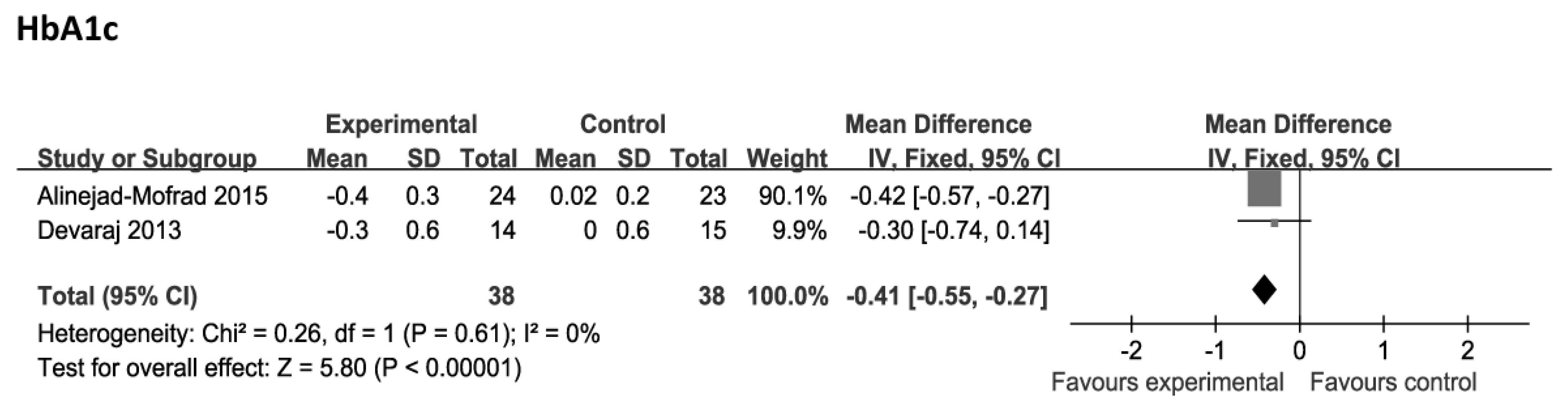
3.2. Meta-Analyses of Primary Outcomes
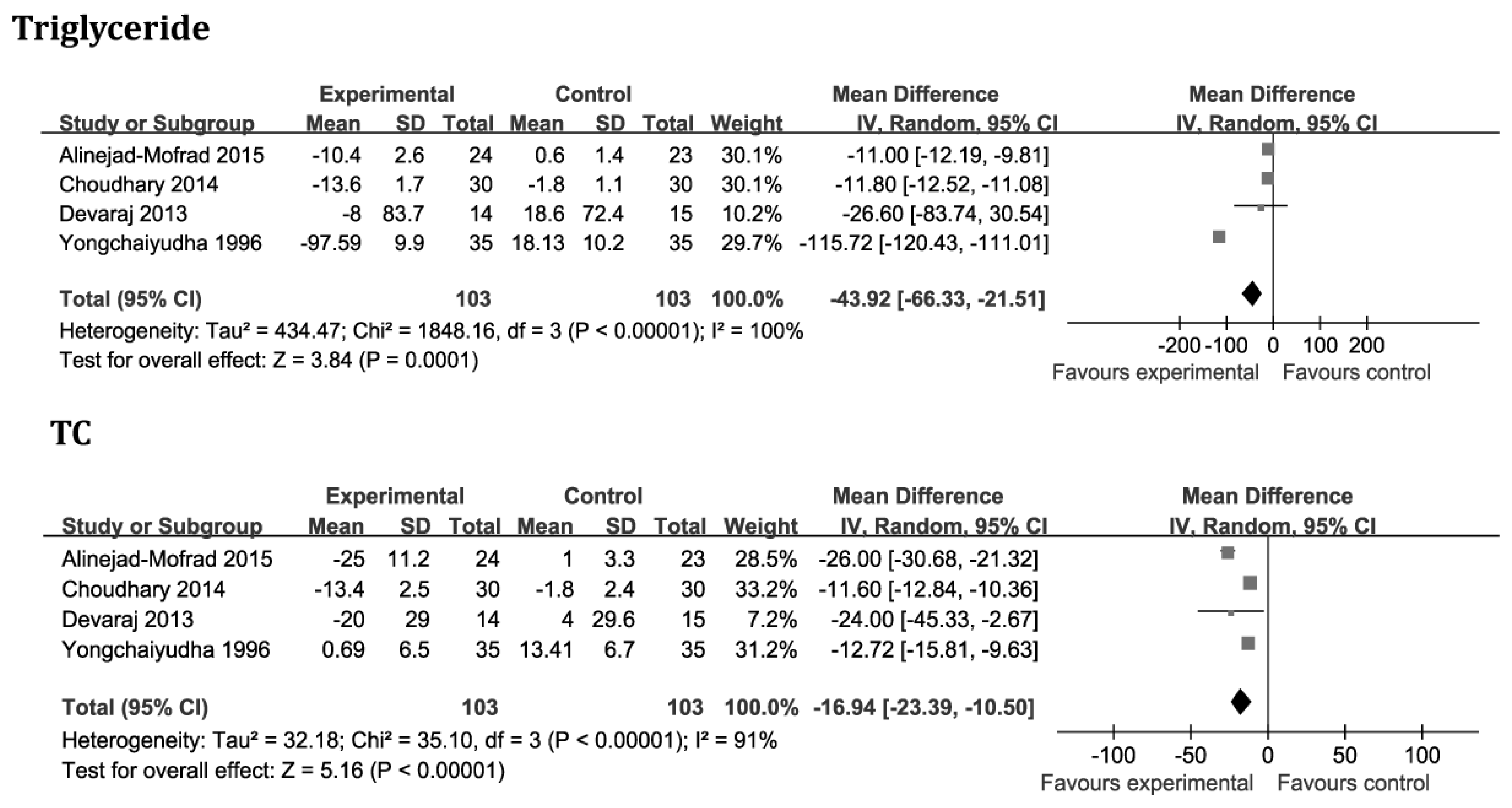
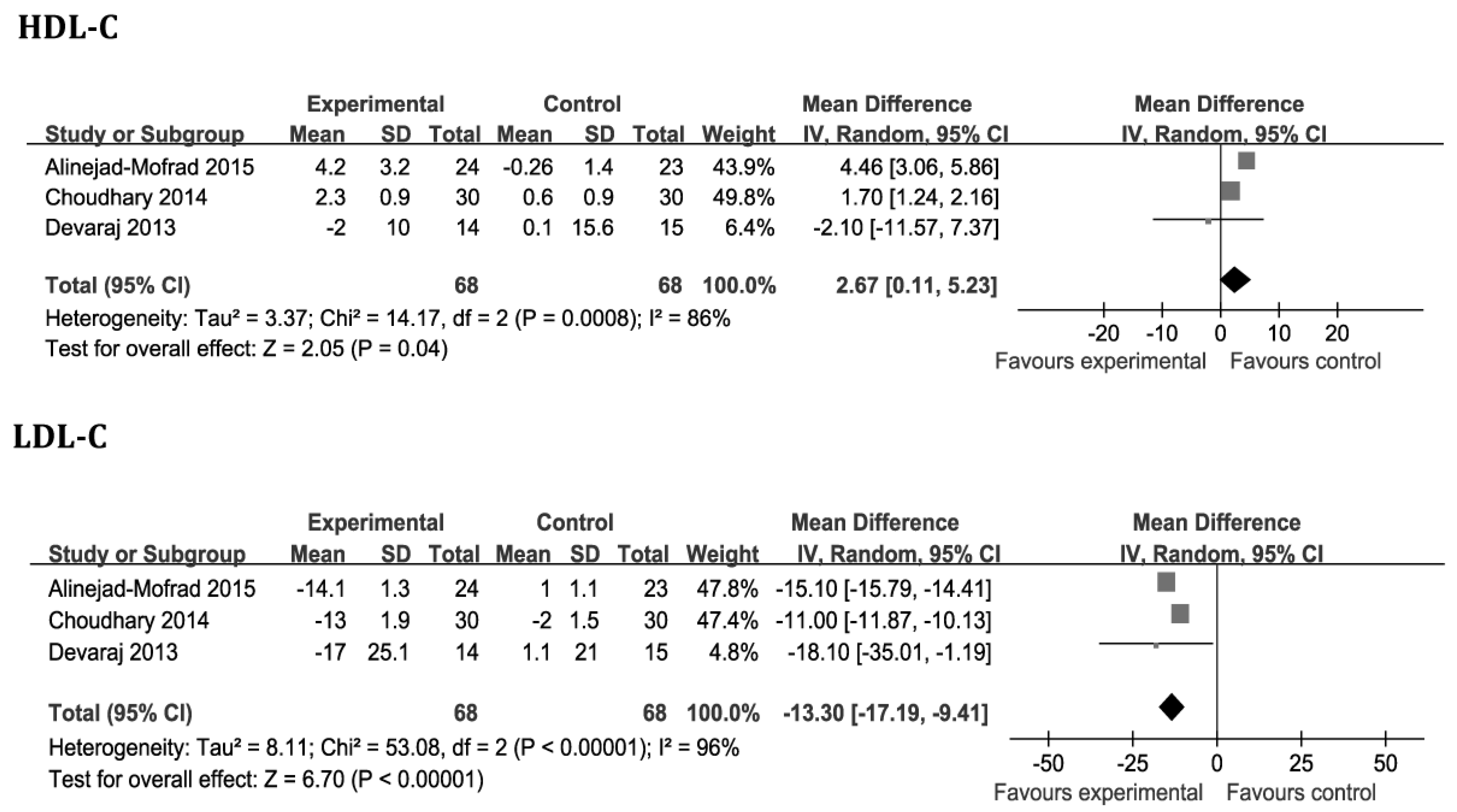
3.3. Meta-Analyses of Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| FBG | Fasting blood glucose |
| HbA1c | Hemoglobin A1c |
| HDL-C | High density lipoprotein-cholesterol |
| ITT | Intention to treat |
| LDL-C | Low density lipoprotein-cholesterol |
| RCT | Randomized clinical trial |
| SMD | Standardized mean difference |
| T2DM | Type 2 diabetes mellitus |
| TC | Total cholesterol |
| WMD | Weighed mean difference |
References
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes-2014. Diabetes Care 2015, 38 (Suppl. S1), S31–S33. [Google Scholar]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef]
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008, 31, 596–615. [Google Scholar]
- Hou, Q.; Li, Y.; Li, L.; Cheng, G.; Sun, X.; Li, S.; Tian, H. The Metabolic Effects of Oats Intake in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 10369–10387. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.I.; Mishra, N. Traditional Indian medicines used for the management of diabetes mellitus. J. Diabetes Res. 2013, 2013, 712092. [Google Scholar] [CrossRef] [PubMed]
- Modak, M.; Dixit, P.; Londhe, J.; Ghaskadbi, S.; Devasagayam, T.P. Indian herbs and herbal drugs used for the treatment of diabetes. J. Clin. Biochem. Nutr. 2007, 40, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Surjushe, A.; Vasani, R.; Saple, D.G. Aloe vera: A short review. Indian J. Dermatol. 2008, 53, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Shelton, R.M. Aloe vera. Its chemical and therapeutic properties. Int. J. Dermatol. 1991, 30, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Hamman, J.H. Composition and applications of Aloe vera leaf gel. Molecules 2008, 13, 1599–1616. [Google Scholar] [CrossRef] [PubMed]
- Radha, M.H.; Laxmipriya, N.P. Evaluation of biological properties and clinical effectiveness of Aloe vera: A systematic review. J. Tradit. Complement. Med. 2014, 5, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Ulbricht, C.; Armstrong, J.; Basch, E.; Basch, S.; Bent, S.; Dacey, C.; Dalton, S.; Foppa, I.; Giese, N.; Hammerness, P.; et al. An evidence-based systematic review of Aloe vera by the natural standard research collaboration. J. Herb. Pharmacother. 2007, 7, 279–323. [Google Scholar] [CrossRef] [PubMed]
- Rajasekaran, S.; Ravi, K.; Sivagnanam, K.; Subramanian, S. Beneficial effects of aloe vera leaf gel extract on lipid profile status in rats with streptozotocin diabetes. Clin. Exp. Pharmacol. Physiol. 2006, 33, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Kim, H.; Kwon, J.; Lee, S.; Kong, H.; Im, S.A.; Lee, Y.H.; Lee, Y.R.; Oh, S.T.; Jo, T.H.; et al. Hypoglycemic and hypolipidemic effects of processed Aloe vera gel in a mouse model of non-insulin-dependent diabetes mellitus. Phytomedicine 2009, 16, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Yagi, A.; Hegazy, S.; Kabbash, A.; Wahab, E.A. Possible hypoglycemic effect of Aloe vera L. high molecular weight fractions on type 2 diabetic patients. Saudi Pharm. J. 2009, 17, 209–215. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. Report of a WHO Consultation. Part 1: Diagnosis and Classification of Diabetes Mellitus; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Yongchaiyudha, S.; Rungpitarangsi, V.; Bunyapraphatsara, N.; Chokechaijaroenporn, O. Antidiabetic activity of Aloe vera L. juice. I. Clinical trial in new cases of diabetes mellitus. Phytomedicine 1996, 3, 241–243. [Google Scholar] [CrossRef]
- Devaraj, S.; Yimam, M.; Brownell, L.A.; Jialal, I.; Singh, S.; Jia, Q. Effects of Aloe vera supplementation in subjects with prediabetes/metabolic syndrome. Metab. Syndr. Relat. Disord. 2013, 11, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.C.; Kim, S.J.; Son, K.Y.; Oh, B.J.; Cho, B.L. Metabolic effects of aloe vera gel complex in obese prediabetes and early non-treated diabetic patients: Randomized controlled trial. Nutrition 2013, 29, 1110–1114. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, M.; Kochhar, A.; Sangha, J. Hypoglycemic and hypolipidemic effect of Aloe vera L. in non-insulin dependent diabetics. J. Food Sci. Technol. 2014, 51, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Alinejad-Mofrad, S.; Foadoddini, M.; Saadatjoo, S.A.; Shayesteh, M. Improvement of glucose and lipid profile status with Aloe vera in pre-diabetic subjects: A randomized controlled-trial. J. Diabetes Metab. Disord. 2015, 14, 22. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Muthusamy, V.S.; Sujatha, S.; Sangeetha, K.N.; Bharathi Raja, R.; Sudhagar, S.; Poornima Devi, N.; Lakshmi, B.S. Aloe emodin glycosides stimulates glucose transport and glycogen storage through PI3K dependent mechanism in L6 myotubes and inhibits adipocyte differentiation in 3T3L1 adipocytes. FEBS Lett. 2010, 584, 3170–3178. [Google Scholar] [CrossRef] [PubMed]
- Beppu, H.; Shimpo, K.; Chihara, T.; Kaneko, T.; Tamai, I.; Yamaji, S.; Ozaki, S.; Kuzuya, H.; Sonoda, S. Antidiabetic effects of dietary administration of Aloe arborescens Miller components on multiple low-dose streptozotocin-induced diabetes in mice: Investigation on hypoglycemic action and systemic absorption dynamics of aloe components. J. Ethnopharmacol. 2006, 103, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Shin, E.; Shin, S.; Kong, H.; Lee, S.; Do, S.G.; Jo, T.H.; Park, Y.I.; Lee, C.K.; Hwang, I.K.; Kim, K. Dietary Aloe Reduces Adipogenesis via the Activation of AMPK and Suppresses Obesity-related Inflammation in Obese Mice. Immune Netw. 2011, 11, 107–113. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Main Diagnoses of Study Participants | Mean FBG (mg/dL) | Mean HbA1c (%) | Mean BMI (kg/m2) | Gender (Male/Female) | Randomized/Analyzed | Daily Dosage (Formulation) | Treatment Duration (Weeks) | Main Outcomes | Adverse Events | Control for Lifestyle Factors | Randomization Appropriate | Allocation Concealed | Sample Size Determined | Groups Similar at Baseline | Blinding | ITT Analysis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yongchaiyudha, 1996 [17] | Early untreated diabetes | 250.7 | Unclear | Unclear | 50/22 | 72/70 | Two tablespoonful (juice) | 6 | Glucose and lipid profile | Unclear | Unclear | Unclear | Unclear | Unclear | Yes | Single blinding | Unclear |
| Devaraj, 2013 [18] | Prediabetes | 109 | 5.9 | 34.7 | 15/29 | 45/44 | 1.0 g (capsules) | 8 | Glucose and lipid profile | Unclear | Normal diet and exercise at least 100 min per week | Unclear | Unclear | Unclear | Yes | Double blinding | Unclear |
| Choi, 2013 [19] | Prediabetes and early untreated diabetes | 116.2 | 6.2 | 27.4 | 96/40 | 136/122 | 2.8 g (capsules) | 8 | Glucose, lipid profile and obesity-related biomarkers | One adverse event | Unclear | With the randomization code generated by software | Unclear | Unclear | Yes | Double blinding | Inadequate |
| Choudhary, 2014 [20] | Untreated diabetes | 130.8 | Unclear | Unclear | 90/0 | 90/90 | 0.2 g (powder) | 12 | Glucose, lipid profile and blood pressure | Unclear | Unclear | Unclear | Unclear | Unclear | Yes | Unclear | Unclear |
| Alinejad-Mofrad, 2015 [21] | Prediabetes | 111.1 | 6 | 28.2 | 21/49 | 72/70 | 1.0 g (capsules) | 8 | Glucose and lipid profile | Unclear | Normal diet and exercise | Blocking randomization | Unclear | Unclear | Yes | Double blinding | Unclear |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Liu, W.; Liu, D.; Zhao, T.; Tian, H. Efficacy of Aloe Vera Supplementation on Prediabetes and Early Non-Treated Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2016, 8, 388. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8070388
Zhang Y, Liu W, Liu D, Zhao T, Tian H. Efficacy of Aloe Vera Supplementation on Prediabetes and Early Non-Treated Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2016; 8(7):388. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8070388
Chicago/Turabian StyleZhang, Yiyi, Wen Liu, Dan Liu, Tieyun Zhao, and Haoming Tian. 2016. "Efficacy of Aloe Vera Supplementation on Prediabetes and Early Non-Treated Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 8, no. 7: 388. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8070388