Determination of Deoxynivalenol Biomarkers in Italian Urine Samples

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Results and Discussion
2.1. Analytical Method
2.2. In-House Validation
2.3. Description of Study Population
2.4. DON Biomarker Levels in Urine Samples
2.5. Regression Analysis Between Food Consumption and DON Level in Urine Samples
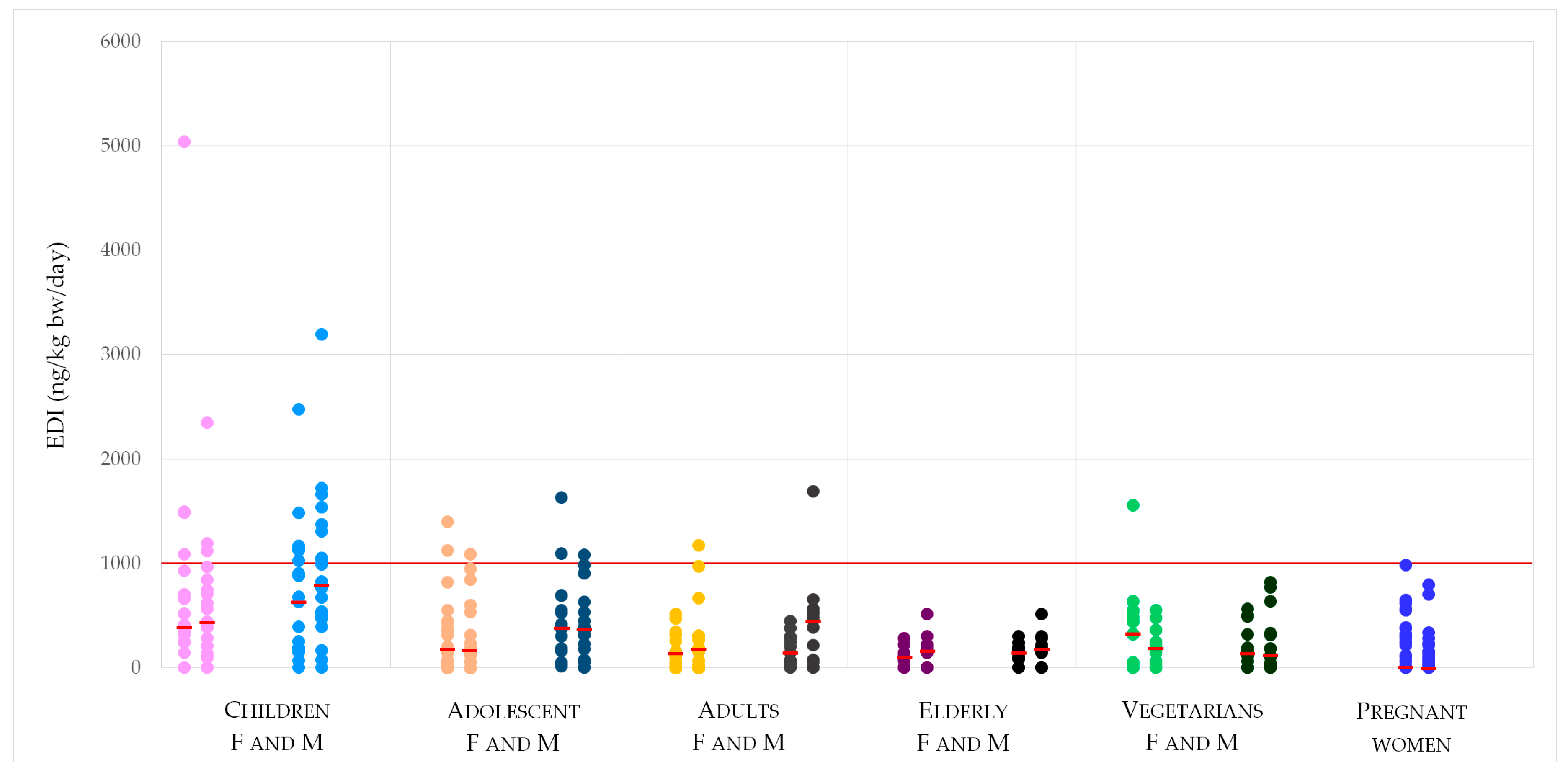
2.6. Estimated DON Daily Intake
- EDI (ng/kg bw/day);
- C = total DON concentration in the analyzed urine samples (ng/mLurine);
- bw = body weight reported in the questionnaire;
- E = urinary excretion rate of DON in 24 h, 72.3% [10]
3. Conclusions
4. Materials and Methods
4.1. Analytical Method
4.1.1. Chemicals and Reagents
4.1.2. Sample Preparation
4.1.3. LC-MS Determination
4.2. In-House Validation
4.3. Study Design
Recruitment of Participants and Urine Sample Collection
4.4. Regression Analysis Between Food Consumption and DON Levels in Urine Samples
4.4.1. Food Frequency Questionnaire and Food Diary
4.4.2. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Puntscher, H.; Kütt, M.L.; Skrinjar, P.; Mikula, H.; Podlech, J.; Fröhlich, J.; Marko, D.; Warth, B. Tracking emerging mycotoxins in food: Development of an LC-MS/MS method for free and modified Alternaria toxins. Anal. Bioanal. Chem. 2018, 410, 4481–4494. [Google Scholar] [CrossRef] [PubMed]
- Ferrigo, D.; Raiola, A.; Causin, R. Fusarium Toxins in Cereals: Occurrence, Legislation, Factors Promoting the Appearance and Their Management. Molecules 2016, 21, 627. [Google Scholar] [CrossRef] [PubMed]
- Audenaert, K.; Vanheule, A.; Höfte, M.; Haesaert, G. Deoxynivalenol: A Major Player in the Multifaceted Response of Fusarium to Its Environment. Toxins 2014, 6, 1–19. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Risks to human and animal health related to the presence of deoxynivalenol and its acetylated and modified forms in food and feed. EFSA J. 2017, 15, 4718–5093. [Google Scholar] [CrossRef]
- Commission Regulation (EC). No 1881/2006 setting maximum levels for certain contaminants in foodstuffs. Off. J. Eur. Union 2006, 364, 5–24. [Google Scholar]
- Visconti, A.; Haidukowski, M.; Pascale, M.; Silvestri, M. Reduction of Deoxynivalenol during durum wheat processing and spaghetti cooking. Toxicol. Lett. 2004, 153, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Brera, C.; Peduto, A.; Debegnach, F.; Pannunzi, E.; Prantera, E.; Gregori, E.; De Giacomo, M.; De Santis, B. Study of the influence of the milling process on the distribution of Deoxynivalenol content from the caryopsis to cooked pasta. Food Control 2012, 32, 309–312. [Google Scholar] [CrossRef]
- Stadler, D.; Lambertini, F.; Woelflingseder, L.; Schwartz-Zimmermann, H.; Marko, D.; Suman, M. The Influence of Processing Parameters on the Mitigation of Deoxynivalenol during Industrial Baking. Toxins 2019, 11, 317. [Google Scholar] [CrossRef]
- Amoriello, T.; Belocchi, A.; Quaranta, F.; Ripa, C.; Melini, F.; Aureli, G. Behaviour of durum wheat cultivars towards deoxynivalenol content: A multi-year assay in Italy. Ital. J. Agron. 2017, 13, 12–20. [Google Scholar] [CrossRef]
- Turner, P.C.; Hopton, R.P.; Lecluse, Y.; White, K.L.M.; Fisher, J.; Lebailly, P. Determinants of urinary deoxynivalenol and de-epoxy deoxynivalenol in male farmers from Normandy, France. J. Agric. Food Chem. 2010, 58, 5206–5212. [Google Scholar] [CrossRef]
- Vidal, A.; Claeys, L.; Mengelers, M.; Vanhoorne, V.; Vervaet, C.; Huybrechts, B.; De Saeger, S.; De Boevre, M. Humans significantly metabolize and excrete the mycotoxin deoxynivalenol and its modified form deoxynivalenol-3-glucoside within 24 hours. Sci. Rep. 2018, 27, 5255–5266. [Google Scholar] [CrossRef]
- Scientific Committee on Food (SCF). Opinion of the Scientific Committee on Food on Fusarium toxins. Part 6: Group Evaluation of T-2 Toxin, HT-2 Toxin, Nivalenol and Deoxynivalenol. 2002. Available online: https://ec.europa.eu/food/sites/food/files/safety/docs/sci-com_scf_out123_en.pdf (accessed on 30 May 2019).
- Joint Expert Committee on Food and Additives (JECFA). Evaluation of certain food additives and contaminants. In Report of the Seventy-Second Meeting of the Joint FAO/WHO Expert Committee on Food Additives; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Chen, L.; Yu, M.; Wu, Q.; Peng, Z.; Wang, D.; Kuca, K.; Yao, P.; Yan, H.; Nussler, A.K.; Liu, L.; et al. Gender and geographical variability in the exposure pattern and metabolism of deoxynivalenol in humans: A review. J. Appl. Toxicol. 2017, 37, 60–70. [Google Scholar] [CrossRef]
- Prelusky, D.B.; Hamilton, R.M.; Trenholm, H.L.; Miller, J.D. Tissue distribution and excretion of radioactivity following administration of 14C-labeled deoxynivalenol to White Leghorn hens. Fundam. Appl. Toxicol. 1986, 7, 635–645. [Google Scholar] [CrossRef]
- Prelusky, D.B.; Trenholm, H.L. Tissue distribution of deoxynivalenol in swine dosed intravenously. J. Sci. Food Agric. 1991, 39, 748–751. [Google Scholar] [CrossRef]
- Schwartz-Zimmermann, H.E.; Hametner, C.; Nagl, V.; Fiby, I.; Macheiner, L.; Winkler, J.; Dänicke, S.; Clark, E.; Pestka, J.J.; Berthiller, F. Glucuronidation of deoxynivalenol (DON) by different animal species: Identifcation of iso-DON glucuronides and iso-deepoxy-DON glucuronides as novel DON metabolites in pigs, rats, mice, and cows. Arch. Toxicol. 2017, 91, 3857–3872. [Google Scholar] [CrossRef]
- Warth, B.; Del Favero, G.; Wiesenberger, G.; Puntscher, H.; Woelflingseder, L.; Fruhmann, P.; Sarkanj, B.; Krska, R.; Schuhmacher, R.; Adam, G.; et al. Identification of a novel human deoxynivalenol metabolite enhancing proliferation of intestinal and urinary bladder cells. Sci. Rep. 2016, 6, 33854. [Google Scholar] [CrossRef] [Green Version]
- Schwartz-Zimmermann, H.E.; Hametner, C.; Nagl, V.; Slavik, V.; Moll, W.-D.; Berthiller, F. Deoxynivalenol (DON) sulfonates as major DON metabolites in rats: From identification to biomarker method development, validation and application. Anal. Bioanal. Chem. 2014, 406, 7911–7924. [Google Scholar] [CrossRef]
- Maul, R.; Warth, B.; Kant, J.S.; Schebb, N.H.; Krska, R.; Koch, M.; Sulyok, M. Investigation of the hepatic glucuronidation pattern of the Fusarium mycotoxin deoxynivalenol in various species. Chem. Res. Toxicol. 2012, 25, 2715–2717. [Google Scholar] [CrossRef]
- Sarkanj, B.; Warth, B.; Uhlig, S.; Abia, W.A.; Sulyok, M.; Klapec, T.; Krska, R.; Banjari, I. Urinary analysis reveals high deoxynivalenol exposure in pregnant women from Croatia. Food Chem. Toxicol. 2013, 62, 231–237. [Google Scholar] [CrossRef]
- Warth, B.; Sulyok, M.; Berthiller, F.; Schuhmacher, R.; Krska, R. New insights into the human metabolism of the Fusarium mycotoxins deoxynivalenol and zearalenone. Toxicol. Lett. 2013, 220, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Ali, N.; Blaszkewicz, M.; Degen, G.H. Assessment of deoxynivalenol exposure among Bangladeshi and German adults by a biomarker-based approach. Toxicol. Lett. 2016, 258, 20–28. [Google Scholar] [CrossRef]
- Ali, N.; Blaszkewicz, M.; Al Nahid, A.; Rahman, M.; Degen, G.H. Deoxynivalenol Exposure Assessment for Pregnant Women in Bangladesh. Toxins 2015, 7, 3845–3857. [Google Scholar] [CrossRef] [Green Version]
- Gratz, S.W.; Richardson, A.J.; Duncan, G.; Holtrop, G. Annual variation of dietary deoxynivalenol exposure during years of different Fusarium prevalence: A pilot biomonitoring study. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2014, 31, 1579–1585. [Google Scholar] [CrossRef]
- Hepworth, S.J.; Hardie, L.J.; Fraser, L.K.; Burley, V.J.; Mijal, R.S.; Wild, C.P.; Azad, R.; McKinney, P.A.; Turner, P.C. Deoxynivalenol exposure assessment in a cohort of pregnant women from Bradford, UK. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2012, 29, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Turner, P.C.; Ji, B.T.; Shu, X.O.; Zheng, W.; Chow, W.H.; Gao, Y.T.; Hardie, L.J. A biomarker survey of urinary deoxynivalenol in China: The Shanghai Women’s Health Study. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2011, 28, 1220–1223. [Google Scholar] [CrossRef]
- Wallin, S.; Gambacorta, L.; Kotova, N.; Lemming, E.W.; Nalsen, C.; Solfrizzo, M.; Olsen, M. Biomonitoring of concurrent mycotoxin exposure among adults in Sweden through urinary multi-biomarker analysis. Food Chem. Toxicol. 2015, 83, 133–139. [Google Scholar] [CrossRef]
- Turner, P.C.; Burley, V.J.; Rothwell, J.A.; White, K.L.M.; Cade, J.E.; Wild, C.P. Deoxynivalenol: Rationale for the development and application of urinary biomarker. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2008, 25, 864–871. [Google Scholar] [CrossRef]
- Solfrizzo, M.; Gambacorta, L.; Visconti, A. Assessment of multi-mycotoxin exposure in southern Italy by urinary multi-biomarker determination. Toxins 2014, 6, 523–538. [Google Scholar] [CrossRef]
- Commission Regulation (EC). No 401/2006 of 23 February 2006 laying down the methods of sampling and analysis for the official control of the levels of mycotoxins in foodstuffs. Off. J. Eur. Union 2006, 70, 12–34. [Google Scholar]
- Hines, R.N.; Sargent, D.; Autrup, H.; Birnbaum, L.S.; Brent, R.L.; Doerrer, N.G.; Cohen Hubal, E.A.; Juberg, D.R.; Laurent, C.; Luebke, R.; et al. Approaches for Assessing Risks to Sensitive Populations: Lessons Learned from Evaluating Risks in the Pediatric Population. Toxicol. Sci. 2010, 113, 4–26. [Google Scholar] [CrossRef]
- Kourtis, A.P.; Read, J.S.; Jamieson, D.J. Pregnancy and infection. N. Engl. J. Med. 2014, 370, 2211–2218. [Google Scholar] [CrossRef]
- Piekkola, S.; Turner, P.C.; Abdel-Hamid, M.; Ezzat, S.; El-Daly, M.; El-Kafrawy, S.; Savchenko, E.; Poussa, T.; Woo, J.C.S.; Mykkänen, H.; et al. Characterisation of aflatoxin and deoxynivalenol exposure among pregnant Egyptian women. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2012, 29, 962–971. [Google Scholar] [CrossRef]
- Pestka, J.J. Deoxynivalenol: Mechanisms of action, human exposure, and toxicological relevance. Arch. Toxicol. 2010, 84, 663–679. [Google Scholar] [CrossRef]
- Turner, P.C.; White, K.L.; Burley, V.J.; Hopton, R.P.; Rajendram, A.; Fisher, J.; Cade, J.E.; Wild, C.P. A comparison of deoxynivalenol intake and urinary deoxynivalenol in UK adults. Biomarkers 2010, 15, 553–562. [Google Scholar] [CrossRef]
- Rodriguez-Carrasco, Y.; Molto, J.C.; Manes, J.; Berrada, H. Exposure assessment approach through mycotoxin/creatinine ratio evaluation in urine by GC-MS/MS. Food Chem. Toxicol. 2014, 72, 69–75. [Google Scholar] [CrossRef]
- Ediage, E.N.; Di Mavungu, J.D.; Song, S.Q.; Sioen, I.; De Saeger, S. Multimycotoxin analysis in urines to assess infant exposure: A case study in Cameroon. Environ. Int. 2013, 57–58, 50–59. [Google Scholar] [CrossRef]
- Brera, C.; De Santis, B.; Debegnach, F.; Miano, B.; Moretti, G.; Lanzone, A.; Del Sordo, G.; Buonsenso, D.; Chiaretti, A.; Hardie, L.; et al. Experimental study of deoxynivalenol biomarkers in urine. EFSA Supporting Publ. 2015, 12, 818E. [Google Scholar] [CrossRef]
- Turner, P.C.; Hopton, R.P.; White, K.L.M.; Fisher, J.; Cade, J.E.; Wild, C.P. Assessment of deoxynivalenol metabolite profiles in UK adults. Food Chem. Toxicol. 2011, 49, 132–135. [Google Scholar] [CrossRef] [Green Version]
- Klingensmith, M.E.; Aziz, A.; Bharat, A.; Fox, A. The Washington Manual of Surgery, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Kliegman, R.M.; Geme, J.S. Nelson: Textbook of Pediatrics, 20th ed.; Elsevier: Philadelphia, PA, USA, 2015. [Google Scholar]
- Mazzachi, B.C.; Peake, M.J.; Ehrhardt, V. Reference range and method comparison studies for enzymatic and Jaffé creatinine assays in plasma and serum and early morning urine. Clin. Lab. 2000, 46, 53–55. [Google Scholar]
- Magnusson, B.; Örnemark, U. (Eds.) Eurachem Guide: The Fitness for Purpose of Analytical Methods—A Laboratory Guide to Method Validation and Related Topics, 2nd ed.; Eurachem: Torino, Italy, 2014; ISBN 978-91-87461-59-0. [Google Scholar]
- Ellison, S.L.R.; Williams, A. Eurachem/CITAC Guide: Quantifying Uncertainty in Analytical Measurement, 3rd ed.; Eurachem: Torino, Italy, 2012. [Google Scholar]
- European Food Safety Authority (EFSA). Use of the EFSA Comprehensive European Food Consumption Database in Exposure Assessment. EFSA J. 2011, 9, 2097–2131. [Google Scholar] [CrossRef]
- Vioque, J.; Navarrete-Muñoz, E.M.; Gimenez-Monzó, D.; García-de-la-Hera, M.; Granado, F.; Young, I.S.; Ramón, R.; Ballester, F.; Murcia, M.; Rebagliato, M.; et al. Reproducibility and validity of a food frequency questionnaire among pregnant women in a Mediterranean area. Nutr. J. 2013, 19, 12–26. [Google Scholar] [CrossRef]


{kind=link}
| Validation Parameter | DON | DOM-1 |
|---|---|---|
| LoD; µg/L | 0.25 | 0.25 |
| Level 1 (LoQ); µg/Lurine | 0.50 | 0.51 |
| Mean value; µg/Lurine | 0.54 | 0.43 |
| sr; µg/Lurine | 0.03 | 0.03 |
| RSDr; % | 5.55 | 6.98 |
| Recovery; % | 109 | 84 |
| Uncertainty; % | 14 | 15 |
| Level 2; µg/Lurine | 2.50 | 2.53 |
| Mean value; µg/Lurine | 2.63 | 2.11 |
| sr; µg/Lurine | 0.10 | 0.14 |
| RSDr; % | 3.80 | 6.63 |
| Recovery; % | 105 | 85 |
| Uncertainty; % | 8 | 18 |
| Level 3; µg/Lurine | 12.50 | 12.63 |
| Mean value; µg/Lurine | 12.16 | 11.65 |
| sr; µg/Lurine | 0.33 | 0.37 |
| RSDr; % | 2.71 | 3.18 |
| Recovery; % | 95 | 93 |
| Uncertainty; % | 8 | 17 |
| Level 4; µg/Lurine | 62.50 | 50.50 |
| Mean value; µg/Lurine | 63.35 | 40.49 |
| sr; µg/Lurine | 3.86 | 0.48 |
| RSDr; % | 6.09 | 1.19 |
| Recovery; % | 101 | 81 |
| Uncertainty; % | 9 | 14 |
| Group Category | Gender a | N b | Weight, kg | Height, cm | BMI c, kg/m2 |
|---|---|---|---|---|---|
| Children (3–9 years) | F | 20 | 27 | 124 | 17.3 |
| M | 20 | 26 | 119 | 17.2 | |
| Adolescent (10–17 years) | F | 20 | 52 | 163 | 19.4 |
| M | 20 | 63 | 173 | 20.7 | |
| Adults (18–64 years) | F | 15 | 63 | 167 | 22.4 |
| M | 16 | 77 | 179 | 24.0 | |
| Elderly (>65 years) | F | 10 | 63 | 161 | 24.4 |
| M | 9 | 70 | 170 | 24.3 | |
| Vegetarians | F | 15 | 61 | 166 | 21.9 |
| M | 16 | 75 | 176 | 24.9 | |
| Pregnant women | F | 42 | 66 | 164 | 24.6 |
| Age Group | Day | Gender a | Samples Above LoQ (%) | Total DON (ng/mLurine) | Total DON (ng/mgcreat) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | P50 | IQR | Free DON (%) | DON-GlcA (%) | Mean | P50 | IQR | ||||
| Children (3–9 Years) | 1 | F (20) | 90 | 11.4 | 5.80 | 6.91 | 24 | 76 | 13.5 | 7.31 | 11.20 |
| M (20) | 95 | 10.3 | 9.46 | 13.11 | 27 | 73 | 12.4 | 9.77 | 8.16 | ||
| 2 | F (20) | 90 | 8.70 | 6.49 | 8.69 | 29 | 71 | 12.9 | 9.42 | 11.65 | |
| M (20) | 95 | 14.0 | 11.9 | 12.60 | 36 | 64 | 17.0 | 13.0 | 12.05 | ||
| Adolescents (10–17 Years) | 1 | F (20) | 80 | 9.83 | 5.36 | 11.89 | 24 | 76 | 9.38 | 6.20 | 11.37 |
| M (20) | 100 | 12.9 | 11.4 | 12.71 | 34 | 66 | 15.6 | 9.30 | 17.54 | ||
| 2 | F (20) | 85 | 9.19 | 5.12 | 7.40 | 15 | 85 | 12.6 | 8.06 | 9.74 | |
| M (20) | 90 | 12.3 | 11.0 | 12.17 | 30 | 70 | 11.3 | 9.96 | 11.89 | ||
| Adults (18–64 Years) | 1 | F (15) | 80 | 5.34 | 4.18 | 7.42 | 44 | 56 | 5.33 | 3.41 | 6.83 |
| M (16) | 88 | 5.35 | 5.08 | 7.12 | 58 | 42 | 4.30 | 3.76 | 4.20 | ||
| 2 | F (15) | 80 | 9.01 | 5.44 | 7.65 | 23 | 77 | 8.35 | 5.54 | 5.87 | |
| M (16) | 81 | 11.8 | 12.6 | 13.94 | 45 | 55 | 7.60 | 6.84 | 11.81 | ||
| Elderly (>65 Years) | 1 | F (10) | 70 | 5.07 | 3.18 | 6.01 | 41 | 59 | 6.69 | 5.13 | 6.10 |
| M (10) | 90 | 4.93 | 4.40 | 4.10 | 41 | 59 | 6.37 | 6.87 | 8.79 | ||
| 2 | F (10) | 60 | 5.51 | 4.40 | 3.25 | 35 | 65 | 7.79 | 5.16 | 3.84 | |
| M (10) | 80 | 6.16 | 5.59 | 3.40 | 20 | 80 | 12.4 | 8.09 | 3.84 | ||
| Vegetarians | 1 | F (15) | 80 | 10.6 | 9.74 | 14.74 | 19 | 81 | 16.1 | 10.1 | 30.75 |
| M (15) | 73 | 4.10 | 3.30 | 5.22 | 35 | 65 | 4.43 | 3.23 | 7.85 | ||
| 2 | F (15) | 80 | 5.53 | 4.17 | 5.34 | 23 | 77 | 8.47 | 8.25 | 12.73 | |
| M (15) | 73 | 5.88 | 3.03 | 7.79 | 30 | 70 | 4.28 | 2.25 | 7.44 | ||
| Pregnant Women | 1 | F (42) | 40 | 4.37 | 0.00 | 8.20 | 28 | 72 | 6.30 | 0.00 | 6.87 |
| 2 | F (42) | 43 | 2.70 | 0.00 | 3.10 | 33 | 67 | 2.84 | 0.00 | 4.91 | |
| Total | 1 | (203) | 76 | 7.67 | 4.58 | 8.63 | 34 | 66 | 9.21 | 5.05 | 9.81 |
| 2 | (203) | 75 | 7.93 | 5.29 | 9.26 | 29 | 71 | 9.03 | 6.07 | 10.41 | |
| Age Group | Day | Gender | Mean | P50 | IQR | P95 | >TDI |
|---|---|---|---|---|---|---|---|
| Children (3–9 Years) | 1 | F (20) | 757 | 385 | 459 | 3265 | 4 (20%) |
| M (20) | 683 | 628 | 870 | 1975 | 6 (30%) | ||
| 2 | F (20) | 577 | 431 | 577 | 1765 | 3 (15%) | |
| M (20) | 937 | 791 | 837 | 2457 | 8 (40%) | ||
| Adolescents (10–17 Years) | 1 | F (20) | 328 | 178 | 393 | 1261 | 2 (10%) |
| M (20) | 427 | 379 | 421 | 1359 | 1 (5%) | ||
| 2 | F (20) | 296 | 170 | 246 | 1019 | 1 (5%) | |
| M (20) | 409 | 367 | 403 | 1030 | 1 (5%) | ||
| Adults (18–64 Years) | 1 | F (15) | 177 | 139 | 247 | 513 | 0 |
| M (16) | 170 | 168 | 237 | 446 | 0 | ||
| 2 | F (15) | 299 | 181 | 254 | 1172 | 1 (7%) | |
| M (16) | 411 | 416 | 463 | 1685 | 1 (7%) | ||
| Elderly (>65 Years) | 1 | F (10) | 104 | 124 | 132 | 284 | 0 |
| M (10) | 137 | 141 | 136 | 299 | 0 | ||
| 2 | F (10) | 169 | 146 | 212 | 515 | 0 | |
| M (10) | 181 | 189 | 129 | 515 | 0 | ||
| Vegetarians | 1 | F (15) | 360 | 323 | 472 | 1555 | 1 (7%) |
| M (15) | 186 | 112 | 194 | 561 | 0 | ||
| 2 | F (15) | 181 | 138 | 174 | 549 | 0 | |
| M (15) | 235 | 119 | 259 | 815 | 0 | ||
| Pregnant Women | 1 | F (42) | 154 | 0 | 271 | 630 | 0 |
| 2 | F (42) | 96 | 0 | 103 | 519 | 0 | |
| Total | 1 | (203) | 329 | 170 | 286 | 1144 | 14 (7%) |
| 2 | (203) | 343 | 181 | 310 | 1128 | 15 (8%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Santis, B.; Debegnach, F.; Miano, B.; Moretti, G.; Sonego, E.; Chiaretti, A.; Buonsenso, D.; Brera, C. Determination of Deoxynivalenol Biomarkers in Italian Urine Samples. Toxins 2019, 11, 441. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080441
De Santis B, Debegnach F, Miano B, Moretti G, Sonego E, Chiaretti A, Buonsenso D, Brera C. Determination of Deoxynivalenol Biomarkers in Italian Urine Samples. Toxins. 2019; 11(8):441. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080441
Chicago/Turabian StyleDe Santis, Barbara, Francesca Debegnach, Brunella Miano, Giorgio Moretti, Elisa Sonego, Antonio Chiaretti, Danilo Buonsenso, and Carlo Brera. 2019. "Determination of Deoxynivalenol Biomarkers in Italian Urine Samples" Toxins 11, no. 8: 441. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins11080441