Infant Botulism: Checklist for Timely Clinical Diagnosis and New Possible Risk Factors Originated from a Case Report and Literature Review

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Case Presentation
3. Results and Discussion
4. Conclusions
5. Materials and Methods
5.1. Diagnosis
5.2. Literature Review on Clinical and Instrumental Criteria for Early Diagnosis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cagan, E.; Peker, E.; Dogan, M.; Caksen, H. Infant botulism. Eurasian J. Med. 2010, 42, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Rosow, L.K.; Strober, J.B. Infant botulism: Review and clinical update. Pediatr. Neurol. 2015, 52, 487–492. [Google Scholar] [CrossRef]
- Smith, T.J.; Williamson, C.H.D.; Hill, K.K.; Johnson, S.L.; Xie, G.; Anniballi, F.; Auricchio, B.; Fernández, R.A.; Caballero, P.A.; Keim, P.; et al. The Distinctive Evolution of. Front. Microbiol. 2021, 12, 566908. [Google Scholar] [CrossRef]
- Dover, N.; Barash, J.R.; Hill, K.K.; Davenport, K.W.; Teshima, H.; Xie, G.; Arnon, S.S. Clostridium botulinum strain Af84 contains three neurotoxin gene clusters: Bont/A2, bont/F4 and bont/F5. PLoS ONE 2013, 8, e61205. [Google Scholar] [CrossRef]
- Peck, M.W.; Smith, T.J.; Anniballi, F.; Austin, J.W.; Bano, L.; Bradshaw, M.; Cuervo, P.; Cheng, L.W.; Derman, Y.; Dorner, B.G.; et al. Historical Perspectives and Guidelines for Botulinum Neurotoxin Subtype Nomenclature. Toxins 2017, 9, 38. [Google Scholar] [CrossRef]
- Rasetti-Escargueil, C.; Lemichez, E.; Popoff, M.R. Toxemia in Human Naturally Acquired Botulism. Toxins 2020, 12, 716. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, M.J.; Adams, J.B.; Doxey, A.C. Botulinum neurotoxin homologs in non-Clostridium species. FEBS Lett. 2015, 589, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Zornetta, I.; Azarnia Tehran, D.; Arrigoni, G.; Anniballi, F.; Bano, L.; Leka, O.; Zanotti, G.; Binz, T.; Montecucco, C. The first non Clostridial botulinum-like toxin cleaves VAMP within the juxtamembrane domain. Sci Rep. 2016, 6, 30257. [Google Scholar] [CrossRef]
- Wentz, T.G.; Muruvanda, T.; Lomonaco, S.; Thirunavukkarasu, N.; Hoffmann, M.; Allard, M.W.; Hodge, D.R.; Pillai, S.P.; Hammack, T.S.; Brown, E.W.; et al. Closed Genome Sequence of Chryseobacterium piperi Strain CTMT/ATCC BAA-1782, a Gram-Negative Bacterium with Clostridial Neurotoxin-Like Coding Sequences. Genome Announc. 2017, 5, e01296-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popoff, M.R. Botulinum Neurotoxins: Still a Privilege of Clostridia? Cell Host Microbe 2018, 23, 145–146. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Lebreton, F.; Mansfield, M.J.; Miyashita, S.I.; Zhang, J.; Schwartzman, J.A.; Tao, L.; Masuyer, G.; Martínez-Carranza, M.; Stenmark, P.; et al. Identification of a Botulinum Neurotoxin-like Toxin in a Commensal Strain of Enterococcus faecium. Cell Host Microbe 2018, 23, 169–176.e166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunt, J.; Carter, A.T.; Stringer, S.C.; Peck, M.W. Identification of a novel botulinum neurotoxin gene cluster in Enterococcus. FEBS Lett. 2018, 592, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Sobel, J. Botulism. Clin. Infect. Dis. 2005, 41, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.A.; Anniballi, F.; Austin, J.W. Adult Intestinal Toxemia Botulism. Toxins 2020, 12, 81. [Google Scholar] [CrossRef] [Green Version]
- Fenicia, L.; Anniballi, F. Infant botulism. Ann Ist Super Sanita 2009, 45, 134–146. [Google Scholar]
- Grech, A.; Collins, C.E.; Holmes, A.; Lal, R.; Duncanson, K.; Taylor, R.; Gordon, A. Maternal exposures and the infant gut microbiome: A systematic review with meta-analysis. Gut Microbes 2021, 13, 1–30. [Google Scholar] [CrossRef]
- Sugiyama, H.; Mills, D.C. Intraintestinal toxin in infant mice challenged intragastrically with Clostridium botulinum spores. Infect. Immun. 1978, 21, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Burr, D.H.; Sugiyama, H. Susceptibility to enteric botulinum colonization of antibiotic-treated adult mice. Infect. Immun. 1982, 36, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Arnon, S.S.; Damus, K.; Chin, J. Infant botulism: Epidemiology and relation to sudden infant death syndrome. Epidemiol. Rev. 1981, 3, 45–66. [Google Scholar] [CrossRef]
- Jian, C.; Carpén, N.; Helve, O.; de Vos, W.M.; Korpela, K.; Salonen, A. Early-life gut microbiota and its connection to metabolic health in children: Perspective on ecological drivers and need for quantitative approach. EBioMedicine 2021, 69, 103475. [Google Scholar] [CrossRef] [PubMed]
- Wilcke, B.W.; Midura, T.F.; Arnon, S.S. Quantitative evidence of intestinal colonization by Clostridium botulinum in four cases of infant botulism. J. Infect. Dis. 1980, 141, 419–423. [Google Scholar] [CrossRef]
- Arnon, S.S.; Damus, K.; Thompson, B.; Midura, T.F.; Chin, J. Protective role of human milk against sudden death from infant botulism. J. Pediatr. 1982, 100, 568–573. [Google Scholar] [CrossRef]
- Panditrao, M.V.; Dabritz, H.A.; Kazerouni, N.N.; Damus, K.H.; Meissinger, J.K.; Arnon, S.S. Seven-Year Case-Control Study in California of Risk Factors for Infant Botulism. J. Pediatr. 2020, 227, 258–267.e258. [Google Scholar] [CrossRef]
- O’Sullivan, A.; Farver, M.; Smilowitz, J.T. The Influence of Early Infant-Feeding Practices on the Intestinal Microbiome and Body Composition in Infants. Nutr. Metab. Insights 2015, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laursen, M.F. Gut Microbiota Development: Influence of Diet from Infancy to Toddlerhood. Ann. Nutr. Metab. 2021, 77, 21–34. [Google Scholar] [CrossRef]
- Arnon, S.S.; Midura, T.F.; Damus, K.; Thompson, B.; Wood, R.M.; Chin, J. Honey and other environmental risk factors for infant botulism. J. Pediatr. 1979, 94, 331–336. [Google Scholar] [CrossRef]
- Fenicia, L.; Anniballi, F.; Aureli, P. Intestinal toxemia botulism in Italy, 1984–2005. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 385–394. [Google Scholar] [CrossRef]
- Nevas, M.; Lindström, M.; Virtanen, A.; Hielm, S.; Kuusi, M.; Arnon, S.S.; Vuori, E.; Korkeala, H. Infant botulism acquired from household dust presenting as sudden infant death syndrome. J. Clin. Microbiol. 2005, 43, 511–513. [Google Scholar] [CrossRef] [Green Version]
- Fenicia, L.; Da Dalt, L.; Anniballi, F.; Franciosa, G.; Zanconato, S.; Aureli, P. A case if infant botulism due to neurotoxigenic Clostridium butyricum type E associated with Clostridium difficile colitis. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 736–738. [Google Scholar]
- Fenicia, L.; Anniballi, F.; Pulitanò, S.; Genovese, O.; Polidori, G.; Aureli, P. A severe case of infant botulism caused by Clostridium botulinum type A with concomitant intestinal viral infections. Eur. J. Pediatr. 2004, 163, 501–502. [Google Scholar] [CrossRef]
- Ringe, H.; Schuelke, M.; Weber, S.; Dorner, B.G.; Kirchner, S.; Dorner, M.B. Infant botulism: Is there an association with thiamine deficiency? Pediatrics 2014, 134, e1436–e1440. [Google Scholar] [CrossRef] [Green Version]
- Midura, T.F.; Snowden, S.; Wood, R.M.; Arnon, S.S. Isolation of Clostridium botulinum from Honey. J. Clin. Microbiol. 1979, 9, 282–283. [Google Scholar] [CrossRef] [PubMed]
- Bianco, M.I.; Lúquez, C.; de Jong, L.I.; Fernández, R.A. Presence of Clostridium botulinum spores in Matricaria chamomilla (chamomile) and its relationship with infant botulism. Int. J. Food Microbiol. 2008, 121, 357–360. [Google Scholar] [CrossRef]
- Brett, M.M.; McLauchlin, J.; Harris, A.; O’Brien, S.; Black, N.; Forsyth, R.J.; Roberts, D.; Bolton, F.J. A case of infant botulism with a possible link to infant formula milk powder: Evidence for the presence of more than one strain of Clostridium botulinum in clinical specimens and food. J. Med. Microbiol. 2005, 54, 769–776. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, T.; Haginoya, K.; Morimoto, T.; Hatakeyama, T.; Tsuchiya, S. A case of infant botulism infection due to consumption of untreated well-water. J. Pediatr. 2014, 164, 931–933. [Google Scholar] [CrossRef]
- Shelley, E.B.; O’Rourke, D.; Grant, K.; McArdle, E.; Capra, L.; Clarke, A.; McNamara, E.; Cunney, R.; McKeown, P.; Amar, C.F.; et al. Infant botulism due to C. butyricum type E toxin: A novel environmental association with pet terrapins. Epidemiol. Infect. 2015, 143, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Xin, W.; Huang, Y.; Ji, B.; Li, P.; Wu, Y.; Liu, J.; Wang, X.; Yang, H.; Kang, L.; Gao, S.; et al. Identification and characterization of Clostridium botulinum strains associated with an infant botulism case in China. Anaerobe 2019, 55, 1–7. [Google Scholar] [CrossRef]
- Johnson, R.O.; Clay, S.A.; Arnon, S.S. Diagnosis and management of infant botulism. Am. J. Dis Child. 1979, 133, 586–593. [Google Scholar] [CrossRef]
- Santos, J.I.; Swensen, P.; Glasgow, L.A. Potentiation of Clostridium botulinum toxin aminoglycoside antibiotics: Clinical and laboratory observations. Pediatrics 1981, 68, 50–54. [Google Scholar]
- Fenicia, L.; Ferrini, A.M.; Anniballi, F.; Mannoni, V.; Aureli, P. Considering the antimicrobial sensitivity of the intestinal botulism agent Clostridium butyricum when treating concomitant infections. Eur. J. Epidemiol. 2003, 18, 1153–1154. [Google Scholar] [CrossRef] [PubMed]
- Barash, J.R.; Castles, J.B.; Arnon, S.S. Antimicrobial Susceptibility of 260 Clostridium botulinum Type A, B, Ba, and Bf Strains and a Neurotoxigenic Clostridium baratii Type F Strain Isolated from California Infant Botulism Patients. Antimicrob Agents Chemother. 2018, 62, e01594-18. [Google Scholar] [CrossRef] [Green Version]
- Mazuet, C.; Yoon, E.J.; Boyer, S.; Pignier, S.; Blanc, T.; Doehring, I.; Meziane-Cherif, D.; Dumant-Forest, C.; Sautereau, J.; Legeay, C.; et al. A penicillin- and metronidazole-resistant Clostridium botulinum strain responsible for an infant botulism case. Clin. Microbiol. Infect. 2016, 22, 644.e7–e12. [Google Scholar] [CrossRef] [Green Version]
- Arnon, S.S. Creation and development of the public service orphan drug Human Botulism Immune Globulin. Pediatrics 2007, 119, 785–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanella de Cuetos, E.E.; Fernandez, R.A.; Bianco, M.I.; Sartori, O.J.; Piovano, M.L.; Lúquez, C.; de Jong, L.I. Equine botulinum antitoxin for the treatment of infant botulism. Clin. Vaccine Immunol. 2011, 18, 1845–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnon, S.S.; Schechter, R.; Maslanka, S.E.; Jewell, N.P.; Hatheway, C.L. Human botulism immune globulin for the treatment of infant botulism. N. Engl. J. Med. 2006, 354, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Arnon, S.S.; Midura, T.F.; Clay, S.A.; Wood, R.M.; Chin, J. Infant botulism. Epidemiological, clinical, and laboratory aspects. JAMA 1977, 237, 1946–1951. [Google Scholar] [CrossRef] [PubMed]
- Francisco, A.M.; Arnon, S.S. Clinical mimics of infant botulism. Pediatrics 2007, 119, 826–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halpin, A.L.; Khouri, J.M.; Payne, J.R.; Nakao, J.H.; Cronquist, A.; Kalas, N.; Mohr, M.; Osborne, M.; O’Dell, S.; Luquez, C.; et al. Type F Infant Botulism: Investigation of Recent Clusters and Overview of This Exceedingly Rare Disease. Clin. Infect. Dis. 2017, 66, S92–S94. [Google Scholar] [CrossRef] [Green Version]
- Khouri, J.M.; Payne, J.R.; Arnon, S.S. More Clinical Mimics of Infant Botulism. J. Pediatr. 2018, 193, 178–182. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, A.R.; Bodensteiner, J.; Gutmann, L. Electrodiagnosis of infantile botulism. J. Child. Neurol. 1994, 9, 362–365. [Google Scholar] [CrossRef]
- Cornblath, D.R.; Sladky, J.T.; Sumner, A.J. Clinical electrophysiology of infantile botulism. Muscle Nerve 1983, 6, 448–452. [Google Scholar] [CrossRef]
- Bernardor, J.; Neveu, J.; Haas, H.; Pitelet, G.; Popoff, M.R.; Mazuet, C.; Bérard, E.; Boulay, C.; Chabrol, B. Infant botulism: Two case reports and electroneuromyogram findings. Arch. Pediatr. 2018, 25, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Witoonpanich, R.; Vichayanrat, E.; Tantisiriwit, K.; Rattanasiri, S.; Ingsathit, A. Electrodiagnosis of botulism and clinico-electrophysiological correlation. Clin. Neurophysiol. 2009, 120, 1135–1138. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, V.; Crawford, T.O. Stimulation single-fiber EMG in infant botulism. Muscle Nerve 1999, 22, 1698–1703. [Google Scholar] [CrossRef]
- Chaudhry, R. Botulism: A diagnostic challenge. Indian J. Med. Res. 2011, 134, 10–12. [Google Scholar] [PubMed]
- Dilena, R.; Abicht, A.; Sergi, P.; Comi, G.P.; Di Fonzo, A.; Chidini, G.; Natacci, F.; Barbieri, S.; Lochmüller, H. Congenital myasthenic syndrome due to choline acetyltransferase mutations in infants: Clinical suspicion and comprehensive electrophysiological assessment are important for early diagnosis. J. Child. Neurol. 2014, 29, 389–393. [Google Scholar] [CrossRef]
- Good, R.J.; Messacar, K.; Stence, N.V.; Press, C.A.; Carpenter, T.C. Abnormal Neuroimaging in a Case of Infant Botulism. Front. Pediatr. 2015, 3, 108. [Google Scholar] [CrossRef] [Green Version]
- Santos Rocha, C.; Hirao, L.A.; Weber, M.G.; Méndez-Lagares, G.; Chang, W.L.W.; Jiang, G.; Deere, J.D.; Sparger, E.E.; Roberts, J.; Barry, P.A.; et al. Subclinical Cytomegalovirus Infection Is Associated with Altered Host Immunity, Gut Microbiota, and Vaccine Responses. J. Virol. 2018, 92, e00167-18. [Google Scholar] [CrossRef] [Green Version]
- Shirey, T.B.; Dykes, J.K.; Lúquez, C.; Maslanka, S.E.; Raphael, B.H. Characterizing the fecal microbiota of infants with botulism. Microbiome 2015, 3, 54. [Google Scholar] [CrossRef] [Green Version]
- Pietrzak, B.; Tomela, K.; Olejnik-Schmidt, A.; Mackiewicz, A.; Schmidt, M. Secretory IgA in Intestinal Mucosal Secretions as an Adaptive Barrier against Microbial Cells. Int. J. Mol. Sci. 2020, 21, 9254. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, T.; Fujinaga, Y.; Jin, Y.; Kabumoto, Y.; Oguma, K. Human milk SIgA binds to botulinum type B 16S toxin and limits toxin adherence on T84 cells. Biochem. Biophys. Res. Commun. 2007, 352, 867–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panditrao, M.V.; Dabritz, H.A.; Kazerouni, N.N.; Damus, K.H.; Meissinger, J.K.; Arnon, S.S. Descriptive Epidemiology of Infant Botulism in California: The First 40 Years. J. Pediatr. 2020, 227, 247–257.e243. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Tchao, C.; Prystajecky, N.; Cutler, J.; Austin, J.W. A summary of surveillance, morbidity and microbiology of laboratory-confirmed cases of infant botulism in Canada, 1979–2019. Can. Commun. Dis Rep. 2021, 47, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Anniballi, F.; Auricchio, B.; Fiore, A.; Lonati, D.; Locatelli, C.A.; Lista, F.; Fillo, S.; Mandarino, G.; De Medici, D. Botulism in Italy, 1986-2015. Euro. Surveill. 2017, 22, 30550. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Infant Botulism Clinical and Instrumental Suspicion Checklist | |
|---|---|
| A. Clinical criteria | |
| A1 | Acute weakness with descending progression as initial cranial involvement as poor feeding, poor suck, fatigability when eating, expressionless face, drooling, weakness or change of cry, lethargy, respiratory insufficiency. |
| A2 | Autonomic signs as altered pupillary reflexes, constipation. |
| A3 | Deep tendon reflex (DTR) normal or reduced, often with relative sparing in comparison with the paralysis degree * |
| A4 | Presence of environmental risk factors as contact with soil (living in rural areas or home renovation environments, parental work in contact with soil and home renovation, honey, or herbal tea ingestion, contact with botulism outbreaks). |
| A5 | Presence of personal predisposing factors as clinical conditions influencing intestinal microbiota and immunity (e.g., recent viral infection history, etc.) |
| B. Brain and spinal MRI | |
| B1 | No parenchymal lesions explaining signs. |
| B2 | No cranial and spinal root MRI gadolinium enhancement (a sign of nerve root inflammation usually found in GBS, the most important mimicker). |
| C. Lumbar puncture | |
| C1 | Normal CSF parameters. |
| C2 | No albumin-cytologic dissociation (an inflammation sign usually found in GBS, the most important mimicker). |
| D. Electrodiagnosis | |
| ENMG basic criteria compatible with IB | |
| D1 | M-NCS: Low CMAP amplitudes. |
| D2 | S-NCS: Normal SNAP amplitude. |
| D3 | N-EMG: Brief-duration and small-amplitude, overly abundant motor-unit action potentials (termed as BSAPs) similar to a myopathic pattern, possible denervation potentials. |
| ENMG specific criteria proving the pre-synaptic block (pathophysiology of IB) ** | |
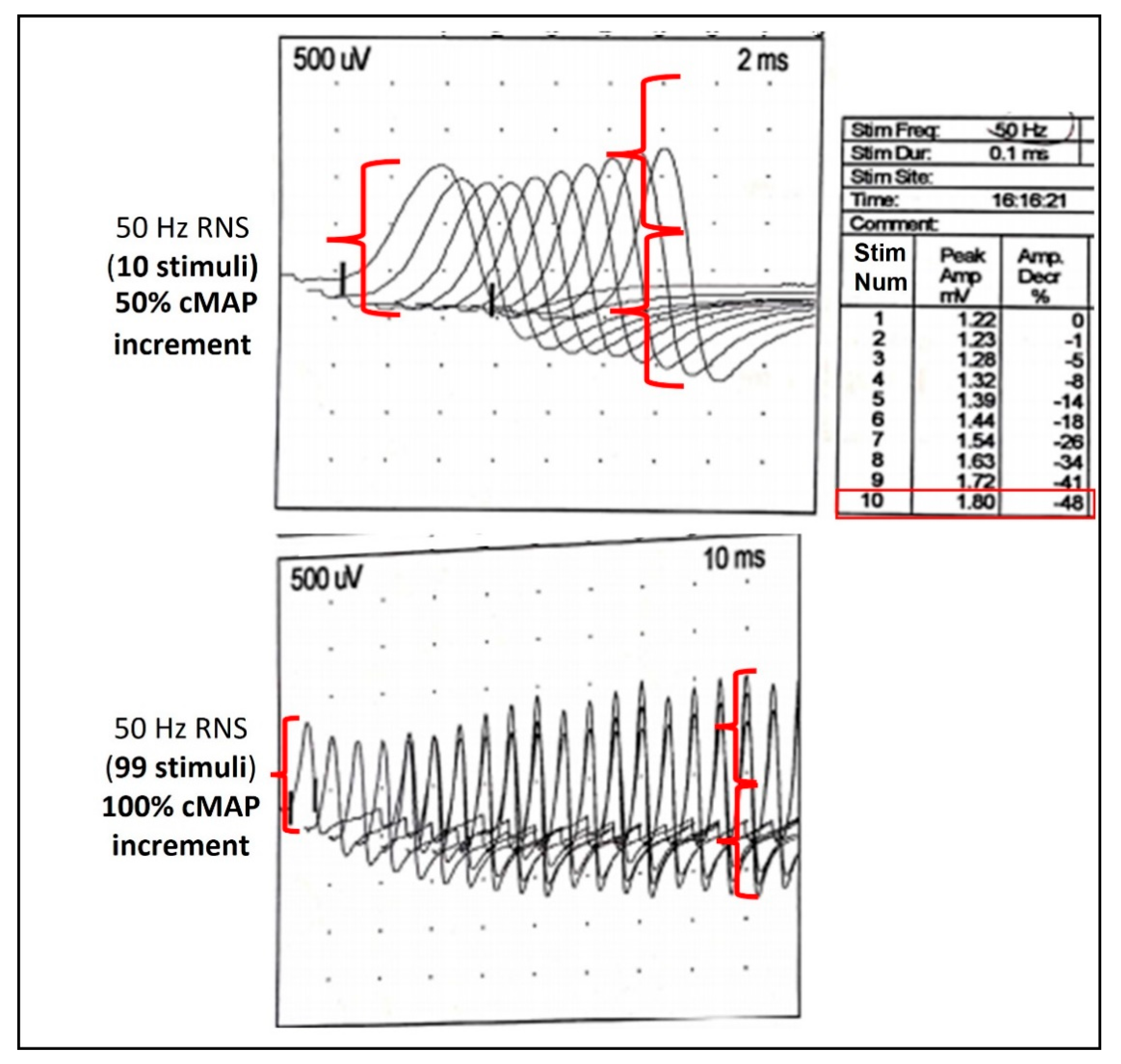
| D4 | RNS: Tetanic stimulation at 50 Hz for 10 s to prove incremental response of cMAP in comparison with a basal reduced CMAP. Being a potential painful test, use sedoanalgesia. |
| D5 | S-SFEMG: increased jitter indicating a NMJ disorder corrected at higher frequency stimulation. |
| E. Laboratory studies usually on clinical specimens (definitive confirmation) *** | |
| E1 | Detection of BoNT-producing Clostridia from fecal specimens. |
| E2 | Detection of BoNTs from fecal specimens (and serum). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dilena, R.; Pozzato, M.; Baselli, L.; Chidini, G.; Barbieri, S.; Scalfaro, C.; Finazzi, G.; Lonati, D.; Locatelli, C.A.; Cappellari, A.; et al. Infant Botulism: Checklist for Timely Clinical Diagnosis and New Possible Risk Factors Originated from a Case Report and Literature Review. Toxins 2021, 13, 860. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13120860
Dilena R, Pozzato M, Baselli L, Chidini G, Barbieri S, Scalfaro C, Finazzi G, Lonati D, Locatelli CA, Cappellari A, et al. Infant Botulism: Checklist for Timely Clinical Diagnosis and New Possible Risk Factors Originated from a Case Report and Literature Review. Toxins. 2021; 13(12):860. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13120860
Chicago/Turabian StyleDilena, Robertino, Mattia Pozzato, Lucia Baselli, Giovanna Chidini, Sergio Barbieri, Concetta Scalfaro, Guido Finazzi, Davide Lonati, Carlo Alessandro Locatelli, Alberto Cappellari, and et al. 2021. "Infant Botulism: Checklist for Timely Clinical Diagnosis and New Possible Risk Factors Originated from a Case Report and Literature Review" Toxins 13, no. 12: 860. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins13120860