In Silico Approach for Immunohistochemical Evaluation of a Cytoplasmic Marker in Breast Cancer

 , and
, and
Abstract
:1. Introduction
2. Experiments and Results
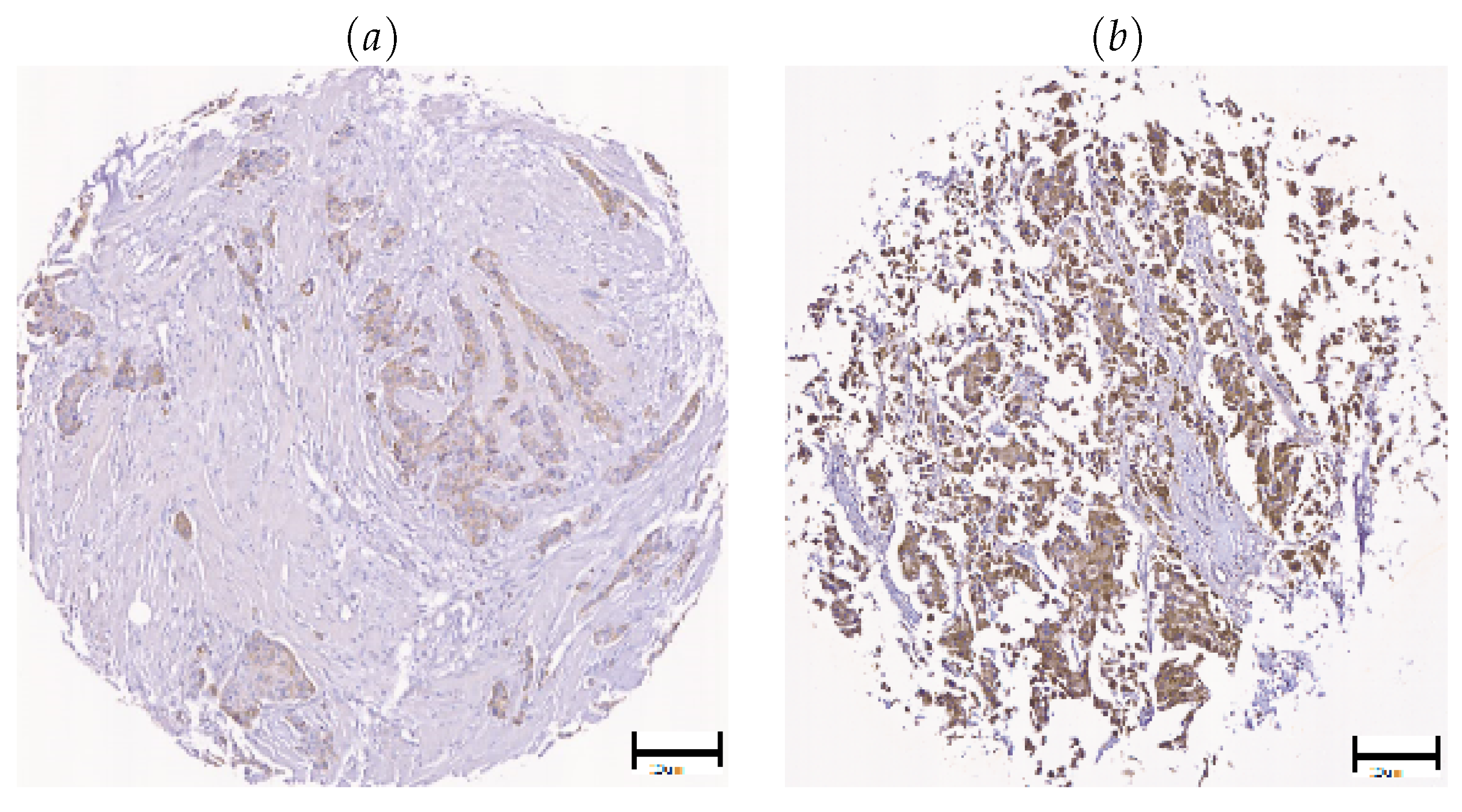
2.1. Evaluation of Block-Based Wnt-1 Segmentation
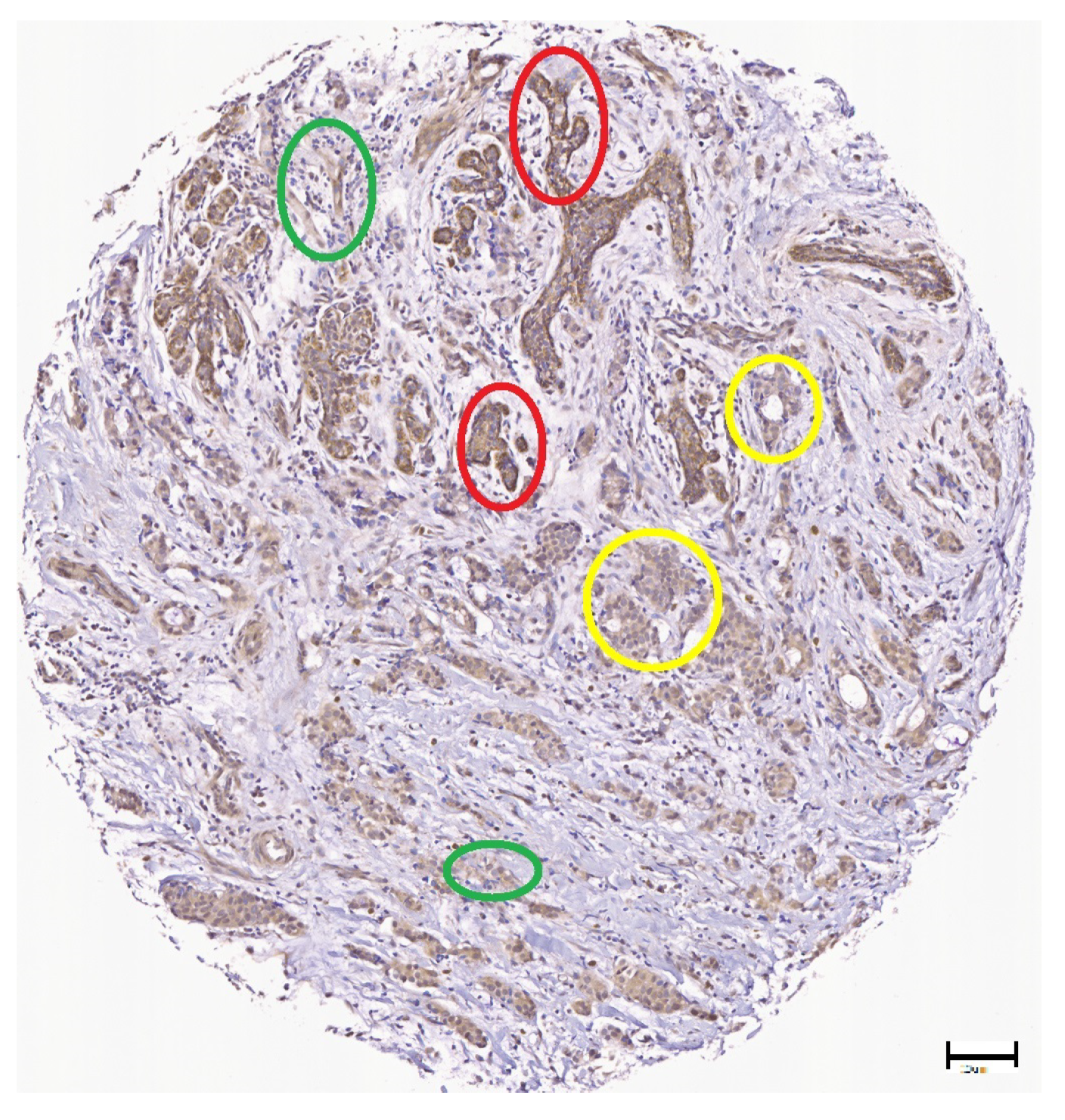
2.2. Evaluation of Block-Based Wnt-1 Classification
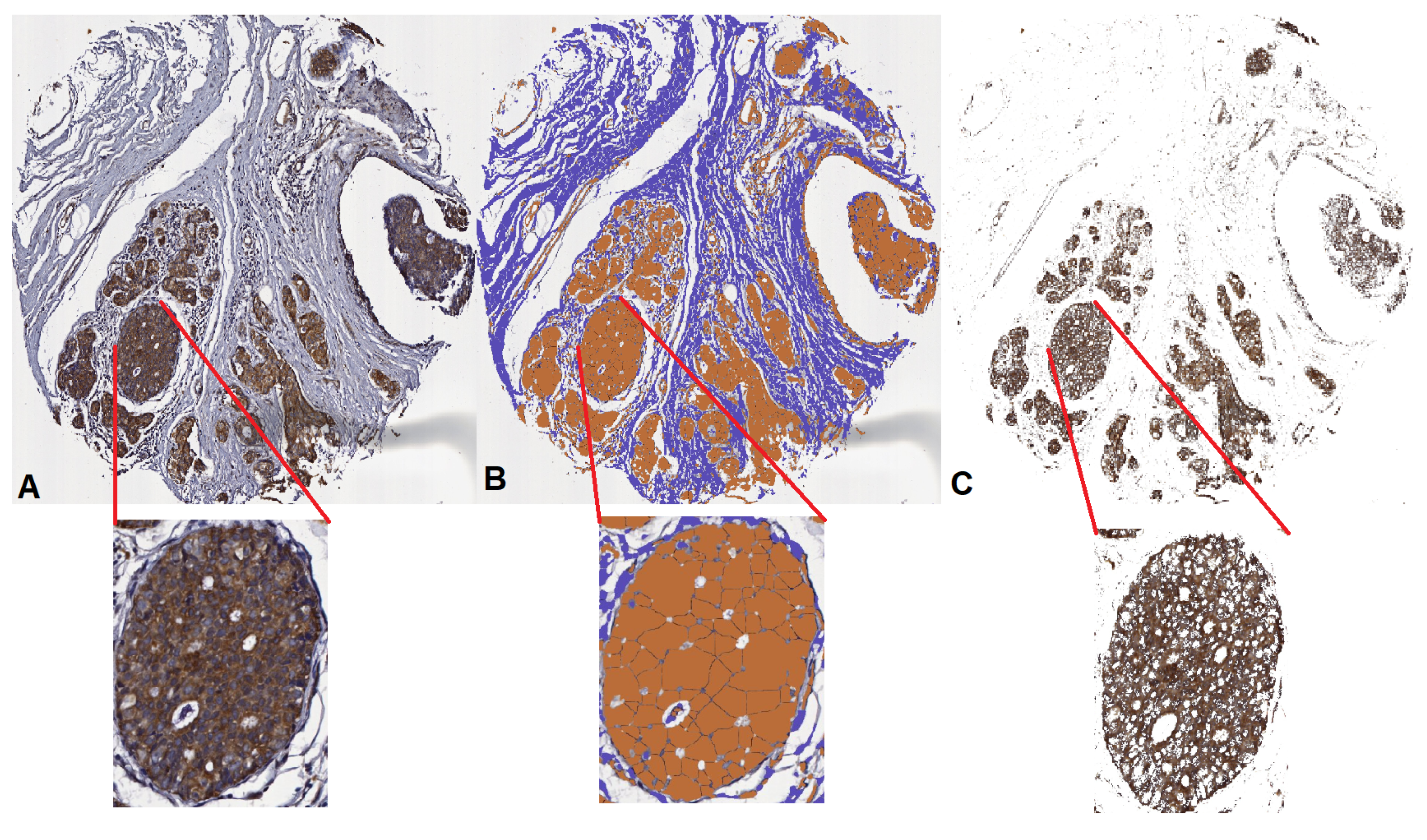
2.3. Evaluation of Wnt-1 Classification in a TMA Tissue Core Image
3. Discussion
4. Materials and Method
4.1. Problem Statement
4.2. Experimental Setup
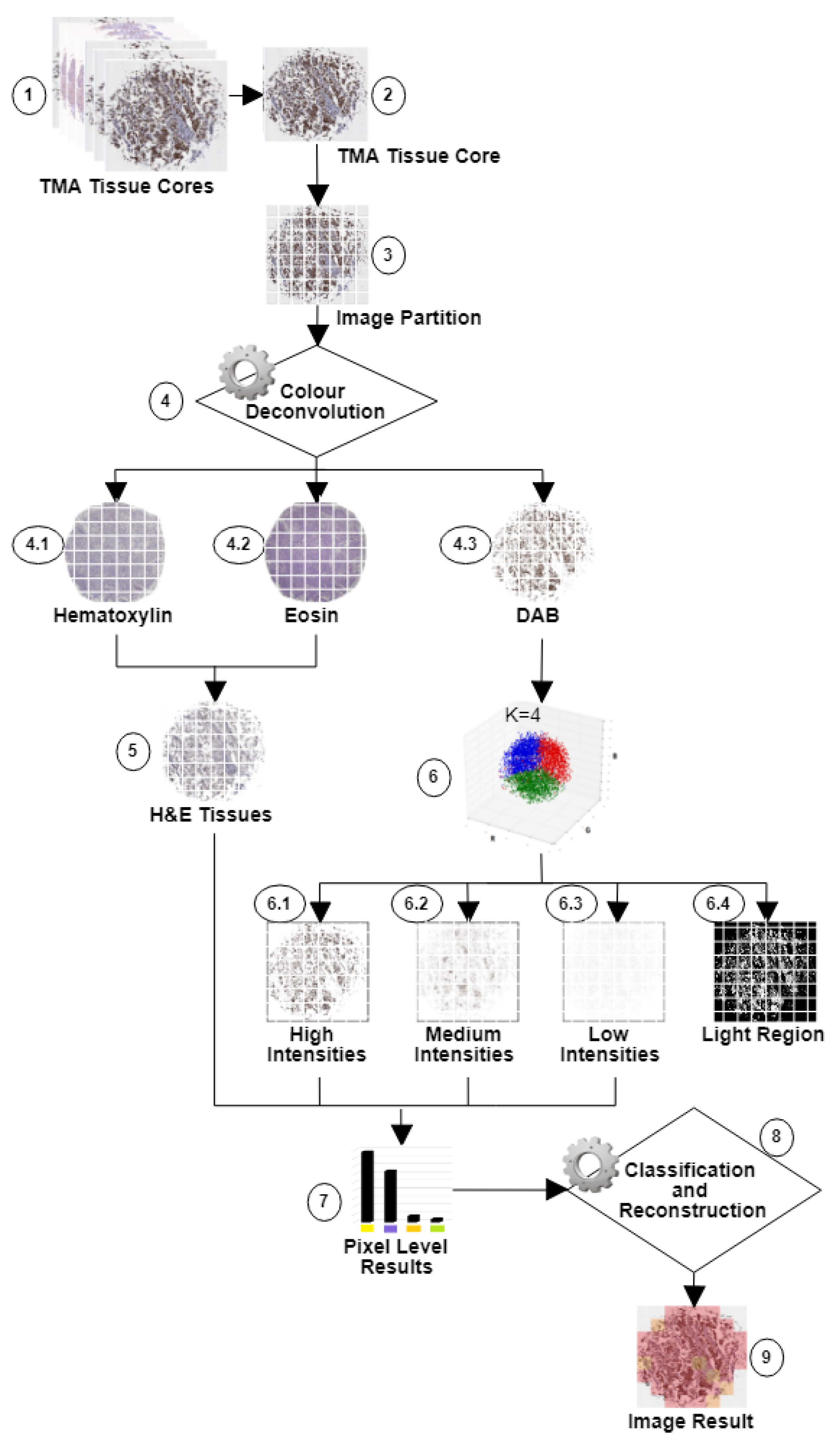
4.3. Partitioning TMA Tissue Cores into Blocks
4.4. Block-Based Wnt-1 Segmentation
4.5. Block-Based Wnt-1 Classification
4.6. Wnt-1 Classification in a TMA Tissue Core Image
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| DAB | Diaminobenzidine |
| H&E | Hematoxylin and Eosin |
| TMA | Tissue Microarray |
| ICC | Intraclass Correlation |
| IHC | Immunohistochemistry |
| MMTV | Mouse Mammary Tumour Virus |
| CSC | Cancer Stem Cell |
| ER | Estrogen Receptor |
| ER+ | Estrogen Receptor-positive |
| PR | Progesterone Receptor |
| DIA | Automated Digital Analysis |
| AQUA | Automated Quantitative Analysis |
| RGB | Red, Green and Blue |
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA A Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society Medical, How Common Is Breast Cancer? 2018. Available online: https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html (accessed on 15 January 2018).
- Cencer Research UK, Cancer Incidence for Common Cancers, 2016. Available online: http://www.cancerresearchuk.org/health-professional/cancer-statistics/incidence/common-cancers-compared#heading-Zero (accessed on 15 January 2018).
- American Cancer Society and International Agency of Research Cancer, in Women, Breast Cancer Is the Most Common Cancer and the #1 Cause of Cancer Death, 2012. Available online: http://canceratlas.cancer.org/the-burden/breast-cancer/ (accessed on 10 October 2018).
- Zhan, T.; Rindtorff, N.; Boutros, M. Wnt-1 signaling in cancer. Oncogene 2017, 36, 1461–1473. [Google Scholar] [CrossRef] [PubMed]
- Piva, M.; Domenici, G.; Iriondo, O.; Rábano, M.; Simões, B.; Comaills, V.; Barredo, I.; López-Ruiz, J.; Zabalza, I.; Kypta, R.; et al. Sox2 promotes tamoxifen resistance in breast cancer cells. EMBO Mol. Med. 2014, 6, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Varmus, R.N.H.E. Many tumors induced by the mouse mammary tumor virus contain a provirus integrated in the same region of the host genome. Cell 1982, 31, 99–109. [Google Scholar]
- Vaillant, F.; Asselin-Labat, M.L.; Shackleton, M.; Forrest, N.C.; Lindeman, G.J.; Visvader, J.E. The Mammary Progenitor Marker CD61/I3 Integrin Identifies Cancer Stem Cells in Mouse Models of Mammary Tumorigenesis. Cancer Res. 2008, 68, 7711–7717. [Google Scholar] [CrossRef] [PubMed]
- Jang, G.B.; Kim, J.Y.; Cho, S.D.; Park, K.S.; Jung, J.Y.; Lee, H.Y.; Hong, I.S.; Nam, J. Blockade of Wnt-1/β-catenin signaling suppresses breast cancer metastasis by inhibiting CSC-like phenotype. Sci. Rep. 2015, 5, 12465. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.J.; Yun, J.A.; Jeon, E.K.; Won, H.S.; Ko, Y.H.; Kim, S.Y. Prognostic significance of RSPO1, WNT1, P16, WT1, and SDC1 expressions in invasive ductal carcinoma of the breast. World J. Surg. Oncol. 2013, 11, 314. [Google Scholar] [CrossRef]
- Jiang, Q.; He, M.; Ma, M.; Wu, H.; Yu, Z.; Guan, S.; Jiang, L.; Wang, Y.; Zheng, D.; Jin, F.; et al. MicroRNA-148a inhibits breast cancer migration and invasion by directly targeting WNT-1. Oncol. Rep. 2016, 35, 1425–1432. [Google Scholar] [CrossRef]
- Halifu, Y.; Liang, J.; Zeng, X.; Ding, Y.; Zhang, X.; Jin, T.; Yakeya, B.; Abudu, D.; Zhou, Y.; Liu, X.; et al. Wnt-11 and SFRP1 as potential prognostic factors and therapeutic targets in cutaneous squamous cell carcinoma. Genet. Mol. Res. 2016, 15, 1–7. [Google Scholar] [CrossRef]
- Xu, X.; Sun, P.; Li, J.; Jheon, S.; Lee, C.; Chung, J. Aberrant Wnt-11/I-Catenin Expression is an Independent Poor Prognostic Marker of Non-small Cell Lung Cancer after Surgery. J. Thorac. Oncol. 2011, 6, 716–724. [Google Scholar] [CrossRef]
- Lee, H.H.; Uen, Y.H.; Tian, Y.F.; Sun, C.S.; Sheu, M.J.; Kuo, H.T.; Koay, L.B.; Lin, C.Y.; Tzeng, C.C.; Cheng, C.J.; et al. Wnt-1 Protein as a Prognostic Biomarker for Hepatitis B–Related and Hepatitis C–Related Hepatocellular Carcinoma after Surgery. Cancer Epidemiol. Prev. Biomark. 2009, 18, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, K.L.; Rasmussen, B.B.; Lykkesfeldt, A.E.; Møller, S.; Ejlertsen, B.; Mouridsen, H.T. Semi-quantitative scoring of potentially predictive markers for endocrine treatment of breast cancer: A comparison between whole sections and tissue microarrays. J. Clin. Pathol. 2007, 60, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Izet, M. E-Learning as New Method of Medical Education. Acta Inform. Med. 2008, 16, 102–117. [Google Scholar]
- Hernández, A.I.; Porta, S.M.; Miralles, M.; García, B.F.; Bolúmar, F. La cuantificación de la variabilidad en las observaciones clínicas. Med. Clin. 1990, 424–429. [Google Scholar]
- Tuominen, V.J.; Ruotoistenmäki, S.; Viitanen, A.; Jumppanen, M.; Isola, J. ImmunoRatio: A publicly available web application for quantitative image analysis of estrogen receptor (ER), progesterone receptor (PR), and Ki-67. Breast Cancer Res. 2010, 12, R56. [Google Scholar] [CrossRef] [PubMed]
- Shi, P.; Zhong, J.; Hong, J.; Huang, R.; Wang, K.; Chen, Y. Automated Ki-67 Quantification of Immunohistochemical Staining Image of Human Nasopharyngeal Carcinoma Xenografts. Sci. Rep. 2016, 6, 32127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, F.; Bi, R.; Yu, B.; Yang, F.; Yang, W.; Shui, R. A Comparison of Visual Assessment and Automated Digital Image Analysis of Ki67 Labeling Index in Breast Cancer. PLoS ONE 2016, 11, e0150505. [Google Scholar] [CrossRef]
- Weberpals, J.I.; Amin, M.S.; Chen, B.E.; Tu, D.; Spaans, J.N.; Squire, J.A.; Eisenhauer, E.A.; Virk, S.; Ma, D.; Duciaume, M.; et al. First application of the Automated QUantitative Analysis (AQUA) technique to quantify PTEN protein expression in ovarian cancer: A correlative study of NCIC CTG OV.16. Gynecol. Oncol. 2016, 486–493. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [Green Version]
- Gustavson, M.D.; Bourke-Martin, B.; Reilly, D.; Cregger, M.; Williams, C.; Mayotte, J.; Zerkowski, M.; Tedeschi, G.; Pinard, R.; Christiansen, J. Standardization of HER2 immunohistochemistry in breast cancer by automated quantitative analysis. Arch. Pathol. Lab. Med. 2009, 133, 1413–1419. [Google Scholar]
- Fischer, A.; Jacobson, K.; Rose, J.; Zeller, R. Hematoxylin and Eosin Staining of Tissue and Cell Sections. Cold Spring Harb. Protoc. 2008. [Google Scholar] [CrossRef] [PubMed]
- Mazo, C.; Trujillo, M.; Salazar, L. An Automatic Segmentation Approach of Epithelial Cells Nuclei. In Progress in Pattern Recognition, Image Analysis, Computer Vision, and Applications; Alvarez, L., Mejail, M., Gomez, L., Jacobo, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 7441, pp. 567–574. [Google Scholar]
- Mazo, C.; Trujillo, M.; Salazar, L. Automatic Classification of Coating Epithelial Tissue. In Progress in Pattern Recognition, Image Analysis, Computer Vision, and Applications; Bayro-Corrochano, E., Hancock, E., Eds.; Springer: Berlin, Germany, 2014; Volume 8827, pp. 311–318. [Google Scholar]
- Mazo, C.; Trujillo, M.; Salazar, L. Identifying Loose Connective and Muscle Tissues on Histology Images. In Progress in Pattern Recognition, Image Analysis, Computer Vision, and Applications; Ruiz-Shulcloper, J., Sanniti di Baja, G., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; Volume 8259, pp. 174–180. [Google Scholar]
- Mazo, C.; Bernal, J.; Trujillo, M.; Alegre, E. Transfer learning for classification of cardiovascular tissues in histological images. Comput. Methods Programs Biomed. 2018, 165, 69–76. [Google Scholar] [CrossRef]
- Mazo, C.; Trujillo, M.; Alegre, E.; Salazar, L. Automatic recognition of fundamental tissues on histology images of the human cardiovascular system. Micron 2016, 89, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mazo, C.; Alegre, E.; Trujillo, M.P.; González-Castro, V. Tissues Classification of the Cardiovascular System Using Texture Descriptors. In Proceedings of the 21st Annual Conference onMedical Image Understanding and Analysis—MIUA 2017, Edinburgh, UK, 11–13 July 2017; pp. 123–132. [Google Scholar]
- Trujillo, C.M.E.A.M. Classification of cardiovascular tissues using LBP based descriptors and a cascade SVM. Comput. Methods Programs Biomed. 2017, 147, 1–10. [Google Scholar]
- Harvey, J.M.; Clark, G.M.; Osborne, C.K.; Allred, D.C. Estrogen Receptor Status by Immunohistochemistry Is Superior to the Ligand-Binding Assay for Predicting Response to Adjuvant Endocrine Therapy in Breast Cancer. J. Clin. Oncol. 1999, 17, 1474. [Google Scholar] [CrossRef] [PubMed]
- Heath, M.; Sarkar, S.; Sanocki, T.; Bowyer, K. Comparison of Edge Detectors. Comput. Vis. Image Underst. 1998, 69, 38–54. [Google Scholar] [CrossRef]
- Unnikrishnan, R.; Pantofaru, C.; Hebert, M. Toward Objective Evaluation of Image Segmentation Algorithms. Ieee Trans. Pattern Anal. Mach. Intell. 2007, 29, 929–944. [Google Scholar] [CrossRef] [Green Version]
- Koch, G.G. Intraclass correlation coefficient. In Encyclopedia of Statistical Sciences; Kotz Samuel, J.N.L., Ed.; John Wiley Sons: Hoboken, NJ, USA, 1982; Volume 4, pp. 213–217. [Google Scholar]
- Koo, T.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Fawcett, T. An introduction to ROC analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Onder, D.; Zengin, S.; Sarioglu, S. A review on color normalization and color deconvolution methods in histopathology. Appl. Immunohistochem. Mol. Morphol. 2014, 22, 713–719. [Google Scholar] [CrossRef]
- Shu, J.; Dolman, G.E.; Duan, J.; Qiu, G.; Ilyas, M. Statistical colour models: An automated digital image analysis method for quantification of histological biomarkers. Biomed. Eng. Online 2016, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Itseez. Open Source Computer Vision Library. Available online: https://github.com/itseez/opencv (accessed on 15 Demceber 2018).
- Ruifrok, A.C.; Johnston, D.A. Quantification of histochemical staining by color deconvolution. Anal. Quant. Cytol. Histol. 2001, 23, 291–299. [Google Scholar] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| [0–1] | [2–3] | [4–6] | [7–8] | F-Score | |
|---|---|---|---|---|---|
| [0–1] | 38 | 5 | 0 | 0 | 0.531 |
| [2–3] | 62 | 34 | 5 | 0 | 0.338 |
| [4–6] | 0 | 54 | 88 | 23 | 0.664 |
| [7–8] | 0 | 7 | 7 | 76 | 0.804 |
| [0–1] | [2–3] | [4–6] | [7–8] | F-Score | |
|---|---|---|---|---|---|
| [0–1] | 47 | 7 | 1 | 0 | 0.606 |
| [2–3] | 47 | 37 | 3 | 0 | 0.396 |
| [4–6] | 6 | 53 | 86 | 37 | 0.610 |
| [7–8] | 0 | 3 | 10 | 63 | 0.716 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazo, C.; Orue-Etxebarria, E.; Zabalza, I.; Vivanco, M.d.M.; Kypta, R.M.; Beristain, A. In Silico Approach for Immunohistochemical Evaluation of a Cytoplasmic Marker in Breast Cancer. Cancers 2018, 10, 517. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers10120517
Mazo C, Orue-Etxebarria E, Zabalza I, Vivanco MdM, Kypta RM, Beristain A. In Silico Approach for Immunohistochemical Evaluation of a Cytoplasmic Marker in Breast Cancer. Cancers. 2018; 10(12):517. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers10120517
Chicago/Turabian StyleMazo, Claudia, Estibaliz Orue-Etxebarria, Ignacio Zabalza, Maria d. M. Vivanco, Robert M. Kypta, and Andoni Beristain. 2018. "In Silico Approach for Immunohistochemical Evaluation of a Cytoplasmic Marker in Breast Cancer" Cancers 10, no. 12: 517. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers10120517