Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-cell Lymphoma

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design and Patients
2.2. Histopathological Review and Immunohistochemistry
2.3. Flow Cytometry Analysis
2.4. Clonality Analysis and IGHV Gene Sequencing
2.5. Fluorescence in Situ Hybridization Analysis
2.6. Endpoints and Statistical Methods
3. Results
3.1. The Combination of Histology and Flow Cytometry Improved the Bone Marrow Involvement Classification
3.2. Clonality Studies Revealed a Unique Clone in most of the Discordant Cases
3.3. FISH Analysis Did Not Find Different Genetic Abnormalities between Concordant and Discordant Groups
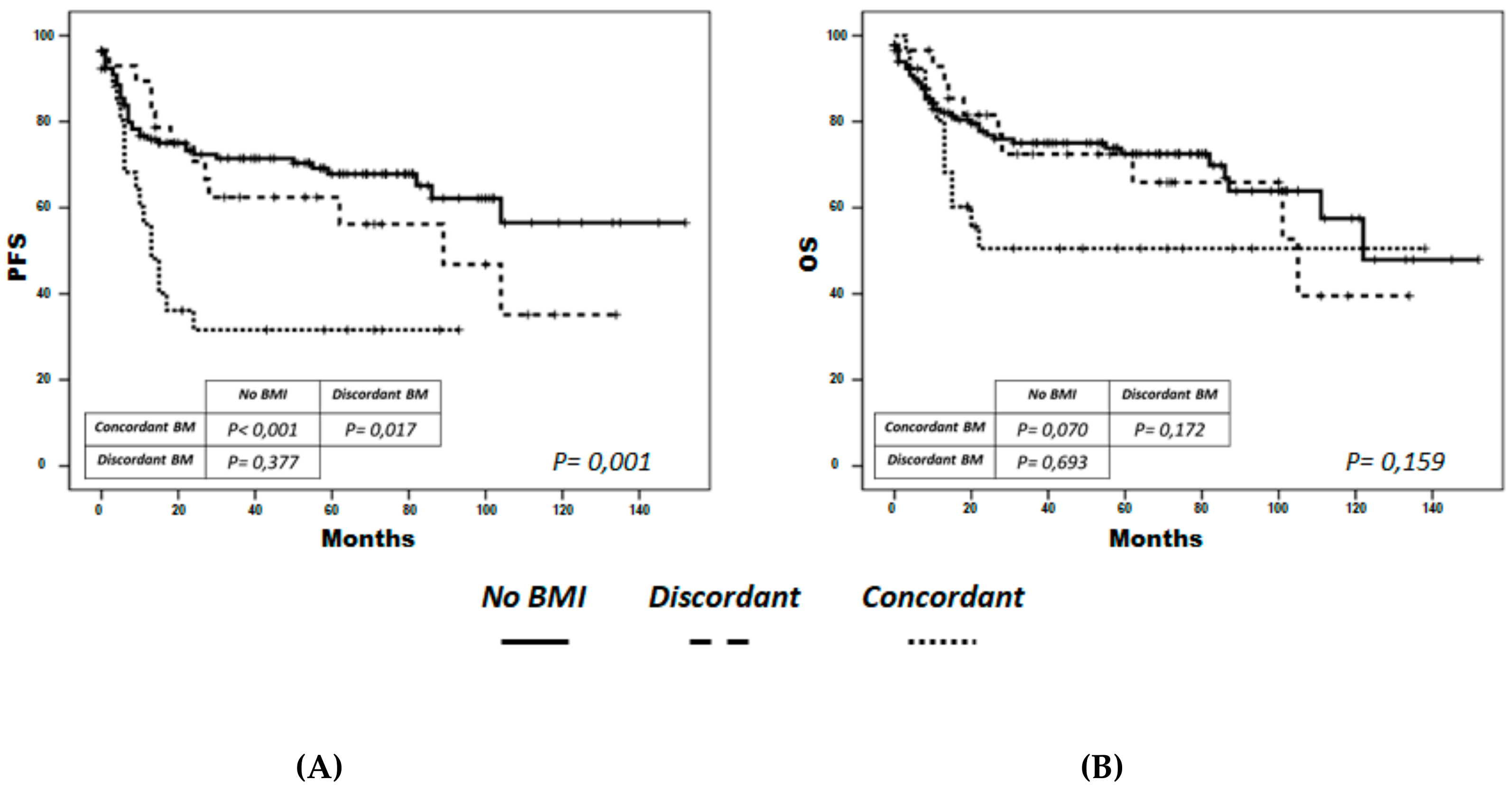
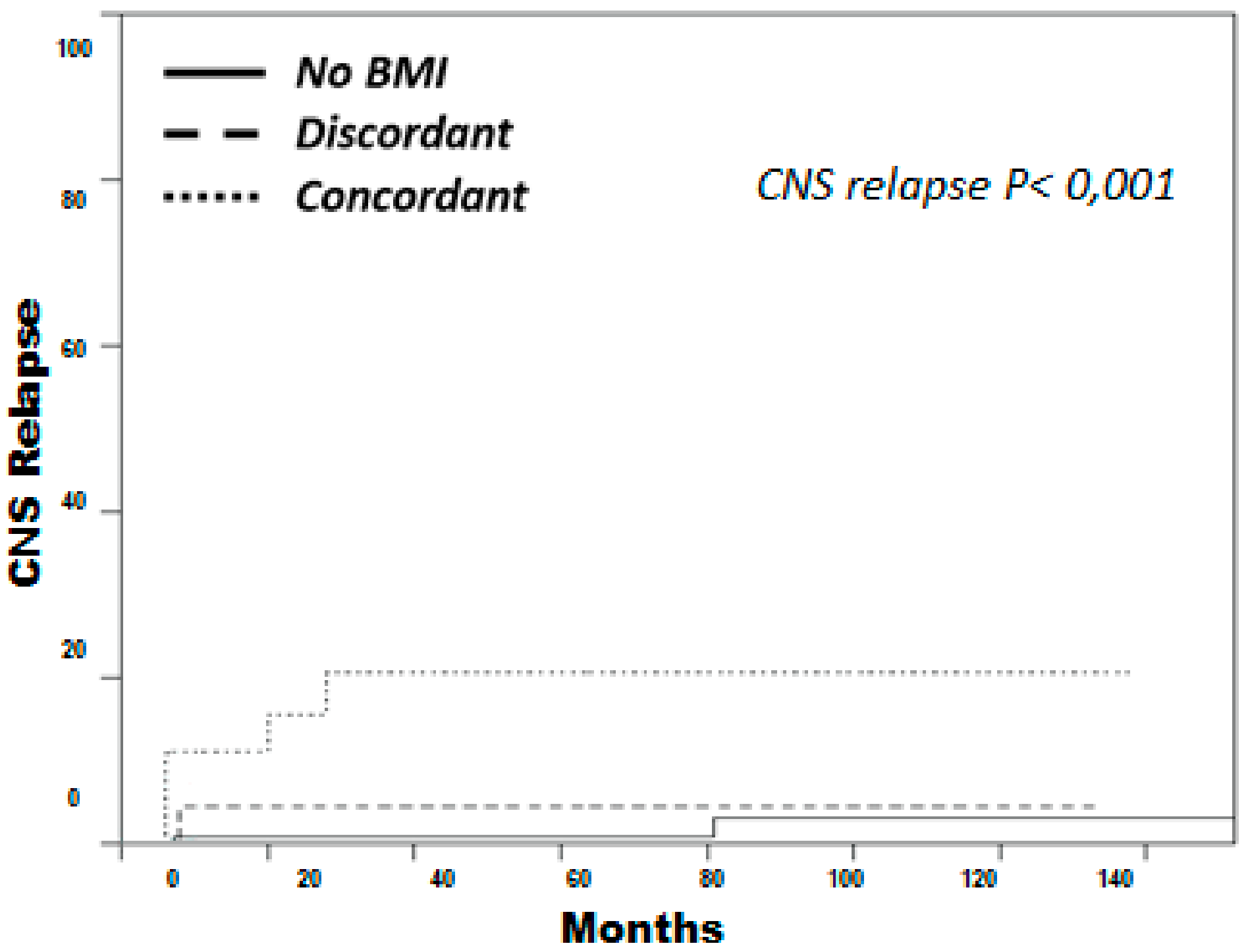
3.4. Concordant BM Cases Displayed Shorter PFS and Higher Incidence of CNS Relapse
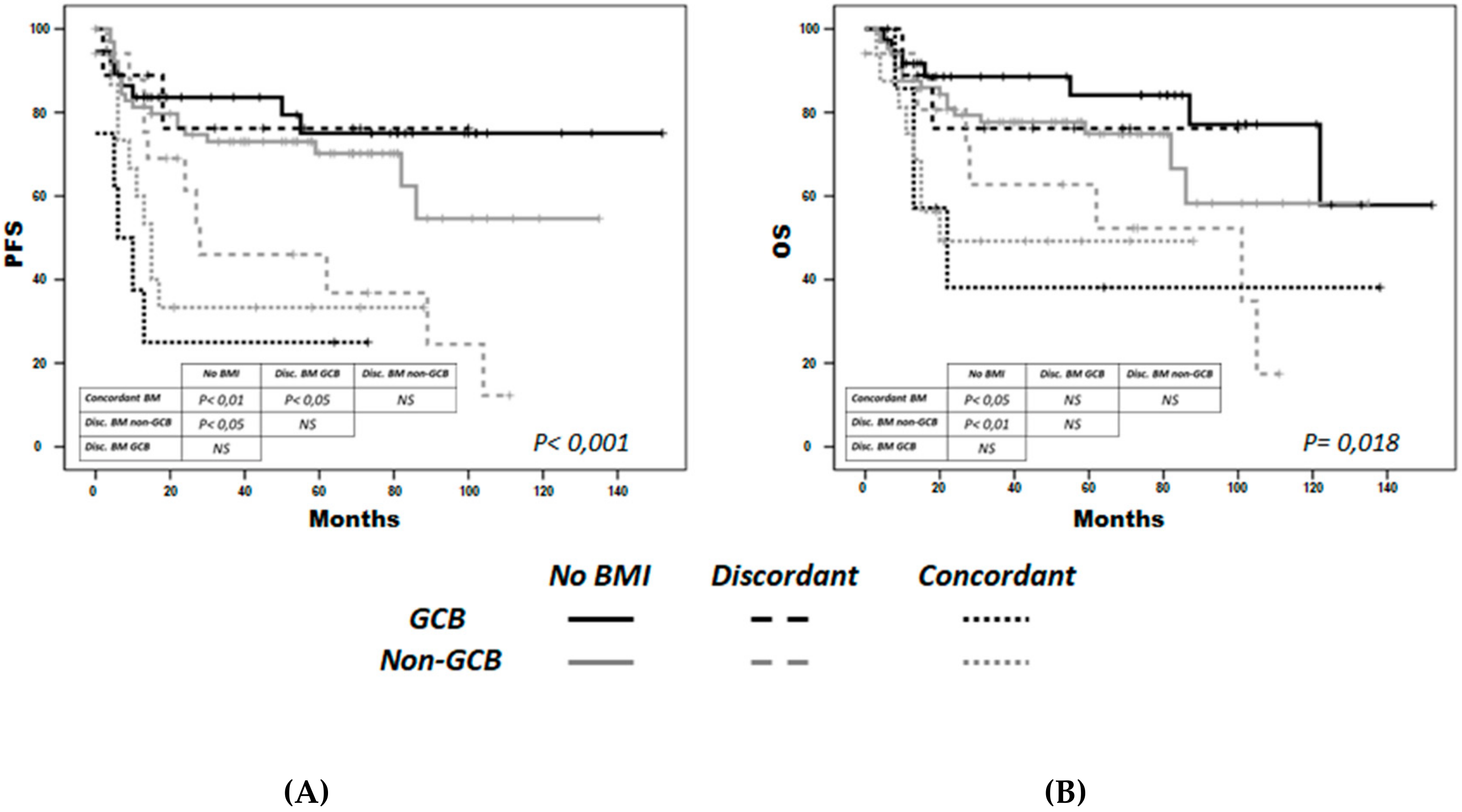
3.5. Non-GCB discordant BM Cases Could Display Shorter PFS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chigrinova, E.; Mian, M.; Scandurra, M.; Greiner, T.C.; Chan, W.C.; Vose, J.M.; Inghirami, G.; Chiappella, A.; Baldini, L.; Ponzoni, M.; et al. Diffuse large B-cell lymphoma with concordant bone marrow involvement has peculiar genomic profile and poor clinical outcome. Hematol. Oncol. 2011, 29, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Sehn, L.H.; Scott, D.W.; Chhanabhai, M.; Berry, B.; Ruskova, A.; Berkahn, L.; Connors, J.M.; Gascoyne, R.D. Impact of concordant and discordant bone marrow involvement on outcome in diffuse large B-cell lymphoma treated with R-CHOP. J. Clin. Oncol. 2011, 29, 1452–1457. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.; Oh, J.I.; Park, S.H.; Jang, S.; Park, C.J.; Huh, J.; Suh, C.; Chi, H.S. Prognostic impact of concordant and discordant cytomorphology of bone marrow involvement in patients with diffuse, large, B-cell lymphoma treated with R-CHOP. J. Clin. Pathol. 2013, 66, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Park, M.J.; Park, S.H.; Park, P.W.; Seo, Y.H.; Kim, K.H.; Seo, J.Y.; Jeong, J.H.; Kim, M.J.; Ahn, J.Y.; Hong, J. Prognostic impact of concordant and discordant bone marrow involvement and cell-of-origin in Korean patients with diffuse large B-cell lymphoma treated with R-CHOP. J. Clin. Pathol. 2015, 68, 733–738. [Google Scholar] [CrossRef]
- Brudno, J.; Tadmor, T.; Pittaluga, S.; Nicolae, A.; Polliack, A.; Dunleavy, K. Discordant bone marrow involvement in non-Hodgkin lymphoma. Blood 2016, 127, 965–970. [Google Scholar] [CrossRef] [Green Version]
- Song, M.K.; Chung, J.S.; Lee, J.J.; Yang, D.H.; Kim, I.S.; Shin, D.H.; Shin, H.J. High Ki-67 expression in involved bone marrow predicts worse clinical outcome in diffuse large B cell lymphoma patients treated with R-CHOP therapy. Int. J. Hematol. 2015, 101, 140–147. [Google Scholar] [CrossRef]
- Lee, K.W.; Yi, J.; Choi, I.S.; Kim, J.H.; Bang, S.M.; Kim, D.W.; Im, S.A.; Kim, T.Y.; Yoon, S.S.; Lee, J.S.; et al. Risk factors for poor treatment outcome and central nervous system relapse in diffuse large B-cell lymphoma with bone marrow involvement. Ann. Hematol. 2009, 88, 829–838. [Google Scholar] [CrossRef]
- Tomita, N.; Takasaki, H.; Ishiyama, Y.; Kishimoto, K.; Ishibashi, D.; Koyama, S.; Ishii, Y.; Takahashi, H.; Numata, A.; Watanabe, R.; et al. Intrathecal methotrexate prophylaxis and central nervous system relapse in patients with diffuse large B-cell lymphoma following rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone. Leuk Lymphoma 2015, 56, 725–729. [Google Scholar] [CrossRef]
- Kremer, M.; Spitzer, M.; Mandl-Weber, S.; Stecker, K.; Schmidt, B.; Höfler, H.; Quintanilla-Martinez, L.; Fend, F. Discordant bone marrow involvement in diffuse large B-cell lymphoma: Comparative molecular analysis reveals a heterogeneous group of disorders. Lab Investig. 2003, 83, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Fisher, D.E.; Jacobson, J.O.; Ault, K.A.; Harris, N.L. Diffuse large cell lymphoma with discordant bone marrow histology. Clinical features and biological implications. Cancer 1989, 64, 1879–1887. [Google Scholar] [CrossRef]
- Hans, C.P.; Weisenburger, D.D.; Greiner, T.C.; Gascoyne, R.D.; Delabie, J.; Ott, G.; Muller-Hermelink, H.K.; Campo, E.; Braziel, R.M.; Jaffe, E.S.; et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004, 103, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, M.L.; Almeida, J.; Vidriales, B.; Lopez-Berges, M.C.; Garcia-Marcos, M.A.; Moro, M.J.; Corrales, A.; Calmuntia, M.J.; San Miguel, J.F.; Orfao, A. Incidence of phenotypic aberrations in a series of 467 patients with B chronic lymphoproliferative disorders: Basis for the design of specific four-color stainings to be used for minimal residual disease investigation. Leukemia 2002, 16, 1460–1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrena, S.; Almeida, J.; Del Carmen García-Macias, M.; López, A.; Rasillo, A.; Sayagués, J.M.; Rivas, R.A.; Gutierrez, M.L.; Ciudad, J.; Flores, T.; et al. Flow cytometry immunophenotyping of fine-needle aspiration specimens: Utility in the diagnosis and classification of non-Hodgkin lymphomas. Histopathology 2011, 58, 906–918. [Google Scholar] [CrossRef] [Green Version]
- Van Dongen, J.J.M.; Langerak, A.W.; Brüggemann, M.; Evans, P.A.S.; Hummel, M.; Lavender, F.L.; Delabesse, E.; Davi, F.; Schuuring, E.; Garcia-Sanz, R.; et al. Design and standardization of PCR primers and protocols for detection of clonal immunoglobulin and T-cell receptor gene recombinations in suspect lymphoproliferations: Report of the BIOMED-2 Concerted Action BMH4-CT98-3936. Leukemia 2003, 17, 2257–2317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sehn, L.H.; Berry, B.; Chhanabhai, M.; Fitzgerald, C.; Gill, K.; Hoskins, P.; Klasa, R.; Savage, K.J.; Shenkier, T.; Sutherland, J.; et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood 2007, 109, 1857–1861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitz, N.; Zeynalova, S.; Nickelsen, M.; Kansara, R.; Villa, D.; Sehn, L.H.; Glass, B.; Scott, D.W.; Gascoyne, R.D.; Connors, J.M.; et al. CNS International Prognostic Index: A Risk Model for CNS Relapse in Patients With Diffuse Large B-Cell Lymphoma Treated With R-CHOP. J. Clin. Oncol. 2016, 34, 3150–3156. [Google Scholar] [CrossRef]
- Martín, A.; Conde, E.; Arnan, M.; Canales, M.A.; Deben, G.; Sancho, J.M.; Andreu, R.; Salar, A.; Garcia-Sanchez, P.; Vazquez, L.; et al. R-ESHAP as salvage therapy for patients with relapsed or refractory diffuse large B-cell lymphoma: The influence of prior exposure to rituximab on outcome. A GEL/TAMO study. Haematologica 2008, 93, 1829–1836. [Google Scholar] [CrossRef] [Green Version]
- Yao, Z.; Deng, L.; Xu-Monette, Z.Y.; Manyam, G.C.; Jain, P.; Tzankov, A.; Visco, C.; Bhagat, G.; Wang, J.; Dybkaer, K.; et al. Concordant bone marrow involvement of diffuse large B-cell lymphoma represents a distinct clinical and biological entity in the era of immunotherapy. Leukemia 2018, 32, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Peñalver, F.J.; Sancho, J.M.; de la Fuente, A.; Olave, M.T.; Martín, A.; Panizo, C.; Perez, E.; Salar, A.; Orfao, A. Guidelines for diagnosis, prevention and management of central nervous system involvement in diffuse large B-cell lymphoma patients by the Spanish Lymphoma Group (GELTAMO). Haematologica 2017, 102, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Cabezas-Quintario, M.A.; Gomez, P.; Yuste-Del Pozo, V.; Valencia-Mesa, A.L.; Sosa, G.; Ricard, P.; Hijas-Gomez, A.I.; Pinedo, F.; Arguelles, M. Bone marrow trephine biopsy involvement by lymphoma: Pattern of involvement and concordance with flow cytometry, in 10 years from a single institution. Clin. Transl. Oncol. 2015, 18, 537–540. [Google Scholar] [CrossRef]
- Van Dongen, J.J.M.; Lhermitte, L.; Böttcher, S.; Almeida, J.; Van der Velden, V.H.J.; Flores-Montero, J.; Rawstron, A.; Asnafi, V.; Lecrevisse, Q.; Lucio, P.; et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia 2012, 26, 1908–1975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortés-Romera, M.; Sabaté-Llobera, A.; Mercadal-Vilchez, S.; Climent-Esteller, F.; Serrano-Maestro, A.; Gámez-Cenzano, C.; González-Barca, E. Bone marrow evaluation in initial staging of lymphoma: 18F-FDG PET/CT versus bone marrow biopsy. Clin. Nucl. Med. 2014, 39, e46–e52. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.B.; Barrington, S.F.; Mikhaeel, N.G.; Hunt, A.A.; Cameron, L.; Morris, T.; Carr, R. PET-CT staging of DLBCL accurately identifies and provides new insight into the clinical significance of bone marrow involvement. Blood 2013, 122, 61–67. [Google Scholar] [CrossRef]
- Jerusalem, G.; Beguin, Y.; Najjar, F.; Hustinx, R.; Fassotte, M.F.; Rigo, P.; Fillet, G. Positron emission tomography (PET) with 18F-fluorodeoxyglucose (18F-FDG) for the staging of low-grade non-Hodgkin’s lymphoma (NHL). Ann. Oncol. 2001, 12, 825–830. [Google Scholar] [CrossRef]
- Chigrinova, E.; Rinaldi, A.; Kwee, I.; Rossi, D.; Rancoita, P.M.; Strefford, J.C.; Oscier, D.; Stamatopoulos, K.; Papadaki, T.; Berger, F.; et al. Two main genetic pathways lead to the transformation of chronic lymphocytic leukemia to Richter syndrome. Blood 2013, 122, 2673–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okosun, J.; Bödör, C.; Wang, J.; Araf, S.; Yang, C.Y.; Pan, C.; Boller, S.; Cittaro, D.; Bozek, M.; Iqbal, S.; et al. Integrated genomic analysis identifies recurrent mutations and evolution patterns driving the initiation and progression of follicular lymphoma. Nat. Genet. 2014, 46, 176–181. [Google Scholar] [CrossRef]
- Pasqualucci, L.; Khiabanian, H.; Fangazio, M.; Vasishtha, M.; Messina, M.; Holmes, A.B.; Ouillette, P.; Trifonov, V.; Rossi, D.; Tabbo, F.; et al. Genetics of follicular lymphoma transformation. Cell Rep. 2014, 6, 130–140. [Google Scholar] [CrossRef] [Green Version]
- Jiménez, C.; Alonso-Álvarez, S.; Alcoceba, M.; Ordóñez, G.R.; García-Álvarez, M.; Prieto-Conde, M.I.; Chillón, M.C.; Balanzategui, A.; Corral, R.; Marín, L.A.; et al. From Waldenström’s macroglobulinemia to aggressive diffuse large B-cell lymphoma: A whole-exome analysis of abnormalities leading to transformation. Blood Cancer J. 2017, 7, e591. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, J.; Sanger, W.G.; Horsman, D.E.; Rosenwald, A.; Pickering, D.L.; Dave, B.; Dave, S.; Xiao, L.; Cao, K.; Zhu, Q.; et al. BCL2 translocation defines a unique tumor subset within the germinal center B-cell-like diffuse large B-cell lymphoma. Am. J. Pathol. 2004, 165, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Visco, C.; Tzankov, A.; Xu-Monette, Z.Y.; Miranda, R.N.; Tai, Y.C.; Li, Y.; Liu, W.M.; d’Amore, E.S.; Li, Y.; Montes-Moreno, S.; et al. Patients with diffuse large B-cell lymphoma of germinal center origin with BCL2 translocations have poor outcome, irrespective of MYC status: A report from an International DLBCL rituximab-CHOP Consortium Program Study. Haematologica 2013, 98, 255–263. [Google Scholar] [CrossRef]
- Ennishi, D.; Mottok, A.; Ben-Neriah, S.; Shulha, H.P.; Farinha, P.; Chan, F.C.; Meissner, B.; Boyle, M.; Hother, C.; Kridel, R.; et al. Genetic profiling of MYC and BCL2 in diffuse large B-cell lymphoma determines cell of origin-specific clinical impact. Blood 2017, 129, 2760–2770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapuy, B.; Stewart, C.; Dunford, A.J.; Kim, J.; Kamburov, A.; Redd, R.A.; Lawrence, M.S.; Roemer, M.G.M.; Li, A.J.; Ziepert, M.; et al. Molecular subtypes of diffuse large B cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat. Med. 2018, 24, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Testoni, M.; Kwee, I.; Greiner, T.C.; Montes-Moreno, S.; Vose, J.; Chan, W.C.; Chiappella, A.; Baldini, L.; Ferreri, A.J.; Gaidano, G.; et al. Gains of MYC locus and outcome in patients with diffuse large B-cell lymphoma treated with R-CHOP. Br. J. Haematol. 2011, 155, 274–277. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Non-infiltrated BM (n = 159) | Discordant BM (n = 37) | Concordant BM (n = 36) | p |
|---|---|---|---|---|
| Gender (Male) | 82 (52%) | 12 (32%) | 20 (56%) | 0.07 |
| Age > 60 years | 106 (67%) | 27 (73%) | 20 (56%) | 0.3 |
| Ann Arbor stage > 2 | 91 (58%) | 37 (100%) | 36 (100%) | <0.001 |
| LDH (high) * | 50 (39%) | 13 (41%) | 20 (77%) | 0.0018 |
| Extranodal sites > 1 * | 27 (20%) | 16 (48%) | 19 (68%) | <0.001 |
| ECOG ≥ 2 * | 41 (32%) | 8 (25%) | 14 (54%) | 0.05 |
| R-IPI > 2 * | 54 (41%) | 20 (59%) | 22 (85%) | <0.001 |
| COO non-GCB * | 64 (63%) | 19 (62%) | 19 (64%) | 0.99 |
| Histology | FCM | |||||||
|---|---|---|---|---|---|---|---|---|
| DLBCL | DLBCL+FL | FL | CLL | MZL-like | LPL-like | NS | Non-Infiltrated | |
| High-grade (Concordant BM, n = 35) | 21 | − | 3 | − | − | − | 1 | 10 |
| Low-grade (Discordant BM, n = 21) | 1 | 1 | 3 | 4 | 2 | − | 6 | 4 |
| Unspecified lymphoid infiltrate (n = 31) * | 1 | − | 4 | 4 | 2 | 1 | 4 | 15 |
| UPN | Sample | % FCM | (14;18) (IGH/BCL2) | 8q24 (MYC) | 3q26 (BCL6) | 17p13.1 (TP53) | COO | BM |
|---|---|---|---|---|---|---|---|---|
| 3470 | LN | 60 | Clonal | Clonal | Clonal | Normal | GCB | C |
| 7062 | LN | 9,5 | Clonal | Normal | Normal | Normal | GCB | C |
| 4512 | BM | 21 | Normal | Normal | Normal | Normal | GCB | C |
| 3999 | LN | 12 | Normal | Normal | Normal | Normal | GCB | C |
| 9102 | BM | 15 | Clonal | Normal | Gain | Normal | GCB | C |
| 9225 | LN | 66,7 | Clonal | Clonal | Normal | Normal | GCB | C |
| 2704 | BM | 15 | Gain | Normal | Normal | Normal | Non-GCB | C |
| 3985 * | LN | 47 | Gain | Gain | Gain | Gain | Non-GCB | C |
| 6908 | LN | 15 | Normal | Normal | Normal | Normal | Non-GCB | C |
| 6156 † | LN | NA | Gain | Gain | Gain | Gain | Non-GCB | C |
| 7288 | LN | 69 | Gain | Normal | NS | Normal | Non-GCB | C |
| 5296 | LN | 15 | Normal | Normal | Normal | Normal | Non-GCB | C |
| 8275 | BM | 36,6 | Normal | Normal | Normal | Normal | Non-GCB | C |
| 9043 | LN–FFPE | NA | Gain | Clonal | Normal | NS | Non-GCB | C |
| 4859 | LN | NA | Clonal | Gain | Normal | Normal | GCB | D |
| 4989 | LN | 75 | Clonal | Normal | Clonal | Normal | GCB | D |
| 7029 | LN | 78 | Normal | Gain | Gain | Normal | GCB | D |
| 8724 * | LN | 93 | Clonal | Clonal | Gain | Gain | GCB | D |
| 3671 | LN | 60 | Normal | Normal | Normal | Normal | Non-GCB | D |
| 8818 | LN | 48 | Clonal | Gain | Normal | Normal | Non-GCB | D |
| 9386 | LN | 64 | Gain | Gain | Gain | Deletion | Non-GCB | D |
| Variable | PFS | OS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Bone marrow infiltration | − | − | − | − | − | − |
| No infiltration (reference) | − | − | − | − | − | − |
| Concordant | 2.2 | 1.1-4.3 | 0.02 | 1.6 | 0.7-3.4 | 0.2 |
| Discordant | 1.5 | 0.7-3 | 0.2 | 1.5 | 0.7-3.2 | 0.3 |
| R-IPI score (0 to 5) | 1.3 | 1.0-1.5 | 0.03 | 1.4 | 1.1-1.8 | 0.004 |
| Bone marrow infiltration and COO | ||||||
| No infiltration (reference) | − | − | − | − | − | − |
| Concordant GCB | 2.9 | 1–8.7 | 0.04 | 1.2 | 0.3–4.4 | 0.2 |
| Concordant Non-GCB | 3 | 1.4–6.4 | 0.003 | 1.6 | 0.7–3.9 | 0.3 |
| Discordant GCB | 0.7 | 0.1–3 | 0.6 | 0.7 | 0.1–3.4 | 0.7 |
| Discordant Non-GCB | 1.9 | 0.9–4.2 | 0.08 | 1.6 | 0.6–3.7 | 0.3 |
| R-IPI score (0 to 5) | 1.2 | 0.9–1.5 | 0.1 | 1.5 | 1.2–1.9 | <0.001 |
| Variable | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| 5-Year CNS Incidence | p-Value | p-Value | HR | 95% CI | |
| Bone marrow infiltration No infiltration Discordant Concordant | 0.8% 7.3% 3.1% | <0.001 | 0.003 | 10.1 | 2.2–46.3 |
| Renal/Adrenal involvement No Yes | 3.8% 22.2% | 0.007 | 0.017 | 7.8 | 1.5–42 |
| Lactate dehydrogenase No Yes | 3.5% 13% | 0.3 | − | − | − |
| ECOG 0–1 2–4 | 4.2% 10% | 0.8 | − | − | − |
| Ann Arbor stage <3 ≥3 | 8% 7% | 0.4 | − | − | − |
| Extranodal sites <2 ≥2 | 3.7% 12.5% | 0.1 | − | − | − |
| Cell of origin GCB Non-GCB | 6.8% 3.5% | 0.8 | − | − | − |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Álvarez, S.; Alcoceba, M.; García-Álvarez, M.; Blanco, O.; Rodríguez, M.; Baile, M.; Caballero, J.C.; Dávila, J.; Vidriales, M.B.; Esteban, C.; et al. Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-cell Lymphoma. Cancers 2020, 12, 474. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12020474
Alonso-Álvarez S, Alcoceba M, García-Álvarez M, Blanco O, Rodríguez M, Baile M, Caballero JC, Dávila J, Vidriales MB, Esteban C, et al. Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-cell Lymphoma. Cancers. 2020; 12(2):474. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12020474
Chicago/Turabian StyleAlonso-Álvarez, Sara, Miguel Alcoceba, María García-Álvarez, Oscar Blanco, Marta Rodríguez, Mónica Baile, Juan Carlos Caballero, Julio Dávila, María Belén Vidriales, Carmen Esteban, and et al. 2020. "Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-cell Lymphoma" Cancers 12, no. 2: 474. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12020474