Genetic Analysis Reveals a Significant Contribution of CES1 to Prostate Cancer Progression in Taiwanese Men

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment and Data Collection
2.2. SNP Selection and Genotyping
2.3. Bioinformatics Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. Ca Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Amundadottir, L.T.; Sulem, P.; Gudmundsson, J.; Helgason, A.; Baker, A.; Agnarsson, B.; Sigurdsson, A.; Benediktsdottir, K.R.; Cazier, J.-B.; Sainz, J.; et al. A common variant associated with prostate cancer in European and African populations. Nat. Genet. 2006, 38, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Yeager, M.; Orr, N.; Hayes, R.B.; Jacobs, K.; Kraft, P.; Wacholder, S.; Minichiello, M.J.; Fearnhead, P.; Yu, K.; Chatterjee, N.; et al. Genome-wide association study of prostate cancer identifies a second risk locus at 8q24. Nat. Genet. 2007, 39, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, F.R.; Al Olama, A.A.; Berndt, S.I.; Benlloch, S.; Ahmed, M.; Saunders, E.; Dadaev, T.; Leongamornlert, D.; Anokian, E.; Cieza-Borrella, C.; et al. Association analyses of more than 140,000 men identify 63 new prostate cancer susceptibility loci. Nat. Genet. 2018, 50, 928–936. [Google Scholar] [CrossRef] [Green Version]
- Farashi, S.; Kryza, T.; Clements, J.; Batra, J. Post-GWAS in prostate cancer: From genetic association to biological contribution. Nat. Rev. Cancer 2018, 19, 46–59. [Google Scholar] [CrossRef]
- Li, W.; Middha, M.; Bicak, M.; Sjoberg, D.; Vertosick, E.; Dahlin, A.; Häggström, C.; Hallmans, G.; Rönn, A.-C.; Stattin, P.; et al. Genome-wide Scan Identifies Role for AOX1 in Prostate Cancer Survival. Eur. Urol. 2018, 74, 710–719. [Google Scholar] [CrossRef]
- Szulkin, R.; Karlsson, R.; Whitington, T.; Aly, M.; Gronberg, H.; Eeles, R.; Easton, U.F.; Kote-Jarai, Z.; Al Olama, A.A.; Benlloch, S.; et al. Genome-wide association study of prostate cancer-specific survival. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1796–1800. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.-N.; Huang, S.-P.; Pao, J.-B.; Chang, T.-Y.; Lan, Y.-H.; Lu, T.-L.; Lee, H.-Z.; Juang, S.-H.; Wu, P.-P.; Pu, Y.-S.; et al. Genetic polymorphisms in androgen receptor-binding sites predict survival in prostate cancer patients receiving androgen-deprivation therapy. Ann. Oncol. 2012, 23, 707–713. [Google Scholar] [CrossRef]
- Lindström, S.; Adami, H.-O.; Bälter, K.A.; Xu, J.; Zheng, S.L.; Stattin, P.; Grönberg, H.; Wiklund, F. Inherited Variation in Hormone-Regulating Genes and Prostate Cancer Survival. Clin. Cancer Res. 2007, 13, 5156–5161. [Google Scholar] [CrossRef] [Green Version]
- Ross, M.; Crow, J.A. Human carboxylesterases and their role in xenobiotic and endobiotic metabolism. J. Biochem. Mol. Toxicol. 2007, 21, 187–196. [Google Scholar] [CrossRef]
- Holmes, R.S.; Wright, M.; Laulederkind, S.J.F.; Cox, L.A.; Hosokawa, M.; Imai, T.; Ishibashi, S.; Lehner, R.; Miyazaki, M.; Perkins, E.J.; et al. Recommended nomenclature for five mammalian carboxylesterase gene families: Human, mouse, and rat genes and proteins. Mamm. Genome 2010, 21, 427–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosokawa, M. Structure and Catalytic Properties of Carboxylesterase Isozymes Involved in Metabolic Activation of Prodrugs. Molecules 2008, 13, 412–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanghani, S.P.; Sanghani, P.C.; Schiel, M.A.; Bosron, W. Human carboxylesterases: An update on CES1, CES2 and CES3. Protein Pept. Lett. 2009, 16, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Ose, A.; Kusuhara, H.; Yamatsugu, K.; Kanai, M.; Shibasaki, M.; Fujita, T.; Yamamoto, A.; Sugiyama, Y. P-glycoprotein Restricts the Penetration of Oseltamivir Across the Blood-Brain Barrier. Drug Metab. Dispos. 2007, 36, 427–434. [Google Scholar] [CrossRef]
- Cai, L.; Tang, X.; Guo, L.; An, Y.; Wang, Y.; Zheng, J. Decreased serum levels of carboxylesterase-2 in patients with ovarian cancer. Tumori J. 2009, 95, 473–478. [Google Scholar] [CrossRef]
- Tang, X.; Wu, H.; Wu, Z.; Wang, G.; Wang, Z.; Zhu, D. Carboxylesterase 2 is Downregulated in Colorectal Cancer Following Progression of the Disease. Cancer Investig. 2008, 26, 178–181. [Google Scholar] [CrossRef]
- Cecchin, E.; Corona, G.; Masier, S.; Biason, P.; Cattarossi, G.; Frustaci, S.; Buonadonna, A.; Colussi, A.; Toffoli, G. Carboxylesterase Isoform 2 mRNA Expression in Peripheral Blood Mononuclear Cells Is a Predictive Marker of the Irinotecan to SN38 Activation Step in Colorectal Cancer Patients. Clin. Cancer Res. 2005, 11, 6901–6907. [Google Scholar] [CrossRef] [Green Version]
- Chiorean, E.G.; Sanghani, S.; Schiel, M.A.; Yu, M.; Burns, M.; Tong, Y.; Hinkle, D.T.; Coleman, N.; Robb, B.; Leblanc, J.; et al. Phase II and gene expression analysis trial of neoadjuvant capecitabine plus irinotecan followed by capecitabine-based chemoradiotherapy for locally advanced rectal cancer: Hoosier Oncology Group GI03-53. Cancer Chemother. Pharmacol. 2012, 70, 25–32. [Google Scholar] [CrossRef]
- Ribelles, N.; Lopez-Siles, J.; Sanchez, A.; Gonzalez, E.; Sánchez, M.J.; Carabantes, F.; Sanchez-Rovira, P.; Marquez, A.; Duenas, R.; Sevilla, I.; et al. A carboxylesterase 2 gene polymorphism as predictor of capecitabine on response and time to progression. Curr. Drug Metab. 2008, 9, 336–343. [Google Scholar] [CrossRef]
- Huang, S.-P.; Huang, L.-C.; Ting, W.-C.; Chen, L.M.; Chang, T.-Y.; Lu, T.-L.; Lan, Y.-H.; Liu, C.-C.; Yang, W.-H.; Lee, H.-Z.; et al. Prognostic Significance of Prostate Cancer Susceptibility Variants on Prostate-Specific Antigen Recurrence after Radical Prostatectomy. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3068–3074. [Google Scholar] [CrossRef] [Green Version]
- Freedland, S.J.; E Sutter, M.; Dorey, F.; Aronson, W.J. Defining the ideal cutpoint for determining PSA recurrence after radical prostatectomy. Urology 2003, 61, 365–369. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Huang, S.-P.; Lin, V.C.; Yu, C.-C.; Chang, T.-Y.; Juang, S.-H.; Bao, B.-Y. Genetic variants in the Hippo pathway predict biochemical recurrence after radical prostatectomy for localized prostate cancer. Sci. Rep. 2015, 5, 8556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, E.Y.; Chang, Y.-J.; Huang, S.-P.; Lin, V.C.; Yu, C.-C.; Huang, C.-Y.; Yin, H.-L.; Chang, T.-Y.; Lu, T.-L.; Bao, B. A common regulatory variant in SLC 35B4 influences the recurrence and survival of prostate cancer. J. Cell. Mol. Med. 2018, 22, 3661–3670. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-P.; Lévesque, E.; Guillemette, C.; Yu, C.-C.; Huang, C.-Y.; Lin, V.C.; Chung, I.-C.; Chen, L.-C.; Laverdière, I.; Lacombe, L.; et al. Genetic variants in microRNAs and microRNA target sites predict biochemical recurrence after radical prostatectomy in localized prostate cancer. Int. J. Cancer 2014, 135, 2661–2667. [Google Scholar] [CrossRef] [PubMed]
- 1000 Genomes Project Consotium; Abecasis, G.R.; Auton, A.; Brooks, L.D.; de Pristo, M.A.; Durbin, R.M.; Handsaker, R.E.; Kang, H.M.; Marth, G.T.; McVean, G.A. An integrated map of genetic variation from 1092 human genomes. Nature 2012, 491, 56–65. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.-N.; Huang, S.-P.; Pao, J.-B.; Hour, T.-C.; Chang, T.-Y.; Lan, Y.-H.; Lu, T.-L.; Lee, H.-Z.; Juang, S.-H.; Wu, P.-P.; et al. Genetic polymorphisms in oestrogen receptor-binding sites affect clinical outcomes in patients with prostate cancer receiving androgen-deprivation therapy. J. Intern. Med. 2011, 271, 499–509. [Google Scholar] [CrossRef]
- Das, S.; Forer, L.; Schönherr, S.; Sidore, C.; Locke, A.E.; Kwong, A.; I Vrieze, S.; Chew, E.Y.; Levy, S.; McGue, M.; et al. Next-generation genotype imputation service and methods. Nat. Genet. 2016, 48, 1284–1287. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Willer, C.J.; Ding, J.; Scheet, P.; Abecasis, G. MaCH: Using sequence and genotype data to estimate haplotypes and unobserved genotypes. Genet. Epidemiol. 2010, 34, 816–834. [Google Scholar] [CrossRef] [Green Version]
- Ward, L.D.; Kellis, M. HaploReg v4: Systematic mining of putative causal variants, cell types, regulators and target genes for human complex traits and disease. Nucleic Acid. Res. 2015, 44, 877–881. [Google Scholar] [CrossRef]
- Consortium, G.T. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 2013, 45, 580–585. [Google Scholar]
- Nakagawa, T.; Kollmeyer, T.M.; Morlan, B.W.; Anderson, S.K.; Bergstralh, E.J.; Davis, B.J.; Asmann, Y.W.; Klee, G.G.; Ballman, K.; Jenkins, R.B. A Tissue Biomarker Panel Predicting Systemic Progression after PSA Recurrence Post-Definitive Prostate Cancer Therapy. PLoS ONE 2008, 3, e2318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.; Lyons, C.; Walker, S.; McQuaid, S.; Hynes, S.; Mitchell, D.; Pang, B.; Logan, G.; McCavigan, A.; O’Rourke, D.; et al. Validation of a Metastatic Assay using biopsies to improve risk stratification in patients with prostate cancer treated with radical radiation therapy. Ann. Oncol. 2018, 29, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Sboner, A.; Demichelis, F.; Calza, S.; Pawitan, Y.; Setlur, S.R.; Hoshida, Y.; Perner, S.; Adami, H.-O.; Fall, K.; Mucci, L.; et al. Molecular sampling of prostate cancer: A dilemma for predicting disease progression. BMC Med. Genom. 2010, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Taylor, B.S.; Schultz, N.; Hieronymus, H.; Gopalan, A.; Xiao, Y.; Carver, B.S.; Arora, V.K.; Kaushik, P.; Cerami, E.; Reva, B.; et al. Integrative Genomic Profiling of Human Prostate Cancer. Cancer Cell 2010, 18, 11–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, Q.; Xu, J.; Osunkoya, A.O.; Sannigrahi, S.; Johnson, B.A.; Zhou, W.; Gillespie, T.; Park, J.Y.; Nam, R.K.; Sugar, L.; et al. Global transcriptome analysis of formalin-fixed prostate cancer specimens identifies biomarkers of disease recurrence. Cancer Res. 2014, 74, 3228–3237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross-Adams, H.; Lamb, A.D.; Dunning, M.; Halim, S.; Lindberg, J.; Massie, C.E.; Egevad, L.; Russell, R.; Ramos-Montoya, A.; Vowler, S.; et al. Integration of copy number and transcriptomics provides risk stratification in prostate cancer: A discovery and validation cohort study. EBioMedicine 2015, 2, 1133–1144. [Google Scholar] [CrossRef] [Green Version]
- Cancer Genome Atlas Research Network. Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Nature 2008, 455, 1061–1068. [Google Scholar] [CrossRef]
- Storey, J.; Tibshirani, R. Statistical significance for genomewide studies. Proc. Nat. Acad. Sci. USA 2003, 100, 9440–9445. [Google Scholar] [CrossRef] [Green Version]
- Taketani, M.; Shii, M.; Ohura, K.; Ninomiya, S.; Imai, T. Carboxylesterase in the liver and small intestine of experimental animals and human. Life Sci. 2007, 81, 924–932. [Google Scholar] [CrossRef]
- McCormick, J.A.; Markey, G.M.; Morris, T.C.M.; Auld, P.W.; Alexander, H.D. Lactoferrin inducible monocyte cytotoxicity defective in esterase deficient monocytes. Br. J. Haematol. 1991, 77, 287–290. [Google Scholar] [CrossRef]
- Burgaleta, C.; Villalba, S.; González, N. Defective activity of monocytes from patients with non-Hodgkin lymphoma. The modulatory effect of granulocyte-macrophage-colony stimulating factor. Cancer 1999, 86, 2133–2137. [Google Scholar] [CrossRef]
- Markey, G.M.; A McCormick, J.; Morris, T.C.; Alexander, H.D.; Nolan, L.; Morgan, L.M.; E Reynolds, M.; Edgar, S.; Bell, A.L.; McCaigue, M.D. Monocyte esterase deficiency in malignant neoplasia. J. Clin. Pathol. 1990, 43, 282–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Yan, B. Photochemotherapeutic Agent 8-Methoxypsoralen Induces Cytochrome P450 3A4 and Carboxylesterase HCE2: Evidence on an Involvement of the Pregnane X Receptor. Toxicol. Sci. 2006, 95, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Cheng, Q.; Ou, Z.; Lee, J.H.; Xu, M.; Kochhar, U.; Ren, S.; Huang, M.; Pflug, B.R.; Xie, W. Pregnane X receptor as a therapeutic target to inhibit androgen activity. Endocrinology 2010, 151, 5721–5729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- di Matteo, C.; D’Andrea, G.; Vecchione, G.; Paoletti, O.; Cappucci, F.; Tiscia, G.L.; Buono, M.; Grandone, E.; Testa, S.; Margaglione, M. Pharmacogenetics of dabigatran etexilate interindividual variability. Thromb. Res. 2016, 144, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Li, X.; Sun, S.; Mei, S.; Ma, N.; Miao, Z.; Peng, S. Impact of genetic polymorphisms related to clopidogrel or acetylsalicylic acid pharmacology on clinical outcome in Chinese patients with symptomatic extracranial or intracranial stenosis. Eur. J. Clin. Pharmacol. 2016, 72, 1195–1204. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n | BCR, n (%) | HR (95% CI) | P |
|---|---|---|---|---|
| Age at diagnosis, years | ||||
| Median (IQR) | 66.0 (62.0–70.0) | |||
| ≤66 | 331 | 115 (34.7) | 1.00 | |
| >66 | 312 | 113 (36.2) | 1.08 (0.83–1.40) | 0.552 |
| PSA at diagnosis, ng/mLa | ||||
| Median (IQR) | 10.9 (7.02–18.41) | |||
| ≤10 | 292 | 74 (25.3) | 1.00 | |
| >10 | 330 | 145 (43.9) | 2.23 (1.68–2.95) | <0.001 |
| Gleason score | ||||
| 2–7 | 531 | 164 (30.9) | 1.00 | |
| 8–10 | 112 | 64 (57.1) | 2.81 (2.10–3.76) | <0.001 |
| Stage a | ||||
| T1/T2 | 363 | 88 (24.2) | 1.00 | |
| T3/T4/N1 | 275 | 136 (49.5) | 2.79 (2.13–3.65) | <0.001 |
| Surgical margin | ||||
| Negative | 459 | 139 (30.3) | 1.00 | |
| Positive | 184 | 89 (48.4) | 2.02 (1.55–2.65) | <0.001 |
| Total | 643 | 228 (35.5) |
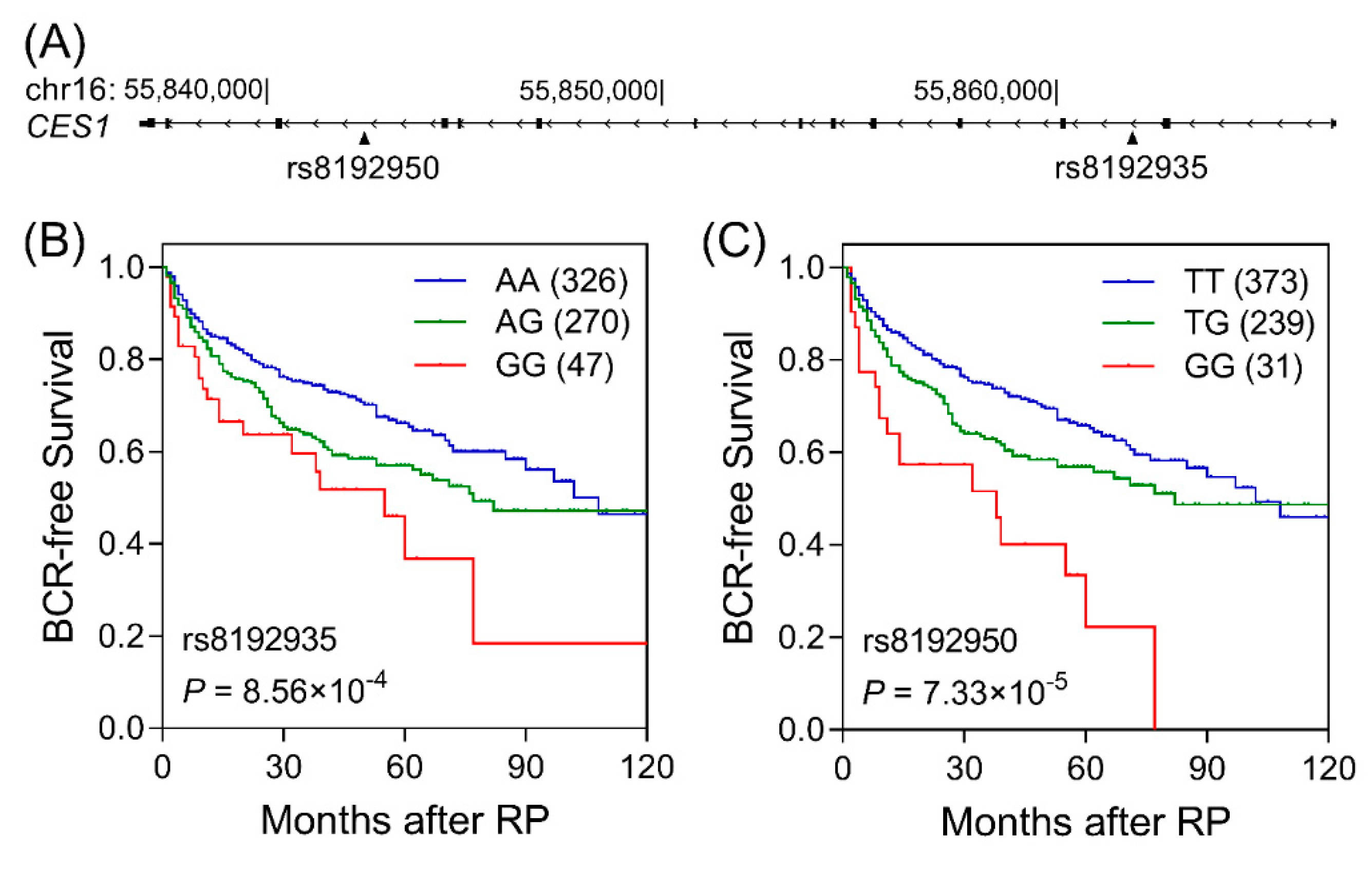
| Gene SNP | Position | Genotype | Frequency | BCR | HR (95% CI) | P | HR (95% CI) a | Pa |
|---|---|---|---|---|---|---|---|---|
| CES1 rs8192935 b | 55861794 | AA/AG/GG | 326/270/47 | 100/106/22 | 1.41 (1.15–1.72) | 9.64 × 10−4 | 1.43 (1.16–1.76) | 9.67 × 10−4 |
| CES1 rs8192950 | 55842404 | TT/TG/GG | 373/239/31 | 114/95/19 | 1.53 (1.24–1.89) | 8.96 × 10−5 | 1.50 (1.24–1.90) | 9.34 × 10−5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ke, C.-C.; Chen, L.-C.; Yu, C.-C.; Cheng, W.-C.; Huang, C.-Y.; Lin, V.C.; Lu, T.-L.; Huang, S.-P.; Bao, B.-Y. Genetic Analysis Reveals a Significant Contribution of CES1 to Prostate Cancer Progression in Taiwanese Men. Cancers 2020, 12, 1346. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051346
Ke C-C, Chen L-C, Yu C-C, Cheng W-C, Huang C-Y, Lin VC, Lu T-L, Huang S-P, Bao B-Y. Genetic Analysis Reveals a Significant Contribution of CES1 to Prostate Cancer Progression in Taiwanese Men. Cancers. 2020; 12(5):1346. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051346
Chicago/Turabian StyleKe, Chien-Chih, Lih-Chyang Chen, Chia-Cheng Yu, Wei-Chung Cheng, Chao-Yuan Huang, Victor C. Lin, Te-Ling Lu, Shu-Pin Huang, and Bo-Ying Bao. 2020. "Genetic Analysis Reveals a Significant Contribution of CES1 to Prostate Cancer Progression in Taiwanese Men" Cancers 12, no. 5: 1346. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051346