
Validation of the Combined Biomarker for Prediction of Response to Checkpoint Inhibitor in Patients with Advanced Cancer


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Statistical Analysis
2.3. Validation in Another Cohort+
3. Results
3.1. Patient Clinicopathologic Characteristics
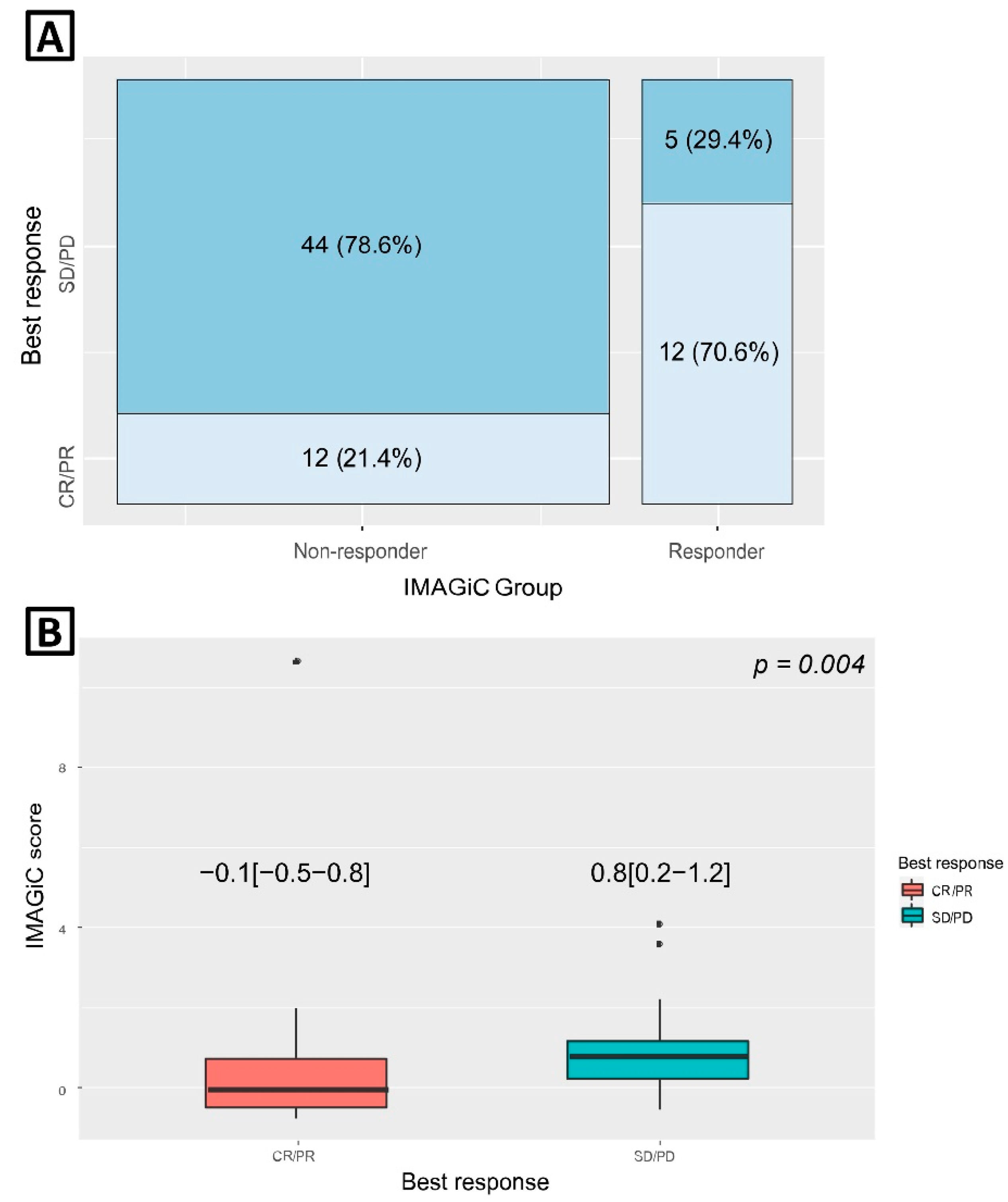
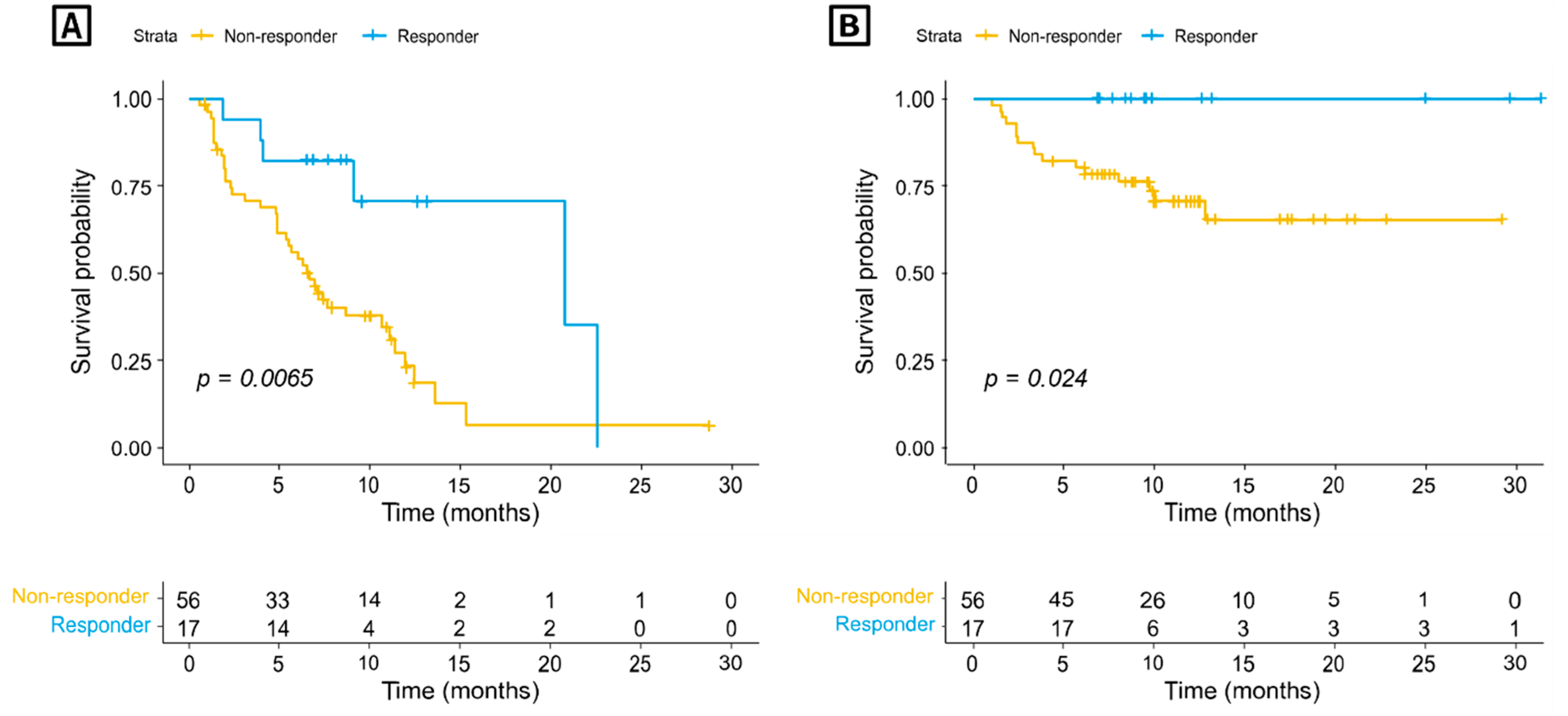
3.2. IMAGiC Score/Group and Treatment Outcome
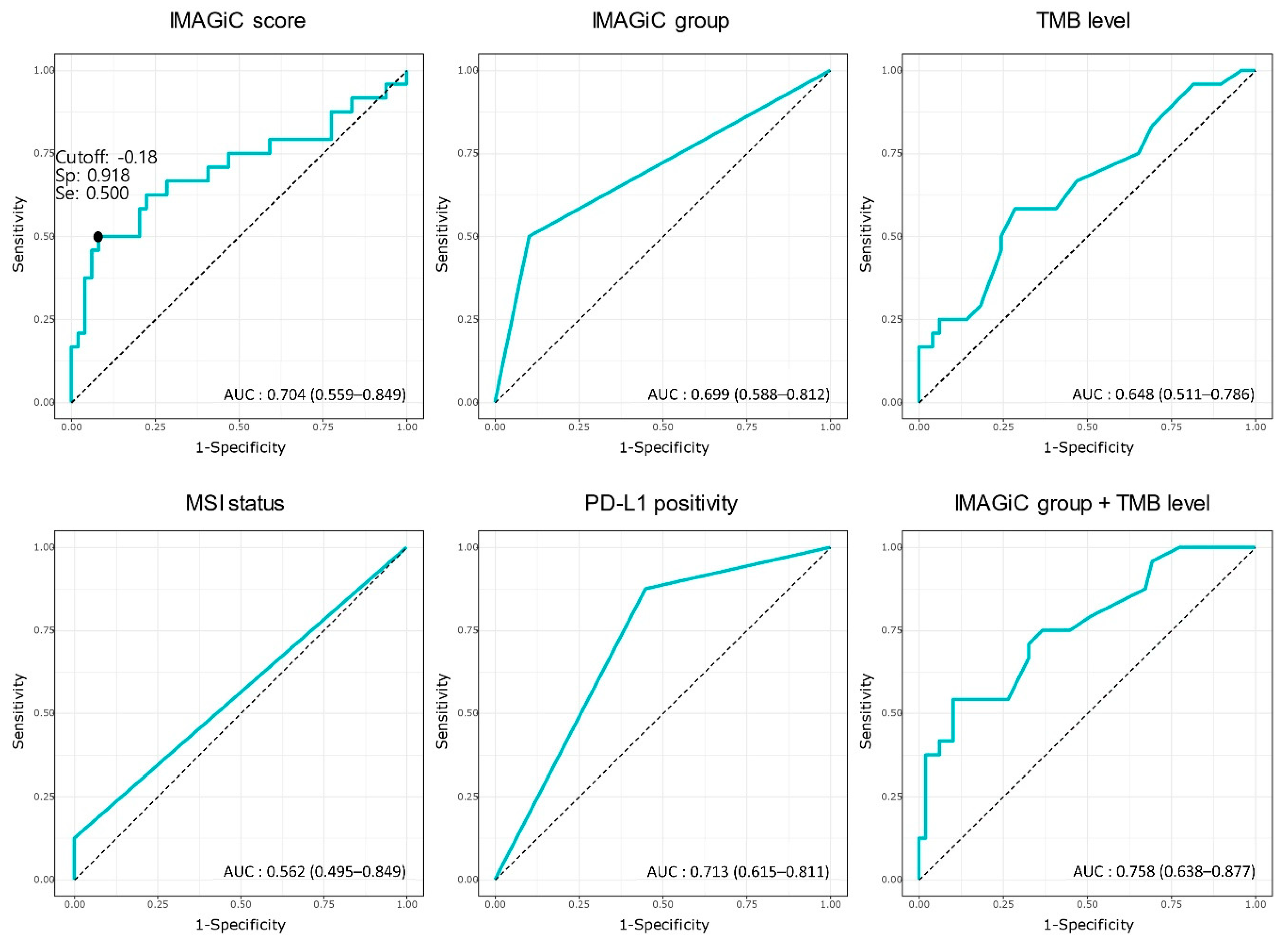
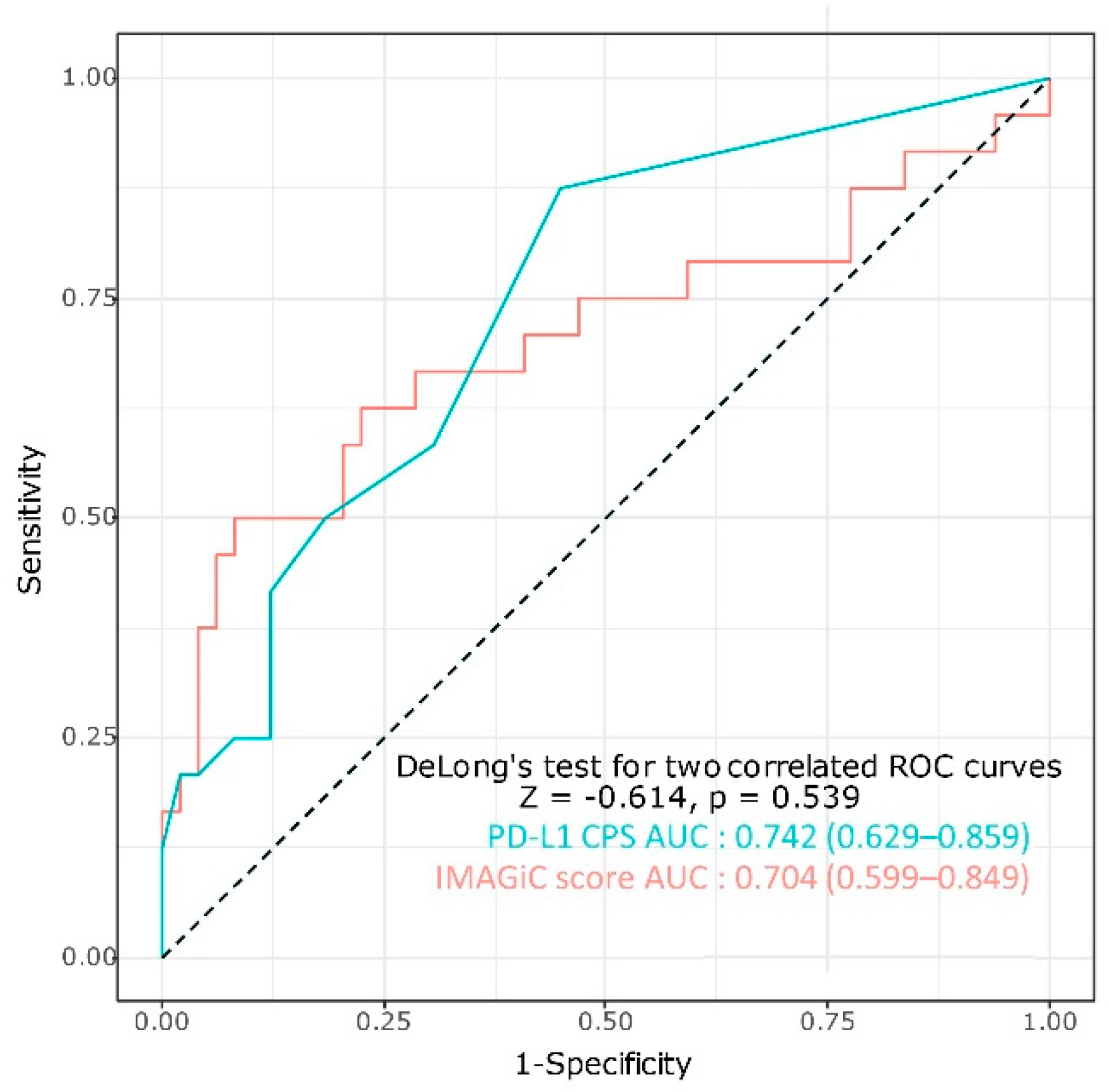
3.3. Association between IMAGiC Score/Group and Other Immunotherapy Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, P.; Allison, J.P. The future of immune checkpoint therapy. Science 2015, 348, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Sosman, J.A.; Atkins, M.B.; Leming, P.D.; et al. Five-Year Survival and Correlates Among Patients With Advanced Melanoma, Renal Cell Carcinoma, or Non-Small Cell Lung Cancer Treated With Nivolumab. JAMA Oncol. 2019, 5, 1411–1420. [Google Scholar] [CrossRef] [Green Version]
- Shao, C.; Li, G.; Huang, L.; Pruitt, S.; Castellanos, E.; Frampton, G.; Carson, K.R.; Snow, T.; Singal, G.; Fabrizio, D.; et al. Prevalence of High Tumor Mutational Burden and Association With Survival in Patients With Less Common Solid Tumors. JAMA Netw Open 2020, 3, e2025109. [Google Scholar] [CrossRef]
- Bonneville, R.; Krook, M.A.; Kautto, E.A.; Miya, J.; Wing, M.R.; Chen, H.Z.; Reeser, J.W.; Yu, L.; Roychowdhury, S. Landscape of Microsatellite Instability Across 39 Cancer Types. JCO Precis. Oncol. 2017, 2017, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-gamma-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef] [PubMed]
- Cristescu, R.; Mogg, R.; Ayers, M.; Albright, A.; Murphy, E.; Yearley, J.; Sher, X.; Liu, X.Q.; Lu, H.; Nebozhyn, M.; et al. Pan-tumor genomic biomarkers for PD-1 checkpoint blockade-based immunotherapy. Science 2018, 362, eaar3593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auslander, N.; Zhang, G.; Lee, J.S.; Frederick, D.T.; Miao, B.; Moll, T.; Tian, T.; Wei, Z.; Madan, S.; Sullivan, R.J.; et al. Robust prediction of response to immune checkpoint blockade therapy in metastatic melanoma. Nat. Med. 2018, 24, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- Heo, Y.J.; Kang, S.Y.; Kim, S.T.; Kang, W.K.; Lee, J.; Kim, K.-M. Combined biomarker for prediction of response to an immune checkpoint inhibitor in metastatic gastric cancer. Precis. Future Med. 2019, 3, 165–175. [Google Scholar] [CrossRef]
- Jung, H.; Kim, H.S.; Kim, J.Y.; Sun, J.M.; Ahn, J.S.; Ahn, M.J.; Park, K.; Esteller, M.; Lee, S.H.; Choi, J.K. DNA methylation loss promotes immune evasion of tumours with high mutation and copy number load. Nat. Commun. 2019, 10, 4278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, J.M.; Pabla, S.; Nesline, M.K.; Glenn, S.T.; Papanicolau-Sengos, A.; Burgher, B.; Andreas, J.; Giamo, V.; Wang, Y.; Lenzo, F.L.; et al. Next generation sequencing of PD-L1 for predicting response to immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, R.; Tan, X.; Xiao, Y.; Wang, X.; Wei, Z.; Wang, J.; Wang, X.; Zhou, H.; Zhang, L.; Shi, Y. Ubiquitin C-terminal hydrolase L1 promotes expression of programmed cell death-ligand 1 in non-small-cell lung cancer cells. Cancer Sci. 2020, 111, 3174–3183. [Google Scholar] [CrossRef] [PubMed]
- Vielnascher, R.M.; Hainzl, E.; Leitner, N.R.; Rammerstorfer, M.; Popp, D.; Witalisz, A.; Rom, R.; Karaghiosoff, M.; Kolbe, T.; Muller, S.; et al. Conditional ablation of TYK2 in immunity to viral infection and tumor surveillance. Transgenic Res. 2014, 23, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Jaggi, M.; Du, C.; Zhang, W.; Balaji, K.C. Protein kinase D1: A protein of emerging translational interest. Front. Biosci. 2007, 12, 3757–3767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Zhong, H.; Qin, Y.; Wei, W.; Li, Z.; Huang, M.; Luo, X. ARMCX Family Gene Expression Analysis and Potential Prognostic Biomarkers for Prediction of Clinical Outcome in Patients with Gastric Carcinoma. Biomed. Res. Int. 2020, 2020, 3575038. [Google Scholar] [CrossRef]
- Samstein, R.M.; Lee, C.H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat. Genet. 2019, 51, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrock, A.B.; Ouyang, C.; Sandhu, J.; Sokol, E.; Jin, D.; Ross, J.S.; Miller, V.A.; Lim, D.; Amanam, I.; Chao, J.; et al. Tumor mutational burden is predictive of response to immune checkpoint inhibitors in MSI-high metastatic colorectal cancer. Ann. Oncol. 2019, 30, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.A.; Bang, Y.J.; Piha-Paul, S.A.; Razak, A.R.A.; Bennouna, J.; Soria, J.C.; Rugo, H.S.; Cohen, R.B.; O’Neil, B.H.; Mehnert, J.M.; et al. T-Cell-Inflamed Gene-Expression Profile, Programmed Death Ligand 1 Expression, and Tumor Mutational Burden Predict Efficacy in Patients Treated With Pembrolizumab Across 20 Cancers: KEYNOTE-028. J. Clin. Oncol. 2019, 37, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Pender, A.; Titmuss, E.; Pleasance, E.D.; Fan, K.Y.; Pearson, H.; Brown, S.D.; Grisdale, C.J.; Topham, J.T.; Shen, Y.; Bonakdar, M.; et al. Genome and Transcriptome Biomarkers of Response to Immune Checkpoint Inhibitors in Advanced Solid Tumors. Clin. Cancer Res. 2021, 27, 202–212. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Response | CR/PR | SD/PD | Total | p-Value |
|---|---|---|---|---|
| (n = 24) | (n = 49) | (n = 73) | ||
| Age (median & quartile range) | 64.0 (54.0; 71.0) | 59.0 (52.0; 67.0) | 61.0 (52.0; 70.0) | 0.466 |
| Gender | 0.457 | |||
| Female | 10 (41.7%) | 26 (53.1%) | 36 (49.3%) | |
| Male | 14 (58.3%) | 23 (46.9%) | 37 (50.7%) | |
| Cancer type | 0.107 | |||
| Cervix cancer | 0 (0.0%) | 1 (2.0%) | 1 (1.4%) | |
| Cholangiocarcinoma | 3 (12.5%) | 7 (14.3%) | 10 (13.7%) | |
| Colorectal cancer | 4 (16.7%) | 0 (0.0%) | 4 (5.5%) | |
| Gastric cancer | 6 (25.0%) | 13 (26.5%) | 19 (26.0%) | |
| Hepatocellular carcinoma | 0 (0.0%) | 1 (2.0%) | 1 (1.4%) | |
| Melanoma | 9 (37.5%) | 16 (32.7%) | 25 (34.2%) | |
| Sarcoma | 0 (0.0%) | 5 (10.2%) | 5 (6.8%) | |
| Urothelial carcinoma | 2 (8.3%) | 6 (12.2%) | 8 (11.0%) | |
| Treatment line of immunotherapy | 0.948 | |||
| 1 | 8 (33.3%) | 15 (30.6%) | 23 (31.5%) | |
| 2 | 8 (33.3%) | 19 (38.8%) | 27 (37.0%) | |
| ≥3 | 8 (33.3%) | 15 (30.6%) | 23 (31.5%) | |
| Immunotherapy regimen | 0.668 | |||
| Atezolizumab containing | 3 (12.5%) | 5 (10.3%) | 8 (11.0%) | |
| Avelumab containing | 1 (4.2%) | 0 (0.0%) | 1 (1.43) | |
| Durvalumab containing | 6 (25.0%) | 13 (26.4%) | 19 (26.0%) | |
| Nivolumab containing | 4 (16.7%) | 11 (22.6%) | 15 (20.6%) | |
| Pembrolizumab containing | 10 (41.6%) | 20 (40.7%) | 30 (41.1%) | |
| Number of immunotherapy cycle (median & quartile range) | 14.0 (11.0; 19.0) | 7.0 (3.0; 9.0) | 9.0 (5.0; 13.0) | <0.001 |
| Total TMB (median & quartile range) | 7.0 (4.3; 10.2) | 4.7 (3.1; 7.0) | 5.5 (3.1; 7.8) | 0.040 |
| TMB | 0.191 | |||
| High (≥10 mutations per megabase) | 6 (25.0%) | 6 (12.2%) | 12 (16.4%) | |
| Low (<10 mutations per megabase) | 18 (75.0%) | 43 (87.8%) | 61 (83.6%) | |
| MSI status | 0.033 | |||
| MSI-H | 3 (12.5%) | 0 (0.0%) | 3 (4.1%) | |
| MSS | 21 (87.5%) | 49 (100.0%) | 70 (95.9%) | |
| PD-L1 CPS | 4.5 (1.0; 15.5) | 0.0 (0.0; 3.0) | 1.0 (0.0; 5.0) | 0.001 |
| IMAGiC Group | <0.001 | |||
| Non-responder | 12 (50.0%) | 44 (89.8%) | 56 (76.7%) | |
| Responder | 12 (50.0%) | 5 (10.2%) | 17 (23.3%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-C.; Heo, Y.-J.; Kang, S.-Y.; Lee, J.; Kim, K.-M. Validation of the Combined Biomarker for Prediction of Response to Checkpoint Inhibitor in Patients with Advanced Cancer. Cancers 2021, 13, 2316. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102316
Kim J-C, Heo Y-J, Kang S-Y, Lee J, Kim K-M. Validation of the Combined Biomarker for Prediction of Response to Checkpoint Inhibitor in Patients with Advanced Cancer. Cancers. 2021; 13(10):2316. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102316
Chicago/Turabian StyleKim, Jin-Chul, You-Jeong Heo, So-Young Kang, Jeeyun Lee, and Kyoung-Mee Kim. 2021. "Validation of the Combined Biomarker for Prediction of Response to Checkpoint Inhibitor in Patients with Advanced Cancer" Cancers 13, no. 10: 2316. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13102316