
Clinical Implication of Liquid Biopsy in Colorectal Cancer Patients Treated with Metastasectomy

 ,
,  ,
,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
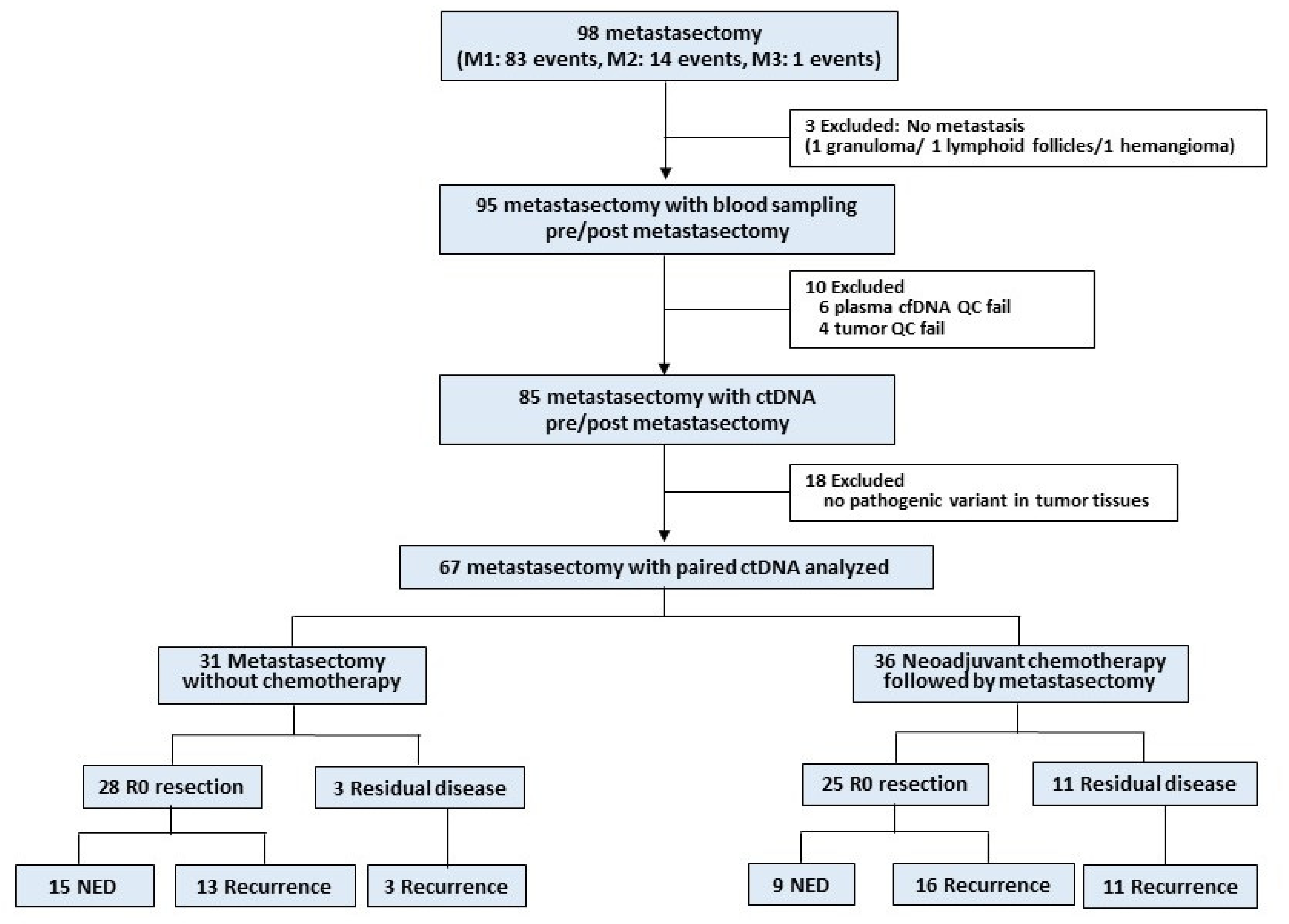
2.1. Study Design and Participants
2.2. Tumor Tissue and Blood Collection and Mutation Analysis by Next-Generation Sequencing
2.3. Tumor-Guided ctDNA Identification
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
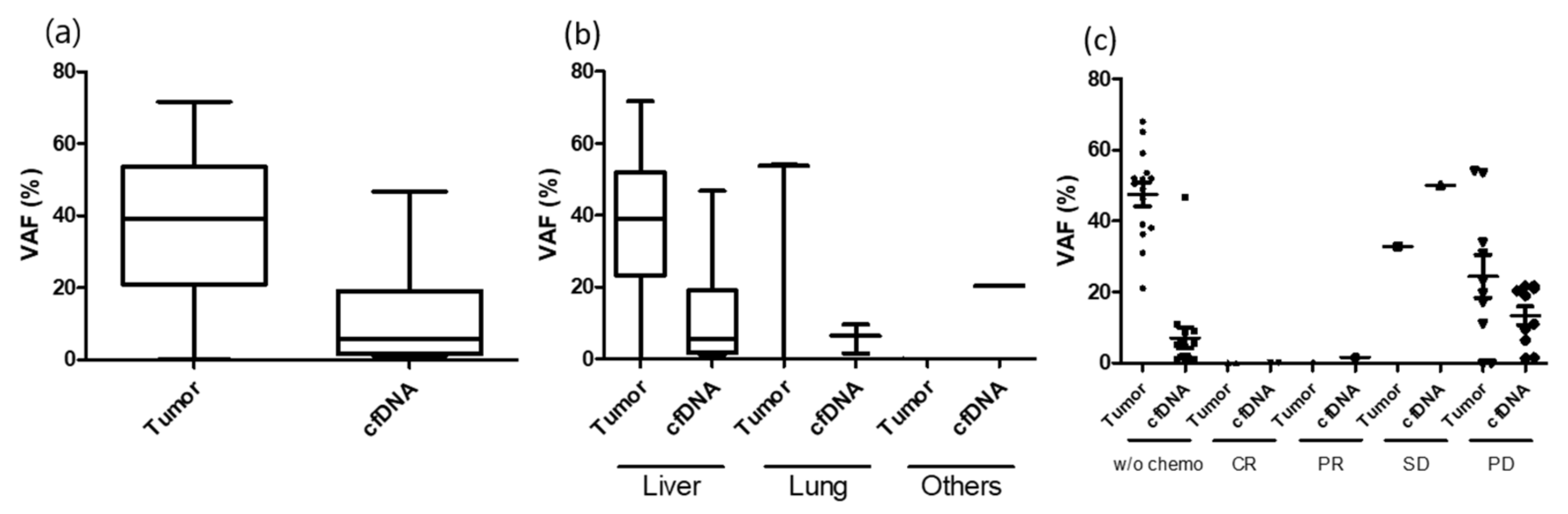
3.2. ctDNA Detection before and after Metastasectomy
3.3. Group 1: Upfront Metastasectomy without Neoadjuvant Chemotherapy (R0 Resection = 28 Cases)
3.4. Group 2: Upfront Metastasectomy without Neoadjuvant Chemotherapy (R0 Resection Failed = 3 Cases)
3.5. Group 3: Neoadjuvant Chemotherapy Followed by Metastasectomy (R0 Resection = 25 Cases)
3.6. Group 4: Neoadjuvant Chemotherapy Followed by Metastasectomy (R0 Resection Failed = 11)
3.7. Longitudinal Tracking with Serial ctDNA Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hong, S.; Won, Y.J.; Park, Y.R.; Jung, K.W.; Kong, H.J.; Lee, E.S. The Community of Population-Based Regional Cancer Registries. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2017. Cancer Res. Treat. 2020, 52, 335–350. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Nordlinger, B.; Adam, R.; Köhne, C.-H.; Pozzo, C.; Poston, G.; Ychou, M.; Rougier, P. Towards a pan-European consensus on the treatment of patients with colorectal liver metastases. Eur. J. Cancer 2006, 42, 2212–2221. [Google Scholar] [CrossRef] [PubMed]
- Biasco, G.; Derenzini, E.; Grazi, G.; Ercolani, G.; Ravaioli, M.; Pantaleo, M.; Brandi, G. Treatment of hepatic metastases from colorectal cancer: Many doubts, some certainties. Cancer Treat. Rev. 2006, 32, 214–228. [Google Scholar] [CrossRef]
- Garden, O.J.; Rees, M.; Poston, G.J.; Mirza, D.; Saunders, M.; Ledermann, J.; Primrose, J.N.; Parks, R.W. Guidelines for resection of colorectal cancer liver metastases. Gut 2006, 55 (Suppl. 3), iii1–iii8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.-S.; Yun, S.H.; Chun, H.-K.; Lee, W.-Y.; Yun, H.-R.; Kim, J.; Kim, K.; Shim, Y.M. Pulmonary resection for metastases from colorectal cancer: Prognostic factors and survival. Int. J. Colorectal Dis. 2007, 22, 699–704. [Google Scholar] [CrossRef]
- Kemeny, N.E.; Chou, J.F.; Boucher, T.M.; Capanu, M.; DeMatteo, R.P.; Jarnagin, W.R.; Allen, P.J.; Fong, Y.C.; Cercek, A.; D’Angelica, M.I. Updated long-term survival for patients with metastatic colorectal cancer treated with liver resection followed by hepatic arterial infusion and systemic chemotherapy. J. Surg. Oncol. 2016, 113, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Penna, C.; Nordlinger, B. Colorectal metastasis (liver and lung). Surg. Clin. N. Am. 2002, 82, 1075–1090. [Google Scholar] [CrossRef]
- Merker, J.D.; Oxnard, G.R.; Compton, C.; Diehn, M.; Hurley, P.; Lazar, A.J.; Lindeman, N.; Lockwood, C.M.; Rai, A.J.; Schilsky, R.L. Circulating tumor DNA analysis in patients with cancer: American Society of Clinical Oncology and College of American Pathologists joint review. J. Clin. Oncol. 2018, 36, 1631–1641. [Google Scholar] [CrossRef] [PubMed]
- Bach, S.; Sluiter, N.R.; Beagan, J.J.; Mekke, J.M.; Ket, J.C.; van Grieken, N.C.; Steenbergen, R.D.; Ylstra, B.; Kazemier, G.; Tuynman, J.B. Circulating tumor DNA analysis: Clinical implications for colorectal cancer patients. A systematic review. JNCI Cancer Spectr. 2019, 3, pkz042. [Google Scholar] [CrossRef]
- Tie, J.; Kinde, I.; Wang, Y.; Wong, H.-L.; Roebert, J.; Christie, M.; Tacey, M.; Wong, R.; Singh, M.; Karapetis, C. Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer. Ann. Oncol. 2015, 26, 1715–1722. [Google Scholar] [CrossRef]
- Wang, Y.; Li, L.; Cohen, J.D.; Kinde, I.; Ptak, J.; Popoli, M.; Schaefer, J.; Silliman, N.; Dobbyn, L.; Tie, J.; et al. Prognostic Potential of Circulating Tumor DNA Measurement in Postoperative Surveillance of Nonmetastatic Colorectal Cancer. JAMA Oncol. 2019, 5, 1118–1123. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Cohen, J.D.; Wang, Y.; Li, L.; Christie, M.; Simons, K.; Elsaleh, H.; Kosmider, S.; Wong, R.; Yip, D. Serial circulating tumour DNA analysis during multimodality treatment of locally advanced rectal cancer: A prospective biomarker study. Gut 2019, 68, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Cohen, J.D.; Wang, Y.; Christie, M.; Simons, K.; Lee, M.; Wong, R.; Kosmider, S.; Ananda, S.; McKendrick, J.; et al. Circulating Tumor DNA Analyses as Markers of Recurrence Risk and Benefit of Adjuvant Therapy for Stage III Colon Cancer. JAMA Oncol. 2019, 5, 1710–1717. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Wang, Y.; Tomasetti, C.; Li, L.; Springer, S.; Kinde, I.; Silliman, N.; Tacey, M.; Wong, H.-L.; Christie, M. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci. Transl. Med. 2016, 8, 346ra392. [Google Scholar] [CrossRef] [Green Version]
- Carrato, A. Adjuvant treatment of colorectal cancer. Gastrointest. Cancer Res. 2008, 2, S42–S46. [Google Scholar]
- Grávalos, C.; García-Escobar, I.; García-Alfonso, P.; Cassinello, J.; Malón, D.; Carrato, A. Adjuvant chemotherapy for stages II, III and IV of colon cancer. Clin. Transl. Oncol. 2009, 11, 526–533. [Google Scholar] [CrossRef]
- Schøler, L.V.; Reinert, T.; Ørntoft, M.-B.W.; Kassentoft, C.G.; Árnadóttir, S.S.; Vang, S.; Nordentoft, I.; Knudsen, M.; Lamy, P.; Andreasen, D. Clinical implications of monitoring circulating tumor DNA in patients with colorectal cancer. Clin. Cancer Res. 2017, 23, 5437–5445. [Google Scholar] [CrossRef] [Green Version]
- Tie, J.; Cohen, J.D.; Lo, S.N.; Wang, Y.; Li, L.; Christie, M.; Lee, M.; Wong, R.; Kosmider, S.; Skinner, I.; et al. Prognostic significance of postsurgery circulating tumor DNA in nonmetastatic colorectal cancer: Individual patient pooled analysis of three cohort studies. Int. J. Cancer 2020. [Google Scholar] [CrossRef]
- Sung, J.S.; Chong, H.Y.; Kwon, N.J.; Kim, H.M.; Lee, J.W.; Kim, B.; Lee, S.B.; Park, C.W.; Choi, J.Y.; Chang, W.J.; et al. Detection of somatic variants and EGFR mutations in cell-free DNA from non-small cell lung cancer patients by ultra-deep sequencing using the ion ampliseq cancer hotspot panel and droplet digital polymerase chain reaction. Oncotarget 2017, 8, 106901–106912. [Google Scholar] [CrossRef] [Green Version]
- Genovese, G.; Kahler, A.K.; Handsaker, R.E.; Lindberg, J.; Rose, S.A.; Bakhoum, S.F.; Chambert, K.; Mick, E.; Neale, B.M.; Fromer, M.; et al. Clonal hematopoiesis and blood-cancer risk inferred from blood DNA sequence. N. Engl. J. Med. 2014, 371, 2477–2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, S.J.; Tsui, D.W.; Murtaza, M.; Biggs, H.; Rueda, O.M.; Chin, S.F.; Dunning, M.J.; Gale, D.; Forshew, T.; Mahler-Araujo, B.; et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N. Engl. J. Med. 2013, 368, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Pecuchet, N.; Zonta, E.; Didelot, A.; Combe, P.; Thibault, C.; Gibault, L.; Lours, C.; Rozenholc, Y.; Taly, V.; Laurent-Puig, P.; et al. Base-Position Error Rate Analysis of Next-Generation Sequencing Applied to Circulating Tumor DNA in Non-Small Cell Lung Cancer: A Prospective Study. PLoS Med. 2016, 13, e1002199. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Walker, A.; Gagnon, R.; Mazumdar, J.; Casey, M.; Long, G.V.; Schadendorf, D.; Flaherty, K.; Kefford, R.; Hauschild, A.; Hwu, P.; et al. Correlation of BRAF Mutation Status in Circulating-Free DNA and Tumor and Association with Clinical Outcome across Four BRAFi and MEKi Clinical Trials. Clin. Cancer Res. 2016, 22, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Reinert, T.; Henriksen, T.V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H.T.; Tin, A.S.; et al. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients With Stages I to III Colorectal Cancer. JAMA Oncol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.; Benesova, L.; Lipska, L.; Belsanova, B.; Minarikova, P.; Veprekova, G.; Zavoral, M.; Minarik, M. Utility of cell-free tumour DNA for post-surgical follow-up of colorectal cancer patients. Anticancer Res. 2012, 32, 1621–1626. [Google Scholar]
- Flamini, E.; Mercatali, L.; Nanni, O.; Calistri, D.; Nunziatini, R.; Zoli, W.; Rosetti, P.; Gardini, N.; Lattuneddu, A.; Verdecchia, G.M.; et al. Free DNA and carcinoembryonic antigen serum levels: An important combination for diagnosis of colorectal cancer. Clin. Cancer Res. 2006, 12, 6985–6988. [Google Scholar] [CrossRef] [Green Version]
- Abbosh, C.; Birkbak, N.J.; Wilson, G.A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D.A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature 2017, 545, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Avanzini, S.; Kurtz, D.M.; Chabon, J.J.; Moding, E.J.; Hori, S.S.; Gambhir, S.S.; Alizadeh, A.A.; Diehn, M.; Reiter, J.G. A mathematical model of ctDNA shedding predicts tumor detection size. Sci. Adv. 2020, 6. [Google Scholar] [CrossRef]
- Oikkonen, J.; Zhang, K.; Salminen, L.; Schulman, I.; Lavikka, K.; Andersson, N.; Ojanpera, E.; Hietanen, S.; Grenman, S.; Lehtonen, R.; et al. Prospective Longitudinal ctDNA Workflow Reveals Clinically Actionable Alterations in Ovarian Cancer. JCO Precis. Oncol. 2019, 3, 1–12. [Google Scholar] [CrossRef]
- Garlan, F.; Laurent-Puig, P.; Sefrioui, D.; Siauve, N.; Didelot, A.; Sarafan-Vasseur, N.; Michel, P.; Perkins, G.; Mulot, C.; Blons, H.; et al. Early Evaluation of Circulating Tumor DNA as Marker of Therapeutic Efficacy in Metastatic Colorectal Cancer Patients (PLACOL Study). Clin. Cancer Res. 2017, 23, 5416–5425. [Google Scholar] [CrossRef] [Green Version]
- Katoh, M.; Unakami, M.; Hara, M.; Fukuchi, S. Bone metastasis from colorectal cancer in autopsy cases. J. Gastroenterol. 1995, 30, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra224. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Clinical Variables | Npatient = 58 (%) | |
|---|---|---|
| Age years (median, range) | 56 (35–78) | |
| Gender | Male | 37 (63.8) |
| Female | 21 (36.2) | |
| Primary tumor site | Ascending colon | 8 (13.8) |
| Descending colon | 20 (34.5) | |
| Rectum | 30 (51.7) | |
| Primary tumor surgery | Yes | 57 (98.3%) |
| No | 1 (1.7%) | |
| Synchronicity of metastasis | Metachronous | 18 (31.1) |
| Synchronous | 40 (68.9) | |
| Metastasectomy organ | Liver | 38 (65.5) |
| Lung | 25 (43.1) | |
| Peritoneum | 4 (6.9) | |
| Lymph node | 2 (3.4) | |
| No | Synchronicity | Variant | Primary Tissue VAF | Metastatic Tissue VAF | Metastatic Site | PreM ctDNA VAF | PostM ctDNA VAF | Recurence | |
|---|---|---|---|---|---|---|---|---|---|
| No CTx | CTx | ||||||||
| ctDNA positive before metastasectomy | |||||||||
| 020b | M | TP53 R196 * | 38.5 | 65.1 | Liver 2.5 cm | 1.2 | 0.0 | N | |
| APC Q1294 * | 25.4 | 51.6 | 0.0 | 0.0 | |||||
| 037b | M | TP53 T211I | 14.9 | 59.1 | Liver 2.5 cm | 46.8 | 0.0 | N | |
| 073 | M | APC T1445Qfs | 21.0 | 26.0 | Liver 7.4 cm | 0.0 | 0.0 | N | |
| APC R876 * | 31.2 | 0.0 | 0.0 | 0.0 | |||||
| TP53 R248W | 23.0 | 21.0 | 1.1 | 0.0 | |||||
| 025a | M | FXW7 R465C | 33.0 | 33.4 | Liver 2.1 cm | 0.0 | 0.0 | N | |
| KRAS G12D | 23.8 | 28.4 | 0.0 | 0.0 | |||||
| TP53 R196 * | 35.9 | 51.8 | 2.1 | 0.0 | |||||
| APC L1488fs | 26.1 | 0 | 0.0 | 0.0 | |||||
| 025b | M | FXW7 R465C | 33.0 | 31.0 | Liver 1.5 cm | 1.1 | 0.0 | Liver LN | |
| KRAS G12D | 23.8 | 36.3 | 2.0 | 0.0 | |||||
| TP53 R196 * | 35.9 | 49.0 | 1.8 | 0.0 | |||||
| APC L1488fs | 26.1 | 0 | 0.0 | 0.0 | |||||
| 050 | M | APC Q1367 * | 32.6 | 34.0 | Liver 3.0 cm | 0.0 | 0.0 | Liver | |
| TP53 R237H | 26.2 | 39.0 | 1.0 | 0.0 | |||||
| BRAF G469E | 0.0 | 1.3 | 0.0 | 0.0 | |||||
| CTNNB1 G34E | 0.0 | 1.4 | 0.0 | 0.0 | |||||
| VHL R161 * | 0.0 | 1.4 | 0.0 | 0.0 | |||||
| 062 | M | APC R1450 * | 35.3 | 52.0 | Liver 3.2 cm | 5.9 | 0.0 | Lung | |
| KRAS G12S | 55.0 | 68.0 | 8.6 | 0.0 | |||||
| TP53 R342 * | 50.9 | 52.0 | 9.0 | 0.0 | |||||
| 092 | M | SMAD4 G419R | QC failed * | 53.6 | Liver 4.7 cm | 11.0 | 0.0 | Lung Liver | |
| ctDNA negative before metastasectomy | |||||||||
| 002 | M | NRAS G12D | 0.0 | 19.0 | Lung 0.9 cm | 0.0 | 0.0 | N | |
| 005 | M | TP53 R282W | 43.0 | 22.0 | Lung 0.8 cm | 0.0 | 0.0 | N | |
| APC R876 * | 34.0 | 14.0 | 0.0 | 0.0 | |||||
| 028b | M | KRAS G12V | 14.3 | 0.0 | PT 4.0 cm | 0.0 | 0.0 | N | |
| PIK3CA E545K | 14.8 | 0.0 | 0.0 | 0.0 | |||||
| SMAD4 R361H | 16.4 | 0.0 | 0.0 | 0.0 | |||||
| SMAD4 E330Q | 16.6 | 50.2 | 0.0 | 0.0 | |||||
| PIK3CA G914R | 14.9 | 0 | 0.0 | 0.0 | |||||
| 034 | M | TP53 R175H | 0.0 | 17.2 | LN 0.9 cm | 0.0 | 0.0 | N | |
| KRAS G12C | 0.0 | 18.0 | 0.0 | 0.0 | |||||
| PIK3CA E545V | 0.0 | 3.3 | 0.0 | 0.0 | |||||
| 041 | M | KRAS A59T | 59.0 | 44.0 | Lung 1.0 cm | 0.0 | 0.0 | N | |
| TP53 R342 * | 44.0 | 22.0 | 0.0 | 0.0 | |||||
| 056 | M | KRAS G12D | 24.0 | 0.0 | Liver 0.7 cm | 0.0 | 0.0 | N | |
| TP53 C238Y | 35.7 | 0.0 | 0.0 | 0.0 | |||||
| 060 | M | TP53 N239 * | 21.0 | 32.0 | Liver 2.0 cm | 0.0 | 0.0 | N | |
| 066 | M | TP53 R282W | 23.4 | 3.9 | Lung 0.4 cm | 0.0 | 0.0 | N | |
| APC R876 * | 31.2 | 0.0 | 0.0 | 0.0 | |||||
| APC E1379 * | 26.4 | 0.0 | 0.0 | 0.0 | |||||
| 068 | M | TP53 R213 * | 0.0 | 25.1 | Lung 1.7 cm | 0.0 | 0.0 | N | |
| 081 | S | KRAS G12S | 30.0 | 29.0 | Lung 1.2 cm | 0.0 | 0.0 | N | |
| APC Q1378 * | 23.0 | 25.0 | 0.0 | 0.0 | |||||
| 093 | M | PIK3CA V344M | BDL * | 17.4 | Lung 1.4 cm | 0.0 | 0.0 | N | |
| 098 | M | KRAS G13D | 0.0 | 21.1 | Liver 2.2 cm | 0.0 | 0.0 | N | |
| APC L1488fs | 22.9 | 0.0 | 0.0 | 0.0 | |||||
| APC E1494fs | 0.0 | 20.4 | 0.0 | 0.0 | |||||
| 007 | M | APC C1289 * | 6.9 | 20.8 | Lung 1.4 cm | 0.0 | 0.0 | PT | |
| PIK3CA E542K | 3.8 | 20.5 | 0.0 | 0.0 | |||||
| TP53 R282W | 2.6 | 14.0 | 0.0 | 0.0 | |||||
| TP53 S99fs * | 2.1 | 11.0 | 0.0 | 0.0 | |||||
| 031a | S | APC R1114 * | 8.1 | 29.4 | Lung 1.4 cm | 0.0 | 0.0 | Lung | |
| KRAS G13C | 13.4 | 42.6 | 0.0 | 0.0 | |||||
| APC R1463fs | 2.0 | 0.0 | 0.0 | 0.0 | |||||
| APC E1345 * | 8.1 | 30.7 | 0.0 | 0.0 | |||||
| 032 | M | KRAS G12D | 22.3 | 29.2 | Lung 1.2 cm | 0.0 | 0.0 | LN | |
| TP53 R282W | 0.0 | 34.6 | 0.0 | 0.0 | |||||
| TP53 S127F | 14.3 | 0.0 | 0.0 | 0.0 | |||||
| APC L1488fs | 13.2 | 0.0 | 0.0 | 0.0 | |||||
| 035 | M | KRAS G12C | 37.7 | 15.6 | Lung 0.5 cm | 0.0 | 0.0 | Lung | |
| TP53 I195T | 41.4 | 17.1 | 0.0 | 0.0 | |||||
| APC R1463fs | 1.9 | 0.0 | 0.0 | 0.0 | |||||
| APC S1501fs | 24.0 | 8.9 | 0.0 | 0.0 | |||||
| 040 | M | KRAS G12D | 3.4 | 18.5 | Lung 0.6 cm | 0.0 | 0.0 | Lung Bone | |
| TP53 S241P | 1.2 | 10.4 | 0.0 | 0.0 | |||||
| PTEN R173H | 1.0 | 0.0 | 0.0 | 0.0 | |||||
| 058 | M | NRAS G12D | 24.6 | 32.7 | Lung 1.0 cm | 0.0 | 0.0 | Lung | |
| TP53 H297fs | 26.2 | 14.6 | 0.0 | 0.0 | |||||
| TP53 R333fs | 22.5 | 10.0 | 0.0 | 0.0 | |||||
| 072 | M | APC R876 * | 17.8 | 10.6 | PT 2.7 cm | 0.0 | 0.0 | PT LN | |
| TP53 R248Q | 16.8 | 10.8 | 0.0 | 0.0 | |||||
| APC Q1303 * | 14.1 | 12.0 | 0.0 | 0.0 | |||||
| 078 | M | KRAS G12V | 41.0 | 12.9 | Lung 1.2 cm | 0.0 | 0.0 | Lung | |
| TP53 R175H | 54.1 | 20.8 | 0.0 | 0.0 | |||||
| No | Synchronicity | Variant | Primary Tissue VAF | Metastatic Tissue VAF | Metastatic Site | PreM ctDNA VAF | PostM ctDNA VAF | Residual | |
|---|---|---|---|---|---|---|---|---|---|
| No CTx | CTx | ||||||||
| ctDNA positive before metastasectomy | |||||||||
| 046 | M | KRAS G12D | 0 | 38.1 | Liver 2.1 cm | 4.4 | 0.0 | Lung <0.5 #4 Pelvic LNs | |
| TP53 G245C | 1.0 | 46.3 | 5.6 | 0.0 | |||||
| APC K1561 * | 0 | 50.5 | 5.0 | 0.0 | |||||
| ctDNA negative before metastasectomy | |||||||||
| 022 | M | TP53 V272M | 39.4 | 55.4 | Liver 3.0 cm | 0.0 | 0.0 | LN 2.2 cm | |
| SMAD4 | 7.4 | 0.0 | |||||||
| 061c | M | TP53 | 51.5 | 25.1 | Lung 2.1 cm | 0.0 | 0.0 | PT | |
| APC H1490fs | 30.2 | 16.2 | 0.0 | 0.0 | |||||
| No | Synchronicity | Variant | Primary Tissue VAF | Metastatic Tissue VAF | Meta Site | PreM ctDNA | PostM ctDNA | Recurence | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No CTx | CTx | Rx | CTx | Rx | |||||||
| ctNDA positive before metastasectomy | |||||||||||
| 001 | S | TP53 I255F | 49.8 | SD | 0.0 | PR | Liver 0.1 cm | 1.6 | 0.0 | N | |
| 036 | S | APC R1114 * | 44.2 | 31.0 | PD | Liver 2.5 cm | 21.0 | 0.0 | N | ||
| APC R1450 * | 21.5 | 17.0 | 11.0 | 0.0 | |||||||
| KRAS G12D | 46.5 | 34.0 | 19.0 | 0.0 | |||||||
| 008b | S | KRAS Q61R | 48.8 | 53.7 | PD | Lung 2.5 cm | 9.6 | 0.0 | Lung | ||
| TP53 R175H | 49.5 | 54.1 | 6.4 | 0.0 | |||||||
| 028a | S | KRAS G12V | 14.3 | 7.8 | PD | Liver 2.2 cm | 0.0 | 0.0 | PT | ||
| PIK3CA E545K | 14.8 | 11. 1 | 1.3 | 0.0 | |||||||
| PIK3CA G914R | 14.9 | 10.2 | 0.0 | 0.0 | |||||||
| SMAD4 E330Q | 16.6 | 8.9 | 0.0 | 0.0 | |||||||
| SMAD4 R361H/C | 16.4 | 1.7 | 0.0 | 0.0 | |||||||
| ctNDA negative before metastasectomy | |||||||||||
| 004 | S | TP53 R273C | 60.4 | 4.1 | PR | Liver 0.8 cm | 0.0 | 0.0 | N | ||
| APC K1308 * | 40.2 | 2.8 | 0.0 | 0.0 | |||||||
| 012 | S | KRAS G12V | 14.6 | 0.0 | CR | Liver 0 cm | 0.0 | 0.0 | N | ||
| PIK3CA H1047R | 20.6 | 0.0 | 0.0 | 0.0 | |||||||
| 031b | S | APC R1114 * | 8.1 | 11.6 | SD | Lung 1.4 cm | 0.0 | 0.0 | N | ||
| APC E1345 * | 8.1 | 15.4 | 0.0 | 0.0 | |||||||
| KRAS G13C | 13.4 | 9.1 | 0.0 | 0.0 | |||||||
| 042 | M | APC Q1378 * | 47.5 | 36.2 | PR | Liver 2.5 cm | 0.0 | 0.0 | N | ||
| KRAS G12D | 29.9 | 18.3 | 0.0 | 0.0 | |||||||
| TP53 R175H | 30.5 | 19.3 | 0.0 | 0.0 | |||||||
| 044 | S | CTNNB1 S45F | 36.8 | 6.5 | PR | Liver 2.2 cm | 0.0 | 0.0 | N | ||
| KRAS G12D | 17.3 | 0.0 | 0.0 | 0.0 | |||||||
| PTEN R335 * | 5.2 | 0.0 | 0.0 | 0.0 | |||||||
| 057 | S | TP53 C275Y | 26.5 | 36.9 | SD | Lung 1.6 cm | 0.0 | 0.0 | N | ||
| 091 | S | APC E1306 * | 18.0 | 0.0 | PR | Liver 0.8 cm | 0.0 | 0.0 | N | ||
| TP53 R175H | 40.2 | 6.2 | 0.0 | 0.0 | |||||||
| APC Q886 * | 26.9 | 4.6 | 0.0 | 0.0 | |||||||
| 006 | S | KRAS G13C | 37.2 | 10.7 | PR | Liver 1.6 cm | 0.0 | 0.0 | Bone | ||
| TP53 R306 * | 34.9 | 9.1 | 0.0 | 0.0 | |||||||
| 011 | M | APC R876 * | 30.6 | 0.0 | PD | Lung 1.0 cm | 0.0 | 0.0 | Lung | ||
| KRAS E545K | 34.3 | 2.2 | 0.0 | 0.0 | |||||||
| TP53 R342 * | 0.0 | 2.5 | 0.0 | 0.0 | |||||||
| SMAD4 R361H | 0.0 | 3.8 | 0.0 | 0.0 | |||||||
| SMAD4 A118V | 64.8 | 0.0 | 0.0 | 0.0 | |||||||
| 014 | S | KRAS Q61H | 25.3 | 5.6 | SD | Liver 2.3 cm | 0.0 | 0.0 | PT | ||
| SMAD4 R361C | 15.2 | 3.0 | 0.0 | 0.0 | |||||||
| 019 | S | PIK3CA G1049R | 3.1 | SD | 3.6 | SD | Liver 0.9 cm | 0.0 | 0.0 | Liver | |
| 020a | S | TP53 R196 * | 38.5 | SD | 21.2 | PR | Liver 2.5 cm | 0.0 | 0.0 | Liver | |
| APC Q1294 * | 25.4 | 13.8 | 0.0 | 0.0 | |||||||
| 027 | S | TP53 R175H | 6.1 | PR | 2.6 | PR | Liver 3.2 cm | 0.0 | 0.0 | Liver Lung | |
| PTEN R335 * | 1.1 | 0.0 | 0.0 | 0.0 | |||||||
| 037a | S | TP53 T211I | 14.9 | 1.0 | PR | Liver 0.5 cm | 0.0 | 0.0 | Liver | ||
| 048 | S | APC R1450 * | 1.5 | 0.0 | PR | Lung 0.6 cm | 0.0 | 0.0 | Lung | ||
| CTNNB1 S37Y | 0.0 | 21.2 | 0.0 | 0.0 | |||||||
| KRAS G12D | 1.4 | 0.0 | 0.0 | 0.0 | |||||||
| PIK3CA E545K | 2.0 | 0.0 | 0.0 | 0.0 | |||||||
| TP53 R209Kfs | 1.8 | 0 | 0.0 | 0.0 | |||||||
| 051b | M | KRAS G13S | 0.0 | 1.1 | PD | Lung 0.9 cm | 0.0 | 0.0 | Lung | ||
| PTEN R130Q | 0.0 | 1.0 | 0.0 | 0.0 | |||||||
| SMAD4 C115Y | 0.0 | 1.2 | 0.0 | 0.0 | |||||||
| TP53 R175H | 10.7 | 40.0 | 0.0 | 0.0 | |||||||
| 052 | S | RB1 A201fs | 0.0 | 5.5 | PR | Lung 0.4 cm | 0.0 | 0.0 | Lung | ||
| 055 | S | KRAS G13D | 60.3 | 16.6 | PR | Liver 3.5 cm | 0.0 | 0.0 | Liver | ||
| 061b | S | TP53? | 51.5 | SD | 27.1 | SD | Lung 0.5 cm | 0.0 | 0.0 | Lung | |
| APC H1490fs | 30.2 | 19.5 | 0.0 | 0.0 | |||||||
| 063 | S | KRAS G12V | BDL | 5.3 | PR | Liver 2.2 cm | 0.0 | 0.0 | Lung | ||
| KRAS A146T | BDL | 25.0 | 0.0 | 0.0 | |||||||
| TP53 V173L | BDL | 2.4 | 0.0 | 0.0 | |||||||
| APC P1381fs | BDL | 15.5 | 0.0 | 0.0 | |||||||
| 067 | S | TP53 M246R | 23.2 | SD | 39.3 | SD | Rec 3.4 cm | 0.0 | 0.0 | PT | |
| No | Synchronicity | Variant | Primary Tissue VAF | Metastatic Tissue VAF | Meta Site | PreM ctDNA VAF | PostM ctDNA VAF | Residual | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No CTx | CTx | Rx | CTx | Rx | |||||||
| ctDNA positive before metastasectomy | |||||||||||
| 053 | S | EBRR2 D769Y | 0 | 71.7 | PD | Liver #2 (2.3) | 32.9 | 50 | Liver multiple Bone | ||
| 076 | S | TP53 I195fs | 19.2 | 0 | PD | PT 4.1 cm | 20.4 | 16.9 | Huge liver | ||
| 079 | M | APC Q1378 * | BDL | 23.2 | PD | Liver #7 | 21.6 | 0 | Lung 0.9 cm | ||
| TP53 S215G | BDL | 19.8 | 21.7 | 0 | |||||||
| 096 | S | KRAS G13D | 31.4 | 8.6 | PR | Liver #9 | 0 | 0 | Liver #2 (<0.5) | ||
| TP53 V73fs | 50.8 | 0 | 0 | 0 | |||||||
| ctDNA negative before metastasectomy | |||||||||||
| 003 | S | TP53 R196 * | 30.2 | 22.8 | PD | Liver 2.3 cm | 0 | 0 | Liver 1.6 cm | ||
| 008a | S | KRAS Q61R | 48.8 | 10.4 | SD | Lung 0.6 cm | 0 0 | 0 0 | Lung 0.8 cm | ||
| TP53 R175H | 49.5 | 10.1 | |||||||||
| 026 | S | TP53 R306 * | 39.7 | 25.2 | PD | Liver #5 PT #5 | 0 | 0 | Liver 0.5 cm | ||
| 051a | S | TP53 R175H | 10.7 | 11.5 | PD | Liver #4 | 0 | 0 | Lung 0.5 cm | ||
| BRAF V471F | 0 | 12.3 | 0 | 0 | |||||||
| 054 | M | KRAS G12D | 45.5 | 49.9 | PD | Liver 1.6 cm PT 2.6 cm | 0 | 10.1 | Liver #6 (<1.0 cm) | ||
| 061a | S | TP53? | 51.5 | SD | 14.5 | PD | Lung 1.0 cm | 0 | 0 | Lung <0.5 cm #2 | |
| APC H1490fs | 30.2 | 12.4 | 0 | 0 | |||||||
| 065 | S | APC R1114 * | 37.5 | 37.5 | PR | Liver #4 | 0 | 3.6 | Liver 1.4 cm | ||
| TP53 G244S | 52.7 | 46.2 | 0 | 2.2 | |||||||
| APC S1356 * | 29.3 | 15.8 | 0 | 2.9 | |||||||
| Clinical Condition | ctDNA Positive (N = 16) | ctDNA Negative (N = 51) | p Value | |
|---|---|---|---|---|
| Neoadjuvant chemotherapy before R0 resection | Yes | 7 | 29 | 0.3587 |
| No | 9 | 22 | ||
| Metastasectomy organ | Liver | 14 | 21 | 0.0045 |
| Lung | 1 | 24 | ||
| Other | 1 | 6 | ||
| Tumor burden (tumor diameter) | >1 cm | 15 | 28 | 0.0183 |
| ≤1 cm | 1 | 23 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Park, Y.-S.; Chang, W.-J.; Choi, J.Y.; Lim, A.; Kim, B.; Lee, S.-B.; Lee, J.-W.; Kim, S.-H.; Kim, J.; et al. Clinical Implication of Liquid Biopsy in Colorectal Cancer Patients Treated with Metastasectomy. Cancers 2021, 13, 2231. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092231
Lee S, Park Y-S, Chang W-J, Choi JY, Lim A, Kim B, Lee S-B, Lee J-W, Kim S-H, Kim J, et al. Clinical Implication of Liquid Biopsy in Colorectal Cancer Patients Treated with Metastasectomy. Cancers. 2021; 13(9):2231. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092231
Chicago/Turabian StyleLee, Soohyeon, Young-Soo Park, Won-Jin Chang, Jung Yoon Choi, Ahreum Lim, Boyeon Kim, Saet-Byeol Lee, Jong-Won Lee, Seon-Hahn Kim, Jin Kim, and et al. 2021. "Clinical Implication of Liquid Biopsy in Colorectal Cancer Patients Treated with Metastasectomy" Cancers 13, no. 9: 2231. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092231