
Combined Simplified Molecular Classification of Gastric Adenocarcinoma, Enhanced by Lymph Node Status: An Integrative Approach

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Cohort
2.2. Preparation of a Next-Generation Tissue Microarray (ngTMA®)
2.3. Performance and Scoring of Immunohistochemistry (IHC) and In Situ Hybridization (ISH)
2.4. Next Generation Sequencing (NGS) Analysis
2.5. Statistical Analysis and Presentation of Data
3. Results
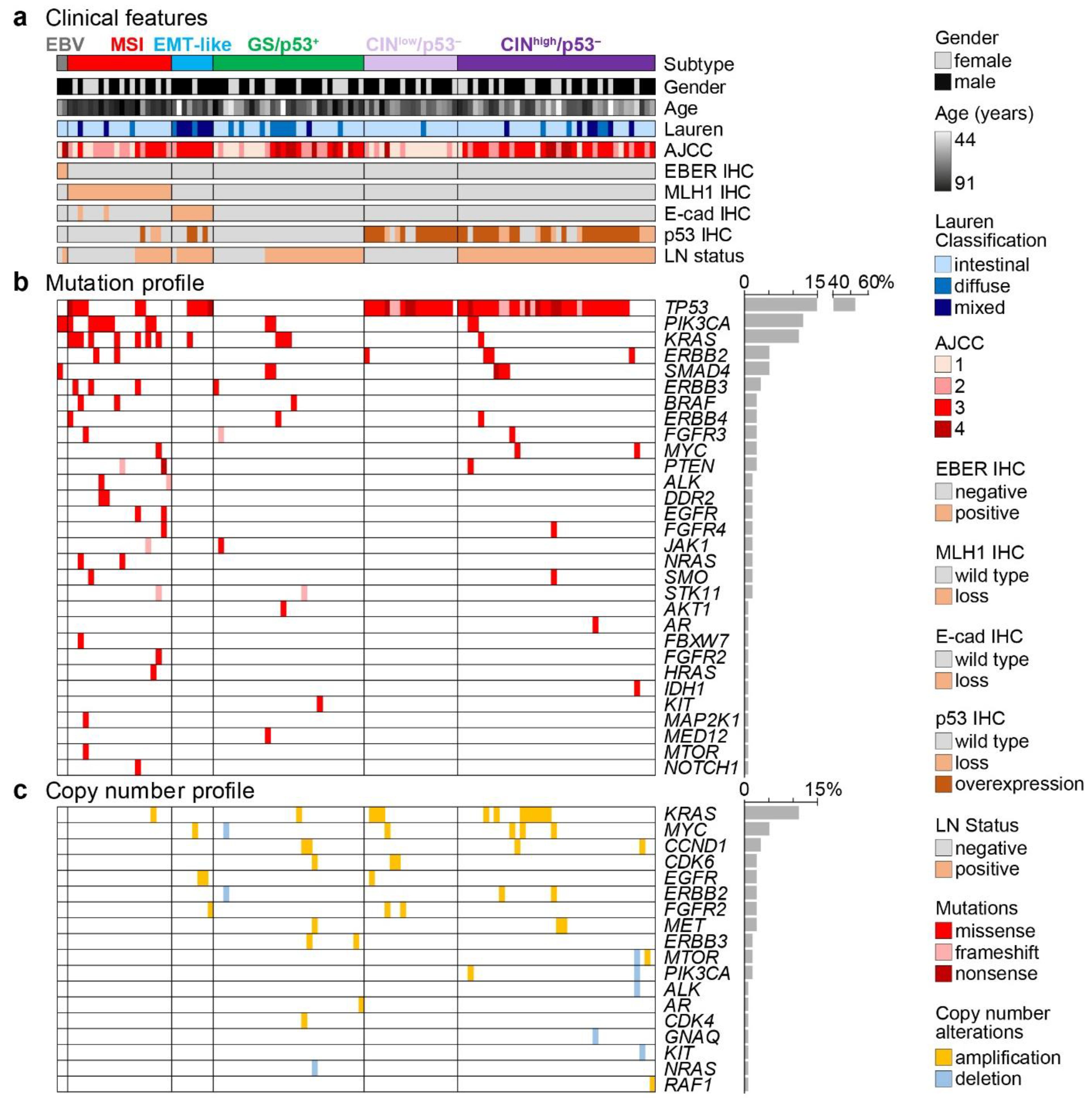
3.1. Patient Data, Histology, In Situ Hybridization and Immunohistochemistry
3.2. Molecular Analysis by Next Generation Sequencing (NGS)
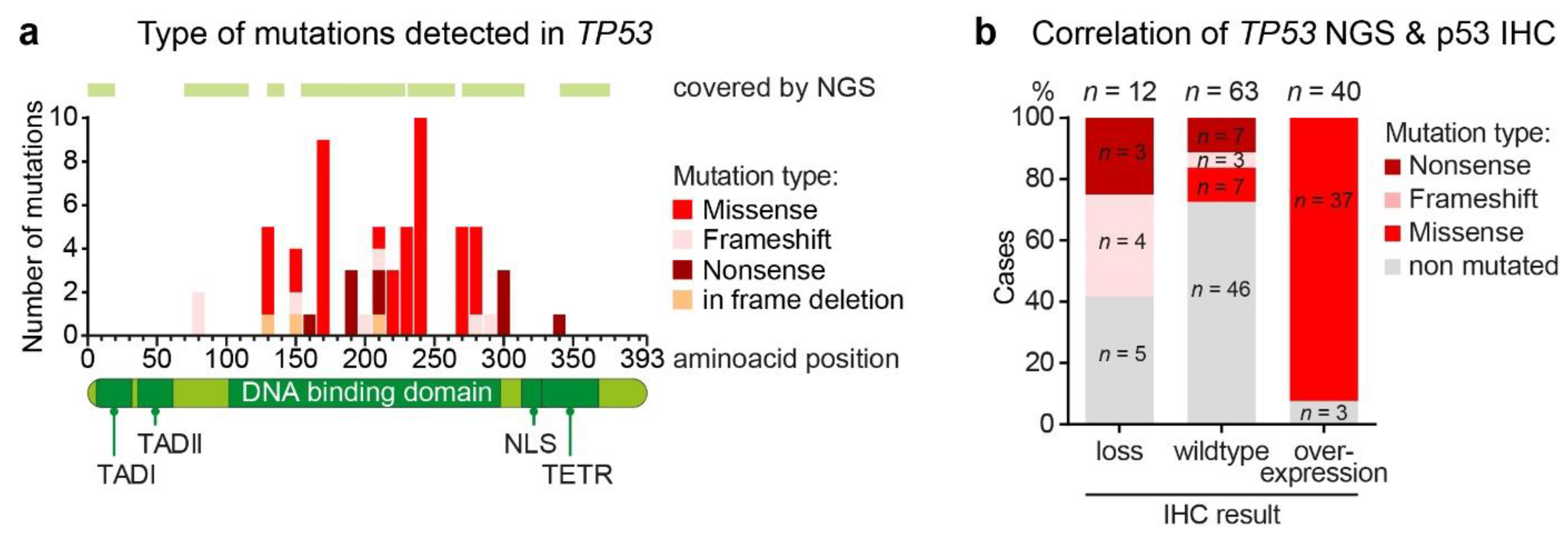
3.3. Aberrant p53 Expression and TP53 Genetic Alterations
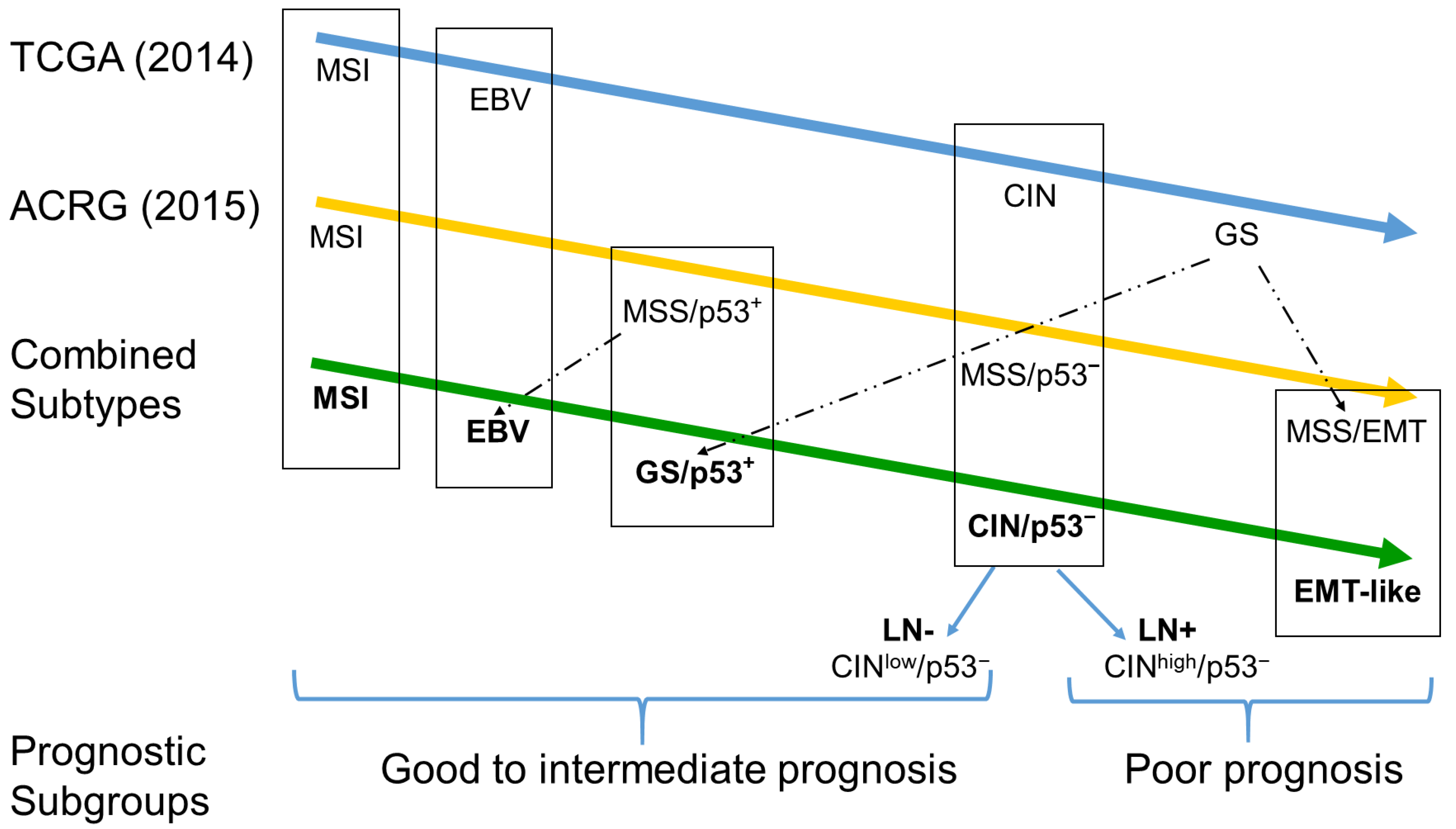
3.4. Classification of GAC Subtype, Based on the TCGA and ACRG Classifications
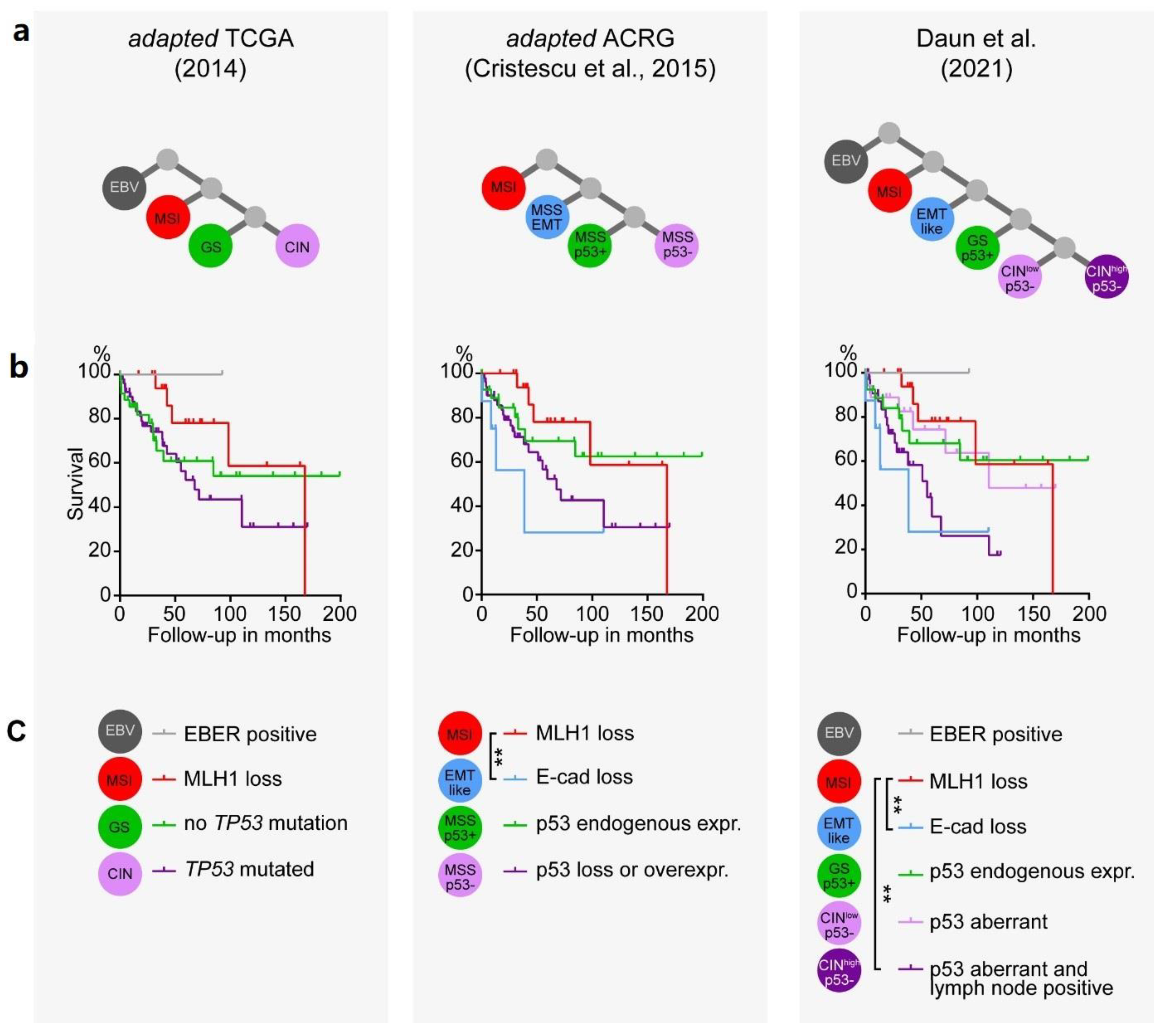
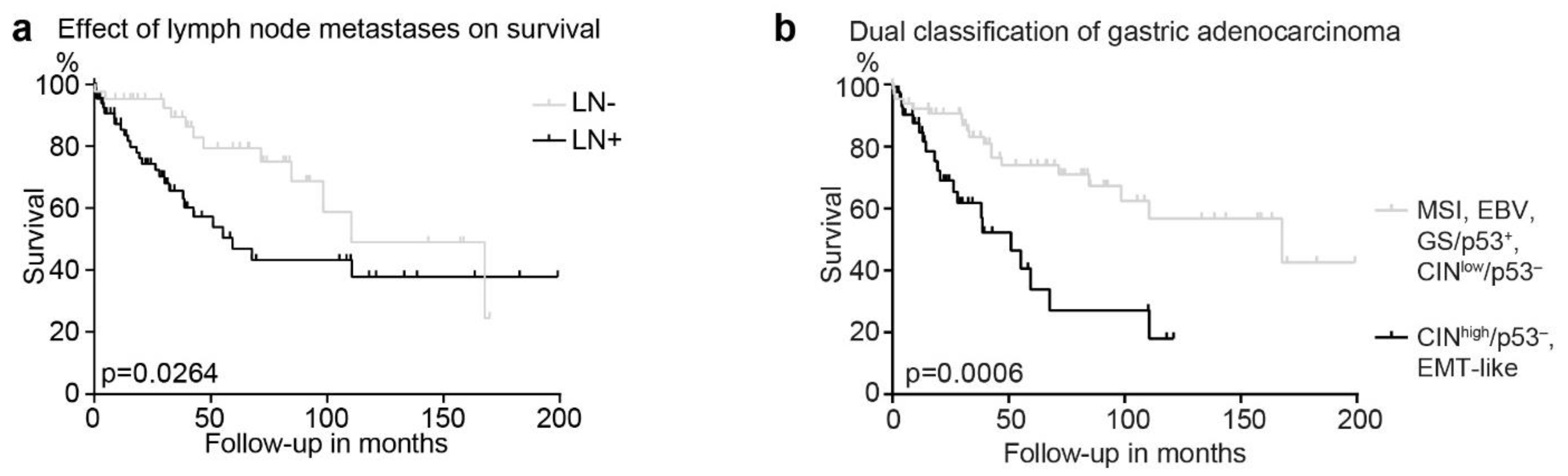
3.5. Survival Analysis within the Classifications of GAC Subtypes and Implementing Lymph Node Metastasis as a Prognostic Marker
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Budgwell, B.; Day, R.; Aloia, T. Managing Early and Late Postoperative Complications Following Gastric Surgery. In Gastric Cancer. Principles and Practice; Strong, V.E., Ed.; Springer: Heidelberg, Germany, 2015; pp. 239–251. [Google Scholar]
- Budgwell, B.; Mansfield, P.F. Open Methods of Resection and Reconstruction for Subtotal and Total Gastrectomy. In Gastric Cancer. Principles and Practice; Strong, V.E., Ed.; Springer: Heidelberg, Germany, 2015; pp. 199–211. [Google Scholar]
- Ku, G.Y.; Ilson, D.H. Gastric Cancer. Principles and Practice; Strong, V.E., Ed.; Springer: Heidelberg, Germany, 2015; pp. 297–303. [Google Scholar]
- Meyer, H.J.; Nutzmann, J.; Wilke, H. Gastric cancer--actual multimodality treatment strategies. Pol. Przegl. Chir. 2012, 84, 461–469. [Google Scholar] [CrossRef]
- Balakrishnan, M.; George, R.; Sharma, A.; Graham, D.Y. Changing Trends in Stomach Cancer Throughout the World. Curr. Gastroenterol. Rep. 2017, 19, 36. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. Digestive System Tumours, 5th ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2019; Volume 1.
- Ajani, J.A.; Lee, J.; Sano, T.; Janjigian, Y.Y.; Fan, D.; Song, S. Gastric adenocarcinoma. Nat. Rev. Dis. Primers 2017, 3, 17036. [Google Scholar] [CrossRef]
- Lauren, P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and So-Called Intestinal-Type Carcinoma: An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Mariette, C.; Carneiro, F.; Grabsch, H.I.; van der Post, R.S.; Allum, W.; de Manzoni, G.; European Chapter of International Gastric Cancer Association. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer 2019, 22, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA Approval Summary: Pembrolizumab for the Treatment of Microsatellite Instability-High Solid Tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef] [Green Version]
- Bass, A.J.; Thorsson, V.; Shmulevich, I.; Reynolds, S.M.; Miller, M.; Bernard, B. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef]
- Sohn, B.H.; Hwang, J.E.; Jang, H.J.; Lee, H.S.; Oh, S.C.; Shim, J.J.; Lee, K.W.; Kim, E.H.; Yim, S.Y.; Lee, S.H.; et al. Clinical Significance of Four Molecular Subtypes of Gastric Cancer Identified by The Cancer Genome Atlas Project. Clin. Cancer Res. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, R.S.; Messing, S.; Tu, X.; McMahon, L.A.; Whitney-Miller, C.L. Immunohistochemistry as a surrogate for molecular subtyping of gastric adenocarcinoma. Hum. Pathol. 2016, 56, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Setia, N.; Agoston, A.T.; Han, H.S.; Mullen, J.T.; Duda, D.G.; Clark, J.W.; Deshpande, V.; Mino-Kenudson, M.; Srivastava, A.; Lennerz, J.K. A protein and mRNA expression-based classification of gastric cancer. Mod. Pathol. 2016, 29, 772–784. [Google Scholar] [CrossRef]
- Pinto, M.P.; Cordova-Delgado, M.; Retamal, I.N.; Munoz-Medel, M.; Bravo, M.L.; Duran, D.; Villanueva, F.; Sanchez, C.; Acevedo, F.; Mondaca, S.; et al. A Molecular Stratification of Chilean Gastric Cancer Patients with Potential Clinical Applicability. Cancers 2020, 12, 1864. [Google Scholar] [CrossRef]
- Ahn, S.; Lee, S.J.; Kim, Y.; Kim, A.; Shin, N.; Choi, K.U.; Lee, C.H.; Huh, G.Y.; Kim, K.M.; Setia, N.; et al. High-throughput Protein and mRNA Expression-based Classification of Gastric Cancers Can Identify Clinically Distinct Subtypes, Concordant With Recent Molecular Classifications. Am. J. Surg. Pathol. 2017, 41, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.; Lee, K.W.; Nam, S.K.; Seo, A.N.; Kim, J.W.; Kim, J.W.; Park, D.J.; Kim, H.H.; Kim, W.H.; Lee, H.S. Development and Validation of an Easy-to-Implement, Practical Algorithm for the Identification of Molecular Subtypes of Gastric Cancer: Prognostic and Therapeutic Implications. Oncologist 2019, 24, e1321–e1330. [Google Scholar] [CrossRef] [Green Version]
- Sanjeevaiah, A.; Cheedella, N.; Hester, C.; Porembka, M.R. Gastric Cancer: Recent Molecular Classification Advances, Racial Disparity, and Management Implications. J. Oncol. Pract. 2018, 14, 217–224. [Google Scholar] [CrossRef]
- Schoop, I.; Maleki, S.S.; Behrens, H.M.; Kruger, S.; Haag, J.; Rocken, C. p53 immunostaining cannot be used to predict TP53 mutations in gastric cancer: Results from a large Central European cohort. Hum. Pathol. 2020, 105, 53–66. [Google Scholar] [CrossRef]
- Zlobec, I.; Suter, G.; Perren, A.; Lugli, A. A next-generation tissue microarray (ngTMA) protocol for biomarker studies. J. Vis. Exp. 2014, e51893. [Google Scholar] [CrossRef] [Green Version]
- Pelliccia, C.; Caselli, E.; Mandarano, M.; Del Sordo, R.; Bellezza, G.; Sidoni, A. The implementation of a commercially available multi-gene profile test for breast cancer characterization in a department of pathology: What have we learned from the first 100 cases? Virchows Arch. 2021, 478, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Businello, G.; Galuppini, F.; Fassan, M. The impact of recent next generation sequencing and the need for a new classification in gastric cancer. Best Pract. Res. Clin. Gastroenterol. 2021, 50–51, 101730. [Google Scholar] [CrossRef] [PubMed]
- Cislo, M.; Filip, A.A.; Arnold Offerhaus, G.J.; Cisel, B.; Rawicz-Pruszynski, K.; Skierucha, M.; Polkowski, W.P. Distinct molecular subtypes of gastric cancer: From Lauren to molecular pathology. Oncotarget 2018, 9, 19427–19442. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Liu, G.; Hu, C. Molecular Classification of Gastric Adenocarcinoma. Gastroenterol. Res. 2019, 12, 275–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulley, M.L. Molecular diagnosis of Epstein-Barr virus-related diseases. J. Mol. Diagn. 2001, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Shia, J. Immunohistochemistry versus microsatellite instability testing for screening colorectal cancer patients at risk for hereditary nonpolyposis colorectal cancer syndrome. Part I. The utility of immunohistochemistry. J. Mol. Diagn. 2008, 10, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Gu, L.; Chen, M.; Guo, D.; Zhu, H.; Zhang, W.; Pan, J.; Zhong, X.; Li, X.; Qian, H.; Wang, X. PD-L1 and gastric cancer prognosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0182692. [Google Scholar] [CrossRef]
- Camargo, M.C.; Kim, W.H.; Chiaravalli, A.M.; Kim, K.M.; Corvalan, A.H.; Matsuo, K.; Yu, J.; Sung, J.J.; Herrera-Goepfert, R.; Meneses-Gonzalez, F.; et al. Improved survival of gastric cancer with tumour Epstein-Barr virus positivity: An international pooled analysis. Gut 2014, 63, 236–243. [Google Scholar] [CrossRef]
- Paasinen-Sohns, A.; Koelzer, V.H.; Frank, A.; Schafroth, J.; Gisler, A.; Sachs, M.; Graber, A.; Rothschild, S.I.; Wicki, A.; Cathomas, G.; et al. Single-Center Experience with a Targeted Next Generation Sequencing Assay for Assessment of Relevant Somatic Alterations in Solid Tumors. Neoplasia 2017, 19, 196–206. [Google Scholar] [CrossRef]
- Boettcher, S.; Miller, P.G.; Sharma, R.; McConkey, M.; Leventhal, M.; Krivtsov, A.V.; Giacomelli, A.O.; Wong, W.; Kim, J.; Chao, S.; et al. A dominant-negative effect drives selection of TP53 missense mutations in myeloid malignancies. Science 2019, 365, 599–604. [Google Scholar] [CrossRef]
- Yemelyanova, A.; Vang, R.; Kshirsagar, M.; Lu, D.; Marks, M.A.; Shih, I.M.; Kurman, R.J. Immunohistochemical staining patterns of p53 can serve as a surrogate marker for TP53 mutations in ovarian carcinoma: An immunohistochemical and nucleotide sequencing analysis. Mod. Pathol. 2011, 24, 1248–1253. [Google Scholar] [CrossRef]
- Koessler, T.; Paradiso, V.; Piscuoglio, S.; Nienhold, R.; Ho, L.; Christinat, Y.; Terracciano, L.M.; Cathomas, G.; Wicki, A.; McKee, T.A.; et al. Reliability of liquid biopsy analysis: An inter-laboratory comparison of circulating tumor DNA extraction and sequencing with different platforms. Lab. Investig. 2020, 100, 1475–1484. [Google Scholar] [CrossRef]
- Ando, K.; Oki, E.; Saeki, H.; Yan, Z.; Tsuda, Y.; Hidaka, G.; Kasagi, Y.; Otsu, H.; Kawano, H.; Kitao, H.; et al. Discrimination of p53 immunohistochemistry-positive tumors by its staining pattern in gastric cancer. Cancer Med. 2015, 4, 75–83. [Google Scholar] [CrossRef]
- Dislich, B.; Blaser, N.; Berger, M.D.; Gloor, B.; Langer, R. Preservation of Epstein-Barr virus status and mismatch repair protein status along the metastatic course of gastric cancer. Histopathology 2020, 76, 740–747. [Google Scholar] [CrossRef]
- Tavakoli, A.; Monavari, S.H.; Solaymani Mohammadi, F.; Kiani, S.J.; Armat, S.; Farahmand, M. Association between Epstein-Barr virus infection and gastric cancer: A systematic review and meta-analysis. BMC Cancer 2020, 20, 493. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n | % |
|---|---|---|
| Gender | ||
| male | 74 | 64.3% |
| female | 41 | 35.7% |
| Age | ||
| range: median (min–max) | 74 (44–91) | |
| Anatomic region | ||
| GEJ | 12 | 10.4% |
| Cardia | 33 | 28.7% |
| Corpus | 16 | 13.9% |
| Antrum | 54 | 47.0% |
| Lauren classification | ||
| Intestinal | 83 | 72.2% |
| Diffuse | 17 | 14.8% |
| mixed | 15 | 13.0% |
| WHO classification | ||
| Tubular | 80 | 69.6% |
| Papillary | 1 | 0.9% |
| Mucinous | 3 | 2.6% |
| Poorly cohesive | 17 | 14.8% |
| Mixed | 14 | 12.2% |
| Pathologic T | n | % |
| 1 | 21 | 18.3% |
| 2 | 24 | 20.9% |
| 3 | 37 | 32.2% |
| 4 | 33 | 28.7% |
| Pathologic N | ||
| 0 | 43 | 37.4% |
| 1+ | 72 | 62.6% |
| Pathologic N according to AJCC | ||
| 0 | 43 | 37.4% |
| 1 | 24 | 20.8% |
| 2 | 18 | 15.7% |
| 3 | 30 | 26.1% |
| Pathologic M | ||
| 0 | 103 | 89.6% |
| 1 | 12 | 10.4% |
| AJCC stage | ||
| 1 | 32 | 28% |
| 2 | 30 | 26% |
| 3 | 41 | 36% |
| 4 | 12 | 10% |
| Characteristic | EBV | MSI | EMT-Like | GS/p53+ | CINlow/p53− | CINhigh/p53− | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | n | % | n | % | n | % | n | % | n | % | n | % | |
| 2 | 1.7% | 20 | 17.4% | 8 | 7.0% | 29 | 25.2% | 18 | 15.7% | 38 | 33.0% | ||
| Gender | |||||||||||||
| male | 2 | 100% | 10 | 50.0% | 7 | 87.5% | 18 | 62.1% | 13 | 72.2% | 24 | 63.2% | 0.5001 |
| female | 0 | 0.0% | 10 | 50.0% | 1 | 12.5% | 11 | 37.9% | 5 | 27.8% | 14 | 36.8% | |
| Age | |||||||||||||
| median (min–max) | 82 (61–91) | 82 (61–91) | 74 (44–81) | 74 (44–90) | 73 (61–89) | 68 (44–84) | 0.0004 a | ||||||
| Median survival | |||||||||||||
| months | undefined | 167.8 | 38.7 | undefined | 110.5 | 55.3 | 0.0372 | ||||||
| Anatomic region | |||||||||||||
| GEJ | 0 | 0.0% | 1 | 5.0% | 0 | 0.0% | 2 | 6.9% | 5 | 27.8% | 4 | 10.5% | 0.0288 |
| Cardia | 1 | 50.0% | 2 | 10.0% | 3 | 37.5% | 8 | 27.6% | 6 | 33.3% | 13 | 34.2% | |
| Corpus | 1 | 50.0% | 1 | 5.0% | 0 | 0.0% | 2 | 6.9% | 2 | 11.1% | 10 | 26.3% | |
| Antrum | 0 | 0.0% | 16 | 80.0% | 5 | 62.5% | 17 | 58.6% | 5 | 27.8% | 11 | 28.9% | |
| Lauren classification | |||||||||||||
| Intestinal | 2 | 100% | 17 | 85.0% | 0 | 0.0% | 19 | 65.5% | 17 | 94.4% | 28 | 73.7% | 0.0404 |
| Diffuse | 0 | 0.0% | 1 | 5.0% | 2 | 25.0% | 9 | 31.0% | 1 | 5.6% | 4 | 10.5% | |
| mixed | 0 | 0.0% | 2 | 10.0% | 6 | 75.0% | 1 | 3.4% | 0 | 0.0% | 6 | 15.8% | |
| WHO classification | |||||||||||||
| Tubular | 2 | 100% | 17 | 85.0% | 0 | 0.0% | 17 | 58.6% | 16 | 88.9% | 28 | 73.7% | 0.3522 |
| Papillary | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | 1 | 3.4% | 0 | 0.0% | 0 | 0.0% | |
| Mucinous | 0 | 0.0% | 1 | 5.0% | 1 | 12.5% | 1 | 3.4% | 0 | 0.0% | 0 | 0.0% | |
| Poorly cohesive | 0 | 0.0% | 0 | 0.0% | 3 | 37.5% | 8 | 27.6% | 1 | 5.6% | 5 | 13.2% | |
| Mixed | 0 | 0.0% | 2 | 10.0% | 4 | 50.0% | 2 | 6.9% | 1 | 5.6% | 5 | 13.2% | |
| Pathologic T | |||||||||||||
| 1 | 0 | 0.0% | 2 | 10.0% | 0 | 0.0% | 7 | 24.1% | 8 | 44.4% | 4 | 10.5% | 0.1517 |
| 2 | 1 | 50.0% | 4 | 20.0% | 1 | 12.5% | 6 | 20.7% | 6 | 33.3% | 6 | 15.8% | |
| 3 | 0 | 0.0% | 8 | 40.0% | 3 | 37.5% | 7 | 24.1% | 4 | 22.2% | 15 | 39.5% | |
| 4 | 1 | 50.0% | 6 | 30.0% | 4 | 50.0% | 9 | 31.0% | 0 | 0.0% | 13 | 34.2% | |
| Pathologic N | |||||||||||||
| 0 | 1 | 50.0% | 13 | 65.0% | 1 | 12.5% | 10 | 34.5% | 18 | 100% | 0 | 0.0% | <0.0001 |
| 1+ | 1 | 50.0% | 7 | 35.0% | 7 | 87.5% | 19 | 65.5% | 0 | 0.0% | 38 | 100% | |
| Pathologic N according to AJCC | |||||||||||||
| 0 | 1 | 50.0% | 13 | 65.0% | 1 | 12.5% | 10 | 34.5% | 18 | 100% | 0 | 0.0% | <0.0001 |
| 1 | 0 | 0.0% | 2 | 10.0% | 0 | 0.0% | 8 | 27.6% | 0 | 0.0% | 14 | 36.8% | |
| 2 | 0 | 0.0% | 3 | 15.0% | 3 | 37.5% | 5 | 17.2% | 0 | 0.0% | 7 | 18.4% | |
| 3 | 1 | 50.0% | 2 | 10.0% | 4 | 50.0% | 6 | 20.7% | 0 | 0.0% | 17 | 44.7% | |
| Pathologic M | |||||||||||||
| 0 | 1 | 50.0% | 20 | 100% | 8 | 100% | 23 | 79.3% | 17 | 94.4% | 34 | 89.5% | 0.1113 |
| 1 | 1 | 50.0% | 0 | 0.0% | 0 | 0.0% | 6 | 20.7% | 1 | 5.6% | 4 | 10.5% | |
| AJCC stage | |||||||||||||
| 1 | 1 | 50% | 5 | 25% | 0 | 0% | 9 | 31% | 13 | 72% | 4 | 11% | <0.0001 |
| 2 | 0 | 0% | 9 | 45% | 1 | 13% | 7 | 24% | 4 | 22% | 9 | 24% | |
| 3 | 0 | 0% | 6 | 30% | 7 | 88% | 7 | 24% | 0 | 0% | 21 | 55% | |
| 4 | 1 | 50% | 0 | 0% | 0 | 0% | 6 | 21% | 1 | 6% | 4 | 11% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daun, T.; Nienhold, R.; Paasinen-Sohns, A.; Frank, A.; Sachs, M.; Zlobec, I.; Cathomas, G. Combined Simplified Molecular Classification of Gastric Adenocarcinoma, Enhanced by Lymph Node Status: An Integrative Approach. Cancers 2021, 13, 3722. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153722
Daun T, Nienhold R, Paasinen-Sohns A, Frank A, Sachs M, Zlobec I, Cathomas G. Combined Simplified Molecular Classification of Gastric Adenocarcinoma, Enhanced by Lymph Node Status: An Integrative Approach. Cancers. 2021; 13(15):3722. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153722
Chicago/Turabian StyleDaun, Till, Ronny Nienhold, Aino Paasinen-Sohns, Angela Frank, Melanie Sachs, Inti Zlobec, and Gieri Cathomas. 2021. "Combined Simplified Molecular Classification of Gastric Adenocarcinoma, Enhanced by Lymph Node Status: An Integrative Approach" Cancers 13, no. 15: 3722. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153722