
Occurrence of Sinonasal Intestinal-Type Adenocarcinoma and Non-Intestinal-Type Adenocarcinoma in Two Countries with Different Patterns of Wood Dust Exposure

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Pathology and Immunohistochemistry
2.3. Work History and Exposure Assessment
2.4. Statistical Analysis
3. Results
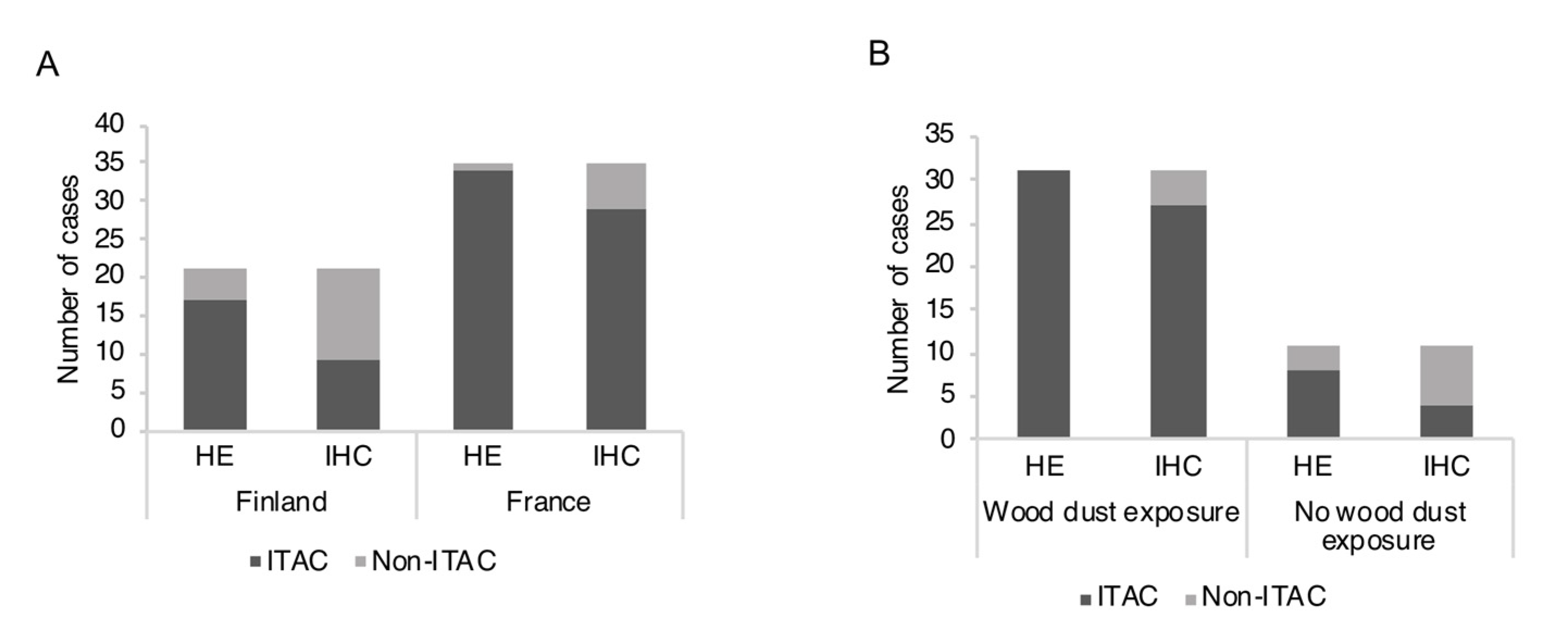
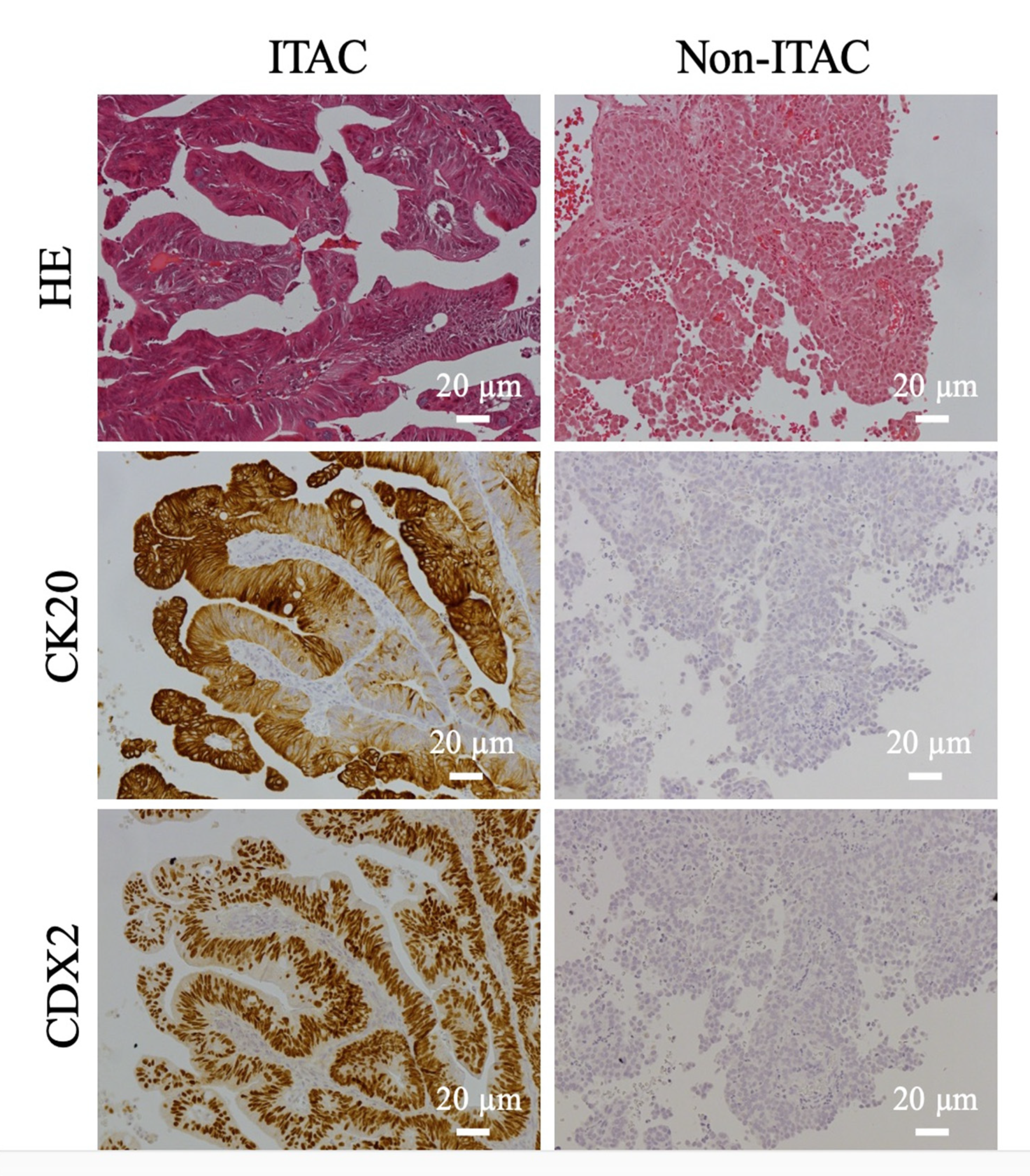
3.1. Classification of SNACs into ITACs and Non-ITACs by Routine HE Staining Is Not Always Supported by IHC
3.2. Relative Numbers of ITAC and Non-ITAC Differ between France and Finland
3.3. ITAC and Occupational Exposure
3.4. Ki-67 Index and CEA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Husgafvel-Pursiainen, K.; Carton, M.; Luce, D.; Wolff, H.; Holmila, R.; Schünssen, V.; Bornholdt, J.; Hansen, J. Sinonasal Cancer. In Occupational Cancers; Anttila, S., Boffetta, P., Eds.; Springer: London, UK, 2014. [Google Scholar]
- International Agency for Research on Cancer (IARC). Cancer risk from occupational exposure to wood dust. A Pooled Analysis of Epidemiological Studies. In IARC Technical Report; IARC: Lyon, France, 1998; p. 30. [Google Scholar]
- International Agency for Research on Cancer (IARC). Arsenic, Metals, Fibres and Dusts. IARC Monogr. Eval. Carcinog. Risk Chem. Hum. 2012, 100C, 407–465. [Google Scholar]
- Stelow, E.B.; Franchi, A.; Wenig, B.M. Intestinal-type adenocarcinoma. In WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.J., Eds.; IARC: Lyon, France, 2017; Volume 9, pp. 23–24. [Google Scholar]
- Stelow, E.B.; Brandwein-Gensler, M.; Franchi, A.; Nicolai, P.; Wenig, B.M. Non-intestinal-type adenocarcinoma. In WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.J., Eds.; IARC: Lyon, France, 2017; Volume 9, pp. 24–26. [Google Scholar]
- Barnes, L. Intestinal-type adenocarcinoma of the nasal cavity and paranasal sinuses. Am. J. Surg. Pathol. 1986, 10, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Leivo, I. Intestinal-type adenocarcinoma: Classification, immunophenotype, molecular features and differential diagnosis. Head Neck Pathol. 2017, 11, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skalova, A.; Sar, A.; Laco, J.; Metelkova, A.; Miesbauerova, M.; Steiner, P.; Svajdler, M.; Michal, M. The Role of SATB2 as a Diagnostic Marker of Sinonasal Intestinal-type Adenocarcinoma. Appl. Immunohistochem. Mol. Morphol. 2018, 26, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Franchi, A.; Massi, D.; Palomba, A.; Biancalani, M.; Santucci, M. CDX-2, cytokeratin 7 and cytokeratin 20 immunohistochemical expression in the differential diagnosis of primary adenocarcinomas of the sinonasal tract. Virchows Arch. 2004, 445, 63–67. [Google Scholar] [CrossRef]
- Resto, V.A.; Krane, J.F.; Faquin, W.C.; Lin, D.T. Immunohistochemical distinction of intestinal-type sinonasal adenocarcinoma from metastatic adenocarcinoma of intestinal origin. Ann. Otol. Rhinol. Laryngol. 2006, 115, 59–64. [Google Scholar] [CrossRef]
- Abecasis, J.; Viana, G.; Pissarra, C.; Pereira, T.; Fonseca, I.; Soares, J. Adenocarcinomas of the nasal cavity and paranasal sinuses: A clinicopathological and immunohistochemical study of 14 cases. Histopathology 2004, 45, 254–259. [Google Scholar] [CrossRef]
- Saber, A.T.; Nielsen, L.R.; Dictor, M.; Hagmar, L.; Micozky, Z.; Wallin, H. K-ras mutations in sinonasal adenocarcinomas in patients occupationally exposed to wood or leather dust. Cancer Lett. 1998, 126, 59–65. [Google Scholar] [CrossRef]
- Wu, T.T.; Barnes, L.; Bakker, A.; Swalsky, P.A.; Finkelstein, S.D. K-ras-2 and p53 genotyping of intestinal-type adenocarcinoma of the nasal cavity and paranasal sinuses. Mod. Pathol. 1996, 9, 199–204. [Google Scholar]
- Licitra, L.; Suardi, S.; Bossi, P.; Locati, L.D.; Mariani, L.; Quattrone, P.; Lo Vullo, S.; Oggionni, M.; Olmi, P.; Cantu, G.; et al. Prediction of TP53 status for primary cisplatin, fluorouracil, and leucovorin chemotherapy in ethmoid sinus intestinal-type adenocarcinoma. J. Clin. Oncol. 2004, 22, 4901–4906. [Google Scholar] [CrossRef]
- Perrone, F.; Oggionni, M.; Birindelli, S.; Suardi, S.; Tabano, S.; Romano, R.; Moiraghi, R.L.; Bimbi, G.; Quattrone, P.; Cantu, G.; et al. TP53, p14ARF, p16INK4a and H-ras gene molecular analysis in intestinal-type adenocarcinoma of the nasal cavity and paranasal sinuses. Int. J. Cancer 2003, 105, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Holmila, R.; Bornholdt, J.; Heikkilä, P.; Suitiala, T.; Fevotte, J.; Cyr, D.; Hansen, J.; Snellman, S.M.; Dictor, M.; Steiniche, T.; et al. Mutations in TP53 tumor suppressor gene in wood dust-related sinonasal cancer. Int. J. Cancer 2010, 127, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Cathro, H.P.; Mills, S.E. Immunophenotypic differences between intestinal-type and low-grade papillary sinonasal adenocarcinomas: An immunohistochemical study of 22 cases utilizing CDX2 and MUC2. Am. J. Surg. Pathol. 2004, 28, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Heffner, D.K.; Hyams, V.J.; Hauck, K.W.; Lingeman, C. Low-grade adenocarcinoma of the nasal cavity and paranasal sinuses. Cancer 1982, 50, 312–322. [Google Scholar] [CrossRef]
- Woestenborghs, H.; Van Eyken, P.; Dans, A. Syringocystadenocarcinoma papilliferum in situ with pagetoid spread: A case report. Histopathology 2006, 48, 869–870. [Google Scholar] [CrossRef]
- Skalova, A.; Cardesa, A.; Leivo, I.; Pfaltz, M.; Ryska, A.; Simpson, R.; Michal, M. Sinonasal tubulopapillary low-grade adenocarcinoma. Histopathological, immunohistochemical and ultrastructural features of poorly recognised entity. Virchows Arch. 2003, 443, 152–158. [Google Scholar] [CrossRef]
- Zur, K.B.; Brandwein, M.; Wang, B.; Som, P.; Gordon, R.; Urken, R.L. Primary description of a new entity, renal cell-like carcinoma of the nasal cavity: Van Meegeren in the house of Vermeer. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Stelow, E.B.; Jo, V.Y.; Mills, S.E.; Carlson, D.L. A histologic and immunohistochemical study describing the diversity of tumors classified as sinonasal high-grade nonintestinal adenocarcinomas. Am. J. Surg. Pathol. 2011, 35, 971–980. [Google Scholar] [CrossRef]
- Purgina, B.; Bastaki, J.M.; Duvvuri, U.; Seethala, R.R. A Subset of Sinonasal Non-Intestinal Type Adenocarcinomas are Truly Seromucinous Adenocarcinomas: A Morphologic and Immunophenotypic Assessment and Description of a Novel Pitfall. Head Neck Pathol. 2015, 9, 436–446. [Google Scholar] [CrossRef] [Green Version]
- Imbus, H.R.; Dyson, W.L. A review of nasal cancer in furniture manufacturing and woodworking in North Carolina, the United States, and other countries. J. Occup. Med. 1987, 29, 734–740. [Google Scholar]
- Ironside, P.; Matthews, J. Adenocarcinoma of the nose and paranasal sinuses in woodworkers in the state of Victoria, Australia. Cancer 1975, 36, 1115–1124. [Google Scholar] [CrossRef]
- Leclerc, A.; Luce, D.; Demers, P.A.; Boffetta, P.; Kogevinas, M.; Belli, S.; Bolm-Audorff, U.; Brinton, L.A.; Colin, D.; Comba, P.; et al. Sinonasal cancer and occupation. Results from the reanalysis of twelve case-control studies. Am. J. Ind. Med. 1997, 31, 153–165. [Google Scholar] [CrossRef]
- Luce, D.; Gerin, M.; Leclerc, A.; Morcet, J.F.; Brugère, J.; Goldberg, M. Sinonasal cancer and occupational exposure to formaldehyde and other substances. Int. J. Cancer 1993, 53, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Kleinsasser, O.; Schroeder, H.G. Adenocarcinomas of the inner nose after exposure to wood dust. Morphological findings and relationships between histopathology and clinical behavior in 79 cases. Arch. Otorhinolaryngol. 1988, 245, 1–15. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC). Wood dust and formaldehyde. In IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans; IARC: Lyon, France, 1995; Volume 62, pp. 35–215. [Google Scholar]
- International Agency for Research on Cancer (IARC). Vol. X, Scientific Publication. In Cancer Incidence in Five Continents; Forman, D., Bray, F., Brewster, D.H., et al., Eds.; IARC: Lyon, France, 2014; Volume 164. [Google Scholar]
- Finnish Cancer Registry. Cancer of the Nose and Nasal Cavities (C30-31)-More Accurate Data. Available online: https://syoparekisteri.fi/ (accessed on 16 February 2017).
- Kauppinen, T.; Vincent, R.; Liukkonen, T.; Grzebyk, M.; Kauppinen, A.; Welling, I.; Arezes, P.; Black, N.; Bochmann, F.; Campelo, F.; et al. Occupational exposure to inhalable wood dust in the member states of the European Union. Ann. Occup. Hyg. 2006, 50, 549–561. [Google Scholar] [PubMed]
- Turner, J.H.; Reh, D.D. Incidence and survival in patients with sinonasal cancer: A historical analysis of population-based data. Head Neck 2012, 34, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Holmila, R.; Cyr, D.; Luce, D.; Heikkilä, P.; Dictor, M.; Steiniche, T.; Stjernvall, T.; Bornholdt, J.; Wallin, H.; Wolff, H.; et al. COX-2 and p53 in human sinonasal cancer: COX-2 expression is associated with adenocarcinoma histology and wood-dust exposure. Int. J. Cancer 2008, 122, 2154–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tilson, M.P.; Gallia, G.L.; Bishop, J.A. Among sinonasal tumors, CDX-2 immunoexpression is not restricted to intestinal-type adenocarcinomas. Head Neck Pathol. 2014, 8, 59–65. [Google Scholar] [CrossRef] [Green Version]
- Blot, W.J.; Chow, W.H.; McLaughlin, J.K. Wood dust and nasal cancer risk. A review of the evidence from North America. J. Occup. Environ. Med. 1997, 39, 148–156. [Google Scholar] [CrossRef]
- U. S. Department of Human Health Services (US DHHS). Report on Carcinogens, Background Document for Wood Dust. In National Toxicology Program (NTP); US DHHS: Washington, DC, USA, 2000. [Google Scholar]
- Brinton, L.A.; Blot, W.J.; Becker, J.A.; Winn, D.M.; Browder, J.P.; Farmer, J.C., Jr.; Fraumeni, J.F., Jr. A case-control study of cancers of the nasal cavity and paranasal sinuses. Am. J. Epidemiol. 1984, 119, 896–906. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, T.L. Occupation and squamous cell cancers of the pharynx and sinonasal cavity. Am. J. Ind. Med. 1989, 16, 493–510. [Google Scholar] [CrossRef]
- Vaughan, T.L.; Davis, S. Wood dust exposure and squamous cell cancers of the upper respiratory tract. Am. J. Epidemiol. 1991, 133, 560–564. [Google Scholar] [CrossRef]
- Demers, P.A.; Kogevinas, M.; Boffetta, P.; Leclerc, A.; Luce, D.; Gérin, M.; Battista, G.; Belli, S.; Bolm-Audorf, U.; Brinton, L.A. Wood dust and sino-nasal cancer: Pooled reanalysis of twelve case-control studies. Am. J. Ind. Med. 1995, 28, 151–166. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Intensity of Staining | CK20 | CDX-2 | ||
|---|---|---|---|---|
| Finland | France | Finland | France | |
| n (%) | n (%) | n (%) | n (%) | |
| 0 | 7 (41.2) | 4 (11.8) | 8 (47.1) | 5 (14.7) |
| 1 | 1 (5.9) | 1 (2.9) | 0 (0) | 1 (2.9) |
| 2 | 0 (0) | 5 (14.7) | 0 (0) | 3 (8.8) |
| 3 | 3 (17.6) | 9 (26.5) | 1 (5.9) | 6 (17.6) |
| 4 | 4 (23.5) | 13 (38.2) | 6 (35.3) | 17 (50.0) |
| 5 | 2 (11.8) | 2 (5.9) | 2 (11.8) | 2 (5.9) |
| Tumor Area Stained | ||||
| <10% | 7 (41.2) | 7 (20.6) | 8 (50.0) | 5 (14.7) |
| 10–30% | 2 (11.8) | 3 (8.8) | 0 (0.0) | 1 (2.9) |
| 40–60% | 2 (11.8) | 7 (20.6) | 0 (0.0) | 6 (17.6) |
| 70–100% | 6 (35.3) | 17 (50.0) | 8 (50.0) | 22 (64.7) |
| SNAC | Classification Based on HE | CK20 Positive | CDX-2 Positive | Classification Based on IHC |
|---|---|---|---|---|
| n | n (% a) | n (% a) | n (% a) | |
| Finland | ||||
| ITAC | 17 | 8 (47.1) | 9 (52.9) | 9 (52.9) |
| Non-ITAC | 4 | 0 (0.0) | 0 (0.0) | 12 (300.0) |
| France | ||||
| ITAC | 34 | 25 (73.5) | 27 (79.4) | 29 (85.3) |
| Non-ITAC | 1 | 0 (0.0) | 0 (0.0) | 6 (600.0) |
| Total | ||||
| ITAC | 51 | 33 (64.7) | 36 (70.6) | 38 (74.5) |
| Non-ITAC | 5 | 0 (0.0) | 0 (0.0) | 18 (360.0) |
| Wood Dust Exposure | (HE) ITAC | (HE) Non-ITAC | (IHC) ITAC | (IHC) Non-ITAC |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Yes | 31 (100.0) | 0 (0.0) | 27 (87.1) | 4 (12.9) |
| No | 8 (72.7) | 3 (27.3) | 4 (36.4) | 7 (63.6) |
| Type of Exposure | ||||
| Mainly Hardwood | 18 (100.0) | 0 (0.0) | 16 (88.9) | 2 (11.1) |
| Mainly Softwood | 6 (100.0) | 0 (0.0) | 5 (83.3) | 1 (16.7) |
| Mixed/unspecified | 7 (100.0) | 0 (0.0) | 6 (85.7) | 1 (14.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leivo, I.; Holmila, R.; Luce, D.; Steiniche, T.; Dictor, M.; Heikkilä, P.; Husgafvel-Pursiainen, K.; Wolff, H. Occurrence of Sinonasal Intestinal-Type Adenocarcinoma and Non-Intestinal-Type Adenocarcinoma in Two Countries with Different Patterns of Wood Dust Exposure. Cancers 2021, 13, 5245. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205245
Leivo I, Holmila R, Luce D, Steiniche T, Dictor M, Heikkilä P, Husgafvel-Pursiainen K, Wolff H. Occurrence of Sinonasal Intestinal-Type Adenocarcinoma and Non-Intestinal-Type Adenocarcinoma in Two Countries with Different Patterns of Wood Dust Exposure. Cancers. 2021; 13(20):5245. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205245
Chicago/Turabian StyleLeivo, Ilmo, Reetta Holmila, Danièle Luce, Torben Steiniche, Michael Dictor, Pirjo Heikkilä, Kirsti Husgafvel-Pursiainen, and Henrik Wolff. 2021. "Occurrence of Sinonasal Intestinal-Type Adenocarcinoma and Non-Intestinal-Type Adenocarcinoma in Two Countries with Different Patterns of Wood Dust Exposure" Cancers 13, no. 20: 5245. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205245