
Use of Diagnostic Criteria from ACR and EU-TIRADS Systems to Improve the Performance of Cytology in Thyroid Nodule Triage

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Selection
2.2. Ultrasound Evaluation
2.3. Cytopathology and Histopathology
- new echographic suspicious features—i.e., US features with ≥2 ACR-TIRADS points;
- >20% increase in size;
- enlarged lymph nodes;
- appearance of new suspicious nodules—i.e., with ACR or EU-TIRADS class ≥ 3.
2.4. Statistical Analysis
3. Results
3.1. ACR vs. EU-TIRADS
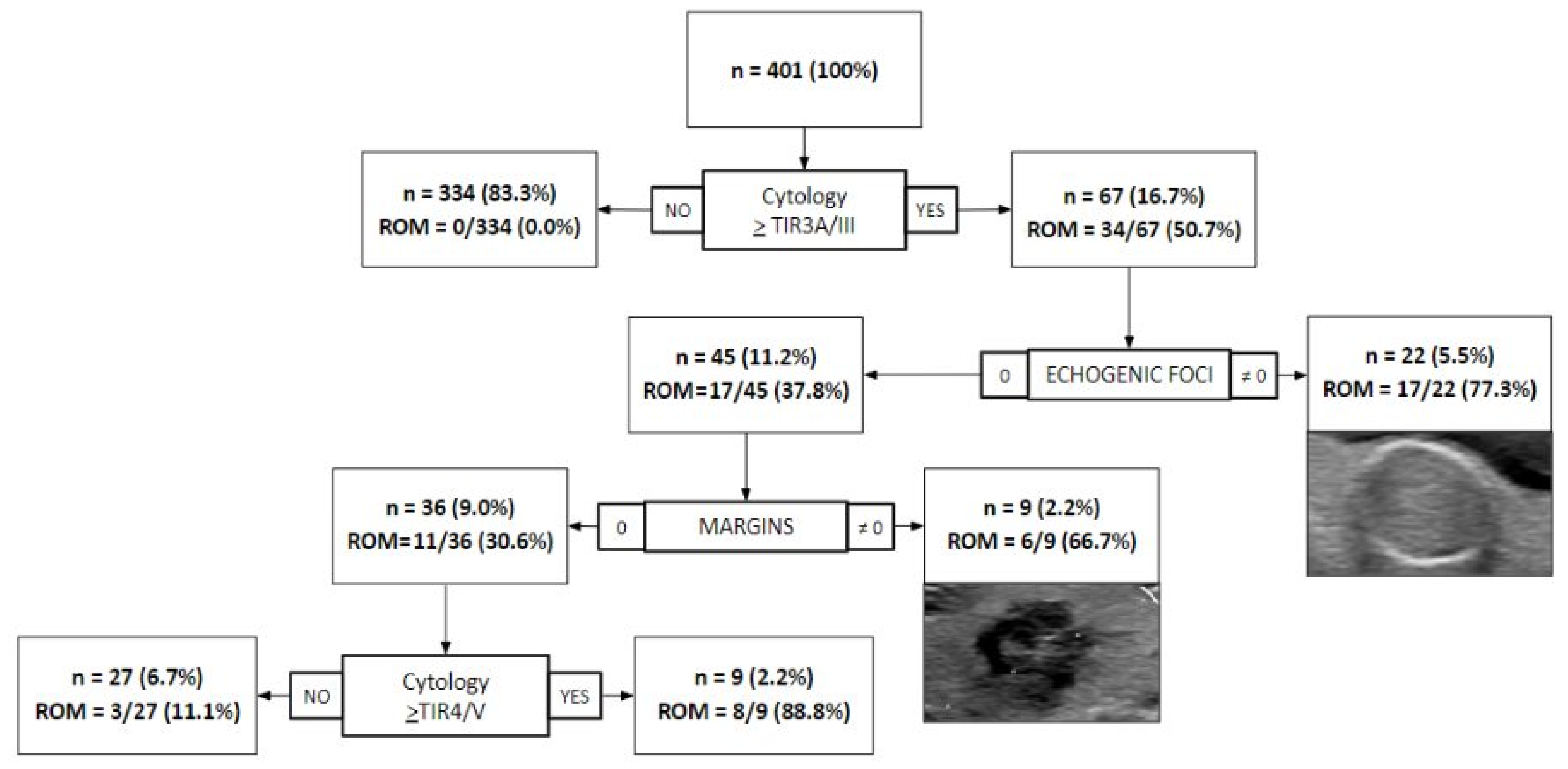
3.2. Combining US Features with Cytology for Diagnostication
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| US | ultrasound |
| FNA | fine-needle aspiration |
| TIRADS | Thyroid Imaging Reporting and Data Systems |
| ACR | American College of Radiology |
| EU | European Thyroid Association |
| AIRC | Italian Association for Research on Cancer |
| SIAPEC | Società Italiana di Anatomia Patologica e Citologia |
| ROM | risk of malignancy |
| PTC | papillary thyroid carcinoma |
| EFVPTC | encapsulated follicular variant of papillary thyroid carcinoma |
References
- Huh, S.; Lee, H.S.; Yoon, J.; Kim, E.-K.; Moon, H.J.; Yoon, J.H.; Park, V.Y.; Kwak, J.Y. Diagnostic Performances and Unnecessary US-FNA Rates of Various TIRADS after Application of Equal Size Thresholds. Sci. Rep. 2020, 10, 10632. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef] [Green Version]
- Horvath, E.; Majlis, S.; Rossi, R.; Franco, C.; Niedmann, J.P.; Castro, A.; Dominguez, M. An Ultrasonogram Reporting System for Thyroid Nodules Stratifying Cancer Risk for Clinical Management. J. Clin. Endocrinol. Metab. 2009, 94, 1748–1751. [Google Scholar] [CrossRef]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid. J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, S.M.; Baek, J.H.; Na, D.G.; Suh, C.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Diagnostic Performance of Practice Guidelines for Thyroid Nodules: Thyroid Nodule Size versus Biopsy Rates. Radiology 2019, 291, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.-Y.; Wang, Y.; Jiang, Y.-X.; Yang, X.; Liu, R.-Y.; Xi, X.-H.; Zhu, S.-L.; Zhao, R.-N.; Lai, X.-J.; Zhang, X.-Y.; et al. Ultrasound Is Helpful to Differentiate Bethesda Class III Thyroid Nodules: A PRISMA-Compliant Systematic Review and Meta-Analysis. Medicine 2017, 96, e6564. [Google Scholar] [CrossRef]
- Leni, D.; Seminati, D.; Fior, D.; Vacirca, F.; Capitoli, G.; Cazzaniga, L.; Di Bella, C.; L’Imperio, V.; Galimberti, S.; Pagni, F. Diagnostic Performances of the ACR-TIRADS System in Thyroid Nodules Triage: A Prospective Single Center Study. Cancers 2021, 13, 2230. [Google Scholar] [CrossRef]
- Xu, T.; Wu, Y.; Wu, R.-X.; Zhang, Y.-Z.; Gu, J.-Y.; Ye, X.-H.; Tang, W.; Xu, S.-H.; Liu, C.; Wu, X.-H. Validation and Comparison of Three Newly-Released Thyroid Imaging Reporting and Data Systems for Cancer Risk Determination. Endocrine 2019, 64, 299–307. [Google Scholar] [CrossRef]
- Shen, Y.; Liu, M.; He, J.; Wu, S.; Chen, M.; Wan, Y.; Gao, L.; Cai, X.; Ding, J.; Fu, X. Comparison of Different Risk-Stratification Systems for the Diagnosis of Benign and Malignant Thyroid Nodules. Front. Oncol. 2019, 9, 378. [Google Scholar] [CrossRef]
- Ahmadi, S.; Oyekunle, T.; Jiang, X.; Scheri, R.; Perkins, J.; Stang, M.; Roman, S.; Sosa, J.A. A direct comparison of the ata and ti-rads ultrasound scoring systems. Endocr. Pract. 2019, 25, 413–422. [Google Scholar] [CrossRef]
- Nardi, F.; Basolo, F.; Crescenzi, A.; Fadda, G.; Frasoldati, A.; Orlandi, F.; Palombini, L.; Papini, E.; Zini, M.; Pontecorvi, A.; et al. Italian Consensus for the Classification and Reporting of Thyroid Cytology. J. Endocrinol. Investig. 2014, 37, 593–599. [Google Scholar] [CrossRef]
- Ali, S.Z.; Cibas, E.S. The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria, and Explanatory Notes; Springer: Berlin/Heidelberg, Germany, 2017; ISBN 9783319605708. [Google Scholar]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedus, L.; Paschke, R.; Valcavi, R.; Vitti, P. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules—2016 Update Appendix. Endocr. Pract. 2016, 22, 1–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacini, F.; Basolo, F.; Bellantone, R.; Boni, G.; Cannizzaro, M.A.; De Palma, M.; Durante, C.; Elisei, R.; Fadda, G.; Frasoldati, A.; et al. Italian Consensus on Diagnosis and Treatment of Differentiated Thyroid Cancer: Joint Statements of Six Italian Societies. J. Endocrinol. Investig. 2018, 41, 849–876. [Google Scholar] [CrossRef] [Green Version]
- Grani, G.; Lamartina, L.; Ascoli, V.; Bosco, D.; Biffoni, M.; Giacomelli, L.; Maranghi, M.; Falcone, R.; Ramundo, V.; Cantisani, V.; et al. Reducing the Number of Unnecessary Thyroid Biopsies While Improving Diagnostic Accuracy: Toward the “Right” TIRADS. J. Clin. Endocrinol. Metab. 2018, 104, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruan, J.-L.; Yang, H.-Y.; Liu, R.-B.; Liang, M.; Han, P.; Xu, X.-L.; Luo, B.-M. Fine Needle Aspiration Biopsy Indications for Thyroid Nodules: Compare a Point-Based Risk Stratification System with a Pattern-Based Risk Stratification System. Eur. Radiol. 2019, 29, 4871–4878. [Google Scholar] [CrossRef]
- Middleton, W.D.; Teefey, S.A.; Reading, C.C.; Langer, J.E.; Beland, M.D.; Szabunio, M.M.; Desser, T.S. Comparison of Performance Characteristics of American College of Radiology TI-RADS, Korean Society of Thyroid Radiology TIRADS, and American Thyroid Association Guidelines. Am. J. Roentgenol. 2018, 210, 1148–1154. [Google Scholar] [CrossRef]
- Kim, P.H.; Suh, C.H.; Baek, J.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Unnecessary Thyroid Nodule Biopsy Rates under Four Ultrasound Risk Stratification Systems: A Systematic Review and Meta-Analysis. Eur. Radiol. 2021, 31, 2877–2885. [Google Scholar] [CrossRef]
- Magri, F.; Chytiris, S.; Croce, L.; Molteni, M.; Bendotti, G.; Gruosso, G.; Tata Ngnitejeu, S.; Agozzino, M.; Rotondi, M.; Chiovato, L. Performance of the ACR TI-RADS and EU TI-RADS Scoring Systems in the Diagnostic Work-up of Thyroid Nodules in a Real-Life Series Using Histology as Reference Standard. Eur. J. Endocrinol. 2020, 183, 521–528. [Google Scholar] [CrossRef]
- Kim, P.H.; Suh, C.H.; Baek, J.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Diagnostic Performance of Four Ultrasound Risk Stratification Systems: A Systematic Review and Meta-Analysis. Thyroid 2020, 30, 1159–1168. [Google Scholar] [CrossRef]
- Castellana, M.; Castellana, C.; Treglia, G.; Giorgino, F.; Giovanella, L.; Russ, G.; Trimboli, P. Performance of Five Ultrasound Risk Stratification Systems in Selecting Thyroid Nodules for FNA. J. Clin. Endocrinol. Metab. 2020, 105, 1659–1669. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Zou, X.; Zeng, H.; Zhao, Y.; Ma, X. Comparison of Diagnostic Performance of Five Different Ultrasound TI-RADS Classification Guidelines for Thyroid Nodules. Front. Oncol. 2020, 10, 598225. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Zhang, B.; Cai, G.; Li, J.; Gu, X. American College of Radiology Thyroid Imaging Report and Data System Combined with K-RAS Mutation Improves the Management of Cytologically Indeterminate Thyroid Nodules. PLoS ONE 2019, 14, e0219383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marina, M.; Zatelli, M.C.; Goldoni, M.; Del Rio, P.; Corcione, L.; Martorana, D.; Percesepe, A.; Bonatti, F.; Mozzoni, P.; Crociara, A.; et al. Combination of Ultrasound and Molecular Testing in Malignancy Risk Estimate of Bethesda Category IV Thyroid Nodules: Results from a Single-Institution Prospective Study. J. Endocrinol. Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Massa, F.; Caraci, P.; Sapino, A.; De Rosa, G.; Volante, M.; Papotti, M. Outcome and Diagnostic Reproducibility of the Thyroid Cytology “indeterminate Categories” SIAPEC/SIE 2014 in a Consecutive Series of 302 Cases. J. Endocrinol. Investig. 2020, 44, 803–809. [Google Scholar] [CrossRef]
- Trimboli, P.; Crescenzi, A.; Giovanella, L. Performance of Italian Consensus for the Classification and Reporting of Thyroid Cytology (ICCRTC) in Discriminating Indeterminate Lesions at Low and High Risk of Malignancy. A Systematic Review and Meta-Analysis. Endocrine 2018, 60, 31–35. [Google Scholar] [CrossRef]
- Hong, M.J.; Na, D.G.; Baek, J.H.; Sung, J.Y.; Kim, J.-H. Cytology-Ultrasonography Risk-Stratification Scoring System Based on Fine-Needle Aspiration Cytology and the Korean-Thyroid Imaging Reporting and Data System. Thyroid 2017, 27, 953–959. [Google Scholar] [CrossRef]
- Na, D.G.; Paik, W.; Cha, J.; Gwon, H.Y.; Kim, S.Y.; Yoo, R.-E. Diagnostic Performance of the Modified Korean Thyroid Imaging Reporting and Data System for Thyroid Malignancy according to Nodule Size: A Comparison with Five Society Guidelines. Ultrasonography 2021, 40, 474–485. [Google Scholar] [CrossRef] [PubMed]
- He, Y.-P.; Xu, H.-X.; Zhao, C.-K.; Sun, L.-P.; Li, X.-L.; Yue, W.-W.; Guo, L.-H.; Wang, D.; Ren, W.-W.; Wang, Q.; et al. Cytologically Indeterminate Thyroid Nodules: Increased Diagnostic Performance with Combination of US TI-RADS and a New Scoring System. Sci. Rep. 2017, 7, 6906. [Google Scholar] [CrossRef] [Green Version]
- Kuru, B.; Kefeli, M.; Danaci, M. Comparison of Five Thyroid Ultrasound Stratification Systems for Differentiation of Benign and Malignant Nodules and to Avoid Biopsy Using Histology as Reference Standard. Endocr. Pract. 2021. [Google Scholar] [CrossRef]


{kind=link}
| ACR-TIRADS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| No Indication of FNA | Indication of FNA | ||||||||
| EU-TIRADS | ACR1 | ACR2 | ACR3 <2.5 cm | ACR4 <1.5 cm | ACR5 <1.0 cm | ACR3 ≥2.5 cm | ACR4 ≥1.5 cm | ACR5 ≥1.0 cm | Total |
| No indication of FNA | |||||||||
| EU 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EU 2 | 30 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 32 |
| EU 3 ≤ 2.0 cm | 0 | 15 | 50 | 3 | 0 | 0 | 1 | 0 | 69 |
| EU 4 ≤ 1.5 cm | 0 | 0 | 19 | 81 | 0 | 0 | 11 | 0 | 111 |
| EU 5 ≤ 1.0 cm | 0 | 0 | 0 | 10 | 3 | 0 | 0 | 6 | 19 |
| Indication of FNA | |||||||||
| EU 3 > 2.0 cm | 0 | 22 | 4 | 0 | 0 | 39 | 9 | 0 | 74 |
| EU 4 > 1.5 cm | 0 | 0 | 8 | 0 | 0 | 16 | 69 | 0 | 93 |
| EU 5 > 1.0 cm | 0 | 0 | 0 | 10 | 0 | 0 | 27 | 45 | 82 |
| Total | 30 | 39 | 81 | 104 | 3 | 55 | 117 | 51 | 480 |
| SIAPEC/Bethesda System | |||||||
|---|---|---|---|---|---|---|---|
| ACR-TIRADS | TIR1c/I | TIR2/II | TIR3A/III | TIR3B/IV | TIR4/V | TIR5/VI | Total |
| No indication of FNA | |||||||
| ACR 1 | 12 | 16 | 2 | 0 | 0 | 0 | 30 |
| ACR 2 | 1 | 33 | 5 | 0 | 0 | 0 | 39 |
| ACR 3 < 2.5 cm | 0 | 63 | 13 | 2 | 2 | 1 | 81 |
| ACR 4 < 1.5 cm | 0 | 72 | 21 | 4 | 3 | 4 | 104 |
| ACR 5 < 1.0 cm | 0 | 0 | 2 | 0 | 1 | 0 | 3 |
| Indication of FNA | |||||||
| ACR 3 ≥ 2.5 cm | 1 | 35 | 15 | 3 | 1 | 0 | 55 |
| ACR 4 ≥ 1.5 cm | 1 | 77 | 29 | 7 | 3 | 0 | 117 |
| ACR 5 ≥ 1.0 cm | 0 | 23 | 9 | 5 | 2 | 12 | 51 |
| Total | 15 | 319 | 96 | 21 | 12 | 17 | 480 |
| SIAPEC/Bethesda System | |||||||
|---|---|---|---|---|---|---|---|
| EU-TIRADS | TIR1c/I | TIR2/II | TIR3A/III | TIR3B/IV | TIR4/V | TIR5/VI | Total |
| No indication of FNA | |||||||
| EU 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EU 2 | 12 | 18 | 2 | 0 | 0 | 0 | 32 |
| EU 3 ≤ 2.0 cm | 0 | 54 | 11 | 1 | 2 | 1 | 69 |
| EU 4 ≤ 1.5 cm | 0 | 84 | 21 | 3 | 2 | 1 | 111 |
| EU 5 ≤ 1.0 cm | 0 | 7 | 7 | 2 | 2 | 1 | 19 |
| Indication of FNA | |||||||
| EU 3 > 2.0 cm | 2 | 47 | 20 | 4 | 1 | 0 | 74 |
| EU 4 > 1.5 cm | 1 | 67 | 20 | 3 | 2 | 0 | 93 |
| EU 5 > 1.0 cm | 0 | 42 | 15 | 8 | 3 | 14 | 82 |
| Total | 15 | 319 | 96 | 21 | 12 | 17 | 480 |
| TP | FP | TN | FN | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |
|---|---|---|---|---|---|---|---|---|
| ACR | 23 | 157 | 210 | 11 | 67.6 (23/34) | 57.2 (210/367) | 12.8 (23/180) | 95.0 (210/221) |
| [49.5–82.6] | [52.0–62.3] | [8.3–18.6] | [91.3–97.5] | |||||
| EU | 24 | 179 | 188 | 10 | 70.6 (24/34) | 51.2 (188/367) | 11.8 (24/203) | 94.9 (188/198) |
| [52.5–84.9] | [46.0–56.4] | [7.7–17.1] | [90.9–97.6] | |||||
| Cytology | 34 | 33 | 334 | 0 | 100 (34/34) | 91.0 (334/367) | 50.7 (34/67) | 100 (334/334) |
| [89.7–100] | [87.6–93.7] | [38.2–63.2] | [98.9–100] | |||||
| Cytology +EF/M | 31 | 9 | 358 | 3 | 91.2 (31/34) | 97.5 (358/367) | 77.5 (31/40) | 99.2 (358/361) |
| [76.3–98.1] | [95.4–98.9] | [61.5–89.2] | [97.6–99.8] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seminati, D.; Capitoli, G.; Leni, D.; Fior, D.; Vacirca, F.; Di Bella, C.; Galimberti, S.; L’Imperio, V.; Pagni, F. Use of Diagnostic Criteria from ACR and EU-TIRADS Systems to Improve the Performance of Cytology in Thyroid Nodule Triage. Cancers 2021, 13, 5439. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215439
Seminati D, Capitoli G, Leni D, Fior D, Vacirca F, Di Bella C, Galimberti S, L’Imperio V, Pagni F. Use of Diagnostic Criteria from ACR and EU-TIRADS Systems to Improve the Performance of Cytology in Thyroid Nodule Triage. Cancers. 2021; 13(21):5439. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215439
Chicago/Turabian StyleSeminati, Davide, Giulia Capitoli, Davide Leni, Davide Fior, Francesco Vacirca, Camillo Di Bella, Stefania Galimberti, Vincenzo L’Imperio, and Fabio Pagni. 2021. "Use of Diagnostic Criteria from ACR and EU-TIRADS Systems to Improve the Performance of Cytology in Thyroid Nodule Triage" Cancers 13, no. 21: 5439. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215439