
Risk of Second Primary Malignancies among Patients with Early Gastric Cancer Exposed to Recurrent Computed Tomography Scans

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
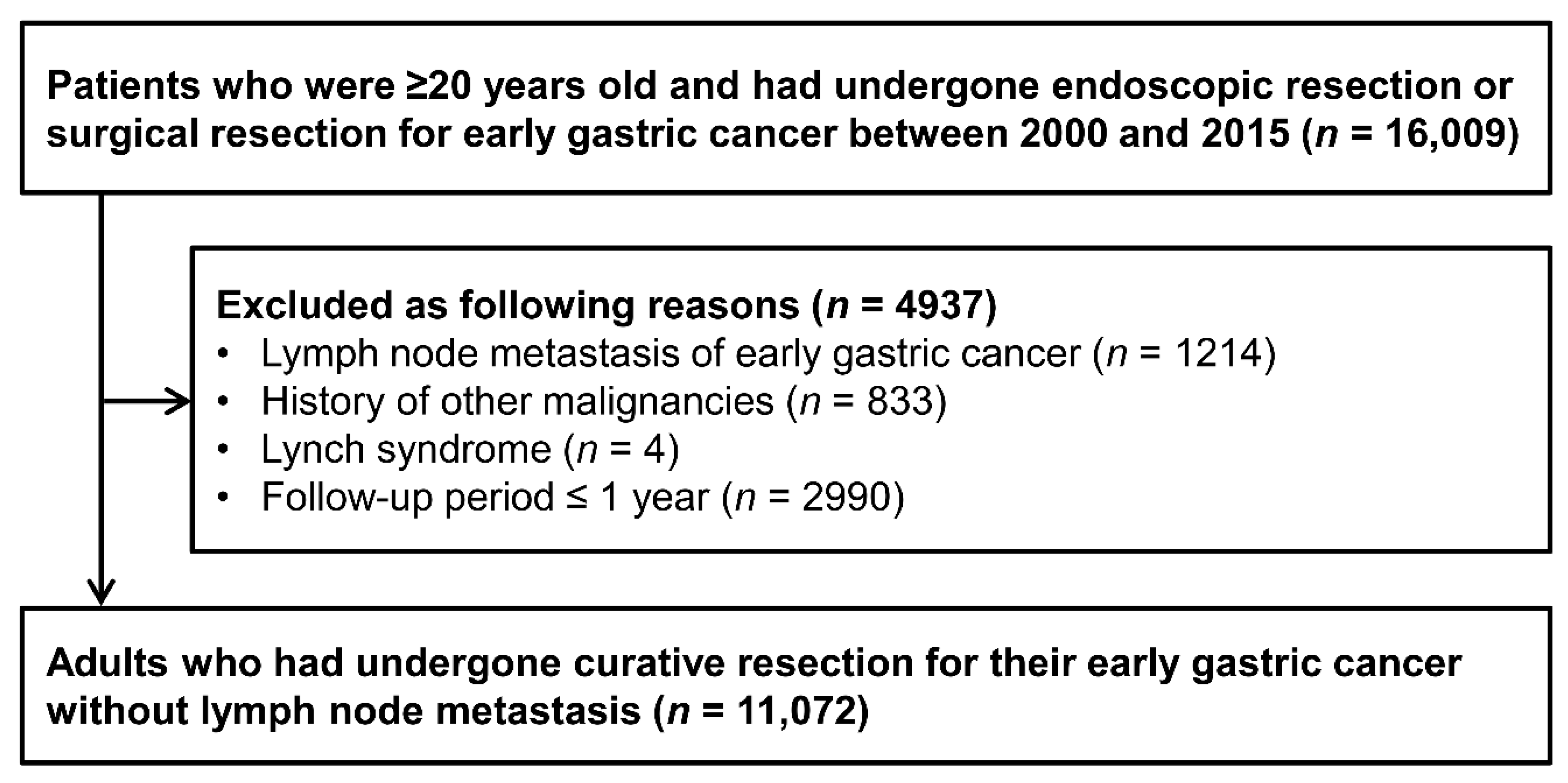
2.1. Study Population
2.2. Study Outcomes
2.3. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mettler, F.A., Jr.; Bhargavan, M.; Faulkner, K.; Gilley, D.B.; Gray, J.E.; Ibbott, G.S.; Lipoti, J.A.; Mahesh, M.; McCrohan, J.L.; Stabin, M.G.; et al. Radiologic and nuclear medicine studies in the United States and worldwide: Frequency, radiation dose, and comparison with other radiation sources—1950–2007. Radiology 2009, 253, 520–531. [Google Scholar] [CrossRef]
- Nam, S.Y.; Choi, I.J.; Park, K.W.; Kim, C.G.; Lee, J.Y.; Kook, M.C.; Lee, J.S.; Park, S.R.; Lee, J.H.; Ryu, K.W.; et al. Effect of repeated endoscopic screening on the incidence and treatment of gastric cancer in health screenees. Eur. J. Gastroenterol. Hepatol. 2009, 21, 855–860. [Google Scholar] [CrossRef]
- Kim, Y.I.; Kim, Y.W.; Choi, I.J.; Kim, C.G.; Lee, J.Y.; Cho, S.J.; Eom, B.W.; Yoon, H.M.; Ryu, K.W.; Kook, M.C. Long-term survival after endoscopic resection versus surgery in early gastric cancers. Endoscopy 2015, 47, 293–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyo, J.H.; Lee, H.; Min, B.H.; Lee, J.H.; Choi, M.G.; Lee, J.H.; Sohn, T.S.; Bae, J.M.; Kim, K.M.; Ahn, J.H.; et al. Long-Term Outcome of Endoscopic Resection vs. Surgery for Early Gastric Cancer: A Non-inferiority-Matched Cohort Study. Am. J. Gastroenterol. 2016, 111, 240–249. [Google Scholar] [CrossRef] [PubMed]
- An, J.Y.; Heo, G.U.; Cheong, J.H.; Hyung, W.J.; Choi, S.H.; Noh, S.H. Assessment of open versus laparoscopy-assisted gastrectomy in lymph node-positive early gastric cancer: A retrospective cohort analysis. J. Surg. Oncol. 2010, 102, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Min, B.H.; Kim, E.R.; Kim, K.M.; Park, C.K.; Lee, J.H.; Rhee, P.L.; Kim, J.J. Surveillance strategy based on the incidence and patterns of recurrence after curative endoscopic submucosal dissection for early gastric cancer. Endoscopy 2015, 47, 784–793. [Google Scholar] [CrossRef] [Green Version]
- Seo, N.; Han, K.; Hyung, W.J.; Chung, Y.E.; Park, C.H.; Kim, J.H.; Lee, S.K.; Kim, M.J.; Noh, S.H.; Lim, J.S. Stratification of Postsurgical Computed Tomography Surveillance Based on the Extragastric Recurrence of Early Gastric Cancer. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Lee, S.; Choi, K.D.; Hong, S.M.; Park, S.H.; Gong, E.J.; Na, H.K.; Ahn, J.Y.; Jung, K.W.; Lee, J.H.; Kim, D.H.; et al. Pattern of extragastric recurrence and the role of abdominal computed tomography in surveillance after endoscopic resection of early gastric cancer: Korean experiences. Gastric. Cancer 2017, 20, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.S.; Kim, S.H.; Kim, S.G.; Han, J.K. Early Gastric Cancers: Is CT Surveillance Necessary after Curative Endoscopic Submucosal Resection for Cancers That Meet the Expanded Criteria? Radiology 2016, 281, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Mettler, F.A., Jr.; Wiest, P.W.; Locken, J.A.; Kelsey, C.A. CT scanning: Patterns of use and dose. J. Radiol. Prot. 2000, 20, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Hall, E.J. Computed tomography—An increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Rehani, M.M.; Berry, M. Radiation doses in computed tomography. The increasing doses of radiation need to be controlled. BMJ 2000, 320, 593–594. [Google Scholar] [CrossRef]
- Park, C.H.; Kim, E.H.; Chung, H.; Park, J.C.; Shin, S.K.; Lee, S.K.; Lee, Y.C.; Lee, H. Role of computed tomography scan for the primary surveillance of mucosal gastric cancer after complete resection by endoscopic submucosal dissection. Surg. Endosc. 2014, 28, 1307–1313. [Google Scholar] [CrossRef]
- Mettler, F.A., Jr.; Huda, W.; Yoshizumi, T.T.; Mahesh, M. Effective doses in radiology and diagnostic nuclear medicine: A catalog. Radiology 2008, 248, 254–263. [Google Scholar] [CrossRef]
- Smith-Bindman, R.; Lipson, J.; Marcus, R.; Kim, K.P.; Mahesh, M.; Gould, R.; Berrington de Gonzalez, A.; Miglioretti, D.L. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch. Intern. Med. 2009, 169, 2078–2086. [Google Scholar] [CrossRef] [PubMed]
- Preston, D.L.; Pierce, D.A.; Shimizu, Y.; Cullings, H.M.; Fujita, S.; Funamoto, S.; Kodama, K. Effect of recent changes in atomic bomb survivor dosimetry on cancer mortality risk estimates. Radiat Res. 2004, 162, 377–389. [Google Scholar] [CrossRef]
- Pierce, D.A.; Preston, D.L. Radiation-related cancer risks at low doses among atomic bomb survivors. Radiat Res. 2000, 154, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Preston, D.L.; Ron, E.; Tokuoka, S.; Funamoto, S.; Nishi, N.; Soda, M.; Mabuchi, K.; Kodama, K. Solid cancer incidence in atomic bomb survivors: 1958–1998. Radiat Res. 2007, 168, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.Y.; Muo, C.H.; Lin, C.Y.; Jen, Y.M.; Yang, M.H.; Lin, J.C.; Sung, F.C.; Kao, C.H. Paediatric head CT scan and subsequent risk of malignancy and benign brain tumour: A nation-wide population-based cohort study. Br. J. Cancer 2014, 110, 2354–2360. [Google Scholar] [CrossRef]
- Journy, N.; Rehel, J.L.; Ducou Le Pointe, H.; Lee, C.; Brisse, H.; Chateil, J.F.; Caer-Lorho, S.; Laurier, D.; Bernier, M.O. Are the studies on cancer risk from CT scans biased by indication? Elements of answer from a large-scale cohort study in France. Br. J. Cancer 2015, 112, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Mathews, J.D.; Forsythe, A.V.; Brady, Z.; Butler, M.W.; Goergen, S.K.; Byrnes, G.B.; Giles, G.G.; Wallace, A.B.; Anderson, P.R.; Guiver, T.A.; et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: Data linkage study of 11 million Australians. BMJ 2013, 346, f2360. [Google Scholar] [CrossRef] [Green Version]
- Miglioretti, D.L.; Johnson, E.; Williams, A.; Greenlee, R.T.; Weinmann, S.; Solberg, L.I.; Feigelson, H.S.; Roblin, D.; Flynn, M.J.; Vanneman, N.; et al. The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk. JAMA Pediatr. 2013, 167, 700–707. [Google Scholar] [CrossRef]
- Pearce, M.S.; Salotti, J.A.; Little, M.P.; McHugh, K.; Lee, C.; Kim, K.P.; Howe, N.L.; Ronckers, C.M.; Rajaraman, P.; Sir Craft, A.W.; et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: A retrospective cohort study. Lancet 2012, 380, 499–505. [Google Scholar] [CrossRef] [Green Version]
- Meulepas, J.M.; Ronckers, C.M.; Smets, A.; Nievelstein, R.A.J.; Gradowska, P.; Lee, C.; Jahnen, A.; van Straten, M.; de Wit, M.Y.; Zonnenberg, B.; et al. Radiation Exposure From Pediatric CT Scans and Subsequent Cancer Risk in the Netherlands. J. Natl. Cancer Inst. 2019, 111, 256–263. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Bruesewitz, M.R.; Kofler, J.M., Jr. CT dose reduction and dose management tools: Overview of available options. Radiographics 2006, 26, 503–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalra, M.K.; Maher, M.M.; Toth, T.L.; Hamberg, L.M.; Blake, M.A.; Shepard, J.A.; Saini, S. Strategies for CT radiation dose optimization. Radiology 2004, 230, 619–628. [Google Scholar] [CrossRef]
- Stopsack, K.H.; Cerhan, J.R. Cumulative Doses of Ionizing Radiation From Computed Tomography: A Population-Based Study. Mayo Clin. Proc. 2019, 94, 2011–2021. [Google Scholar] [CrossRef] [PubMed]
- Tonolini, M.; Valconi, E.; Vanzulli, A.; Bianco, R. Radiation overexposure from repeated CT scans in young adults with acute abdominal pain. Emerg. Radiol. 2018, 25, 21–27. [Google Scholar] [CrossRef]
- Sodickson, A.; Baeyens, P.F.; Andriole, K.P.; Prevedello, L.M.; Nawfel, R.D.; Hanson, R.; Khorasani, R. Recurrent CT, cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology 2009, 251, 175–184. [Google Scholar] [CrossRef]
- Youn, H.G.; An, J.Y.; Choi, M.G.; Noh, J.H.; Sohn, T.S.; Kim, S. Recurrence after curative resection of early gastric cancer. Ann. Surg. Oncol. 2010, 17, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Baiocchi, G.L.; Marrelli, D.; Verlato, G.; Morgagni, P.; Giacopuzzi, S.; Coniglio, A.; Marchet, A.; Rosa, F.; Capponi, M.G.; Di Leo, A.; et al. Follow-up after gastrectomy for cancer: An appraisal of the Italian research group for gastric cancer. Ann. Surg. Oncol. 2014, 21, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Hur, H.; Song, K.Y.; Park, C.H.; Jeon, H.M. Follow-up strategy after curative resection of gastric cancer: A nationwide survey in Korea. Ann. Surg. Oncol. 2010, 17, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, R.; Coburn, N.G.; Seevaratnam, R.; Mahar, A.; Helyer, L.; Law, C.; Singh, S. A systematic review of patient surveillance after curative gastrectomy for gastric cancer: A brief review. Gastric. Cancer 2012, 15 (Suppl. 1), S164–S167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Effects of Exposure to Low Levels of Ionizing Radiation: Beir V; National Academies Press (US): Washington, DC, USA, 1990. [CrossRef]
- Hall, P. Radiation-associated urinary bladder cancer. Scand. J. Urol. Nephrol. Suppl. 2008, 85–88. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Male Patients | Female Patients | p Value | |
|---|---|---|---|---|
| Number of patients | 11,072 | 7412 | 3660 | |
| Age (years) | 56.5 ± 11.03 | 57.3 ± 10.4 | 54.8 ± 11.8 | <0.001 |
| <50 | 2962 (26.8%) | 1724 (23.3%) | 1238 (33.8%) | |
| ≥50 | 8110 (73.2%) | 5688 (76·7%) | 2422 (66.2%) | |
| Smoking status | <0.001 | |||
| Never | 6875 (62.1%) | 3346 (45.1%) | 3529 (96.4%) | |
| Past | 2369 (21.4%) | 2303 (31.1%) | 66 (1.8%) | |
| Current | 1828 (16.5%) | 1763 (23.8%) | 65 (1.8%) | |
| Comorbidities | ||||
| Myocardial infarction | 51 (0.5%) | 46 (0.6%) | 5 (0.1%) | <0.001 |
| Congestive heart failure | 61 (0.6%) | 51 (0.7%) | 10 (0.3%) | 0.008 |
| Peripheral vascular dis. | 72 (0.7%) | 66 (0.9%) | 6 (0.2%) | <0.001 |
| Cerebrovascular dis. | 348 (3.1%) | 258 (3.5%) | 90 (2.5%) | 0.004 |
| Dementia | 29 (0.3%) | 17 (0.2%) | 12 (0.3%) | 0.449 |
| Chronic pulmonary dis. | 362 (3.3%) | 285 (3.8%) | 77 (2.1%) | <0.001 |
| Connective tissue dis. | 32 (0.3%) | 9 (0.1%) | 23 (0.6%) | <0.001 |
| Peptic ulcer dis. | 1375 (12.4%) | 996 (13.4%) | 379 (10.4%) | <0.001 |
| Diabetes (without complications) | 643 (5.8%) | 496 (6.7%) | 147 (4.0%) | <0.001 |
| Diabetes (with complications) | 91 (0.8%) | 69 (0.9%) | 22 (0.6%) | 0.090 |
| Paraplegia/hemiplegia | 5 (0.0%) | 5 (0.1%) | 0 (0.0%) | 0.273 |
| Mild liver disease | 445 (4.0%) | 332 (4.5%) | 113 (3.1%) | 0.001 |
| Moderate or severe liver disease | 1 (0.0%) | 1 (0.0%) | 0 (0.0%) | 1.000 |
| Renal disease | 91 (0.8%) | 72 (1.0%) | 19 (0.5%) | 0.018 |
| Covariates. | Adjusted HR (95% CI) |
|---|---|
| Abdomen (with pelvis) CT scans | |
| Continuous variable | 1.09 (1.03–1.14) |
| Binary | |
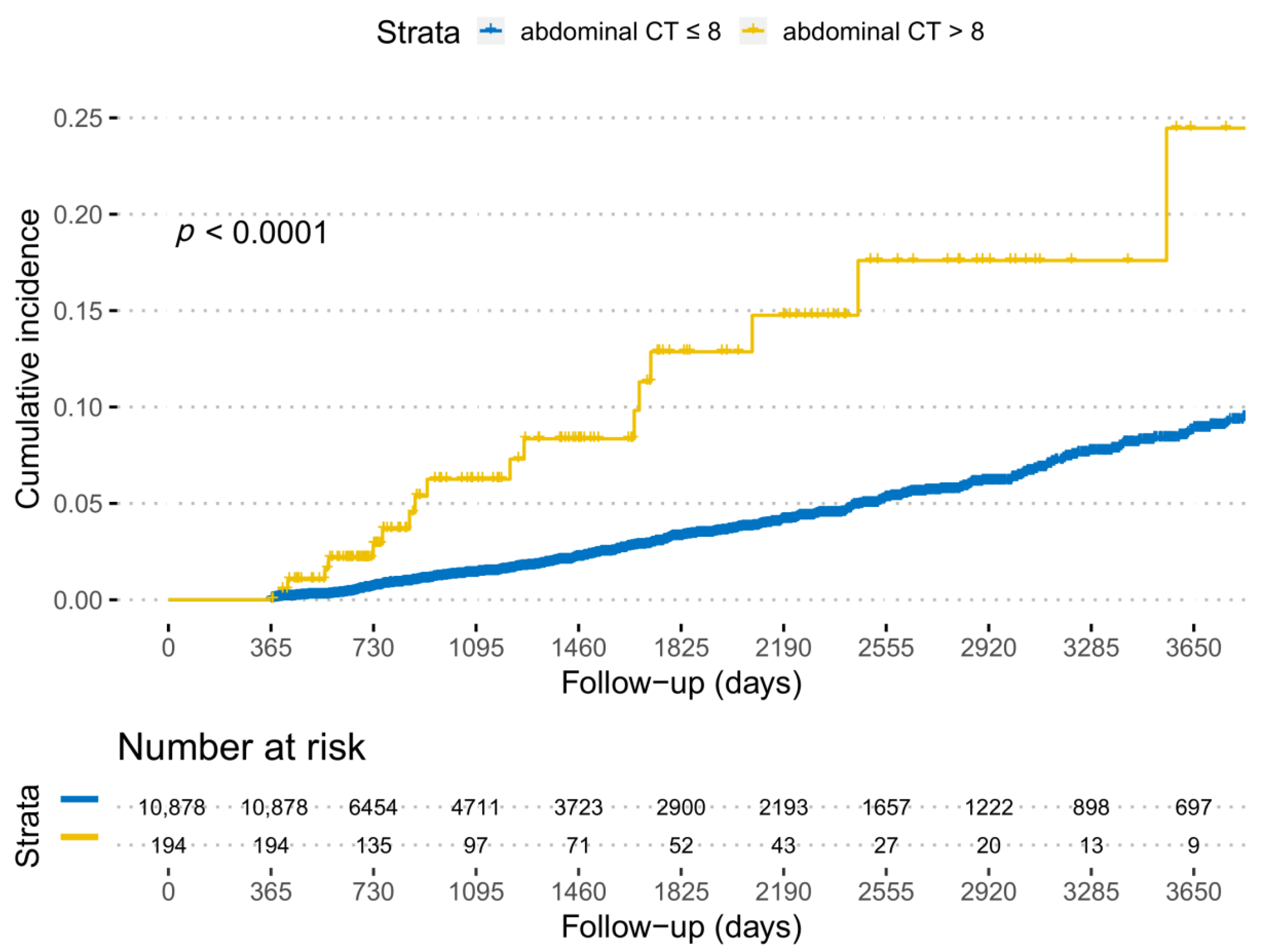
| 8 | Reference |
| 8 | 2.73 (1.66–4.50) |
| Tertile | |
| 0–6 | Reference |
| 7–8 | 1.31 (0.95–1.81) |
| 8 | 2.85 (1.72–4.71) |
| Age (continuous variable) | 1.06 (1.05–1.07) |
| <50 | Reference |
| ≥50 | 2.64 (1.87–3.73) |
| Sex | |
| Female | Reference |
| Male | 1.61 (1.17–2.21) |
| Smoking status | |
| Never | Reference |
| Past or current | 1.58 (1.23–2.03) |
| Comorbidities | |
| Myocardial infarction | 0.78 (0.18–3.39) |
| Congestive heart failure | 0.54 (0.07–3.90) |
| Peripheral vascular dis. | 0.14 (0.02–1.01) |
| Cerebrovascular dis. | 0.99 (0.58–1.69) |
| Dementia | 0.95 (0.13–7.02) |
| Chronic pulmonary dis. | 0.91 (0.54–1.54) |
| Connective tissue dis. | |
| Peptic ulcer dis. | 1.13 (0.81–1.57) |
| Diabetes (without complications) | 1.00 (0.64–1.55) |
| Diabetes (with complications) | 1.12 (0.46–2.68) |
| Paraplegia/hemiplegia | 2.33 (0.28–19.50) |
| Mild liver disease | 1.95 (1.35–2.81) |
| Moderate or severe liver disease | |
| Renal disease | 0.60 (0.15–2.45) |
| Cohort (n = 11,072) | NHIS Cohort (n = 7908) | |||||
|---|---|---|---|---|---|---|
| No. of Cases | Incidence Rate (per 1000 Person-Years) | Adjusted HR (95% CI) | No. of Cases | Incidence Rate (per 1000 Person-Years) | Adjusted HR (95% CI) | |
| Intra-abdominal SPM | 322 | 7.36 | 1.09 (1.03–1.14) | 271 | 8.82 | 1.14 (1.07–1.22) |
| Liver | 50 | 1.14 | 1.10 (1.01–1.20) | 58 | 1.89 | 1.16 (1.01–1.34) |
| Gallbladder and biliary tract | 41 | 0.94 | 0.90 (0.63–1.28) | 18 | 0.59 | 1.24 (0.97–1.58) |
| Pancreas | 33 | 0.75 | 1.28 (1.15–1.43) | 32 | 1.04 | 1.36 (1.18–1.57) |
| Small bowel | 3 | 0.07 | 1.37 (0.65–2.92) | 0 | 0 | - |
| Colon and rectum | 83 | 1.9 | 1.04 (0.92–1.17) | 53 | 1.73 | 0.87 (0.69–1.10) |
| Kidney | 10 | 0.23 | 1.29 (1.03–1.62) | 12 | 0.39 | 1.14 (0.72–1.82) |
| Bladder | 37 | 0.85 | 1.25 (1.11–1.41) | 19 | 0.62 | 1.17 (0.91–1.49) |
| Prostate | 60 | 1.37 | 1.09 (0.99–1.21) | 75 | 2.44 | 1.13 (0.99–1.29) |
| Cervix uteri | 3 | 0.07 | 1.19 (0.58–2.45) | 0 | 0 | - |
| Corpus uteri | 1 | 0.02 | 1.18 (0.34–4.11) | 0 | 0 | - |
| Ovary | 1 | 0.02 | 1.46 (0.34–6.19) | 4 | 0.13 | 1.19 (0.62–2.27) |
| Latent Period | Adjusted HR (95% CI) Continuous Variable | p Value | Adjusted HR (95% CI) 8> Versus ≤8 (Reference) | p Value |
|---|---|---|---|---|
| 1 years | 1.09 (1.03–1.14) | 0.001 | 2.73 (1.66–4.50) | <0.001 |
| 2 years | 1.09 (1.03–1.15) | 0.005 | 2.48 (1.37–4.48) | 0.003 |
| 3 years | 1.06 (0.99–1.14) | 0.105 | 2.17 (1.06–4.47) | 0.035 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.J.; Lee, Y.C.; Min, Y.W.; Lee, H.; Min, B.-H.; Lee, J.H.; Won, H.-H.; Song, K.D.; Jeong, W.K.; Kim, J.J. Risk of Second Primary Malignancies among Patients with Early Gastric Cancer Exposed to Recurrent Computed Tomography Scans. Cancers 2021, 13, 1144. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051144
Kim TJ, Lee YC, Min YW, Lee H, Min B-H, Lee JH, Won H-H, Song KD, Jeong WK, Kim JJ. Risk of Second Primary Malignancies among Patients with Early Gastric Cancer Exposed to Recurrent Computed Tomography Scans. Cancers. 2021; 13(5):1144. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051144
Chicago/Turabian StyleKim, Tae Jun, Yeong Chan Lee, Yang Won Min, Hyuk Lee, Byung-Hoon Min, Jun Haeng Lee, Hong-Hee Won, Kyoung Doo Song, Woo Kyoung Jeong, and Jae J. Kim. 2021. "Risk of Second Primary Malignancies among Patients with Early Gastric Cancer Exposed to Recurrent Computed Tomography Scans" Cancers 13, no. 5: 1144. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13051144