
Patient-Specific Planning for Thermal Magnetic Resonance of Glioblastoma Multiforme

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Voxel Models
2.2. Radiofrequency Applicators and Electromagnetic Field Simulations
- (i)
- The number of independent transmit channels was increased from 8 to 16 to 32. In the denomination of the RF applicators, this is represented at the first position: 8.*/16.*/32.*.
- (ii)
- For the eight and 16 element arrays, the coverage in the cranial–caudal direction was increased in three steps and was encoded in the second position of the RF applicator denomination. Starting in a planar arrangement (*.P.*), first every second element was displaced by half the length of the dipole to obtain an interleaved arrangement (*.I.*), followed by shifting them by the full length of the RF antenna building block to form a two-row arrangement (*.2R.*).
- (iii)
- For every RF applicator configuration of (i) and (ii), the influence of arranging the dipole building blocks in a ring (*.*.R; d = 240 mm) around the head versus an elliptical arrangement with the same circumference but better conformity to the human head (*.*.E; a1 = 220 mm, a2 = 260 mm) was investigated.
- (iv)
- Adding a water bolus between the RF applicator and the patient’s body increases RF coupling and can serve to adjust/decrease the surface temperature [50]. The presence of a water bolus (*.WB) was tested for its influence on the treatment planning outcome for the interleaved arrays 16.I.*.WB.
2.3. Hyperthermia Treatment Planning
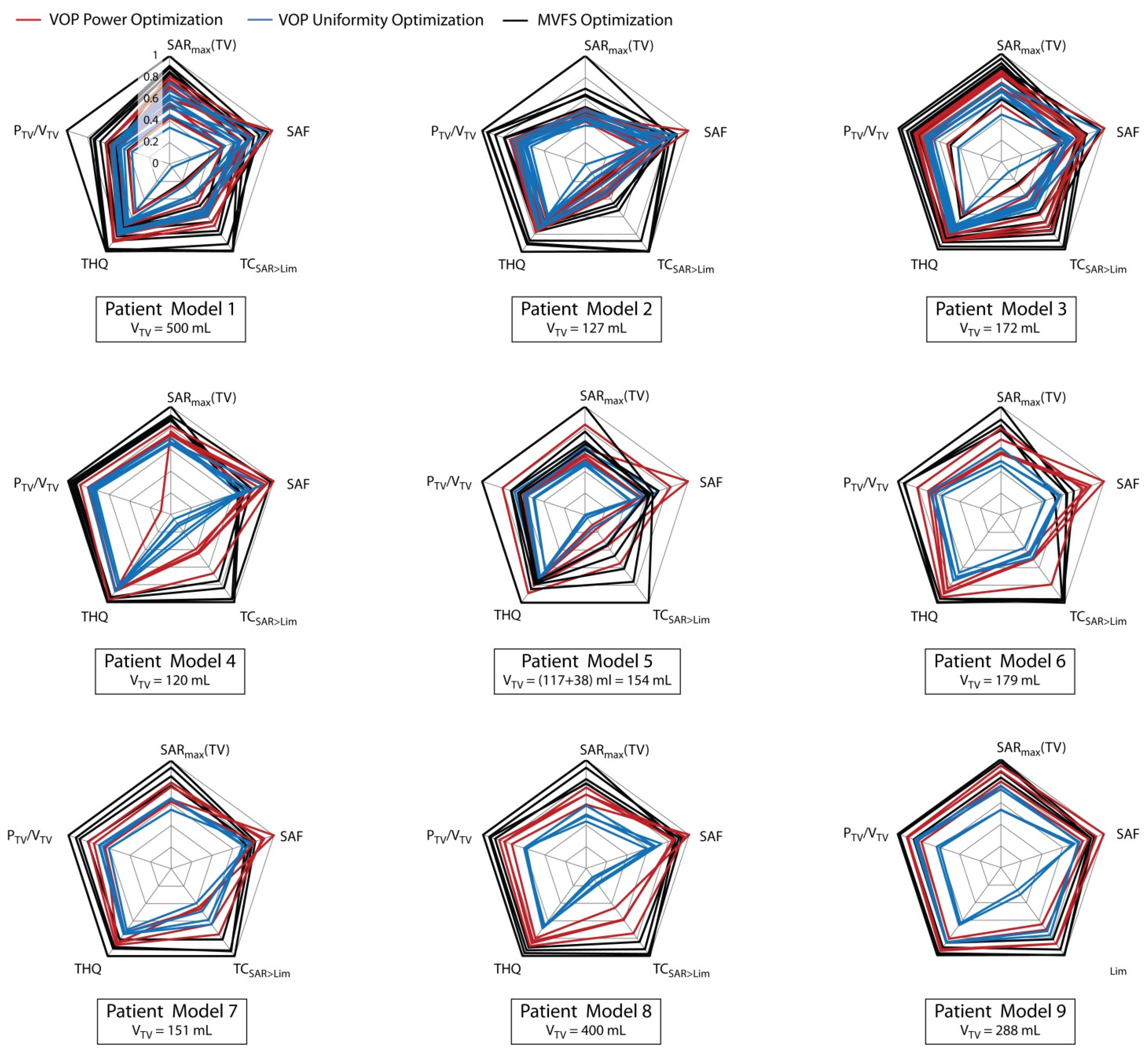
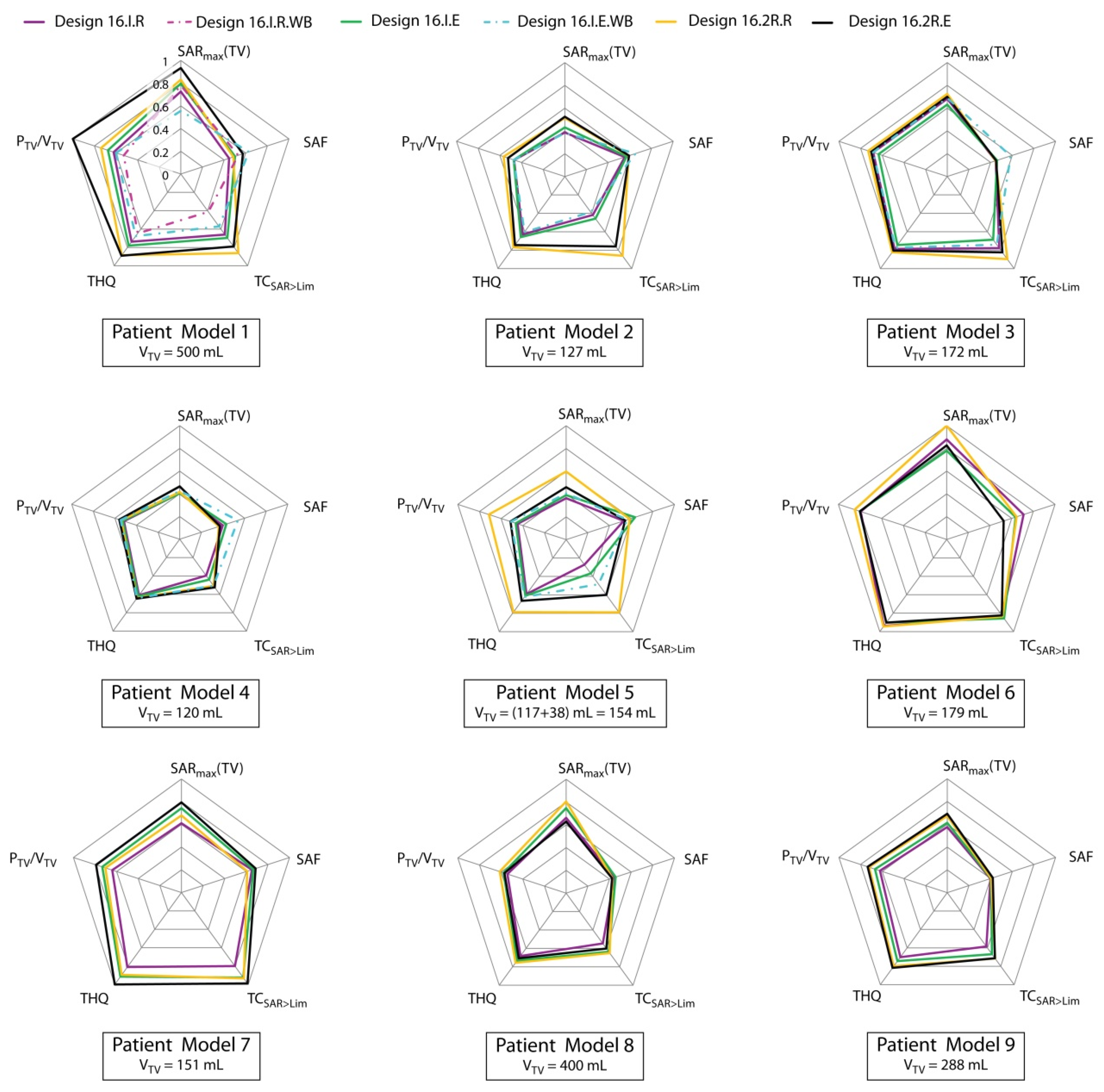
2.4. Performance Analysis
- The maximum SAR10g value reached in the TV SAR10g,max(TV) assesses the absolute RF exposure level.
- The SAR amplification factor (SAF) [33] helps to quantify the sparing of the healthy surrounding tissue by referring the average power deposition in the TV to the average power absorption in the healthy tissue. However, SAF lacks information about the absolute SAR values reached. The SAF concept was introduced to specifically assess the feasibility of RF focusing on a small (ø 3 cm) target in the brain [33]. Furthermore, it lends itself to exploratory comparisons of different arrays because its global optimum can be straightforwardly computed. The best computationally possible SAF (ultimate SAF) achieved by optimal superposition of the E-fields emitted by a cluster of hundreds of dipoles arranged equidistantly around the head serves as a benchmark for HTP results. For deep seated targets, the best SAF reported at 298 MHz was 8.4. Please note that the SAF metric normalizes to the remaining healthy tissue as a whole without enforcing a limit on the local exposure. It is thus to be expected that this value cannot be reproduced for larger TVs, where the ratio between TV and healthy tissue is increased. It is calculated as SAF = SAR10g,mean(TV)/SAR10g,mean(healthy).
- The relative target coverage where the power deposition exposure level exceeds the limit set for the healthy tissue TCSAR>Lim is a measure of the RF energy distribution within the TV. Since this in an investigative metric to judge our HTP outcome, no minimum requirement can be formulated yet. It is quantified as TCSAR>Lim = VTV(SAR > SARlim)/VTV.
- The target-to-hotspot quotient THQ [61] assesses local RF power deposition maxima in healthy tissue by correlating the average power deposition in the TV to the first volumetric percentile of local SAR10g exposure in healthy tissue. We were the first to report a THQ > 1 in HTP of brain tumors [16,62]. THQ is calculated as THQ = SAR10g,mean(TV)/P1,mean(SAR10g(healthy)).
- The volumetric power density in the TV PTV/VTV as a relative measure ensures the comparability of the results between different TVs and might help to differentiate TVs with a good treatment perspective from others. It relates the total power deposited in the TV PTV to its volume VTV. This metric is particularly important, since the deposited power PTV is driving the RF heating in the TV. Relating it to VTV makes it comparable between patient models. For an approximated average tissue density of 1 g/cm³, this metric corresponds to the mean SAR in the TV. We hope that a PTV/VTV > 30 W/L is the minimum we can achieve.
3. Results
3.1. Optimization Algorithm Comparison
3.2. RF Applicator Comparison: Number of Transmit Channels
3.3. Hyperthermia Treatment Planning
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Model | Organ | Assigned Tissue | Electric Conductivity σ (S/m) | Relative Permittivity εr |
|---|---|---|---|---|
| All | Brain | 40% WM + 60% GM | 0.52 | 50.3 |
| Brainstem | 40% WM + 60% GM | 0.52 | 50.3 | |
| Eye | Vitreous humor | 1.52 | 69 | |
| Optical nerve | Nerve | 0.42 | 37 | |
| Chiasm * | White matter | 0.42 | 43.8 | |
| Spinal cord | Nerve | 0.42 | 37 | |
| Ventricles | CSF | 2.22 | 72.8 | |
| External CSF | CSF | 2.22 | 72.8 | |
| Fat | Fat | 0.07 | 11.7 | |
| Muscle | Muscle | 0.77 | 58.2 | |
| Skull | Bone | 0.08 | 13.5 | |
| Cavities * | Lung (inflated) | 0.36 | 24.8 | |
| Pat Model 1 | Tumor growth | Tumor | 1.15 | 66.5 |
| Vessels | Blood | 1.32 | 65.7 | |
| Pituitary gland | Hypothalamus | 0.69 | 60.1 | |
| Hypothalamus | Hypothalamus | 0.69 | 60.1 | |
| Chiasm * | Nerve | 0.42 | 37 | |
| Cavities * | Air | 0 | 1 | |
| Pat Model 2 | Resection cavity | Blood | 1.32 | 65.7 |
| Body ** | 50% Muscle + 50% Fat | 0.42 | 35 | |
| Hypothalamus | Hypothalamus | 0.69 | 60.1 | |
| Blood vessels | Blood | 1.32 | 65.7 | |
| Pat Model 3 | Tumor growth (solid) | Tumor | 1.15 | 66.5 |
| Tumor growth (non-solid) | Tumor | 1.15 | 66.5 | |
| Body | 50% Muscle + 50% Fat | 0.54 | 42.7 | |
| Hypothalamus | Hypothalamus | 0.69 | 60.1 | |
| Blood vessels | Blood | 1.32 | 65.7 | |
| Pat Model 4 | Tumor growth | Tumor | 1.15 | 66.5 |
| Trepanation | Skin | 0.64 | 49.9 | |
| Hypophysis | Hypophysis | 0.85 | 62.5 | |
| Inner ear | 60% Cartilage + 30% bone + 5% cavity + 5% muscle | 0.45 | 39.2 | |
| Pat Model 5 | Tumor growth | Tumor | 1.15 | 66.5 |
| Inner ear | 60% Cartilage + 30% bone + 5% cavity + 5% muscle | 0.45 | 39.2 | |
| Hippocampus | Hippocampus | 0.69 | 60.1 | |
| Lacrimalis | Thyroid Gland | 0.85 | 62.9 | |
| Cerebellum | 40% WM + 60% GM | 0.52 | 50.3 | |
| Pat Model 6 | Resection cavity | Blood | 1.32 | 65.7 |
| Inner ear | 60% Cartilage + 30% bone + 5% cavity + 5% muscle | 0.45 | 39.2 | |
| Pat Model 7 | Tumor growth | Tumor | 1.15 | 66.5 |
| Inner ear | 60% Cartilage + 30% bone + 5% cavity + 5% muscle | 0.45 | 39.2 | |
| Hypophysis | Hypophysis | 0.85 | 62.5 | |
| Pat Model 8 | Tumor growth | Tumor | 1.15 | 66.5 |
| Pituitary gland | Hypophysis | 0.85 | 62.5 | |
| Inner ear | 60% Cartilage + 30% bone + 5% cavity + 5% muscle | 0.45 | 39.2 | |
| Pat Model 9 | Tumor growth | Tumor | 1.15 | 66.5 |
| Inner ear | 60% Cartilage + 30% bone + 5% cavity + 5% muscle | 0.45 | 39.2 |
References
- Sneed, P.K.; Stauffer, P.R.; McDermott, M.W.; Diederich, C.J.; Lamborn, K.R.; Prados, M.D.; Chang, S.; Weaver, K.A.; Spry, L.; Malec, M.K. Survival Benefit of Hyperthermia in a Prospective Randomized Trial of Brachytherapy Boost ± Hyperthermia for Glioblastoma Multiforme. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 287–295. [Google Scholar] [CrossRef]
- Wust, P.; Hildebrandt, B.; Sreenivasa, G.; Rau, B.; Gellermann, J.; Riess, H.; Felix, R.; Schlag, P.M. Hyperthermia in Combined Treatment of Cancer. Lancet Oncol. 2002, 3, 487–497. [Google Scholar] [CrossRef]
- Horsman, M.R.; Jens, O. Hyperthermia: A Potent Enhancer of Radiotherapy. Clin. Oncol. 2007, 19, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Issels, R.D.; Lindner, L.H.; Verweij, J.; Wust, P.; Reichardt, P.; Schem, B.C.; Abdel-Rahman, S.; Daugaard, S.; Salat, C.; Wendtner, C.M. Neo-Adjuvant Chemotherapy Alone or with Regional Hyperthermia for Localised High-Risk Soft-Tissue Sarcoma: A Randomised Phase 3 Multicentre Study. Lancet Oncol. 2010, 11, 561–570. [Google Scholar] [CrossRef] [Green Version]
- Titsworth, W.L.; Murad, G.J.A.; Hoh, B.L.; Rahman, M. Fighting Fire with Fire: The Revival of Thermotherapy for Gliomas. Anticancer Res. 2014, 34, 565–574. [Google Scholar]
- Kok, H.P.; Crezee, J. A Comparison of the Heating Characteristics of Capacitive and Radiative Superficial Hyperthermia. Int. J. Hyperth. 2017, 33, 378–386. [Google Scholar] [CrossRef] [Green Version]
- Datta, N.R.; Bose, A.K.; Kapoor, H.K.; Gupta, S. Head and Neck Cancers: Results of Thermoradiotherapy Versus Radiotherapy. Int. J. Hyperth. 1990, 6, 479–486. [Google Scholar] [CrossRef]
- Paulides, M.M.; Verduijn, G.M.; Van Holthe, N. Status Quo and Directions in Deep Head and Neck Hyperthermia. Radiat. Oncol. 2016, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Coluccia, D.; Fandino, J.; Schwyzer, L.; O’Gorman, R.; Remonda, L.; Anon, J.; Martin, E. and Beat Werner. First Noninvasive Thermal Ablation of a Brain Tumor with Mr-Guided Focused ultrasound. J. Ther. Ultrasound 2014, 2, 17. [Google Scholar] [CrossRef] [Green Version]
- Maloney, E.; Hwang, J.H. Emerging Hifu Applications in Cancer Therapy. Int. J. Hyperth. 2015, 31, 302–309. [Google Scholar] [CrossRef]
- Schneider, C.S.; Woodworth, G.F.; Vujaskovic, Z.; Mishra, M.V. Radiosensitization of High-Grade Gliomas through Induced Hyperthermia: Review of Clinical Experience and the Potential Role of Mr-Guided Focused Ultrasound. Radiother. Oncol. 2020, 142, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Fiorentini, G.; Sarti, D.; Milandri, C.; Dentico, P.; Mambrini, A.; Fiorentini, C.; Mattioli, G.; Casadei, V.; Guadagni, S. Modulated Electrohyperthermia in Integrative Cancer Treatment for Relapsed Malignant Glioblastoma and Astrocytoma: Retrospective Multicenter Controlled Study. Integr. Cancer Ther. 2019, 18. [Google Scholar] [CrossRef] [Green Version]
- Kok, H.P.; Navarro, F.; Strigari, L.; Cavagnaro, M.; Crezee, J. Locoregional Hyperthermia of Deep-Seated Tumours Applied with Capacitive and Radiative Systems: A Simulation Study. Int. J. Hyperth. 2018, 34, 714–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wust, P. Thermotherapy in Oncology; UNI-MED Verlag: Bremen, Germany, 2016. [Google Scholar]
- Winter, L.; Özerdem, C.; Hoffmann, W.; Santoro, D.; Müller, A.; Waiczies, H.; Seemann, R.; Graessl, A.; Wust, P.; Niendorf, T. Design and Evaluation of a Hybrid Radiofrequency Applicator for Magnetic Resonance Imaging and Rf Induced Hyperthermia: Electromagnetic Field Simulations up to 14.0 Tesla and Proof-of-Concept at 7.0 Tesla. PLoS ONE 2013, 8, e61661. [Google Scholar] [CrossRef]
- Oberacker, E.; Kuehne, A.; Oezerdem, C.; Nadobny, J.; Weihrauch, M.; Beck, M.; Zschaeck, S.; Diesch, C.; Eigentler, T.W.; Waiczies, H. Radiofrequency Applicator Concepts for Thermal Magnetic Resonance of Brain Tumors at 297 Mhz (7.0 Tesla). Int. J. Hyperth. 2020, 37, 549–563. [Google Scholar] [CrossRef]
- Rodrigues, D.; Ellsworth, J.; Turner, P. Feasibility of Heating Brain Tumors Using a 915 Mhz Annular Phased Array. IEEE Antennas Wirel. Propag. Lett. 2021, 20, 423–427. [Google Scholar] [CrossRef]
- Takook, P.; Persson, M.; Gellermann, J.; Trefná, H.D. Compact Self-Grounded Bow-Tie Antenna Design for an Uwb Phased-Array Hyperthermia Applicator. Int. J. Hyperth. 2017, 33, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Kuehne, A.; Oberacker, E.; Waiczies, H.; Niendorf, T. Solving the Time-and Frequency-Multiplexed Problem of Constrained Radiofrequency Induced Hyperthermia. Cancers 2020, 12, 1072. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, K.; Bouras, A.; Bozec, D.; Ivkov, R.; Hadjipanayis, C. Magnetic Hyperthermia Therapy for the Treatment of Glioblastoma: A Review of the Therapy’s History, Efficacy and Application in Humans. Int. J. Hyperth. 2018, 34, 1316–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, R.; Sharma, D. Evolution of Magnetic Hyperthermia for Glioblastoma Multiforme Therapy. ACS Chem. Neurosci. 2019, 10, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- McDannold, N.; Vykhodtseva, N.; Jolesz, F.A.; Hynynen, K. Mri Investigation of the Threshold for Thermally Induced Blood–Brain Barrier Disruption and Brain Tissue Damage in the Rabbit Brain. Magn. Reson. Med. Off. J. Int. Soc. Magn. Reson. Med. 2004, 51, 913–923. [Google Scholar] [CrossRef]
- Zhang, F.; Xu, C.L.; Liu, C.M. Drug Delivery Strategies to Enhance the Permeability of the Blood-Brain Barrier for Treatment of Glioma. Drug Des. Dev. Ther. 2015, 9, 2089–2100. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Wang, C.; Wang, L.; Chen, Y. A Comprehensive Review in Improving Delivery of Small-Molecule Chemotherapeutic Agents Overcoming the Blood-Brain/Brain Tumor Barriers for Glioblastoma Treatment. Drug Deliv. 2019, 26, 551–565. [Google Scholar] [CrossRef]
- Besse, H.C.; Barten-van Rijbroek, A.D.; van der Wurff-Jacobs, K.M.G.; Bos, C.; Moonen, C.T.W.; Deckers, R. Tumor Drug Distribution after Local Drug Delivery by Hyperthermia, in vivo. Cancers 2019, 11, 1512. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Winter, L.; Navarro, L.; Ku, M.C.; Periquito, J.S.; Pham, M.; Hoffmann, W.; Theune, L.E.; Calderón, M.; Niendorf, T. Controlled Release of Therapeutics from Thermoresponsive Nanogels: A Thermal Magnetic Resonance Feasibility Study. Cancers 2020, 12, 1380. [Google Scholar] [CrossRef]
- Han, H.; Eigentler, T.W.; Wang, S.; Kretov, E.; Winter, L.; Hoffmann, W.; Grass, E.; Niendorf, T. Design, Implementation, Evaluation and Application of a 32-Channel Radio Frequency Signal Generator for Thermal Magnetic Resonance Based Anti-Cancer Treatment. Cancers 2020, 12, 1720. [Google Scholar] [CrossRef] [PubMed]
- Trefna, D.H.; Jonathan, J.; Vessman, B.; Wanemark, J.; Woxlin, E.; Hjalmarsson, A.; Adelbäck, L.; Takook, P.; Gellermann, J.; Lannering, B. Antenna Applicator for Microwave Hyperthermia Treatment of Pediatric Brain Cancer. In Proceedings of the 8th European Conference on Antennas and Propagation, EuCAP 2014, The Hague, The Netherlands, 6–11 April 2014. [Google Scholar]
- Schooneveldt, G.; Trefná, H.D.; Persson, M.; De Reijke, T.M.; Blomgren, K.; Kok, H.P.; Crezee, H. Hyperthermia Treatment Planning Including Convective Flow in Cerebrospinal Fluid for Brain Tumour Hyperthermia Treatment Using a Novel Dedicated Paediatric Brain Applicator. Cancers 2019, 11, 1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulides, M.M.; Bakker, J.F.; Neufeld, E.; van der Zee, J.; Jansen, P.P.; Levendag, P.C.; van Rhoon, G.C. The Hypercollar: A Novel Applicator for Hyperthermia in the Head and Neck. Int. J. Hyperth. 2007, 23, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Wust, P.; Seebass, M.; Nadobny, J.; Deuflhard, P.; Mönich, G.; Felix, R. Simulation Studies Promote Technological Development of Radiofrequency Phased Array Hyperthermia. Int. J. Hyperth. 1996, 12, 477–494. [Google Scholar] [CrossRef]
- Canters, R.A.M.; Paulides, M.M.; Franckena, M.; Mens, J.W.; van Rhoon, G.C. Benefit of Replacing the Sigma-60 by the Sigma-Eye Applicator. Strahlenther. Onkol. 2013, 189, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Guérin, B.; Villena, J.F.; Polimeridis, A.G.; Adalsteinsson, E.; Daniel, L.; White, J.K.; Rosen, B.R.; Wald, L.L. Computation of Ultimate Sar Amplification Factors for Radiofrequency Hyperthermia in Non-Uniform Body Models: Impact of Frequency and Tumour Location. Int. J. Hyperth. 2018, 34, 87–100. [Google Scholar] [CrossRef]
- Bellizzi, G.G.; Drizdal, T.; van Rhoon, G.C.; Crocco, L.; Isernia, T.; Paulides, M.M. The Potential of Constrained Sar Focusing for Hyperthermia Treatment Planning: Analysis for the Head & Neck Region. Phys. Med. Biol. 2018, 64, 015013. [Google Scholar] [PubMed]
- Niyazi, M.; Geisler, J.; Siefert, A.; Schwarz, S.B.; Ganswindt, U.; Garny, S.; Schnell, O.; Suchorska, B.; Kreth, F.W.; Tonn, J.C. Fet–Pet for Malignant Glioma Treatment Planning. Radiother. Oncol. 2011, 99, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Niyazi, M.; Brada, M.; Chalmers, A.J.; Combs, S.E.; Erridge, S.C.; Fiorentino, A.; Grosu, A.L.; Lagerwaard, F.J.; Minniti, G.; Mirimanoff, R.O. Estro-Acrop Guideline “Target Delineation of Glioblastomas”. Radiother. Oncol. 2016, 118, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.F. Regional Hyperthermia with an Annular Phased Array. IEEE Trans. Biomed. Eng. 1984, BME-31, 106–114. [Google Scholar] [CrossRef]
- Turner, P.F.; Schaefermeyer, T. Bsd-2000 Approach for Deep Local and Regional Hyperthermia: Clinical Utility. Strahlenther. Onkol. Organ Dtsch. Rontgenges. 1989, 165, 700–704. [Google Scholar]
- Eigentler, T.W.; Winter, L.; Han, H.; Oberacker, E.; Kuehne, A.; Waiczies, H.; Schmitter, S.; Boehmert, L.; Prinz, C.; Trefna, H.D. Wideband Self-Grounded Bow-Tie Antenna for Thermal Mr. NMR Biomed. 2020, 33, e4274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niendorf, T.; Oezerdem, C.; Ji, Y.; Oberacker, E.; Kuehne, A.; Waiczies, H.; Winter, L. Radiative Rf Antenna Arrays for Cardiac, Brain and Thermal Magnetic Resonance at Ultrahigh and Extreme Magnetic Field Strengths: Concepts, Electromagnetic Field Simulations and Applications. In Proceedings of the 2017 International Conference on Electromagnetics in Advanced Applications (ICEAA), Verona, Italy, 11−15 September 2017. [Google Scholar]
- Ji, Y.; Hoffmann, W.; Pham, M.; Dunn, A.E.; Han, H.; Özerdem, C.; Waiczies, H.; Rohloff, M.; Endemann, B.; Boyer, C. High Peak and High Average Radiofrequency Power Transmit/Receive Switch for Thermal Magnetic Resonance. Magn. Reson. Med. 2018, 80, 2246–2255. [Google Scholar] [CrossRef]
- Young, I.R.; Hand, J.W.; Oatridge, A.; Prior, M.V. Modeling and Observation of Temperature Changes in Vivo Using Mri. Magn. Reson. Med. 1994, 32, 358–369. [Google Scholar] [CrossRef]
- de Senneville, D.; Quesson, B.B.; Moonen, C.T.W. Magnetic Resonance Temperature Imaging. Int. J. Hyperth. 2005, 21, 515–531. [Google Scholar] [CrossRef] [Green Version]
- Winter, L.; Oberacker, E.; Paul, K.; Ji, Y.; Oezerdem, C.; Ghadjar, P.; Thieme, A.; Budach, V.; Wust, P.; Niendorf, T. Magnetic Resonance Thermometry: Methodology, Pitfalls and Practical Solutions. Int. J. Hyperth. 2016, 32, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Winter, L.; Niendorf, T. Electrodynamics and Radiofrequency Antenna Concepts for Human Magnetic Resonance at 23.5 t (1 ghz) and Beyond. Magn. Reson. Mater. Phys. Biol. Med. 2016, 29, 641–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadobny, J.; Weihrauch, M.; Zschaeck, S.; Lim, A.; Beck, M.; Chrzon, B.C.; Herz, E.; Wust, P.; Ghadjar, P. Fast and Efficient Generation of Patient Models for Hyperthermia Based on Radiation Therapy Contours. In Proceedings of the 32nd Annual Meeting of the European Society for Hyperthermic Oncology, Berlin, Germany, 16–19 May 2018. [Google Scholar]
- Restivo, M.C.; van den Berg, C.A.T.; van Lier, A.L.H.M.W.; Polders, D.L.; Raaijmakers, A.J.E.; Luijten, P.R.; Hoogduin, H. Local Specific Absorption Rate in Brain Tumors at 7 Tesla. Magn. Reson. Med. 2016, 75, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Camelia, G. Compilation of the Dielectric Properties of Body Tissues at Rf and Microwave Frequencies; DTIC Document: Reston, VA, USA, 1996. [Google Scholar]
- Hasgall, P.A.; Neufeld, E.; Gosselin, M.C.; Klingenbck, A.; Kuster, N.K. IT’IS Database for Thermal and Electromagnetic Parameters of Biological Tissues; Version 4.0; IT’IS: Zurich, Switzerland, 2018. [Google Scholar] [CrossRef]
- Ebrahimi-Ganjeh, M.A.; Attari, A.R. Study of Water Bolus Effect on Sar Penetration Depth and Effective Field Size for Local Hyperthermia. Prog. Electromagn. Res. 2008, 4, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Kuehne, A.; Seifert, F.; Ittermann, B. Gpu-Accelerated Sar Computation with Arbitrary Averaging Shapes. In Proceedings of the 20th ISMRM Annual Meeting and Exhibition, Melbourne, Australia, 5–11 May 2012. [Google Scholar]
- IEEE. Recommended Practice for Determining the Spatial-Peak Specific Absorption Rate (Sar) in the Human Body Due to Wireless Communications Devices: Measurement Techniques; IEEE: Washington, DC, USA, 2003. [Google Scholar]
- Caputa, K.; Okoniewski, M.; Stuchly, M.A. An Algorithm for Computations of the Power Deposition in Human Tissue. IEEE Antennas Propag. Mag. 1999, 41, 102–107. [Google Scholar] [CrossRef]
- Kuehne, A.; Goluch, S.; Waxmann, P.; Seifert, F.; Ittermann, B.; Moser, E.; Laistler, E. Power Balance and Loss Mechanism Analysis in Rf Transmit Coil Arrays. Magn. Reson. Med. 2015, 74, 1165–1176. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, P.R. The Relationship of Temperature Rise to Specific Absorption Rate and Current in the Human Leg for Exposure to Electromagnetic Radiation in the High Frequency Band. Phys. Med. Biol. 2003, 48, 3143–3155. [Google Scholar] [CrossRef] [PubMed]
- Hirata, A.; Shirai, K.; Fujiwara, O. On Averaging Mass of Sar Correlating with Temperature Elevation Due to a Dipole Antenna. Prog. Electromagn. Res. 2008, 84, 221–237. [Google Scholar] [CrossRef] [Green Version]
- Morimoto, R.; Laakso, I.; De Santis, V.; Hirata, A. Relationship between Peak Spatial-Averaged Specific Absorption Rate and Peak Temperature Elevation in Human Head in Frequency Range of 1–30 Ghz. Phys. Med. Biol. 2016, 61, 5406–5425. [Google Scholar] [CrossRef] [PubMed]
- Razmadze, A.; Shoshiashvili, L.; Kakulia, D.; Zaridze, R.; Bit-Babik, G.; Faraone, A. Influence of Specific Absorption Rate Averaging Schemes on Correlation between Mass-Averaged Specific Absorption Rate and Temperature Rise. Electromagnetics 2009, 29, 77–90. [Google Scholar] [CrossRef]
- Eichfelder, G.; Gebhardt, M. Local Specific Absorption Rate Control for Parallel Transmission by Virtual Observation Points. Magn Reson Med. 2011, 66, 1468–1476. [Google Scholar] [CrossRef]
- Oberacker, E.; Kuehne, A.; Nadobny, J.; Zschaeck, S.; Weihrauch, M.; Waiczies, H.; Ghadjar, P.; Wust, P.; Niendorf, T.; Winter, L. Radiofrequency Applicator Concepts for Simultaneous Mr Imaging and Hyperthermia Treatment of Glioblastoma Multiforme. Curr. Dir. Biomed. Eng. 2017, 3, 473–477. [Google Scholar] [CrossRef] [Green Version]
- Canters, R.A.M.; Wust, P.; Bakker, J.F.; Van Rhoon, G.C. A Literature Survey on Indicators for Characterisation and Optimisation of Sar Distributions in Deep Hyperthermia, a Plea for Standardisation. Int. J. Hyperth. 2009, 25, 593–608. [Google Scholar] [CrossRef]
- Takook, P. Optimising Microwave Hyperthermia Antenna Systems; Chalmers University of Technology: Gothenburg, Sweden, 2018. [Google Scholar]
- Lee, H.K.; Antell, A.G.; Perez, C.A.; Straube, W.L.; Ramachandran, G.; Myerson, R.J.; Emami, B.; Molmenti, E.P.; Buckner, A.; Lockett, M.A. Superficial Hyperthermia and Irradiation for Recurrent Breast Carcinoma of the Chest Wall: Prognostic Factors in 196 Tumors. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 365–375. [Google Scholar] [CrossRef]
- Bellizzi, G.G.; Drizdal, T.; van Rhoon, G.C.; Crocco, L.; Isernia, T.; Paulides, M.M. Predictive Value of Sar Based Quality Indicators for Head and Neck Hyperthermia Treatment Quality. Int. J. Hyperth. 2019, 36, 456–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberacker, E.; Kuehne, A.; Diesch, C.; Eigentler, T.W.; Nadobny, J.; Ghadjar, P.; Wust, P.; Niendorf, T. Rf Power Deposition Optimization Algorithms for Thermal Mr Targeting Human Brain Tumors. In Proceedings of the ISMRM & SMRT Virtual Conference & Exhibition, 8–14 August 2020. [Google Scholar]
- Canters, R.A.M.; Franckena, M.; van der Zee, J.; Van Rhoon, G.C. Complaint-Adaptive Power Density Optimization as a Tool for Htp-Guided Steering in Deep Hyperthermia Treatment of Pelvic Tumors. Phys. Med. Biol. 2008, 53, 6799. [Google Scholar] [CrossRef] [PubMed]
- Paulides, M.M.; Bakker, J.F.; Linthorst, M.; Van der Zee, J.; Rijnen, Z.; Neufeld, E.; Pattynama, P.M.T.; Jansen, P.P.; Levendag, P.C.; Van Rhoon, G.C. The Clinical Feasibility of Deep Hyperthermia Treatment in the Head and Neck: New Challenges for Positioning and Temperature Measurement. Phys. Med. Biol. 2010, 55, 2465. [Google Scholar] [CrossRef] [Green Version]
- Kok, H.P.; Korshuize- van Straten, L.; Bakker, A.; Oldenhof, R.K.; Geijsen, E.D.; Stalpers, L.J.A.; Crezee, J. Online Adaptive Hyperthermia Treatment Planning During Locoregional Heating to Suppress Treatment-Limiting Hot Spots. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 1039–1047. [Google Scholar] [CrossRef]
- Dubin, A.E.; Patapoutian, A. Nociceptors: The Sensors of the Pain Pathway. J. Clin. Investig. 2010, 120, 3760–3772. [Google Scholar] [CrossRef] [Green Version]
- Zanoli, M.; Trefná, H.D. Optimization of Microwave Hyperthermia Array Applicators Using Field Interpolation. In Proceedings of the 2019 IEEE International Symposium on Antennas and Propagation and USNC-URSI Radio Science Meeting, Atlanta, GA, USA, 7–12 July 2019. [Google Scholar]
- Vidal, A.A.V. Systematic Product Development of an Anthropomorphic Head Phantom for Ultrahigh Field Magnetic Resonance Induced Hyperthermia Designed for Brain Tumor Therapy; Technische Universität Berlin: Berlin, Germany, 2018. [Google Scholar]
- Oberacker, H.H.E.; Kuehne, A.; Wang, S.; Eigentler, T.W.; Grass, E.; Niendorf, T. Multi-Channel Rf Supervision Module for Thermal Magnetic Resonance Based Cancer Therapy. Cancers 2021, 13, 1001. [Google Scholar]







| Patient Model | Metric | Highest Value | Design | Algorithm | Number of Excitations |
|---|---|---|---|---|---|
| Pat Model 1 (V = 500 mL) | SAR10g,max (W/kg) | 134.2 | 16.2R.E | MVFS optimization | 2 |
| SAF | 3.8 | 16.I.E.WB | VOP power optimization | 1 | |
| TCSAR>Lim (%) | 83.5 | 16.2R.R | MVFS optimization | 2 | |
| THQ | 1.5 | 16.2R.E = 32.2R.E | MVFS optimization | 2/3 | |
| PTV/VTV (W/L) | 66.8 | 16.2R.E | MVFS optimization | 2 | |
| Pat Model 2 (V = 127 mL) | SAR10g,max (W/kg) | 117.5 | 32.2R.E | MVFS optimization | 2 |
| SAF | 4.3 | 16.I.E.WB | VOP power optimization | 1 | |
| TCSAR>Lim (%) | 84 | 32.2R.R | MVFS optimization | 2 | |
| THQ | 1.4 | 32.2R.E | MVFS optimization | 2 | |
| PTV/VTV (W/L) | 40 | 32.2R.E | MVFS optimization | 2 | |
| Pat Model 3 (V = 172 mL) | SAR10g,max (W/kg) | 114.4 | 32.2R.R | MVFS optimization | 2 |
| SAF | 3.5 | 16.I.E.WB | VOP power optimization | 1 | |
| TCSAR>Lim (%) | 96.9 | 32.2R.R | MVFS optimization | 2 | |
| THQ | 1.5 | 32.2R.R | MVFS optimization | 2 | |
| PTV/VTV (W/L) | 53.1 | 32.2R.R | MVFS optimization | 2 | |
| Pat Model 4 (V = 120 mL) | SAR10g,max (W/kg) | 66.9 | 16.2R.E | MVFS optimization | 2 |
| SAF | 3.2 | 16.I.E.WB | VOP power optimization | 1 | |
| TCSAR>Lim (%) | 50.8 | 16.2R.E | MVFS optimization | 2 | |
| THQ | 1.1 | 16.2R.E | MVFS optimization | 2 | |
| PTV/VTV (W/L) | 37.4 | 16.2R.E | MVFS optimization | 2 | |
| Pat Model 5 (V = 117 + 38 mL) | SAR10g,max (W/kg) | 86.1 | 16.2R.R | MVFS optimization | 3 |
| SAF | 5.2 | 16.I.E.WB | VOP power optimization | 1 | |
| TCSAR>Lim (%) | 76.5 | 16.2R.R | MVFS optimization | 3 | |
| THQ | 1.3 | 16.2R.R | MVFS optimization | 3 | |
| PTV/VTV (W/L) | 47.7 | 16.2R.R | MVFS optimization | 3 | |
| Pat Model 6 (V = 179 mL) | SAR10g,max (W/kg) | 143.9 | 16.2R.R | MVFS optimization | 2 |
| SAF | 5.8 | 16.2R.R | VOP power optimization | 1 | |
| TCSAR>Lim (%) | 83.1 | 16.I.E | MVFS optimization | 2 | |
| THQ | 1.6 | 16.2R.R | MVFS optimization | 2 | |
| PTV/VTV (W/L) | 56.8 | 16.2R.R | MVFS optimization | 2 | |
| Pat Model 7 (V = 151 mL) | SAR10g,max (W/kg) | 114.3 | 16.2R.E | MVFS optimization | 2 |
| SAF | 4.9 | 16.2R.E | VOP power optimization | 1 | |
| TCSAR>Lim (%) | 95.8 | 16.2R.E | MVFS optimization | 2 | |
| THQ | 1.6 | 16.2R.E | MVFS optimization | 2 | |
| PTV/VTV (W/L) | 52.8 | 16.2R.E | MVFS optimization | 2 | |
| Pat Model 8 (V = 400 mL) | SAR10g,max (W/kg) | 115.8 | 16.2R.R | MVFS optimization | 2 |
| SAF | 2.9 | 16.I.R | VOP power optimization | 2 | |
| TCSAR>Lim (%) | 63.1 | 16.2R.R | MVFS optimization | 2 | |
| THQ | 1.2 | 16.2R.R | MVFS optimization | 2 | |
| PTV/VTV (W/L) | 41 | 16.2R.R | MVFS optimization | 2 | |
| Pat Model 9 (V = 288 mL) | SAR10g,max (W/kg) | 99.7 | 16.2R.E | MVFS optimization | 3 |
| SAF | 2.7 | 16.2R.E | VOP power optimization | 3 | |
| TCSAR>Lim (%) | 69.3 | 16.2R.R | MVFS optimization | 3 | |
| THQ | 1.3 | 16.2R.E | MVFS optimization | 3 | |
| PTV/VTV (W/L) | 49.1 | 16.2R.E | MVFS optimization | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oberacker, E.; Diesch, C.; Nadobny, J.; Kuehne, A.; Wust, P.; Ghadjar, P.; Niendorf, T. Patient-Specific Planning for Thermal Magnetic Resonance of Glioblastoma Multiforme. Cancers 2021, 13, 1867. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13081867
Oberacker E, Diesch C, Nadobny J, Kuehne A, Wust P, Ghadjar P, Niendorf T. Patient-Specific Planning for Thermal Magnetic Resonance of Glioblastoma Multiforme. Cancers. 2021; 13(8):1867. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13081867
Chicago/Turabian StyleOberacker, Eva, Cecilia Diesch, Jacek Nadobny, Andre Kuehne, Peter Wust, Pirus Ghadjar, and Thoralf Niendorf. 2021. "Patient-Specific Planning for Thermal Magnetic Resonance of Glioblastoma Multiforme" Cancers 13, no. 8: 1867. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13081867