
Elevated Serotonin and NT-proBNP Levels Predict and Detect Carcinoid Heart Disease in a Large Validation Study

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample Size
2.3. Patient Selection
2.4. Echocardiography
2.5. Blood Sampling
2.6. Enzyme Immunoassays
2.7. Statistical Analysis
3. Results
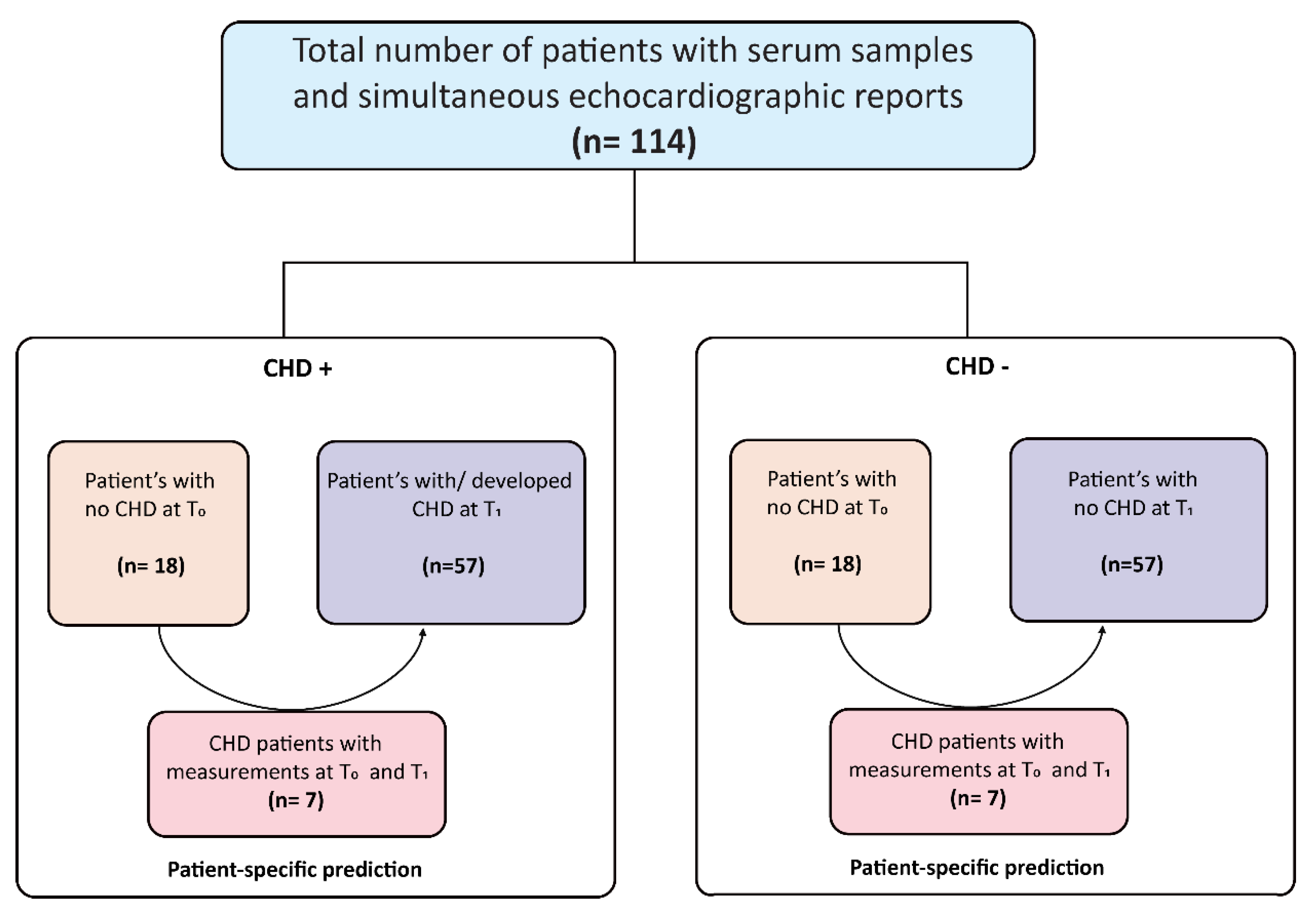
3.1. Patients
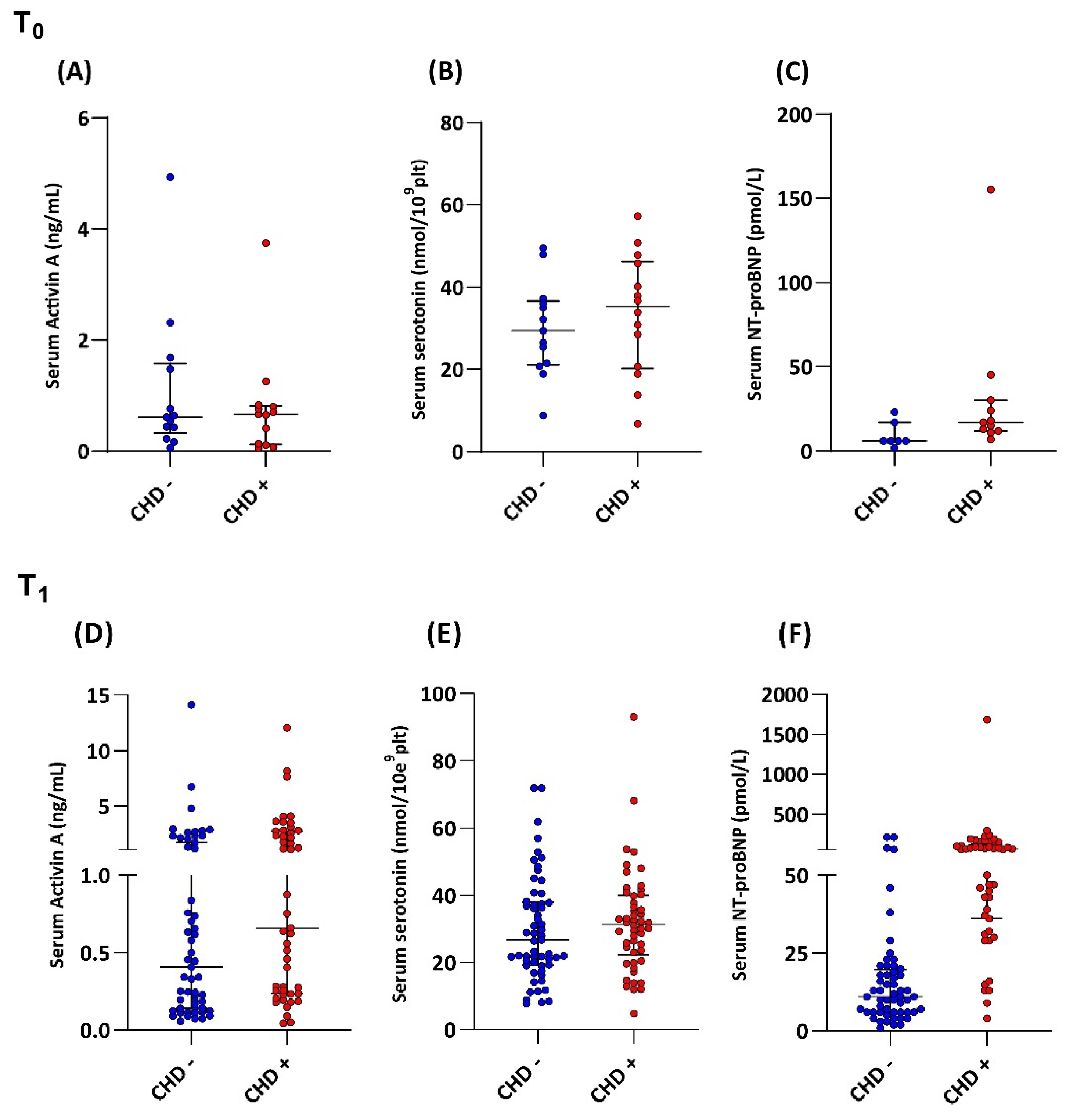
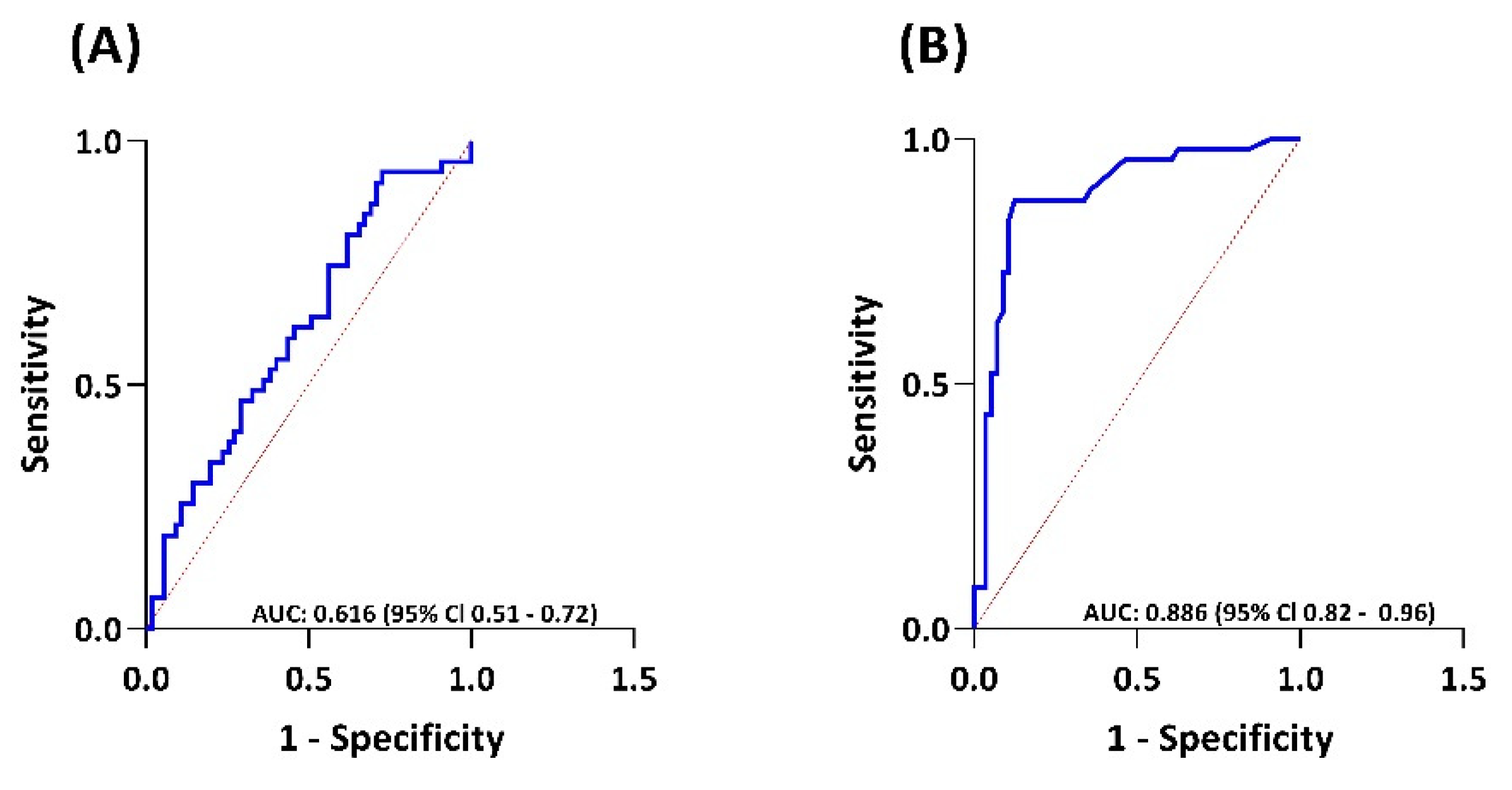
3.2. Biomarkers in the Prediction of Carcinoid Heart Disease
3.3. Biomarkers in the Detection of Carcinoid Heart Disease
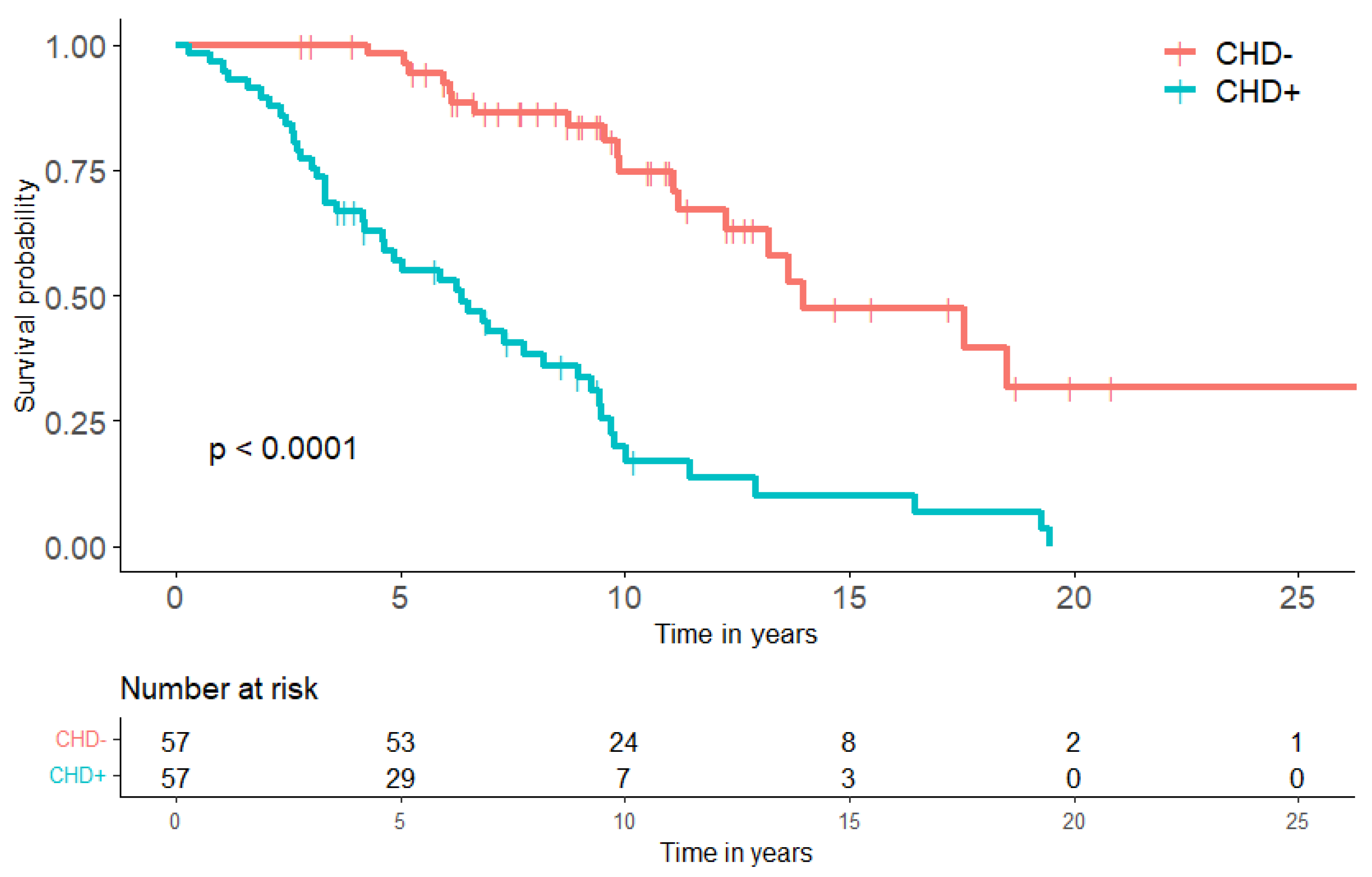
3.4. Follow Up and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Dasari, A. Epidemiology, Incidence, and Prevalence of Neuroendocrine Neoplasms: Are There Global Differences? Curr. Oncol. Rep. 2021, 23, 43. [Google Scholar] [CrossRef] [PubMed]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef] [PubMed]
- Korse, T.; Taal, B.; van Velthuysen, M.; Visser, O. Incidence and survival of neuroendocrine tumours in the Netherlands according to histological grade: Experience of two decades of cancer registry. Eur. J. Cancer 2013, 49, 1975–1983. [Google Scholar] [CrossRef] [PubMed]
- Mota, J.M.; Sousa, L.G.; Riechelmann, R.P. Complications from carcinoid syndrome: Review of the current evidence. Ecancermedicalscience 2016, 10, 662. [Google Scholar] [CrossRef] [Green Version]
- Pellikka, P.A.; Tajik, J.; Khanderia, B.K.; Seward, J.B.; Callahan, J.A.; Pitot, H.C.; Kvols, L.K. Carcinoid Heart Disease: Clinical and Echocardiographic Spectrum in 74 Patients. Circulation 1993, 87, 1188–1196. [Google Scholar] [CrossRef] [Green Version]
- Laskaratos, F.M.; Rombouts, K.; Caplin, M.; Toumpanakis, C.; Thirlwell, C.; Mandair, D. Neuroendocrine tumors and fibrosis: An unsolved mystery? Cancer 2017, 123, 4770–4790. [Google Scholar] [CrossRef] [Green Version]
- Hassan, S. Carcinoid heart disease. Heart 2017, 103, 1488–1495. [Google Scholar] [CrossRef]
- Oleinikov, K.; Avniel-Polak, S.; Gross, D.J.; Grozinsky-Glasberg, S. Carcinoid Syndrome: Updates and Review of Current Therapy. Curr. Treat. Options Oncol. 2019, 20, 70. [Google Scholar] [CrossRef]
- Grozinsky-Glasberg, S.; Grossman, A.B.; Gross, D.J. Carcinoid Heart Disease: From Pathophysiology to Treatment—‘Something in the Way It Moves’. Neuroendocrinology 2015, 101, 263–273. [Google Scholar] [CrossRef]
- Uema, D.; Alves, C.; Mesquita, M.; Nunez, J.E.; Siepmann, T.; Angel, M.; Rego, J.F.M.; Weschenfelder, R.; Rocha Filho, D.R.; Costa, F.P.; et al. Carcinoid Heart Disease and Decreased Overall Survival among Patients with Neuroendocrine Tumors: A Retrospective Multicenter Latin American Cohort Study. J. Clin. Med. 2019, 8, 405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westberg, G.; Wangberg, B.; Ahlman, H.; Bergh, C.H.; Beckman-Suurkula, M.; Caidahl, K. Prediction of prognosis by echocardiography in patients with midgut carcinoid syndrome. Br. J. Surg. 2001, 88, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Laskaratos, F.M.; Diamantopoulos, L.; Walker, M.; Walton, H.; Khalifa, M.; El-Khouly, F.; Koffas, A.; Demetriou, G.; Caplin, M.; Toumpanakis, C.; et al. Prognostic Factors for Survival among Patients with Small Bowel Neuroendocrine Tumours Associated with Mesenteric Desmoplasia. Neuroendocrinology 2018, 106, 366–380. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Raja, S.G.; Toumpanakis, C.; Caplin, M.E.; Dreyfus, G.D.; Davar, J. Outcomes, risks and complications of cardiac surgery for carcinoid heart disease. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2011, 40, 168–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niederle, B.; Pape, U. ENETS Consensus Guidelines Update for Neuroendocrine Neoplasms of the Jejunum and Ileum. Neuroendocrinology 2016, 103, 125–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutcheson, J.D.; Setola, V.; Roth, B.L.; Merryman, W.D. Serotonin receptors and heart valve disease—It was meant 2B. Pharmacol. Ther. 2011, 132, 146–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musunuru, S.; Carpenter, J.E.; Sippel, R.S.; Kunnimalaiyaan, M.; Chen, H. A mouse model of carcinoid syndrome and heart disease. J. Surg. Res. 2005, 126, 102–105. [Google Scholar] [CrossRef]
- Bergestuen, D.S.; Edvardsen, T.; Aakhus, S.; Ueland, T.; Oie, E.; Vatn, M.; Aukrust, P.; Thiis-Evensen, E. Activin A in carcinoid heart disease: A possible role in diagnosis and pathogenesis. Neuroendocrinology 2010, 92, 168–177. [Google Scholar] [CrossRef]
- Bergestuen, D.S.; Gravning, J.; Haugaa, K.H.; Sahakyan, L.G.; Aakhus, S.; Thiis-Evensen, E.; Oie, E.; Aukrust, P.; Attramadal, H.; Edvardsen, T. Plasma CCN2/connective tissue growth factor is associated with right ventricular dysfunction in patients with neuroendocrine tumors. BMC Cancer 2010, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Lichtenauer, M.; Pichler, T.; Eder, S.; Mirna, M.; Magnes, T.; Wernly, B.; Paar, V.; Jung, C.; Prinz, E.; Seitelberger, R.; et al. Carcinoid heart disease involving the left heart: A case report and biomarker analysis. ESC Heart Fail 2019, 6, 222–227. [Google Scholar] [CrossRef]
- Hofland, J.; Lamarca, A.; Steeds, R.; Toumpanakis, C.; Srirajaskanthan, R.; Riechelmann, R.; Panzuto, F.; Frilling, A.; Denecke, T.; Christ, E.; et al. Synoptic reporting of echocardiography in carcinoid heart disease (ENETS Carcinoid Heart Disease Task Force). J. Neuroendocrinol. 2021, 34, e13060. [Google Scholar] [CrossRef] [PubMed]
- Nederlandse Vereniging voor Cardiologie, Werkgroep Echocardiografie. Echocardiografie Laboratorium, Richtlijn voor de Praktijk; Nederlandse Vereniging voor Cardiologie: Utrecht, The Netherlands, 2018. [Google Scholar]
- Korse, C.M.; Buning-Kager, J.C.G.M.; Linders, T.C.; Heijboer, A.C.; van den Broek, D.; Tesselaar, M.E.T.; van Tellingen, O.; van Rossum, H.H. A serum and platelet-rich plasma serotonin assay using liquid chromatography tandem mass spectrometry for monitoring of neuroendocrine tumor patients. Clin. Chim. Acta 2017, 469, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Korse, C.M.; Taal, B.G.; de Groot, C.A.; Bakker, R.H.; Bonfrer, J.M. Chromogranin-A and N-terminal pro-brain natriuretic peptide: An excellent pair of biomarkers for diagnostics in patients with neuroendocrine tumor. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 4293–4299. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L.; van Kimmenade, R.; Lainchbury, J.; Bayes-Genis, A.; Ordonez-Llanos, J.; Santalo-Bel, M.; Pinto, Y.M.; Richards, M. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: An international pooled analysis of 1256 patients: The International Collaborative of NT-proBNP Study. Eur. Heart J. 2006, 27, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Van Rossum, A.P.; Vlasveld, L.T.; Boesten, L.S.M. De diagnostische waarde van NT-proBNP bij hartfalen. Ned. Tijdschr. Voor Geneeskd. 2011, 155, A2885. [Google Scholar]
- Jin, C.; Sharma, A.N.; Thevakumar, B.; Majid, M.; Al Chalaby, S.; Takahashi, N.; Tanious, A.; Arockiam, A.D.; Beri, N.; Amsterdam, E.A. Carcinoid Heart Disease: Pathophysiology, Pathology, Clinical Manifestations, and Management. Cardiology 2021, 146, 65–73. [Google Scholar] [CrossRef]
- Dobson, R.; Burgess, M.I.; Banks, M.; Pritchard, D.M.; Vora, J.; Valle, J.W.; Wong, C.; Chadwick, C.; George, K.; Keevil, B.; et al. The association of a panel of biomarkers with the presence and severity of carcinoid heart disease: A cross-sectional study. PLoS ONE 2013, 8, e73679. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharyya, S.; Toumpanakis, C.; Caplin, M.E.; Davar, J. Usefulness of N-terminal pro-brain natriuretic peptide as a biomarker of the presence of carcinoid heart disease. Am. J. Cardiol. 2008, 102, 938–942. [Google Scholar] [CrossRef]
- Dobson, R.; Burgess, M.I.; Valle, J.W.; Pritchard, D.M.; Vora, J.; Wong, C.; Chadwick, C.; Keevi, B.; Adaway, J.; Hofmann, U.; et al. Serial surveillance of carcinoid heart disease: Factors associated with echocardiographic progression and mortality. Br. J. Cancer 2014, 111, 1703–1709. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharyya, S.; Toumpanakis, C.; Chilkunda, D.; Caplin, M.E.; Davar, J. Risk factors for the development and progression of carcinoid heart disease. Am. J. Cardiol. 2011, 107, 1221–1226. [Google Scholar] [CrossRef]
- Buchanan-Hughes, A.; Pashley, A.; Feuilly, M.; Marteau, F.; Pritchard, D.M.; Singh, S. Carcinoid Heart Disease: Prognostic Value of 5-Hydroxyindoleacetic Acid Levels and Impact on Survival: A Systematic Literature Review. Neuroendocrinology 2021, 111, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fijalkowski, R.; Reher, D.; Rinke, A.; Gress, T.M.; Schrader, J.; Baum, R.P.; Kaemmerer, D.; Horsch, D. Clinical Features and Prognosis of Patients with Carcinoid Syndrome and Carcinoid Heart Disease—A Retrospective Multicentric Study of 276 Patients. Neuroendocrinology 2021. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, B.I.; Hauso, O.; Drozdov, I.; Kidd, M.; Modlin, I.M. Carcinoid heart disease. Int. J. Cardiol. 2008, 129, 318–324. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | |||
|---|---|---|---|
| Characteristic | CHD− (n = 57) | CHD+ (n = 57) | p-Value |
| Sex, n (%) | |||
| Male | 26 (45.6) | 32 (56.1) | |
| Female | 31 (54.4) | 25 (43.9) | 0.349 |
| Median age at diagnosis, years (range) | 57.9 (32.3–76.9) | 59.7 (26.8–81.7) | 0.290 |
| Primary tumor, n (%) | n/a † | ||
| Small intestine | 56 (98.2) | 37 (64.9) | |
| Ovarium | 0 | 2 (3.5) | |
| Lung | 0 | 2 (3.5) | |
| Unknown | 1 (1.8) | 16 (28.1) | |
| Patients receiving treatments, n (%) | 16 (28.1) | 28 (49.1) | 0.034 ¥ |
| Beta blockers | 8 (14.0) | 8 (14.0) | |
| ACE-inhibitor | 2 (3.5) | 5 (8.8) | |
| Calcium antagonist | 7 (12.3) | 5 (8.8) | |
| Nitrates | 0 | 2 (3.5) | |
| ARB | 0 | 5 (8.8) | |
| Diuretics | 1 (1.8) | 21 (36.8) | |
| Median CHD score (range) | n/a | 10 (3–21) | n/a |
| Echocardiographic Characteristic | CHD Patients (n = 57) |
|---|---|
| TV regurgitation, n (%) | |
| Mild | 1 (1.8) |
| Moderate | 12 (21.1) |
| Severe | 44 (77.2) |
| TV leaflet thickening, n (%) | |
| None | 5 (8.8) |
| Mild | 10 (17.5) |
| Moderate | 22 (38.6) |
| Severe | 37 (64.9) |
| Missing | 20 (35.1) |
| PV regurgitation, n (%) | |
| None | 4 (7.0) |
| Mild | 8 (14.0) |
| Moderate | 11 (19.3) |
| Severe | 13 (22.8) |
| Missing | 21 (36.8) |
| RV dilation, n (%) | |
| None | 10 (17.5) |
| Mild | 7 (12.3) |
| Moderate | 17 (29.8) |
| Severe | 11 (19.3) |
| Missing | 12 (21.1) |
| RV impairment, n (%) | |
| None | 32 (56.1) |
| Mild | 5 (8.8) |
| Moderate | 2 (3.5) |
| Severe | 1 (1.8) |
| Missing | 17 (29.8) |
| MV regurgitation, n (%) | |
| None | 6 (10.5) |
| Mild | 22 (38.6) |
| Moderate | 7 (12.3) |
| Severe | 3 (5.3) |
| Missing | 19 (33.3) |
| AV regurgitation, n (%) | |
| None | 13 (22.8) |
| Mild | 15 (26.3) |
| Moderate | 3 (5.3) |
| Severe | 0 |
| Missing | 26 (45.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levy, S.; Kilgallen, A.B.; Korse, C.M.; Oerlemans, M.I.F.J.; Sluijter, J.P.G.; van Laake, L.W.; Valk, G.D.; Tesselaar, M.E.T. Elevated Serotonin and NT-proBNP Levels Predict and Detect Carcinoid Heart Disease in a Large Validation Study. Cancers 2022, 14, 2361. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102361
Levy S, Kilgallen AB, Korse CM, Oerlemans MIFJ, Sluijter JPG, van Laake LW, Valk GD, Tesselaar MET. Elevated Serotonin and NT-proBNP Levels Predict and Detect Carcinoid Heart Disease in a Large Validation Study. Cancers. 2022; 14(10):2361. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102361
Chicago/Turabian StyleLevy, Sonja, Aoife B. Kilgallen, Catharina M. Korse, Marish I. F. J. Oerlemans, Joost P. G. Sluijter, Linda W. van Laake, Gerlof D. Valk, and Margot E. T. Tesselaar. 2022. "Elevated Serotonin and NT-proBNP Levels Predict and Detect Carcinoid Heart Disease in a Large Validation Study" Cancers 14, no. 10: 2361. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102361