
Sex Differences in the Prevalence of Head and Neck Cancers: A 10-Year Follow-Up Study of 10 Million Healthy People

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
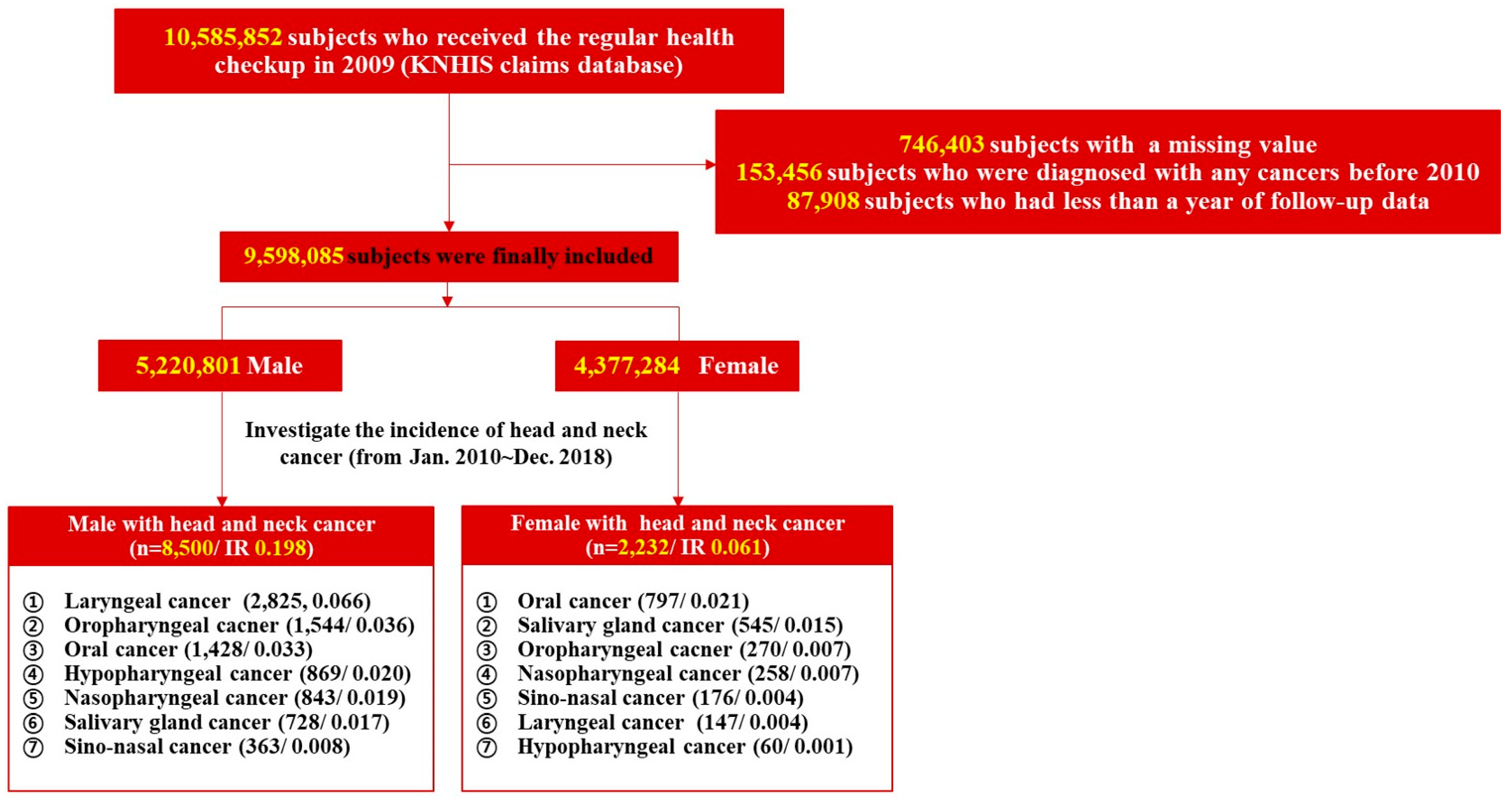
2.1. Data Source and Study Population
2.2. Study Design and Patient Selection
2.3. Potential Confounders
2.4. Outcome Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cook, M.B.; Dawsey, S.M.; Freedman, N.D.; Inskip, P.D.; Wichner, S.M.; Quraishi, S.M.; Devesa, S.S.; McGlynn, K.A. Sex disparities in cancer incidence by period and age. Cancer Epidemiol. Biomarkers Prev. 2009, 18, 1174–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edgren, G.; Liang, L.; Adami, H.O.; Chang, E.T. Enigmatic sex disparities in cancer incidence. Eur. J. Epidemiol. 2012, 27, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.M.; Sherman, R.L.; Henley, S.J.; Jemal, A.; Siegel, D.A.; Feuer, E.J.; Firth, A.U.; Kohler, B.A.; Scott, S.; Ma, J.; et al. Annual Report to the Nation on the Status of Cancer, Featuring Cancer in Men and Women Age 20–49 Years. J. Natl. Cancer Inst. 2019, 111, 1279–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, M.; Cioffi, G.; Wang, J.; Waite, K.A.; Ostrom, Q.T.; Kruchko, C.; Lathia, J.D.; Rubin, J.B.; Berens, M.E.; Connor, J.; et al. Sex Differences in Cancer Incidence and Survival: A Pan-Cancer Analysis. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Clayton, J.A.; Tannenbaum, C. Reporting Sex, Gender, or Both in Clinical Research? JAMA 2016, 316, 1863–1864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polderman, T.J.C.; Kreukels, B.P.C.; Irwig, M.S.; Beach, L.; Chan, Y.M.; Derks, E.M.; Esteva, I.; Ehrenfeld, J.; Heijer, M.D.; Posthuma, D.; et al. The Biological Contributions to Gender Identity and Gender Diversity: Bringing Data to the Table. Behav. Genet. 2018, 48, 95–108. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Suh, J.D.; Cho, J.H. Trends in Head and Neck Cancer in South Korea Between 1999 and 2012. Clin. Exp. Otorhinolaryngol. 2016, 9, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Dorak, M.T.; Karpuzoglu, E. Gender differences in cancer susceptibility: An inadequately addressed issue. Front. Genet. 2012, 3, 268. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.S. Introduction: Health of the health care system in Korea. Soc. Work. Public Health 2010, 25, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef] [PubMed]
- Hashibe, M.; Brennan, P.; Benhamou, S.; Castellsague, X.; Chen, C.; Curado, M.P.; Dal Maso, L.; Daudt, A.W.; Fabianova, E.; Fernandez, L.; et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: Pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J. Natl. Cancer Inst. 2007, 99, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Anantharaman, D.; Marron, M.; Lagiou, P.; Samoli, E.; Ahrens, W.; Pohlabeln, H.; Slamova, A.; Schejbalova, M.; Merletti, F.; Richiardi, L.; et al. Population attributable risk of tobacco and alcohol for upper aerodigestive tract cancer. Oral Oncol. 2011, 47, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Conway, D.I.; Brenner, D.R.; McMahon, A.D.; Macpherson, L.M.; Agudo, A.; Ahrens, W.; Bosetti, C.; Brenner, H.; Castellsague, X.; Chen, C.; et al. Estimating and explaining the effect of education and income on head and neck cancer risk: INHANCE consortium pooled analysis of 31 case-control studies from 27 countries. Int. J. Cancer 2015, 136, 1125–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, D.I.; Petticrew, M.; Marlborough, H.; Berthiller, J.; Hashibe, M.; Macpherson, L.M. Socioeconomic inequalities and oral cancer risk: A systematic review and meta-analysis of case-control studies. Int. J. Cancer 2008, 122, 2811–2819. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, R.A.; Weiderpass, E.; Tajara, E.H.; Ström, P.; Carvalho, A.L.; de Carvalho, M.B.; Kanda, J.L.; Moyses, R.A.; Wünsch-Filho, V. Diabetes mellitus, metformin and head and neck cancer. Oral Oncol. 2016, 61, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Khanna, A.; Sturgis, E.M.; Dahlstrom, K.R.; Xu, L.; Wei, Q.; Li, G.; Gross, N.D. Association of pretreatment body mass index with risk of head and neck cancer: A large single-center study. Am. J. Cancer Res. 2021, 11, 2343–2350. [Google Scholar]
- Christakoudi, S.; Kakourou, A.; Markozannes, G.; Tzoulaki, I.; Weiderpass, E.; Brennan, P.; Gunter, M.; Dahm, C.C.; Overvad, K.; Olsen, A.; et al. Blood pressure and risk of cancer in the European Prospective Investigation into Cancer and Nutrition. Int. J. Cancer 2020, 146, 2680–2693. [Google Scholar] [CrossRef]
- Clocchiatti, A.; Cora, E.; Zhang, Y.; Dotto, G.P. Sexual dimorphism in cancer. Nat. Rev. Cancer 2016, 16, 330–339. [Google Scholar] [CrossRef] [Green Version]
- Chlebowski, R.T.; Wactawski-Wende, J.; Ritenbaugh, C.; Hubbell, F.A.; Ascensao, J.; Rodabough, R.J.; Rosenberg, C.A.; Taylor, V.M.; Harris, R.; Chen, C.; et al. Estrogen plus progestin and colorectal cancer in postmenopausal women. New Engl. J. Med. 2004, 350, 991–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, J.W.; Hsu, I.; Xu, D.; Miyamoto, H.; Liang, L.; Wu, X.R.; Shyr, C.R.; Chang, C. Decreased tumorigenesis and mortality from bladder cancer in mice lacking urothelial androgen receptor. Am. J. Pathol. 2013, 182, 1811–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, H.; Yang, Z.; Chen, Y.T.; Ishiguro, H.; Uemura, H.; Kubota, Y.; Nagashima, Y.; Chang, Y.J.; Hu, Y.C.; Tsai, M.Y.; et al. Promotion of bladder cancer development and progression by androgen receptor signals. J. Natl. Cancer Inst. 2007, 99, 558–568. [Google Scholar] [CrossRef] [Green Version]
- Giuliano, A.R.; Nyitray, A.G.; Kreimer, A.R.; Pierce Campbell, C.M.; Goodman, M.T.; Sudenga, S.L.; Monsonego, J.; Franceschi, S. EUROGIN 2014 roadmap: Differences in human papillomavirus infection natural history, transmission and human papillomavirus-related cancer incidence by gender and anatomic site of infection. Int. J. Cancer 2015, 136, 2752–2760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertin, M.; Thébaud-Mony, A.; Counil, E. Do Women and Men Have the Same Patterns of Multiple Occupational Carcinogenic Exposures? Results from a Cohort of Cancer Patients. Ann. Work. Expo. Health 2018, 62, 450–464. [Google Scholar] [CrossRef] [PubMed]
- Pukkala, E.; Martinsen, J.I.; Lynge, E.; Gunnarsdottir, H.K.; Sparén, P.; Tryggvadottir, L.; Weiderpass, E.; Kjaerheim, K. Occupation and cancer—follow-up of 15 million people in five Nordic countries. Acta Oncol. 2009, 48, 646–790. [Google Scholar] [CrossRef] [Green Version]
- Özdemir, B.C.; Csajka, C.; Dotto, G.P.; Wagner, A.D. Sex Differences in Efficacy and Toxicity of Systemic Treatments: An Undervalued Issue in the Era of Precision Oncology. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2680–2683. [Google Scholar] [CrossRef]
- Williams, L.A.; Richardson, M.; Marcotte, E.L.; Poynter, J.N.; Spector, L.G. Sex ratio among childhood cancers by single year of age. Pediatric Blood Cancer 2019, 66, e27620. [Google Scholar] [CrossRef]
- Fish, E.N. The X-files in immunity: Sex-based differences predispose immune responses. Nat. Rev. Immunol. 2008, 8, 737–744. [Google Scholar] [CrossRef]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Inst. 2000, 92, 709–720. [Google Scholar] [CrossRef]
- Henle, G.; Henle, W. Epstein-Barr virus-specific IgA serum antibodies as an outstanding feature of nasopharyngeal carcinoma. Int. J. Cancer 1976, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lleo, A.; Battezzati, P.M.; Selmi, C.; Gershwin, M.E.; Podda, M. Is autoimmunity a matter of sex? Autoimmun. Rev. 2008, 7, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Li, W.-Z.; Lv, S.-H.; Liu, G.-Y.; Liang, H.; Xia, W.-X.; Xiang, Y.-Q. Age-dependent changes of gender disparities in nasopharyngeal carcinoma survival. Biol. Sex Differ. 2021, 12, 18. [Google Scholar] [CrossRef]
- OuYang, P.Y.; Zhang, L.N.; Lan, X.W.; Xie, C.; Zhang, W.W.; Wang, Q.X.; Su, Z.; Tang, J.; Xie, F.Y. The significant survival advantage of female sex in nasopharyngeal carcinoma: A propensity-matched analysis. Br. J. Cancer 2015, 112, 1554–1561. [Google Scholar] [CrossRef] [Green Version]
- Lewin, F.; Norell, S.E.; Johansson, H.; Gustavsson, P.; Wennerberg, J.; Biörklund, A.; Rutqvist, L.E. Smoking tobacco, oral snuff, and alcohol in the etiology of squamous cell carcinoma of the head and neck: A population-based case-referent study in Sweden. Cancer 1998, 82, 1367–1375. [Google Scholar] [CrossRef]
- Franceschi, S.; Bidoli, E.; Negri, E.; Barbone, F.; La Vecchia, C. Alcohol and cancers of the upper aerodigestive tract in men and women. Cancer Epidemiol. Biomarkers Prev. 1994, 3, 299–304. [Google Scholar]
- Kato, I.; Nomura, A.M. Alcohol in the aetiology of upper aerodigestive tract cancer. Eur. J. Cancer B Oral Oncol. 1994, 30b, 75–81. [Google Scholar] [CrossRef]
- Choi, S.Y.; Kahyo, H. Effect of cigarette smoking and alcohol consumption in the aetiology of cancer of the oral cavity, pharynx and larynx. Int. J. Epidemiol. 1991, 20, 878–885. [Google Scholar] [CrossRef]
- Marshall, B.J.; Warren, J.R. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1984, 1, 1311–1315. [Google Scholar] [CrossRef]
- Yokoyama, A.; Yokoyama, T.; Omori, T.; Matsushita, S.; Mizukami, T.; Takahashi, H.; Higuchi, S.; Maruyama, K.; Ishii, H.; Hibi, T. Helicobacter pylori, chronic atrophic gastritis, inactive aldehyde dehydrogenase-2, macrocytosis and multiple upper aerodigestive tract cancers and the risk for gastric cancer in alcoholic Japanese men. J. Gastroenterol. Hepatol. 2007, 22, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Kurtaran, H.; Uyar, M.E.; Kasapoglu, B.; Turkay, C.; Yilmaz, T.; Akcay, A.; Kanbay, M. Role of Helicobacter pylori in pathogenesis of upper respiratory system diseases. J. Natl. Med. Assoc. 2008, 100, 1224–1230. [Google Scholar] [CrossRef]
- Lu, Y.T.; Hsin, C.H.; Lu, Y.C.; Wu, M.C.; Huang, J.Y.; Huang, C.C.; Wang, P.H.; Yang, S.F. Risk of head and neck cancer in patients with peptic ulcers and the effect of Helicobacter pylori treatment. Sci. Rep. 2021, 11, 6229. [Google Scholar] [CrossRef] [PubMed]
- Laffont, S.; Seillet, C.; Guéry, J.-C. Estrogen Receptor-Dependent Regulation of Dendritic Cell Development and Function. Front. Immunol. 2017, 8, 108. [Google Scholar] [CrossRef] [Green Version]
- Verma, A.; Schwartz, N.; Cohen, D.J.; Boyan, B.D.; Schwartz, Z. Estrogen signaling and estrogen receptors as prognostic indicators in laryngeal cancer. Steroids 2019, 152, 108498. [Google Scholar] [CrossRef]
- Fei, M.; Zhang, J.; Zhou, J.; Xu, Y.; Wang, J. Sex-related hormone receptor in laryngeal squamous cell carcinoma: Correlation with androgen estrogen-ɑ and prolactin receptor expression and influence of prognosis. Acta Otolaryngol. 2018, 138, 66–72. [Google Scholar] [CrossRef]
- Verma, A.; Schwartz, N.; Cohen, D.J.; Patel, V.; Nageris, B.; Bachar, G.; Boyan, B.D.; Schwartz, Z. Loss of Estrogen Receptors is Associated with Increased Tumor Aggression in Laryngeal Squamous Cell Carcinoma. Sci. Rep. 2020, 10, 4227. [Google Scholar] [CrossRef]
- Atef, A.; El-Rashidy, M.A.; Elzayat, S.; Kabel, A.M. The prognostic value of sex hormone receptors expression in laryngeal carcinoma. Tissue Cell 2019, 57, 84–89. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Male (n = 5,220,801) | Female (n = 4,377,284) | p-Value |
|---|---|---|---|
| Age (years) | 45.63 ± 13.43 | 48.64 ± 14.5 | <0.0001 * |
| Age group | <0.0001 * | ||
| <40 years | 1,944,807 (37.25%) | 1,085,391 (24.8%) | |
| 40–64 years | 2,723,688 (52.17%) | 2,619,380 (59.84%) | |
| ≥65 years | 552,306 (10.58%) | 672,513 (15.36%) | |
| Smoking status | <0.0001 * | ||
| Never-smoker | 1,612,028 (30.88%) | 4,160,334 (95.04%) | |
| Ex-smoker | 1,256,220 (24.06%) | 69,232 (1.58%) | |
| Current smoker | 2,352,553 (45.06%) | 147,718 (3.37%) | |
| Drinking status | <0.0001 * | ||
| None | 1,674,378 (32.07%) | 3,264,933 (74.59%) | |
| Mild (<30 g/day) | 2,828,959 (54.19%) | 1,063,614 (24.3%) | |
| Heavy (≥30 g/day) | 717,464 (13.74%) | 48,737 (1.11%) | |
| Low income | 785,104 (15.04%) | 1,092,812 (24.97%) | <0.0001 * |
| Regular exercise | 1,030,226 (19.73%) | 678,186 (15.49%) | <0.0001 * |
| Height (cm) | 170.01 ± 6.44 | 156.48 ± 6.22 | <0.0001 * |
| Weight (kg) | 69.87 ± 10.54 | 56.73 ± 8.42 | <0.0001 * |
| Body mass index (kg/m2) | 24.13 ± 3.33 | 23.19 ± 3.54 | <0.0001 * |
| Body mass index (kg/m2) | <0.0001 * | ||
| <25 | 3,276,855 (62.77%) | 3,189,643 (72.87%) | |
| ≥25 | 1,943,946 (37.23%) | 1,187,641 (27.13%) | |
| Waist circumference (cm) | 83.56 ± 8.26 | 76.2 ± 9.3 | <0.0001 * |
| Abdominal obesity(waist circumference, M ≥ 90 cm/F ≥ 85 cm) | 1,115,781 (21.37%) | 768,973 (17.57%) | <0.0001 * |
| Glucose (mM) | 99.06 ± 25.77 | 95.07 ± 21.14 | <0.0001 * |
| Diabetes mellitus | 508,895 (9.75%) | 321,744 (7.35%) | <0.0001 * |
| Systolic BP (mmHg) | 124.66 ± 14.13 | 119.76 ± 15.71 | <0.0001 * |
| Diastolic BP (mmHg) | 78.05 ± 9.72 | 74.25 ± 10.09 | <0.0001 * |
| Hypertension | 1,395,431 (26.73%) | 1,071,413 (24.48%) | <0.0001 * |
| eGFR (mL/min/1.73 m2) | 87.99 ± 51.5 | 87.21 ± 36.52 | <0.0001 * |
| Chronic kidney disease (eGFR < 60) | 314,306 (6.02%) | 344,244 (7.86%) | <0.0001 * |
| Total cholesterol (mM) | 194.67 ± 40.93 | 196.15 ± 42.08 | <0.0001 * |
| HDL cholesterol (mM) | 53.56 ± 31.54 | 60 ± 33.83 | <0.0001 * |
| LDL cholesterol (mM) | 118.42 ± 190.63 | 122.75 ± 214.43 | <0.0001 * |
| Triglyceride (mM) | 129.15 (129.09–129.21) | 95.75 (95.7–95.8) | <0.0001 * |
| Dyslipidemia | 866,675 (16.6%) | 869,691 (19.87%) | <0.0001 * |
| Per 1000 Person-Years | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number | Event | Duration | Rate | HR (95% CI) | ||||||
| Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | |||||
| All head and neck cancers | ||||||||||
| Male | 5,220,801 | 8500 | 42,731,332.51 | 0.19892 | 3.238 (3.09, 3.392) | <0.0001 | 2.83 (2.67, 3) | <0.0001 | 2.816 (2.656, 2.985) | <0.0001 |
| Female | 4,377,284 | 2232 | 36,231,562.63 | 0.0616 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| Laryngeal cancer | ||||||||||
| Male | 5,220,801 | 2825 | 42,747,447.1 | 0.06609 | 16.306 (13.816, 19.244) | <0.0001 | 11.036 (9.218, 13.213) | <0.0001 | 10.981 (9.171, 13.148) | <0.0001 |
| Female | 4,377,284 | 147 | 36,238,096.36 | 0.00406 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| Sinonasal cancer | ||||||||||
| Male | 5,220,801 | 363 | 42,755,919.66 | 0.00849 | 1.754 (1.465, 2.1) | <0.0001 | 1.77 (1.398, 2.242) | <0.0001 | 1.758 (1.388, 2.226) | <0.0001 |
| Female | 4,377,284 | 176 | 36,238,089.5 | 0.00486 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| Hypopharyngeal cancer | ||||||||||
| Male | 5,220,801 | 869 | 42,754,938.24 | 0.02033 | 12.345 (9.504, 16.037) | <0.0001 | 9.987 (7.505, 13.289) | <0.0001 | 9.949 (7.476, 13.239) | <0.0001 |
| Female | 4,377,284 | 60 | 36,238,435.42 | 0.00166 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| Oropharyngeal cancer | ||||||||||
| Male | 5,220,801 | 1544 | 42,752,316.34 | 0.03612 | 4.856 (4.267, 5.527) | <0.0001 | 4.613 (3.963, 5.371) | <0.0001 | 4.589 (3.942, 5.343) | <0.0001 |
| Female | 4,377,284 | 270 | 36,237,728.87 | 0.00745 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| Oral cancer | ||||||||||
| Male | 5,220,801 | 1428 | 42,752,896.93 | 0.0334 | 1.523 (1.396, 1.661) | <0.0001 | 1.483 (1.32, 1.666) | <0.0001 | 1.472 (1.31, 1.654) | <0.0001 |
| Female | 4,377,284 | 797 | 36,236,352.3 | 0.02199 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| Nasopharyngeal cancer | ||||||||||
| Male | 5,220,801 | 843 | 42,754,118.86 | 0.01972 | 2.778 (2.417, 3.194) | <0.0001 | 2.798 (2.353, 3.327) | <0.0001 | 2.805 (2.359, 3.336) | <0.0001 |
| Female | 4377284 | 258 | 36237707.17 | 0.00712 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
| Salivary gland cancer | ||||||||||
| Male | 5,220,801 | 728 | 42,754,522.91 | 0.01703 | 1.132 (1.013, 1.265) | 0.0285 | 1.145 (0.983, 1.335) | 0.0815 | 1.139 (0.977, 1.327) | 0.0966 |
| Female | 4,377,284 | 545 | 36,236,699.52 | 0.01504 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-O.; Nam, I.-C.; Kim, C.-S.; Park, S.-J.; Lee, D.-H.; Kim, H.-B.; Han, K.-D.; Joo, Y.-H. Sex Differences in the Prevalence of Head and Neck Cancers: A 10-Year Follow-Up Study of 10 Million Healthy People. Cancers 2022, 14, 2521. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102521
Park J-O, Nam I-C, Kim C-S, Park S-J, Lee D-H, Kim H-B, Han K-D, Joo Y-H. Sex Differences in the Prevalence of Head and Neck Cancers: A 10-Year Follow-Up Study of 10 Million Healthy People. Cancers. 2022; 14(10):2521. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102521
Chicago/Turabian StylePark, Jun-Ook, Inn-Chul Nam, Choung-Soo Kim, Sung-Joon Park, Dong-Hyun Lee, Hyun-Bum Kim, Kyung-Do Han, and Young-Hoon Joo. 2022. "Sex Differences in the Prevalence of Head and Neck Cancers: A 10-Year Follow-Up Study of 10 Million Healthy People" Cancers 14, no. 10: 2521. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14102521