
Prostate Cancer Survivors Present Long-Term, Residual Systemic Immune Alterations

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Enrolment and Follow-Up
2.2. Blood Collection, Isolation of PBMCs and Plasma
2.3. Immune Phenotyping of PBMCs
2.4. Hierarchical Gating Strategy
2.5. Investigating the Protein Profile of Plasma Samples
2.6. Statistical Analyses
3. Results
3.1. Demographics and Clinical Parameters of Prostate Cancer Patients Treated with LDR Brachytherapy
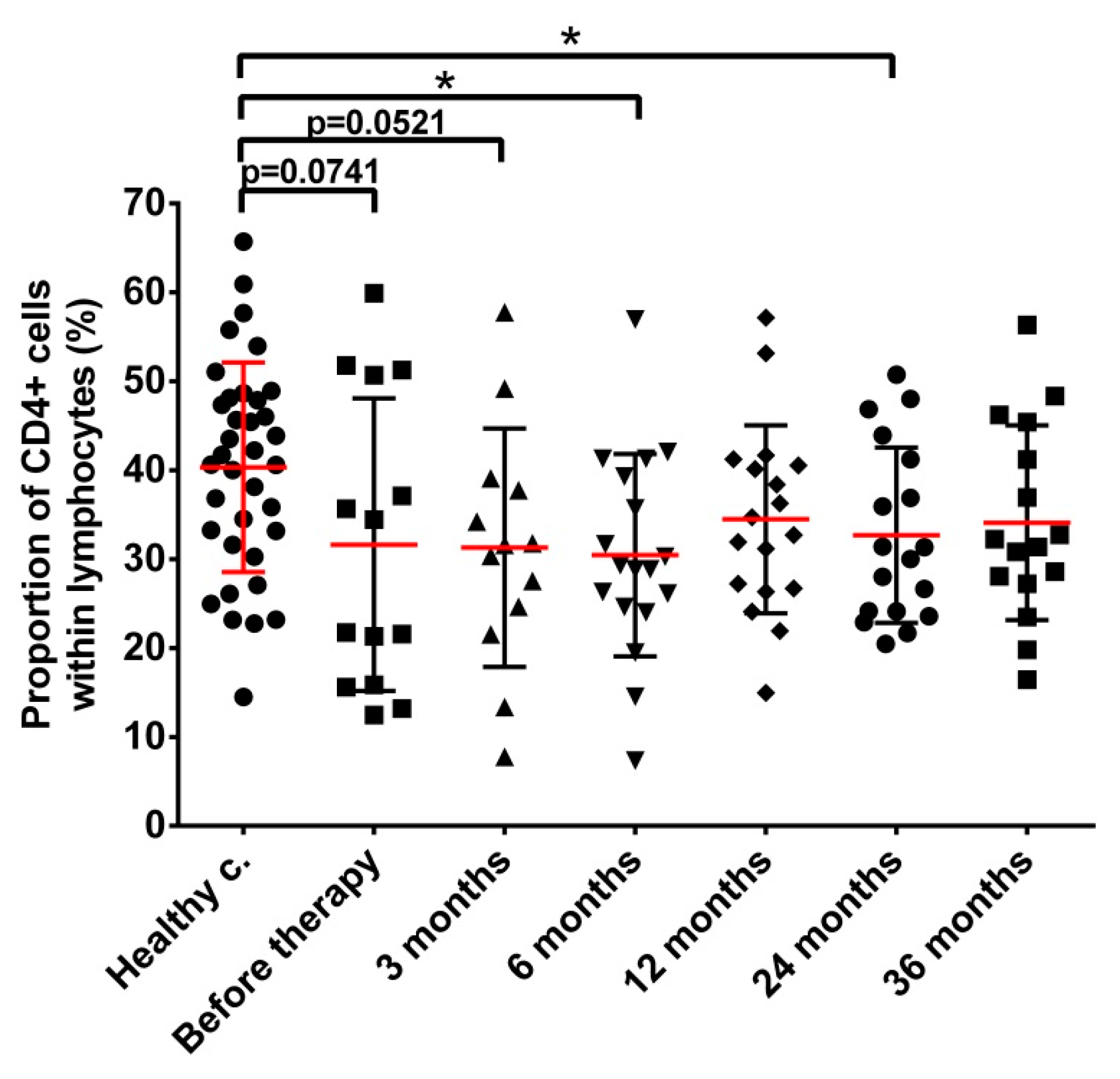
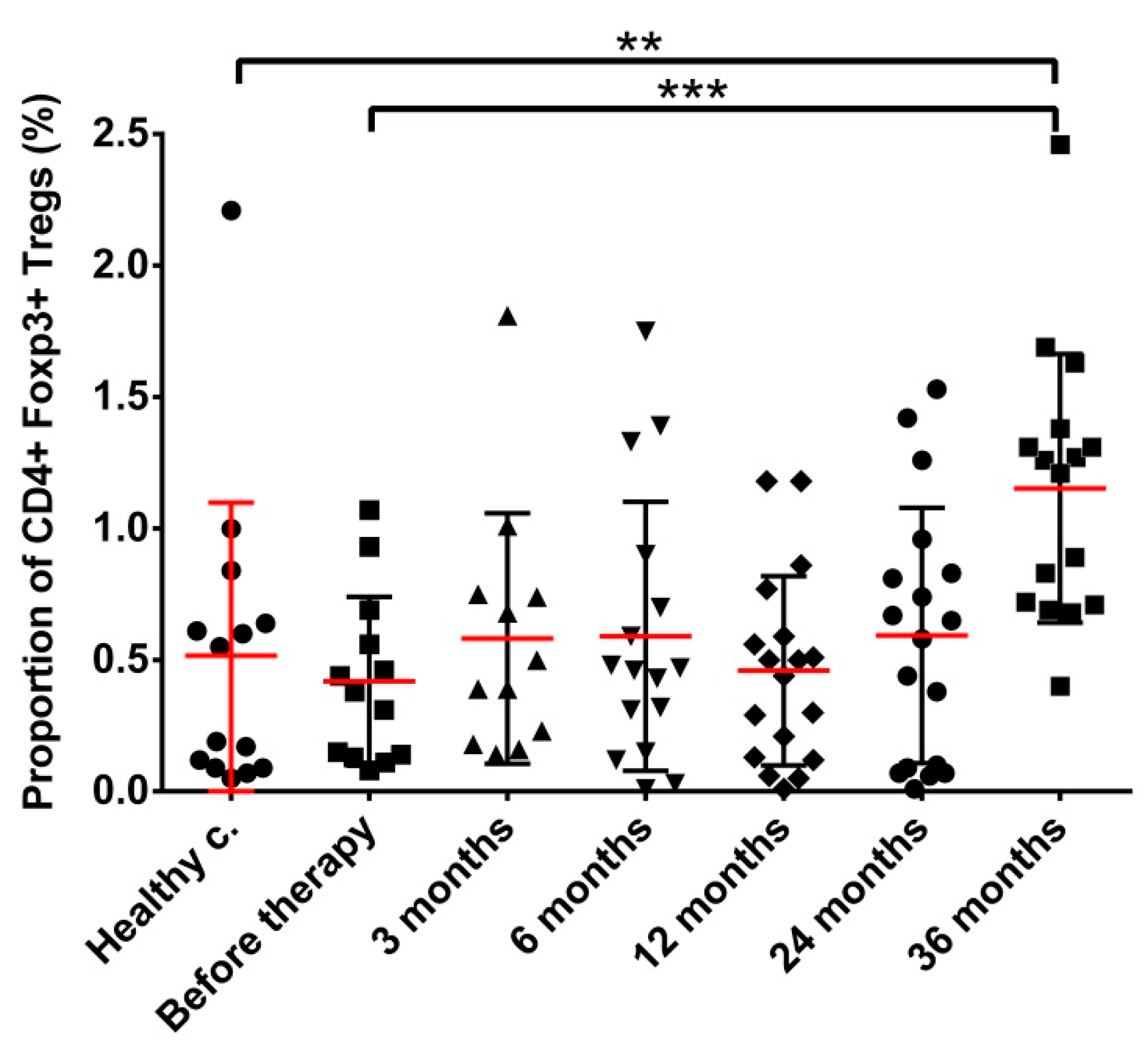
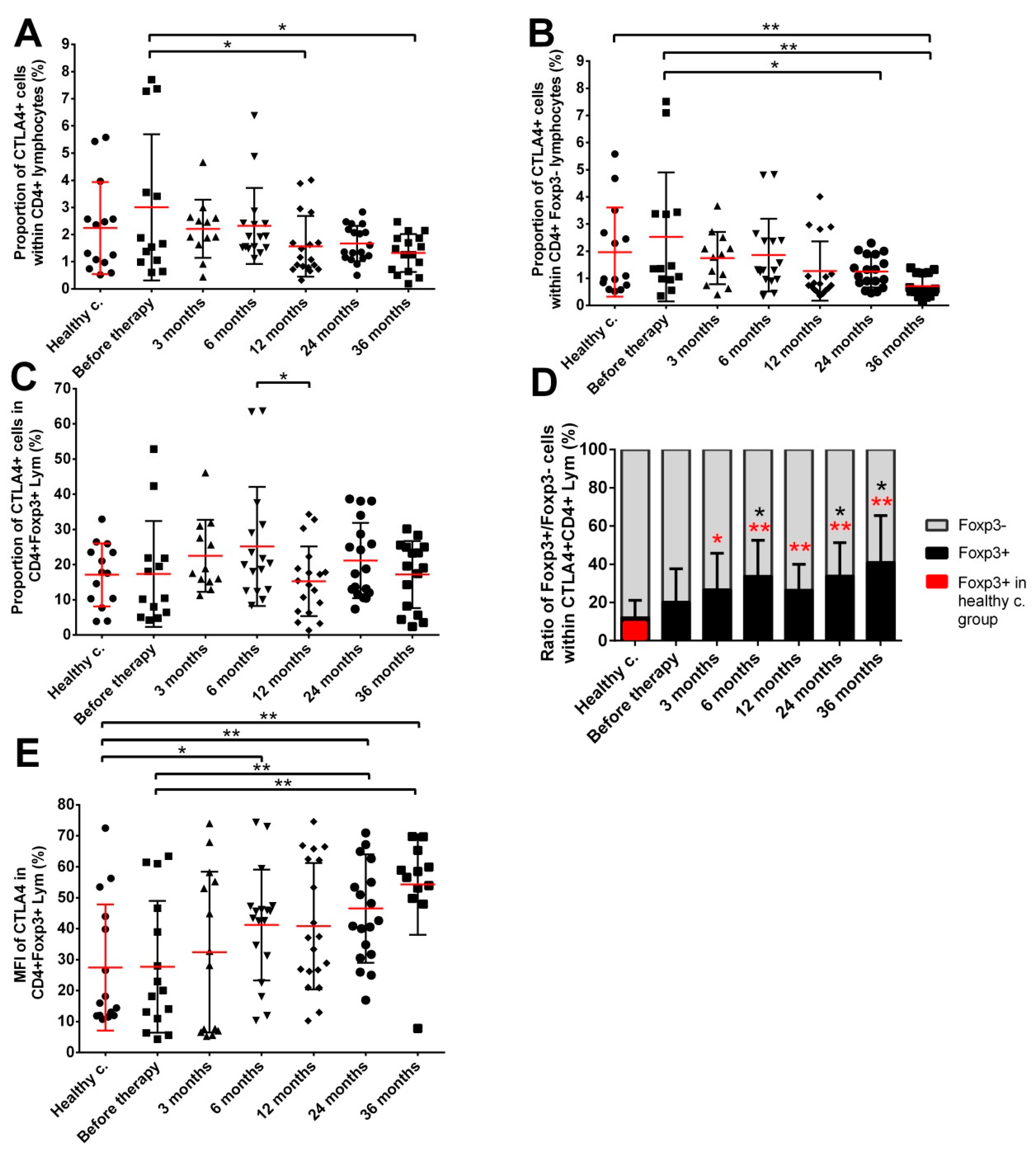
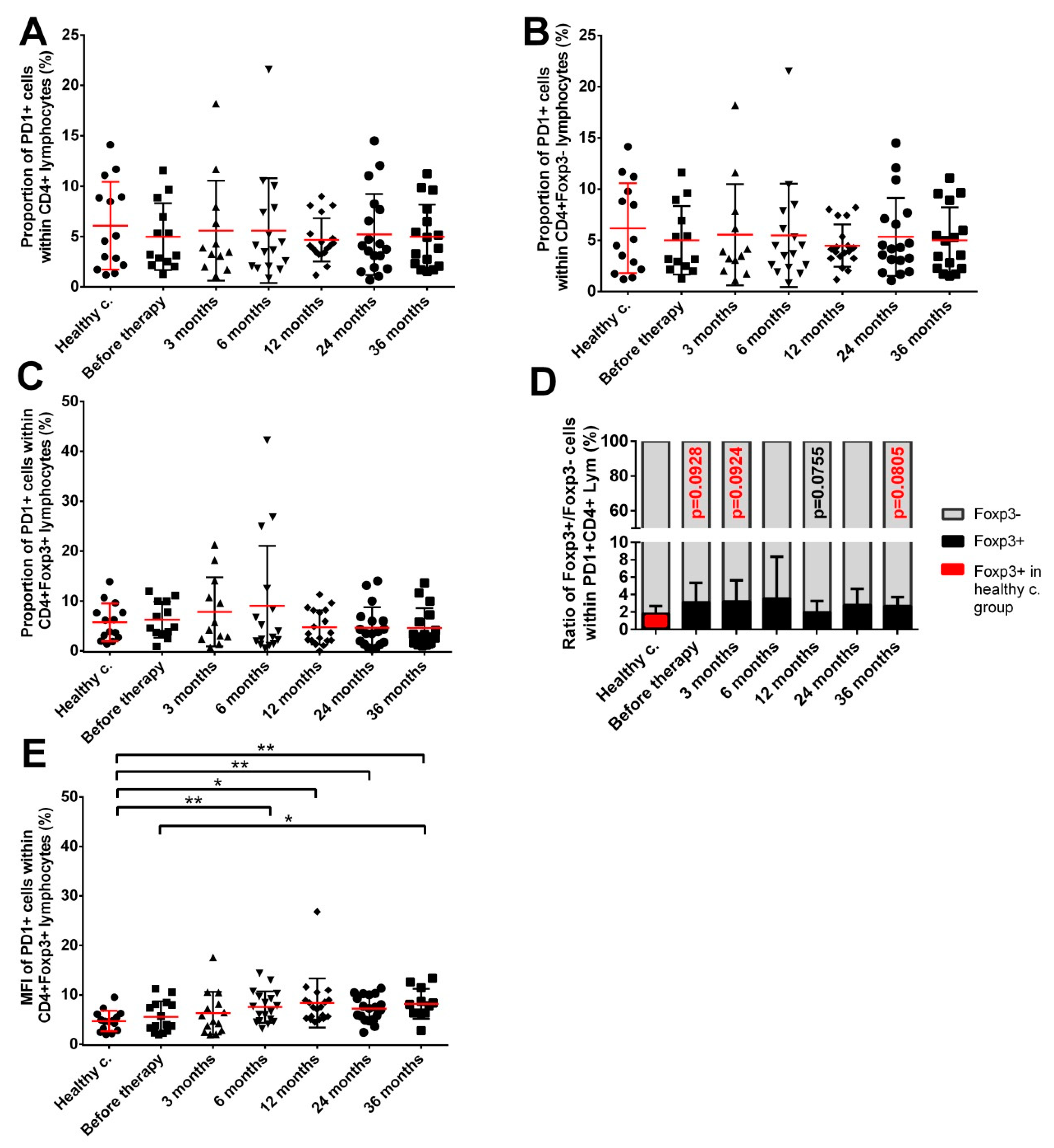
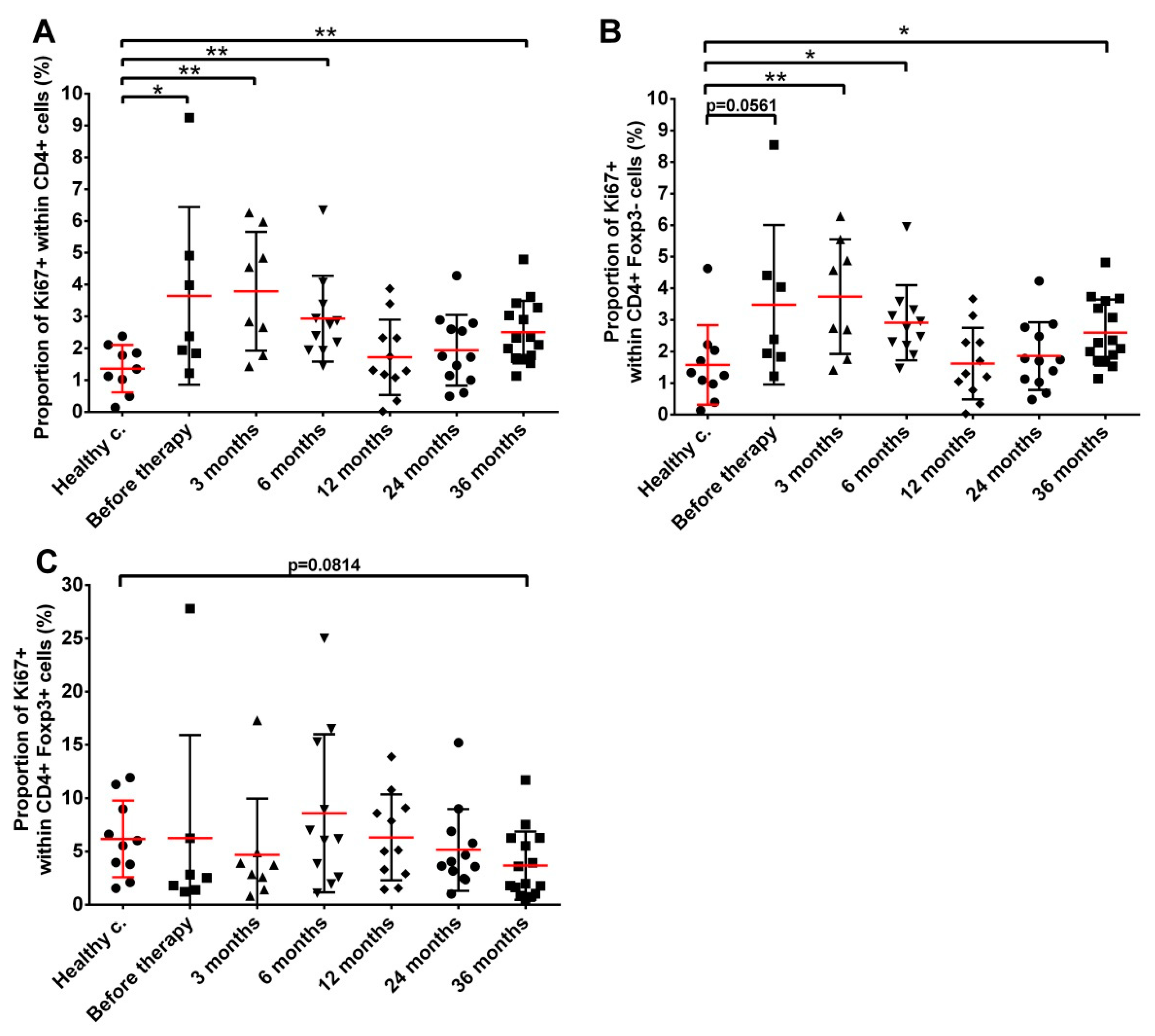
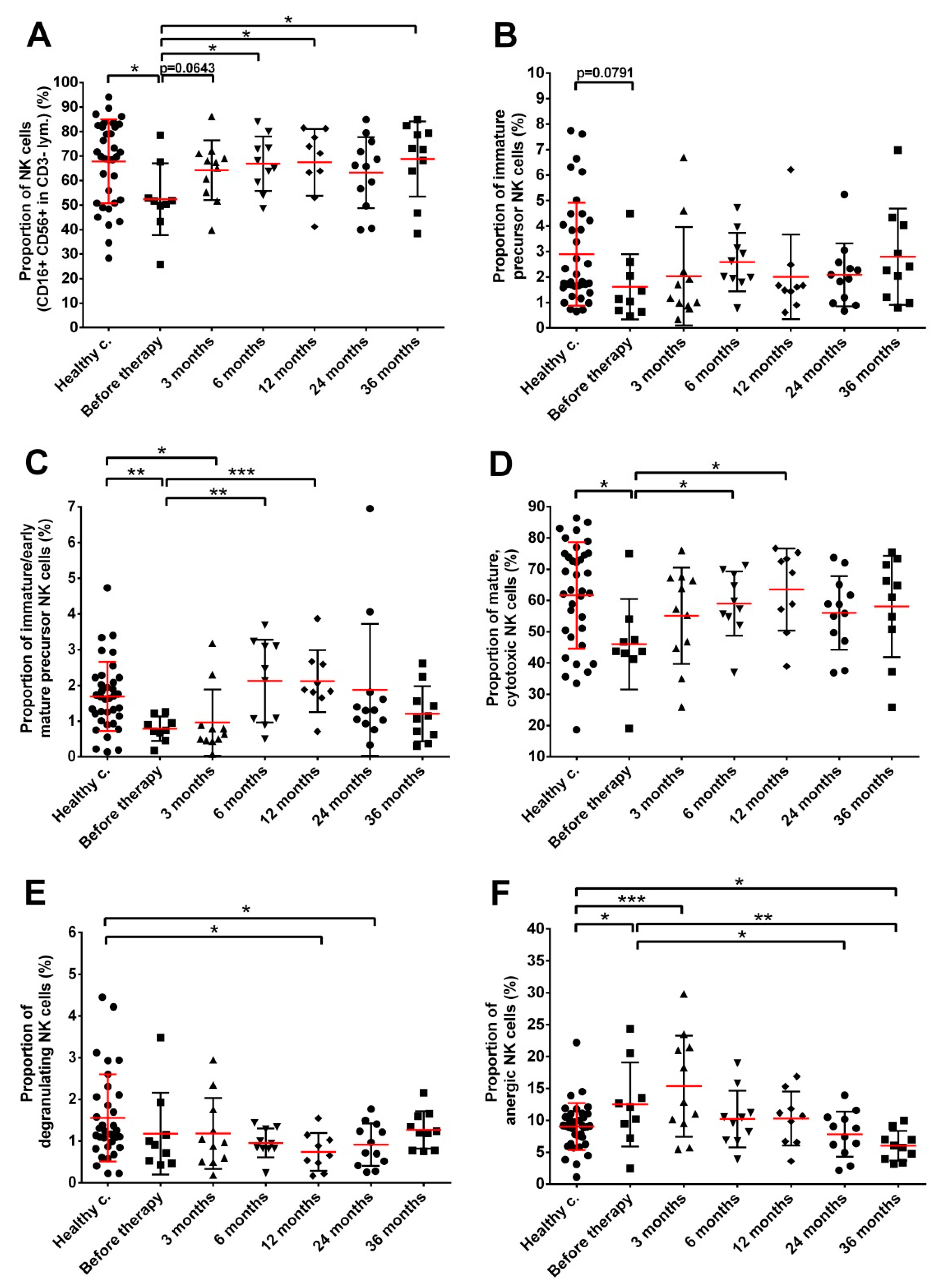
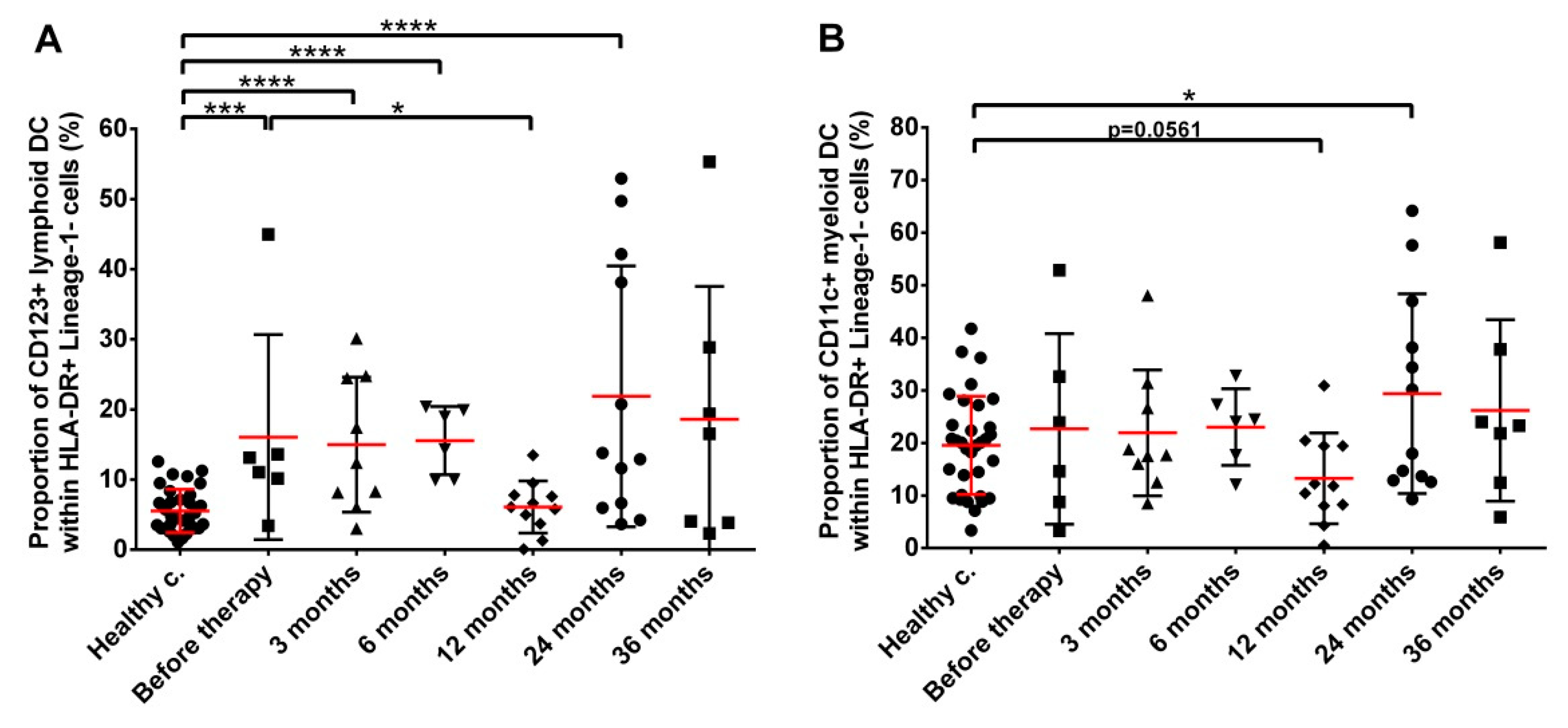
3.2. Low Dose Rate Brachytherapy Induces Persistent Changes in the Distribution and Phenotype of Several PBMC Subpopulations in Prostate Cancer Patients
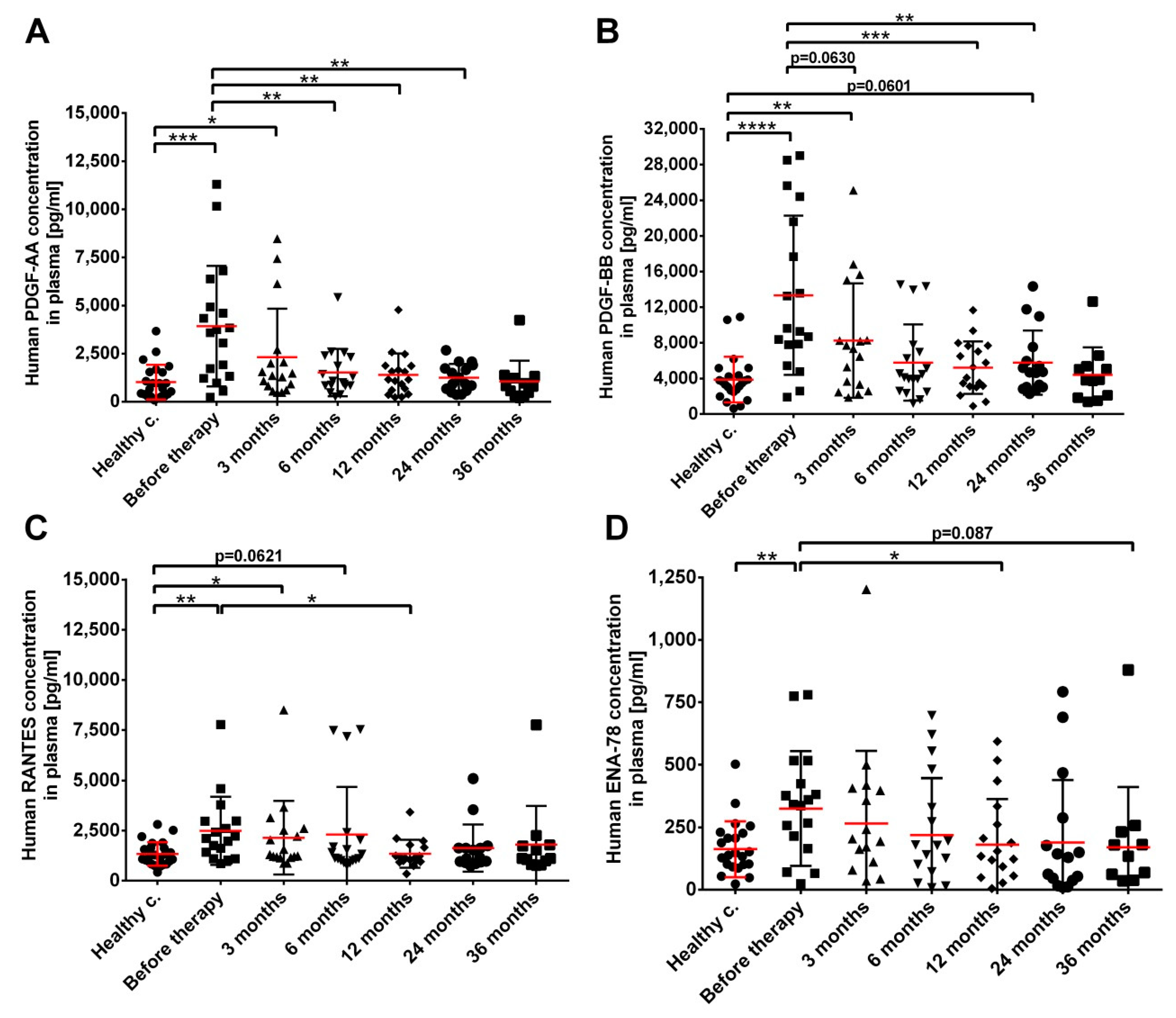
3.3. Increased Plasma Levels of Growth Factors and Chemokines in Prostate Cancer Patients Prior to RT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, S.; Wang, S.; Snuderl, M.; Karajannis, M.A. Pre-treatment lymphopenia and indication of tumor-induced systemic immunosuppression in medulloblastoma. J. Neurooncol. 2018, 136, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Alghamri, M.S.; Kamran, N.; Kadiyala, P.; Lowenstein, P.R.; Castro, M.G. Functional assay to assess T-cell inhibitory properties of myeloid derived suppressor cells (MDSCs) isolated from the tumor microenvironment of murine glioma models. Methods Enzymol. 2020, 632, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Bucher, C.; Munger, M.E.; Highfill, S.L.; Tolar, J.; Munn, D.H.; Levine, B.L.; Riddle, M.; June, C.H.; Vallera, D.A.; et al. Depletion of endogenous tumor-associated regulatory T cells improves the efficacy of adoptive cytotoxic T-cell immunotherapy in murine acute myeloid leukemia. Blood 2009, 114, 3793–3802. [Google Scholar] [CrossRef] [PubMed]
- Le Buanec, H.; Cohen, L.; Paturance, S.; Burny, A.; Gallo, R.C.; Zagury, D. Therapeutic vaccine to control stromal tumor-induced immunosuppression in human uterine cervixc cancer. Cell. Mol. Biol. 2003, 49, 667–671. [Google Scholar]
- Yan, L.; Da Silva, D.M.; Verma, B.; Gray, A.; Brand, H.E.; Skeate, J.G.; Porras, T.B.; Kanodia, S.; Kast, W.M. Forced LIGHT expression in prostate tumors overcomes Treg mediated immunosuppression and synergizes with a prostate tumor therapeutic vaccine by recruiting effector T lymphocytes. Prostate 2015, 75, 280–291. [Google Scholar] [CrossRef] [Green Version]
- Favaloro, J.; Brown, R.; Aklilu, E.; Yang, S.; Suen, H.; Hart, D.; Fromm, P.; Gibson, J.; Khoo, L.; Ho, P.J.; et al. Myeloma skews regulatory T and pro-inflammatory T helper 17 cell balance in favor of a suppressive state. Leuk. Lymphoma 2014, 55, 1090–1098. [Google Scholar] [CrossRef]
- Grauer, O.M.; Nierkens, S.; Bennink, E.; Toonen, L.W.; Boon, L.; Wesseling, P.; Sutmuller, R.P.; Adema, G.J. CD4+FoxP3+ regulatory T cells gradually accumulate in gliomas during tumor growth and efficiently suppress antiglioma immune responses in vivo. Int. J. Cancer 2007, 121, 95–105. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Balazs, K.; Antal, L.; Safrany, G.; Lumniczky, K. Blood-Derived Biomarkers of Diagnosis, Prognosis and Therapy Response in Prostate Cancer Patients. J. Pers. Med. 2021, 11, 296. [Google Scholar] [CrossRef]
- Sebesta, E.M.; Anderson, C.B. The Surgical Management of Prostate Cancer. Semin. Oncol. 2017, 44, 347–357. [Google Scholar] [CrossRef]
- Aima, M.; DeWerd, L.A.; Mitch, M.G.; Hammer, C.G.; Culberson, W.S. Dosimetric characterization of a new directional low-dose rate brachytherapy source. Med. Phys. 2018, 45, 3848–3860. [Google Scholar] [CrossRef] [PubMed]
- Barringer, B.S. The treatment by radium of carcinoma of the prostate and bladder: Preliminary report. J. Am. Med. Assoc. 1916, LXVII, 1442–1445. [Google Scholar] [CrossRef] [Green Version]
- Stish, B.J.; Davis, B.J.; Mynderse, L.A.; Deufel, C.L.; Choo, R. Brachytherapy in the Management of Prostate Cancer. Surg. Oncol. Clin. N. Am. 2017, 26, 491–513. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; MacManus, M.; Kron, T.; Best, N.; Smith, J.; Lobachevsky, P.; Ball, D.; Martin, O. A pattern of early radiation-induced inflammatory cytokine expression is associated with lung toxicity in patients with non-small cell lung cancer. PLoS ONE 2014, 9, e109560. [Google Scholar] [CrossRef] [PubMed]
- Frey, B.; Mika, J.; Jelonek, K.; Cruz-Garcia, L.; Roelants, C.; Testard, I.; Cherradi, N.; Lumniczky, K.; Polozov, S.; Napieralska, A.; et al. Systemic modulation of stress and immune parameters in patients treated for prostate adenocarcinoma by intensity-modulated radiation therapy or stereotactic ablative body radiotherapy. Strahlenther. Onkol. 2020, 196, 1018–1033. [Google Scholar] [CrossRef]
- Jelonek, K.; Pietrowska, M.; Widlak, P. Systemic effects of ionizing radiation at the proteome and metabolome levels in the blood of cancer patients treated with radiotherapy: The influence of inflammation and radiation toxicity. Int. J. Radiat. Biol. 2017, 93, 683–696. [Google Scholar] [CrossRef]
- Golden, E.B.; Chhabra, A.; Chachoua, A.; Adams, S.; Donach, M.; Fenton-Kerimian, M.; Friedman, K.; Ponzo, F.; Babb, J.S.; Goldberg, J.; et al. Local radiotherapy and granulocyte-macrophage colony-stimulating factor to generate abscopal responses in patients with metastatic solid tumours: A proof-of-principle trial. Lancet Oncol. 2015, 16, 795–803. [Google Scholar] [CrossRef]
- Doix, B.; Trempolec, N.; Riant, O.; Feron, O. Low Photosensitizer Dose and Early Radiotherapy Enhance Antitumor Immune Response of Photodynamic Therapy-Based Dendritic Cell Vaccination. Front. Oncol. 2019, 9, 811. [Google Scholar] [CrossRef]
- Gupta, A.; Probst, H.C.; Vuong, V.; Landshammer, A.; Muth, S.; Yagita, H.; Schwendener, R.; Pruschy, M.; Knuth, A.; van den Broek, M. Radiotherapy promotes tumor-specific effector CD8+ T cells via dendritic cell activation. J. Immunol. 2012, 189, 558–566. [Google Scholar] [CrossRef] [Green Version]
- Lugade, A.A.; Moran, J.P.; Gerber, S.A.; Rose, R.C.; Frelinger, J.G.; Lord, E.M. Local radiation therapy of B16 melanoma tumors increases the generation of tumor antigen-specific effector cells that traffic to the tumor. J. Immunol. 2005, 174, 7516–7523. [Google Scholar] [CrossRef] [Green Version]
- Diamond, M.S.; Kinder, M.; Matsushita, H.; Mashayekhi, M.; Dunn, G.P.; Archambault, J.M.; Lee, H.; Arthur, C.D.; White, J.M.; Kalinke, U.; et al. Type I interferon is selectively required by dendritic cells for immune rejection of tumors. J. Exp. Med. 2011, 208, 1989–2003. [Google Scholar] [CrossRef] [PubMed]
- Hald, S.M.; Bremnes, R.M.; Al-Shibli, K.; Al-Saad, S.; Andersen, S.; Stenvold, H.; Busund, L.T.; Donnem, T. CD4/CD8 co-expression shows independent prognostic impact in resected non-small cell lung cancer patients treated with adjuvant radiotherapy. Lung Cancer 2013, 80, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoud, S.M.; Paish, E.C.; Powe, D.G.; Macmillan, R.D.; Grainge, M.J.; Lee, A.H.; Ellis, I.O.; Green, A.R. Tumor-infiltrating CD8+ lymphocytes predict clinical outcome in breast cancer. J. Clin. Oncol. 2011, 29, 1949–1955. [Google Scholar] [CrossRef] [PubMed]
- Schaue, D.; Comin-Anduix, B.; Ribas, A.; Zhang, L.; Goodglick, L.; Sayre, J.W.; Debucquoy, A.; Haustermans, K.; McBride, W.H. T-cell responses to survivin in cancer patients undergoing radiation therapy. Clin. Cancer Res. 2008, 14, 4883–4890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, C.I.; Kim, D.; Ahn, S.G.; Bae, S.J.; Cha, C.; Park, S.; Park, S.; Kim, S.I.; Lee, H.S.; Park, J.Y.; et al. Radiotherapy-Induced High Neutrophil-to-Lymphocyte Ratio is a Negative Prognostic Factor in Patients with Breast Cancer. Cancers 2020, 12, 1896. [Google Scholar] [CrossRef] [PubMed]
- Dovsak, T.; Ihan, A.; Didanovic, V.; Kansky, A.; Verdenik, M.; Hren, N.I. Effect of surgery and radiotherapy on complete blood count, lymphocyte subsets and inflammatory response in patients with advanced oral cancer. BMC Cancer 2018, 18, 235. [Google Scholar] [CrossRef] [Green Version]
- Formenti, S.C.; Demaria, S. Systemic effects of local radiotherapy. Lancet Oncol. 2009, 10, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Postow, M.A.; Callahan, M.K.; Barker, C.A.; Yamada, Y.; Yuan, J.; Kitano, S.; Mu, Z.; Rasalan, T.; Adamow, M.; Ritter, E.; et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N. Engl. J. Med. 2012, 366, 925–931. [Google Scholar] [CrossRef] [Green Version]
- Balazs, K.; Kis, E.; Badie, C.; Bogdandi, E.N.; Candeias, S.; Garcia, L.C.; Dominczyk, I.; Frey, B.; Gaipl, U.; Juranyi, Z.; et al. Radiotherapy-Induced Changes in the Systemic Immune and Inflammation Parameters of Head and Neck Cancer Patients. Cancers 2019, 11, 1324. [Google Scholar] [CrossRef] [Green Version]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Barry, M.J.; Fowler, F.J., Jr.; O’Leary, M.P.; Bruskewitz, R.C.; Holtgrewe, H.L.; Mebust, W.K.; Cockett, A.T. The American Urological Association symptom index for benign prostatic hyperplasia. J. Urol. 1992, 148, 1549–1557; discussion 1564. [Google Scholar] [CrossRef]
- Clark, A.; Fallowfield, L.J. Quality of life measurements in patients with malignant disease: A review. J. R. Soc. Med. 1986, 79, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaronson, N.K.; Bullinger, M.; Ahmedzai, S. A modular approach to quality-of-life assessment in cancer clinical trials. Recent Results Cancer Res. 1988, 111, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Rotte, A. Combination of CTLA-4 and PD-1 blockers for treatment of cancer. J. Exp. Clin. Cancer Res. 2019, 38, 255. [Google Scholar] [CrossRef] [PubMed]
- Chikuma, S.; Abbas, A.K.; Bluestone, J.A. B7-independent inhibition of T cells by CTLA-4. J. Immunol. 2005, 175, 177–181. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.L.; Kuchroo, J.R.; Sage, P.T.; Liang, D.; Francisco, L.M.; Buck, J.; Thaker, Y.R.; Zhang, Q.; McArdel, S.L.; Juneja, V.R.; et al. PD-1 restraint of regulatory T cell suppressive activity is critical for immune tolerance. J. Exp. Med. 2021, 218, e20182232. [Google Scholar] [CrossRef]
- Osman, S.O.; Horn, S.; Brady, D.; McMahon, S.J.; Yoosuf, A.B.; Mitchell, D.; Crowther, K.; Lyons, C.A.; Hounsell, A.R.; Prise, K.M.; et al. Prostate cancer treated with brachytherapy; an exploratory study of dose-dependent biomarkers and quality of life. Radiat. Oncol. 2017, 12, 53. [Google Scholar] [CrossRef] [Green Version]
- Gogineni, E.; Rana, Z.; Soberman, D.; Sidiqi, B.; D’Andrea, V.; Lee, L.; Potters, L.; Parashar, B. Biochemical Control and Toxicity Outcomes of Stereotactic Body Radiation Therapy Versus Low-Dose-Rate Brachytherapy in the Treatment of Low- and Intermediate-Risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 1232–1242. [Google Scholar] [CrossRef]
- Mukai, Y.; Hayashi, N.; Koike, I.; Kaizu, H.; Takano, S.; Sugiura, M.; Ito, E.; Sato, M.; Uemura, H.; Yao, M.; et al. Acute and late toxicities in localized prostate cancer patients treated with low-dose (125)I brachytherapy (110 Gy) in combination with external beam radiation therapy versus brachytherapy alone (160 Gy). J. Contemp. Brachyther. 2018, 10, 397–404. [Google Scholar] [CrossRef]
- Kishan, A.U.; Kupelian, P.A. Late rectal toxicity after low-dose-rate brachytherapy: Incidence, predictors, and management of side effects. Brachytherapy 2015, 14, 148–159. [Google Scholar] [CrossRef]
- Sylvester, J.E.; Grimm, P.D.; Wong, J.; Galbreath, R.W.; Merrick, G.; Blasko, J.C. Fifteen-year biochemical relapse-free survival, cause-specific survival, and overall survival following I(125) prostate brachytherapy in clinically localized prostate cancer: Seattle experience. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Min, B. Spontaneous T Cell Proliferation: A Physiologic Process to Create and Maintain Homeostatic Balance and Diversity of the Immune System. Front. Immunol. 2018, 9, 547. [Google Scholar] [CrossRef] [PubMed]
- Wing, K.; Onishi, Y.; Prieto-Martin, P.; Yamaguchi, T.; Miyara, M.; Fehervari, Z.; Nomura, T.; Sakaguchi, S. CTLA-4 control over Foxp3+ regulatory T cell function. Science 2008, 322, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Gianchecchi, E.; Fierabracci, A. Inhibitory Receptors and Pathways of Lymphocytes: The Role of PD-1 in Treg Development and Their Involvement in Autoimmunity Onset and Cancer Progression. Front. Immunol. 2018, 9, 2374. [Google Scholar] [CrossRef] [Green Version]
- Kubo, M.; Satoh, T.; Ishiyama, H.; Tabata, K.I.; Tsumura, H.; Komori, S.; Iwamura, M.; Baba, S.; Hayakawa, K.; Kawamura, T.; et al. Enhanced activated T cell subsets in prostate cancer patients receiving iodine-125 low-dose-rate prostate brachytherapy. Oncol. Rep. 2018, 39, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Erlandsson, A.; Carlsson, J.; Lundholm, M.; Falt, A.; Andersson, S.O.; Andren, O.; Davidsson, S. M2 macrophages and regulatory T cells in lethal prostate cancer. Prostate 2019, 79, 363–369. [Google Scholar] [CrossRef]
- Miyara, M.; Yoshioka, Y.; Kitoh, A.; Shima, T.; Wing, K.; Niwa, A.; Parizot, C.; Taflin, C.; Heike, T.; Valeyre, D.; et al. Functional delineation and differentiation dynamics of human CD4+ T cells expressing the FoxP3 transcription factor. Immunity 2009, 30, 899–911. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.M.; Pisa, P. Tumor escape mechanisms in prostate cancer. Cancer Immunol. Immunother. 2007, 56, 81–87. [Google Scholar] [CrossRef]
- Karpisheh, V.; Mousavi, S.M.; Naghavi Sheykholeslami, P.; Fathi, M.; Mohammadpour Saray, M.; Aghebati-Maleki, L.; Jafari, R.; Majidi Zolbanin, N.; Jadidi-Niaragh, F. The role of regulatory T cells in the pathogenesis and treatment of prostate cancer. Life Sci. 2021, 284, 119132. [Google Scholar] [CrossRef]
- Miller, A.M.; Lundberg, K.; Ozenci, V.; Banham, A.H.; Hellstrom, M.; Egevad, L.; Pisa, P. CD4+CD25high T cells are enriched in the tumor and peripheral blood of prostate cancer patients. J. Immunol. 2006, 177, 7398–7405. [Google Scholar] [CrossRef] [Green Version]
- Bastid, J.; Regairaz, A.; Bonnefoy, N.; Dejou, C.; Giustiniani, J.; Laheurte, C.; Cochaud, S.; Laprevotte, E.; Funck-Brentano, E.; Hemon, P.; et al. Inhibition of CD39 enzymatic function at the surface of tumor cells alleviates their immunosuppressive activity. Cancer Immunol. Res. 2015, 3, 254–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, F.; Yu, M.; Cavanagh, M.M.; Hutter Saunders, J.; Qi, Q.; Ye, Z.; Le Saux, S.; Sultan, W.; Turgano, E.; Dekker, C.L.; et al. Expression of CD39 on Activated T Cells Impairs their Survival in Older Individuals. Cell Rep. 2016, 14, 1218–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michel, T.; Poli, A.; Cuapio, A.; Briquemont, B.; Iserentant, G.; Ollert, M.; Zimmer, J. Human CD56bright NK Cells: An Update. J. Immunol. 2016, 196, 2923–2931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amand, M.; Iserentant, G.; Poli, A.; Sleiman, M.; Fievez, V.; Sanchez, I.P.; Sauvageot, N.; Michel, T.; Aouali, N.; Janji, B.; et al. Human CD56(dim)CD16(dim) Cells As an Individualized Natural Killer Cell Subset. Front. Immunol. 2017, 8, 699. [Google Scholar] [CrossRef]
- Cooper, M.A.; Fehniger, T.A.; Caligiuri, M.A. The biology of human natural killer-cell subsets. Trends Immunol. 2001, 22, 633–640. [Google Scholar] [CrossRef]
- Forconi, C.S.; Oduor, C.I.; Oluoch, P.O.; Ong’echa, J.M.; Munz, C.; Bailey, J.A.; Moormann, A.M. A New Hope for CD56(neg)CD16(pos) NK Cells as Unconventional Cytotoxic Mediators: An Adaptation to Chronic Diseases. Front. Cell. Infect. Microbiol. 2020, 10, 162. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Cheng, H.; Zhang, Y.; Fan, K.; Luo, G.; Fan, Z.; Huang, Q.; Lu, Y.; Jin, K.; Wang, Z.; et al. Anergic natural killer cells educated by tumor cells are associated with a poor prognosis in patients with advanced pancreatic ductal adenocarcinoma. Cancer Immunol. Immunother. 2018, 67, 1815–1823. [Google Scholar] [CrossRef]
- Mamessier, E.; Bourgin, C.; Olive, D. When breast cancer cells start to fend the educational process of NK cells off. Oncoimmunology 2013, 2, e26688. [Google Scholar] [CrossRef] [Green Version]
- Baxevanis, C.N.; Gritzapis, A.D.; Papamichail, M. In vivo antitumor activity of NKT cells activated by the combination of IL-12 and IL-18. J. Immunol. 2003, 171, 2953–2959. [Google Scholar] [CrossRef] [Green Version]
- Min, X.Y.; Liu, C.F.; Cao, B.; Zhang, T.; Yang, X.; Ma, N.; Wang, N.; Li, K. Human CD3(+)CD56(+)NKT-like cells express a range of complement receptors and C3 activation has negative effects on these cell activity and effector function. Hum. Immunol. 2021, 82, 625–633. [Google Scholar] [CrossRef]
- Wu, L.; Van Kaer, L. Natural killer T cells in health and disease. Front. Biosci. 2011, 3, 236–251. [Google Scholar] [CrossRef] [Green Version]
- Tahir, S.M.; Cheng, O.; Shaulov, A.; Koezuka, Y.; Bubley, G.J.; Wilson, S.B.; Balk, S.P.; Exley, M.A. Loss of IFN-gamma production by invariant NK T cells in advanced cancer. J. Immunol. 2001, 167, 4046–4050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowak, M.; Schmidt-Wolf, I.G. Natural killer T cells subsets in cancer, functional defects in prostate cancer and implications for immunotherapy. Cancers 2011, 3, 3661–3675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastelic-Gavillet, B.; Sarivalasis, A.; Lozano, L.E.; Wyss, T.; Inoges, S.; de Vries, I.J.M.; Dartiguenave, F.; Jichlinski, P.; Derre, L.; Coukos, G.; et al. Quantitative and qualitative impairments in dendritic cell subsets of patients with ovarian or prostate cancer. Eur. J. Cancer 2020, 135, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Minkov, P.; Gulubova, M.; Ivanova, K.; Obretenov, E.; Ananiev, J. CD11c- and CD123-positive dendritic cells in development of antitumour immunity in non-small cell lung cancer patients. Pol. J. Pathol. 2019, 70, 109–114. [Google Scholar] [CrossRef]
- Ye, F.; Yu, Y.; Hu, Y.; Lu, W.; Xie, X. Alterations of dendritic cell subsets in the peripheral circulation of patients with cervical carcinoma. J. Exp. Clin. Cancer Res. 2010, 29, 78. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, R.; Kassianos, A.J.; Swindle, P.; Hart, D.N.; Radford, K.J. Numerical and functional assessment of blood dendritic cells in prostate cancer patients. Prostate 2006, 66, 180–192. [Google Scholar] [CrossRef]
- Adekoya, T.O.; Richardson, R.M. Cytokines and Chemokines as Mediators of Prostate Cancer Metastasis. Int. J. Mol. Sci. 2020, 21, 4449. [Google Scholar] [CrossRef]
- Bouraoui, Y.; Ricote, M.; Garcia-Tunon, I.; Rodriguez-Berriguete, G.; Touffehi, M.; Rais, N.B.; Fraile, B.; Paniagua, R.; Oueslati, R.; Royuela, M. Pro-inflammatory cytokines and prostate-specific antigen in hyperplasia and human prostate cancer. Cancer Detect. Prev. 2008, 32, 23–32. [Google Scholar] [CrossRef]
- Esfahani, M.; Ataei, N.; Panjehpour, M. Biomarkers for evaluation of prostate cancer prognosis. Asian Pac. J. Cancer Prev. 2015, 16, 2601–2611. [Google Scholar] [CrossRef] [Green Version]
- Christensen, E.; Pintilie, M.; Evans, K.R.; Lenarduzzi, M.; Menard, C.; Catton, C.N.; Diamandis, E.P.; Bristow, R.G. Longitudinal cytokine expression during IMRT for prostate cancer and acute treatment toxicity. Clin. Cancer Res. 2009, 15, 5576–5583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, O.A.; Yin, X.; Forrester, H.B.; Sprung, C.N.; Martin, R.F. Potential strategies to ameliorate risk of radiotherapy-induced second malignant neoplasms. Semin. Cancer Biol. 2016, 37–38, 65–76. [Google Scholar] [CrossRef]
- Zhao, R.; Bei, X.; Yang, B.; Wang, X.; Jiang, C.; Shi, F.; Wang, X.; Zhu, Y.; Jing, Y.; Han, B.; et al. Endothelial cells promote metastasis of prostate cancer by enhancing autophagy. J. Exp. Clin. Cancer Res. 2018, 37, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, K.K.; Fink, L.M.; Hughes, B.M.; Shmaysani, H.M.; Sung, C.C.; Hauer-Jensen, M. Differential effect of radiation on endothelial cell function in rectal cancer and normal rectum. Am. J. Surg. 1998, 176, 642–647. [Google Scholar] [CrossRef]
- Milliat, F.; Francois, A.; Tamarat, R.; Benderitter, M. Role of endothelium in radiation-induced normal tissue damages. Ann. Cardiol. Angeiol. 2008, 57, 139–148. [Google Scholar] [CrossRef]
- Tanji, N.; Kikugawa, T.; Ochi, T.; Taguchi, S.; Sato, H.; Sato, T.; Sugahara, T.; Hamada, H.; Asai, S.; Matsumoto, A. Circulating Cytokine Levels in Patients with Prostate Cancer: Effects of Neoadjuvant Hormonal Therapy and External-beam Radiotherapy. Anticancer Res. 2015, 35, 3379–3383. [Google Scholar]
- Heldin, C.H. Platelet-derived growth factor--an introduction. Cytokine Growth Factor Rev. 2004, 15, 195–196. [Google Scholar] [CrossRef]
- Kazlauskas, A. PDGFs and their receptors. Gene 2017, 614, 1–7. [Google Scholar] [CrossRef]
- Andrae, J.; Gallini, R.; Betsholtz, C. Role of platelet-derived growth factors in physiology and medicine. Genes Dev. 2008, 22, 1276–1312. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wu, J.Z.; Yang, Y.Q.; Ma, R.; Zhang, J.Y.; Feng, J.F. Expression of growthregulated oncogene1, hepatocyte growth factor, plateletderived growth factorAA and soluble Eselectin and their association with highrisk human papillomavirus infection in squamous cell carcinoma of the uterine cervix. Mol. Med. Rep. 2014, 10, 1013–1024. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Ye, H.; Liu, Z.; Xu, C.; Zhang, Z.; Liu, Y.; Sun, Y. Platelet-derived growth factor-BB accelerates prostate cancer growth by promoting the proliferation of mesenchymal stem cells. J. Cell. Biochem. 2013, 114, 1510–1518. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Jendrossek, V.; Belka, C. The role of PDGF in radiation oncology. Radiat. Oncol. 2007, 2, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nister, M.; Libermann, T.A.; Betsholtz, C.; Pettersson, M.; Claesson-Welsh, L.; Heldin, C.H.; Schlessinger, J.; Westermark, B. Expression of messenger RNAs for platelet-derived growth factor and transforming growth factor-alpha and their receptors in human malignant glioma cell lines. Cancer Res. 1988, 48, 3910–3918. [Google Scholar] [PubMed]
- Huang, R.; Wang, S.; Wang, N.; Zheng, Y.; Zhou, J.; Yang, B.; Wang, X.; Zhang, J.; Guo, L.; Wang, S.; et al. CCL5 derived from tumor-associated macrophages promotes prostate cancer stem cells and metastasis via activating beta-catenin/STAT3 signaling. Cell Death Dis. 2020, 11, 234. [Google Scholar] [CrossRef]
- Arenberg, D.A.; Keane, M.P.; DiGiovine, B.; Kunkel, S.L.; Morris, S.B.; Xue, Y.Y.; Burdick, M.D.; Glass, M.C.; Iannettoni, M.D.; Strieter, R.M. Epithelial-neutrophil activating peptide (ENA-78) is an important angiogenic factor in non-small cell lung cancer. J. Clin. Investig. 1998, 102, 465–472. [Google Scholar] [CrossRef]
- Kuo, P.L.; Chen, Y.H.; Chen, T.C.; Shen, K.H.; Hsu, Y.L. CXCL5/ENA78 increased cell migration and epithelial-to-mesenchymal transition of hormone-independent prostate cancer by early growth response-1/snail signaling pathway. J. Cell. Physiol. 2011, 226, 1224–1231. [Google Scholar] [CrossRef]
- Gyuleva, I.M.; Penkova, K.I.; Rupova, I.T.; Panova, D.Y.; Djounova, J.N. Assessment of Some Immune Parameters in Occupationally Exposed Nuclear Power Plant Workers: Flow Cytometry Measurements of T Lymphocyte Subpopulations and Immunoglobulin Determination. Dose-Response 2015, 13, 1559325815611901. [Google Scholar] [CrossRef]
- Gyuleva, I.; Panova, D.; Djounova, J.; Rupova, I.; Penkova, K. Assessment of Some Immune Parameters in Occupationally Exposed Nuclear Power Plants Workers: Flow cytometry Measurements of T, B, NK and NKT Cells. Dose-Response 2015, 13, 1559325815611901. [Google Scholar] [CrossRef]
- Lumniczky, K.; Impens, N.; Armengol, G.; Candeias, S.; Georgakilas, A.G.; Hornhardt, S.; Martin, O.A.; Rodel, F.; Schaue, D. Low dose ionizing radiation effects on the immune system. Environ. Int. 2021, 149, 106212. [Google Scholar] [CrossRef]
- De Padova, S.; Urbini, M.; Schepisi, G.; Virga, A.; Meggiolaro, E.; Rossi, L.; Fabbri, F.; Bertelli, T.; Ulivi, P.; Ruffilli, F.; et al. Immunosenescence in Testicular Cancer Survivors: Potential Implications of Cancer Therapies and Psychological Distress. Front. Oncol. 2020, 10, 564346. [Google Scholar] [CrossRef]
- Sulicka-Grodzicka, J.; Surdacki, A.; Seweryn, M.; Mikolajczyk, T.; Rewiuk, K.; Guzik, T.; Grodzicki, T. Low-grade chronic inflammation and immune alterations in childhood and adolescent cancer survivors: A contribution to accelerated aging? Cancer Med. 2021, 10, 1772–1782. [Google Scholar] [CrossRef] [PubMed]
- Prinsen, H.; van Laarhoven, H.W.; Pots, J.M.; Duiveman-de Boer, T.; Mulder, S.F.; van Herpen, C.M.; Jacobs, J.F.; Leer, J.W.; Bleijenberg, G.; Stelma, F.F.; et al. Humoral and cellular immune responses after influenza vaccination in patients with postcancer fatigue. Hum. Vaccines Immunother. 2015, 11, 1634–1640. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Code | Age (years) | Risk Classification | TNM Classification | Gleason Score (GS) | Hormone Type | Duration of Hormone Therapy Before RT (months) |
|---|---|---|---|---|---|---|
| P053 | 62 | 2 | cT2c cN0 M0 | 3 + 2 | 0 | 0 |
| P056 | 73 | 1 | cT2a cN0 M0 | 3 + 3 | LHRH antagonist | 6 |
| P057 | 61 | 1 | cT2b cN0 M0 | 3 + 3 | LHRH agonist | 3 |
| P058 | 67 | 2 | cT2a cN0 M0 | 3 + 4 | 0 | 0 |
| P061 | 73 | 2 | cT2c cN0 M0 | 3 + 3 | 0 | 0 |
| P062 | 69 | 2 | cT2a cN0 M0 | 3 + 3 | LHRH agonist | 3 |
| P068 | 72 | 2 | cT1c cN0 M0 | 3 + 3 | TAB | 3 |
| P069 | 62 | 1 | cT2b cN0 M0 | 3 + 2 | 0 | 0 |
| P071 | 74 | 3 | cT1c cN0 M0 | 3 + 3 | LHRH agonist | 38 |
| P072 * | 68 | 2 | cT2b cN0 M0 | 3 + 4 | LHRH agonist | 1 |
| P080 | 75 | 2 | cT1c cN0 M0 | 3 + 4 | LHRH agonist | 5 |
| P081 | 76 | 1 | cT2a cN0 M0 | 2 + 2 | LHRH agonist | 34 |
| P083 | 72 | 2 | cT2c cN0 M0 | 3 + 3 | LHRH agonist | 3 |
| P084 | 63 | 1 | cT2a cN0 M0 | 2 + 3 | LHRH antagonist | 3 |
| P085 * | 52 | 2 | cT2c cN0 M0 | 3 + 3 | 0 | 0 |
| P091 * | 72 | 2 | cT2c cN0 M0 | 3 + 3 | LHRH agonist | 3 |
| P092 | 77 | 2 | cT1c cN0 M0 | 3 + 4 | LHRH agonist | 3 |
| P094 | 69 | 1 | cT2a cN0 M0 | - | LHRH agonist | 6 |
| P095 | 70 | 1 | cT2a cN0 M0 | 3 + 3 | 0 | 0 |
| P170 | 64 | 2 | cT2c cN0 M0 | 3 + 3 | 0 | 0 |
| P176 | 72 | 2 | cT1c cN0 M0 | 3 + 3 | 0 | 0 |
| PSA Level (ng/mL) | ||||||
|---|---|---|---|---|---|---|
| Patient Code | Before Therapy | 3 Months after Therapy | 6 Months after Therapy | 12 Months after Therapy | 24 Months after Therapy | 36 Months after Therapy |
| P053 | 7.00 | 0.57 | 0.28 | 0.01 | 0.14 | 0.10 |
| P056 | 0.90 | 1.00 | 0.69 | 0.40 | 0.55 | 0.30 |
| P057 | 1.64 | 2.07 | 1.36 | 1.89 | 1.40 | 0.40 |
| P058 | 12.20 | 6.44 | 2.94 | 1.04 | 0.28 | n |
| P061 | 11.40 | 1.87 | 1.07 | 0.01 | 0.21 | 0.16 |
| P062 | 0.93 | 1.63 | 1.28 | 0.76 | 0.68 | 0.77 |
| P068 | 0.09 | 0.60 | 0.90 | 0.60 | 0.60 | 0.40 |
| P069 | 4.73 | 1.15 | 0.60 | 2,10 | 1.20 | 1.50 |
| P071 | 1.14 | 0.50 | 0.34 | 0.59 | 0.23 | 1.34 |
| P072 | 13.9 | 0.09 | 0.04 | n | n | n |
| P080 | 0.09 | 0.30 | 0.33 | 0.42 | 1.60 | 5.70 |
| P081 | 1.73 | 0.09 | 0.06 | 0.07 | 0.15 | n |
| P083 | 0.75 | 0.38 | 0.41 | 1.13 | 0.43 | 0.26 |
| P084 | n | 0.05 | 0.07 | 0.15 | 0.35 | 0.05 |
| P085 | 5.01 | 5.50 | 6.60 | 0.15 | n | n |
| P091 | 4.74 | 2.3 | 1.97 | n | n | n |
| P092 | 0.09 | 0 | 0 | 0.16 | 0.27 | 0.11 |
| P094 | 2.55 | 0.8 | 0.61 | 0.82 | 0.45 | n |
| P095 | 8.13 | 0.70 | 0.57 | 0.27 | 0 | n |
| P170 | 7.80 | 0.98 | 0.37 | 0.38 | n | n |
| P176 | 12.4 | 1 | 0.09 | 0.06 | n | n |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balázs, K.; Kocsis, Z.S.; Ágoston, P.; Jorgo, K.; Gesztesi, L.; Farkas, G.; Székely, G.; Takácsi-Nagy, Z.; Polgár, C.; Sáfrány, G.; et al. Prostate Cancer Survivors Present Long-Term, Residual Systemic Immune Alterations. Cancers 2022, 14, 3058. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14133058
Balázs K, Kocsis ZS, Ágoston P, Jorgo K, Gesztesi L, Farkas G, Székely G, Takácsi-Nagy Z, Polgár C, Sáfrány G, et al. Prostate Cancer Survivors Present Long-Term, Residual Systemic Immune Alterations. Cancers. 2022; 14(13):3058. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14133058
Chicago/Turabian StyleBalázs, Katalin, Zsuzsa S. Kocsis, Péter Ágoston, Kliton Jorgo, László Gesztesi, Gyöngyi Farkas, Gábor Székely, Zoltán Takácsi-Nagy, Csaba Polgár, Géza Sáfrány, and et al. 2022. "Prostate Cancer Survivors Present Long-Term, Residual Systemic Immune Alterations" Cancers 14, no. 13: 3058. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14133058