
A Combination of Sorafenib, an Immune Checkpoint Inhibitor, TACE and Stereotactic Body Radiation Therapy versus Sorafenib and TACE in Advanced Hepatocellular Carcinoma Accompanied by Portal Vein Tumor Thrombus


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
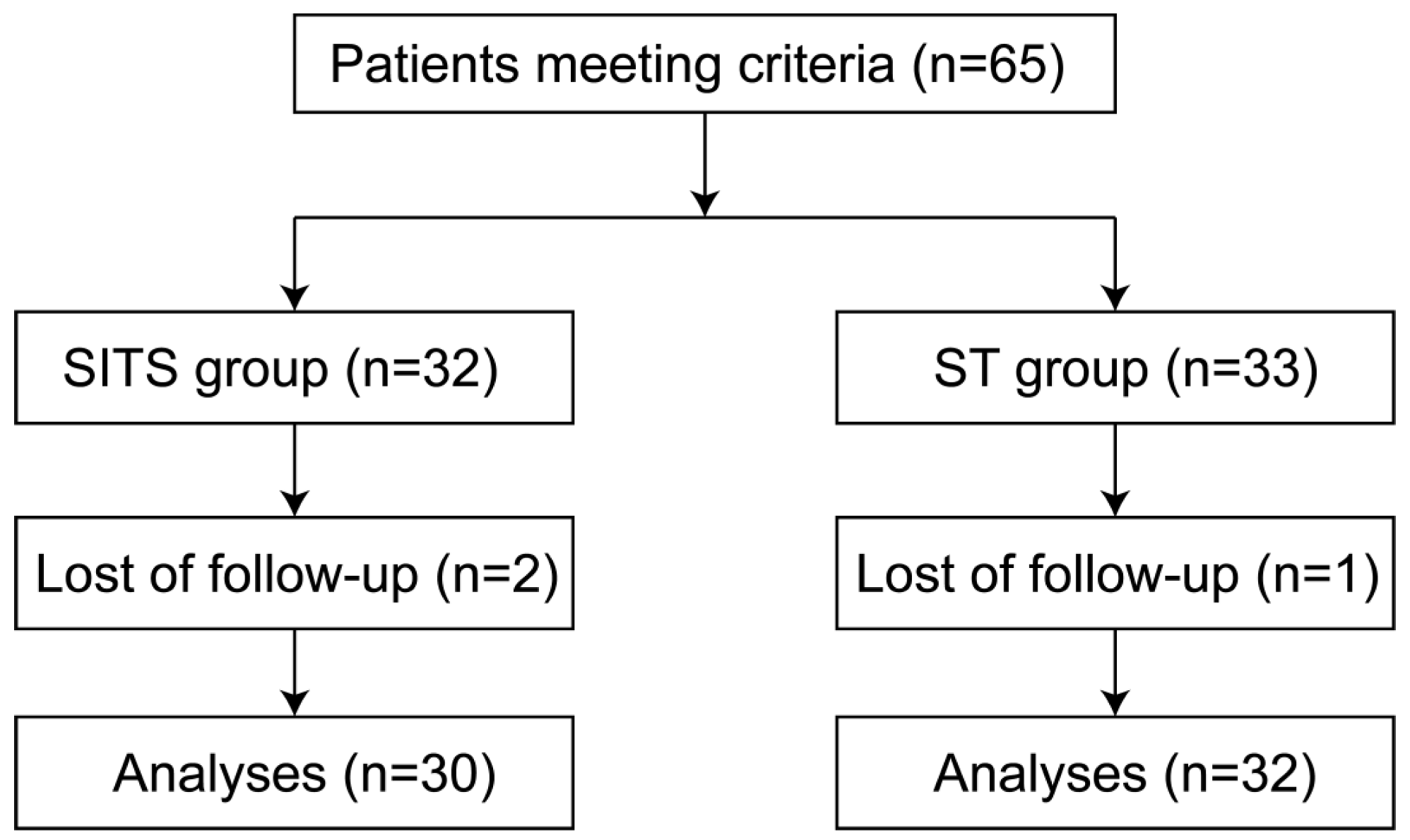
2.1. Patients
2.2. Study Design
2.3. Data Collection and Definitions
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
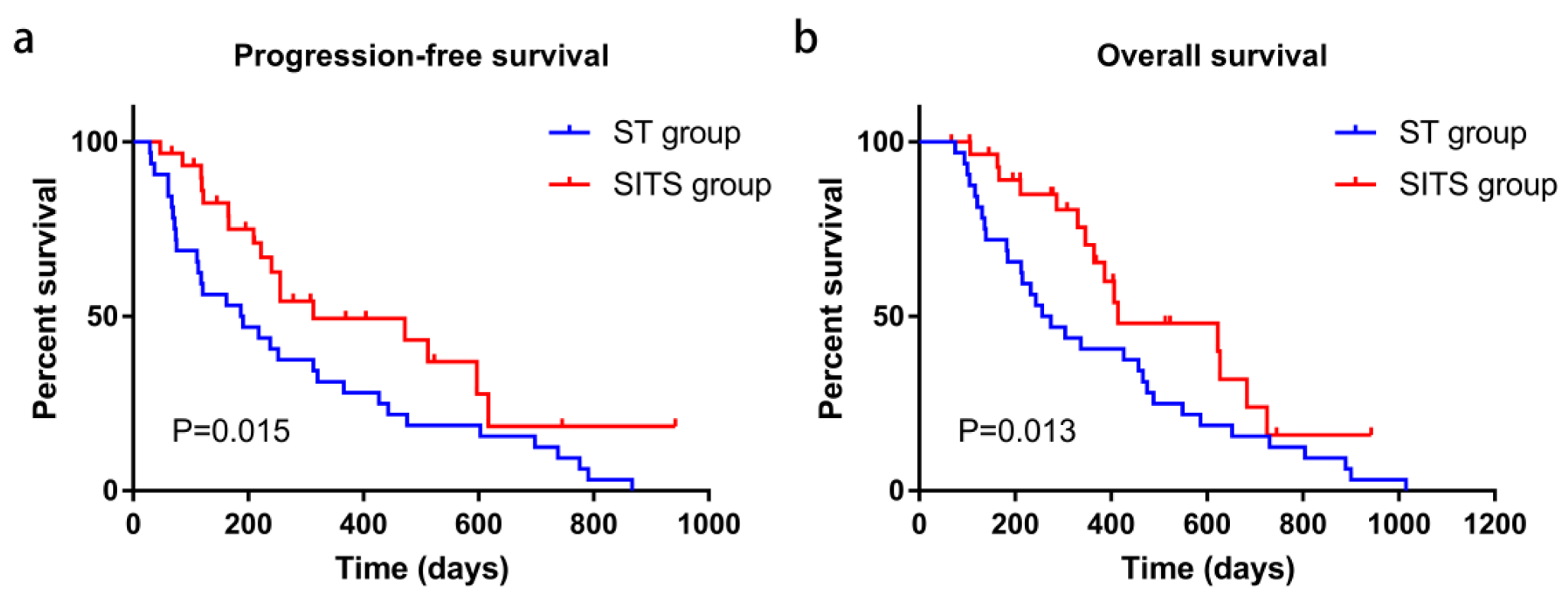
3.2. Effectiveness of the Combination Therapies
3.3. Univariable and Multivariable COX Regression Analyses
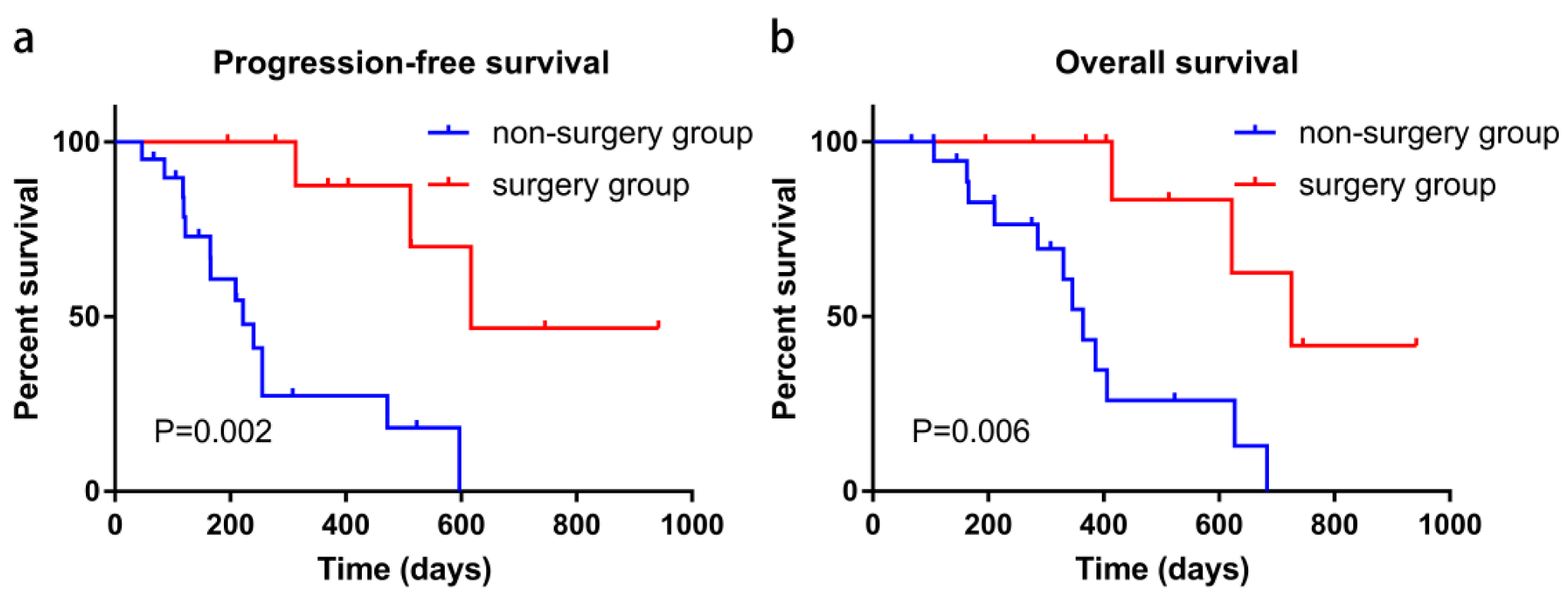
3.4. Role of Secondary Surgery in the SITS Combination Therapy
3.5. AEs of the Combination Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BCLC | the Barcelona Clinic Liver Cancer |
| CT | computed tomography |
| HCC | hepatocellular carcinoma |
| ICI | immune checkpoint inhibitors |
| mRECIST | the modified Response Evaluation Criteria in Solid Tumors |
| NCI-CTCAE | The National Cancer Institute–Common Terminology Criteria for Adverse Events |
| ORR | overall response rate |
| OS | overall survival |
| PFS | progression-free survival |
| PVTT | portal vein tumor thrombus |
| SBRT | stereotactic body radiation therapy |
| SD | standard deviation |
| TACE | transcatheter arterial chemoembolization |
| TKI | tyrosine kinase inhibitor |
References
- Ogasawara, S.; Koroki, K.; Kanzaki, H.; Kobayashi, K.; Kiyono, S.; Nakamura, M.; Kanogawa, N.; Saito, T.; Kondo, T.; Nakagawa, R.; et al. Changes in therapeutic options for hepatocellular carcinoma in Asia. Liver Int. 2021, 42, 2055–2066. [Google Scholar] [CrossRef]
- European Association For The Study Of The Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.-M.; Lai, E.C.; Zhang, C.; Yu, H.-W.; Liu, Z.; Wan, B.-J.; Liu, L.-M.; Tian, Z.-H.; Deng, H.; Sun, Q.-H.; et al. The strategies for treating primary hepatocellular carcinoma with portal vein tumor thrombus. Int. J. Surg. 2015, 20, 8–16. [Google Scholar] [CrossRef]
- Mähringer-Kunz, A.; Steinle, V.; Düber, C.; Weinmann, A.; Koch, S.; Schmidtmann, I.; Schotten, S.; Hinrichs, J.B.; Graafen, D.; Pinto dos Santos, D.; et al. Extent of portal vein tumour thrombosis in patients with hepatocellular carcinoma: The more, the worse? Liver Int. 2019, 39, 324–331. [Google Scholar] [CrossRef]
- Cheng, S.; Chen, M.; Cai, J.; Sun, J.; Guo, R.; Bi, X.; Lau, W.Y.; Wu, M.; on behalf of Chinese Association of Liver Cancer and Chinese Medical Doctor Association. Chinese Expert Consensus on Multidisciplinary Diagnosis and Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombus (2018 Edition). Liver Cancer 2020, 9, 28–40. [Google Scholar] [CrossRef]
- Luo, F.; Li, M.; Ding, J.; Zheng, S. The Progress in the Treatment of Hepatocellular Carcinoma With Portal Vein Tumor Thrombus. Front. Oncol. 2021, 11, 635731. [Google Scholar] [CrossRef]
- Huang, Y.; Zhang, Z.; Liao, W.; Hu, K.; Wang, Z. Combination of Sorafenib, Camrelizumab, Transcatheter Arterial Chemoembolization, and Stereotactic Body Radiation Therapy as a Novel Downstaging Strategy in Advanced Hepatocellular Carcinoma With Portal Vein Tumor Thrombus: A Case Series Study. Front. Oncol. 2021, 11, 650394. [Google Scholar] [CrossRef]
- Shi, J.; Lai, E.C.H.; Li, N.; Guo, W.-X.; Xue, J.; Lau, W.Y.; Wu, M.-C.; Cheng, S.-Q. Surgical Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombus. Ann. Surg. Oncol. 2010, 17, 2073–2080. [Google Scholar] [CrossRef]
- European Association For The Study Of The Liver. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [Green Version]
- Cannella, R.; Taibbi, A.; Porrello, G.; Burgio, M.D.; Cabibbo, G.; Bartolotta, T.V. Hepatocellular carcinoma with macrovascular invasion: Multimodality imaging features for the diagnosis. Diagn. Interv. Radiol. 2020, 26, 531–540. [Google Scholar] [CrossRef]
- Roderburg, C.; Özdirik, B.; Wree, A.; Demir, M.; Tacke, F. Systemic treatment of hepatocellular carcinoma: From sorafenib to combination therapies. Hepatic Oncol. 2020, 7, P20. [Google Scholar] [CrossRef]
- Li, X.; Wang, Y.; Ye, X.; Liang, P. Locoregional Combined With Systemic Therapies for Advanced Hepatocellular Carcinoma: An Inevitable Trend of Rapid Development. Front. Mol. Biosci. 2021, 8, 635243. [Google Scholar] [CrossRef]
- Wu, F.-X.; Chen, J.; Bai, T.; Zhu, S.-L.; Yang, T.-B.; Qi, L.-N.; Zou, L.; Li, Z.-H.; Ye, J.-Z.; Li, L.-Q. The safety and efficacy of transarterial chemoembolization combined with sorafenib and sorafenib mono-therapy in patients with BCLC stage B/C hepatocellular carcinoma. BMC Cancer 2017, 17, 645. [Google Scholar] [CrossRef]
- Shuanggang, C.; Shen, L.; Qiu, Z.; Qi, H.; Cao, F.; Xie, L.; Fan, W. Transarterial chemoembolization combined with microwave ablation and apatinib in patients with Barcelona clinic liver cancer Stage C hepatocellular carcinoma: A propensity score matching analysis. J. Cancer Res. Ther. 2020, 16, 250–257. [Google Scholar]
- Meng, M.; Li, W.; Yang, X.; Huang, G.; Wei, Z.; Ni, Y.; Han, X.; Wang, J.; Ye, X. Transarterial chemoembolization, ablation, tyrosine kinase inhibitors, and immunotherapy (TATI): A novel treatment for patients with advanced hepatocellular carcinoma. J. Cancer Res. Ther. 2020, 16, 327–334. [Google Scholar]
- Hughes, P.E.; Caenepeel, S.; Wu, L.C. Targeted Therapy and Checkpoint Immunotherapy Combinations for the Treatment of Cancer. Trends Immunol. 2016, 37, 462–476. [Google Scholar] [CrossRef]
- Frederick, D.T.; Piris, A.; Cogdill, A.P.; Cooper, Z.A.; Lezcano, C.; Ferrone, C.R.; Mitra, D.; Boni, A.; Newton, L.P.; Liu, C.; et al. BRAF Inhibition Is Associated with Enhanced Melanoma Antigen Expression and a More Favorable Tumor Microenvironment in Patients with Metastatic Melanoma. Clin. Cancer Res. 2013, 19, 1225–1231. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, S.; Sho, M.; Yamato, I.; Yoshiji, H.; Wakatsuki, K.; Nishiwada, S.; Yagita, H.; Nakajima, Y. Simultaneous blockade of programmed death 1 and vascular endothelial growth factor receptor 2 (VEGFR2) induces synergistic anti-tumour effect in vivo. Clin. Exp. Immunol. 2013, 172, 500–506. [Google Scholar] [CrossRef]
- Spranger, S.; Bao, R.; Gajewski, T.F. Melanoma-intrinsic β-catenin signalling prevents anti-tumour immunity. Nature 2015, 523, 231–235. [Google Scholar] [CrossRef]
- Peng, W.; Chen, J.Q.; Liu, C.; Malu, S.; Creasy, C.; Tetzlaff, M.T.; Xu, C.; McKenzie, J.A.; Zhang, C.; Liang, X.; et al. Loss of PTEN Promotes Resistance to T Cell–Mediated Immunotherapy. Cancer Discov. 2016, 6, 202–216. [Google Scholar] [CrossRef] [Green Version]
- Chiappinelli, K.B.; Zahnow, C.A.; Ahuja, N.; Baylin, S.B. Combining Epigenetic and Immunotherapy to Combat Cancer. Cancer Res. 2016, 76, 1683–1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagarsheth, N.; Peng, D.; Kryczek, I.; Wu, K.; Li, W.; Zhao, E.; Zhao, L.; Wei, S.; Frankel, T.; Vatan, L.; et al. PRC2 Epigenetically Silences Th1-Type Chemokines to Suppress Effector T-Cell Trafficking in Colon Cancer. Cancer Res. 2016, 76, 275–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, D.; Kryczek, I.; Nagarsheth, N.; Zhao, L.; Wei, S.; Wang, W.; Sun, Y.; Zhao, E.; Vatan, L.; Szeliga, W.; et al. Epigenetic silencing of TH1-type chemokines shapes tumour immunity and immunotherapy. Nature 2015, 527, 249–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubas, M.J.; Kumar, S.S. The Combined Use of SBRT and Immunotherapy—A Literature Review. Curr. Oncol. Rep. 2020, 22, 117. [Google Scholar] [CrossRef]
- Sharabi, A.B.; Lim, M.; DeWeese, T.L.; Drake, C.G. Radiation and checkpoint blockade immunotherapy: Radiosensitisation and potential mechanisms of synergy. Lancet Oncol. 2015, 16, e498–e509. [Google Scholar] [CrossRef]
- Hatzidakis, A.; Müller, L.; Krokidis, M.; Kloeckner, R. Local and Regional Therapies for Hepatocellular Carcinoma and Future Combinations. Cancers 2022, 14, 2469. [Google Scholar] [CrossRef]
- Jacob, R.; Turley, F.; Redden, D.T.; Saddekni, S.; Aal, A.K.; Keene, K.; Yang, E.; Zarzour, J.; Bolus, D.; Smith, J.K.; et al. Adjuvant stereotactic body radiotherapy following transarterial chemoembolization in patients with non-resectable hepatocellular carcinoma tumours of ≥3 cm. HPB 2015, 17, 140–149. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Romasanta, L.A.; Portillo, E.G.-D.; Rodríguez-Gutiérrez, A.; Matías-Pérez, Á. Stereotactic Radiotherapy for Hepatocellular Carcinoma, Radiosensitization Strategies and Radiation-Immunotherapy Combination. Cancers 2021, 13, 192. [Google Scholar] [CrossRef]
- Lau, W.Y.; Lai, E.C.H. Salvage Surgery Following Downstaging of Unresectable Hepatocellular Carcinoma—A Strategy to Increase Resectability. Ann. Surg. Oncol. 2007, 14, 3301–3309. [Google Scholar] [CrossRef]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Sia, D.; Jiao, Y.; Martinez-Quetglas, I.; Kuchuk, O.; Villacorta-Martin, C.; de Moura, M.C.; Putra, J.; Campreciós, G.; Bassaganyas, L.; Akers, N.; et al. Identification of an Immune-specific Class of Hepatocellular Carcinoma, Based on Molecular Features. Gastroenterology 2017, 153, 812–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | ST Group (n = 32) | SITS Group (n = 30) | p-Value |
|---|---|---|---|
| Age (years) | 51.00 (40.50, 61.00) | 52.00 (43.25, 59.25) | 0.555 |
| Gender | 0.418 | ||
| Male | 30 (93.8) | 26 (86.7) | |
| Female | 2 (6.3) | 4 (13.3) | |
| HBsAg | 0.613 | ||
| Positive | 29 (90.6) | 29 (96.7) | |
| Negative | 3 (9.4) | 1 (3.3) | |
| Liver cirrhosis | 0.101 | ||
| Yes | 29 (90.6) | 22 (73.3) | |
| No | 3 (9.4) | 8 (26.7) | |
| Tumor size (cm) | 7.85 (6.10, 11.63) | 9.00 (7.00, 13.28) | 0.302 |
| Number of tumors | 0.799 | ||
| Single | 14 (43.8) | 15 (50.0) | |
| Multiple | 18 (56.2) | 15 (50.0) | |
| Cheng’s PVTT classification | 0.367 | ||
| I | 5 (15.6) | 2 (6.7) | |
| II | 13 (40.6) | 17 (56.7) | |
| III | 14 (43.8) | 11 (36.7) | |
| AFP (ng/mL) | 0.311 | ||
| ≤400 | 15 (46.9) | 10 (33.3) | |
| >400 | 17 (53.1) | 20 (66.7) | |
| Albumin (g/L) | 37.90 (33.80, 42.38) | 39.90 (34.90, 42.63) | 0.423 |
| Total Bilirubin (μmol/L) | 15.55 (10.95, 29.45) | 15.50 (10.38, 21.75) | 0.073 |
| Prothrombin Time (s) | 13.95 (12.38, 14.78) | 13.05 (12.28, 13.73) | 0.130 |
| Child–Pugh classification | 0.197 | ||
| A | 27 (84.4) | 29 (96.7) | |
| B | 5 (15.6) | 1 (3.3) | |
| ICI | - | ||
| Camrelizumab | - | 22 (73.3) | |
| Tislelizumab | - | 8 (26.7) |
| Characteristic | ST Group (n = 32) | SITS Group (n = 30) | p-Value |
|---|---|---|---|
| Best overall response | 0.020 | ||
| Complete response | 0 (0.0) | 6 (20.0) | |
| Partial response | 8 (25.0) | 10 (33.3) | |
| Stable disease | 9 (28.1) | 7 (23.3) | |
| Progressive disease | 15 (46.9) | 7 (23.3) | |
| Objective response rate | 8 (25.0) | 16 (53.3) | 0.036 |
| Disease control rate | 17 (53.1) | 23 (76.7) | 0.067 |
| Successful downstaging | 0 (0.0) | 12 (40.0) | - |
| Variable | PFS | |
|---|---|---|
| HR (95% CI) | p-Value | |
| Univariable analysis | ||
| Age (years) | 0.979 (0.956, 1.002) | 0.072 |
| Gender (male vs. female) | 1.437 (0.560, 3.686) | 0.451 |
| HBsAg (positive vs. negative) | 1.268 (0.390, 4.120) | 0.693 |
| Liver cirrhosis (yes vs. no) | 0.800 (0.544, 1.177) | 0.257 |
| Tumor size (cm) | 1.066 (0.987, 1.150) | 0.103 |
| Number of tumors (multiple vs. single) | 1.828 (1.028, 3.250) | 0.040 |
| Cheng’s PVTT classification | ||
| II vs. I | 0.663 (0.282, 1.560) | 0.346 |
| III vs. I | 0.928 (0.388, 2.221) | 0.868 |
| AFP (>400 vs. ≤400) | 1.269 (0.711, 2.265) | 0.420 |
| Albumin (g/L) | 1.025 (0.972, 1.082) | 0.360 |
| Total Bilirubin (μmol/L) | 1.009 (0.980, 1.037) | 0.555 |
| Prothrombin Time (s) | 0.873 (0.699, 1.090) | 0.229 |
| Child–Pugh classification (B vs. A) | 2.396 (1.001, 5.740) | 0.049 |
| Combination therapy (SITS vs. ST) | 0.522 (0.288, 0.946) | 0.032 |
| Multivariable analyses | ||
| Age (years) | 0.985 (0.961, 1.010) | 0.251 |
| Number of tumors (multiple vs. single) | 2.241 (1.147, 4.375) | 0.018 |
| Child–Pugh classification (B vs. A) | 3.373 (1.308, 8.697) | 0.012 |
| Combination therapy (SITS vs. ST) | 0.462 (0.252, 0.845) | 0.012 |
| Variable | OS | |
|---|---|---|
| HR (95% CI) | p-Value | |
| Univariable analyses | ||
| Age (years) | 0.984 (0.961, 1.008) | 0.192 |
| Gender (male vs. female) | 1.154 (0.722, 1.842) | 0.550 |
| HBsAg (positive vs. negative) | 1.095 (0.336, 3.563) | 0.881 |
| Liver cirrhosis (yes vs. no) | 0.817 (0.542, 1.231) | 0.334 |
| Tumor size (cm) | 1.072 (0.989, 1.161) | 0.092 |
| Number of tumors (multiple vs. single) | 1.708 (0.944, 3.092) | 0.077 |
| Cheng’s PVTT classification | ||
| II vs. I | 0.673 (0.285, 1.586) | 0.365 |
| III vs. I | 0.828 (0.340, 2.018) | 0.678 |
| AFP (>400 vs. ≤400) | 1.341 (0.735, 2.447) | 0.338 |
| Albumin (g/L) | 1.028 (0.971, 1.090) | 0.342 |
| Total Bilirubin (μmol/L) | 1.008 (0.979, 1.038) | 0.591 |
| Prothrombin Time (s) | 0.876 (0.699, 1.099) | 0.253 |
| Child–Pugh classification (B vs. A) | 2.524 (1.051, 6.062) | 0.038 |
| Combination therapy (SITS vs. ST) | 0.541 (0.290, 1.008) | 0.053 |
| Multivariable analyses | ||
| Tumor size (cm) | 1.087 (0.994, 1.190) | 0.068 |
| Number of tumors (multiple vs. single) | 1.880 (0.935, 3.782) | 0.077 |
| Child–Pugh classification (B vs. A) | 5.241 (1.878, 14.628) | 0.002 |
| Combination therapy (SITS vs. ST) | 0.478 (0.256, 0.893) | 0.021 |
| Characteristic | ST Group (n = 32) | SITS Group (n = 30) | p-Value |
|---|---|---|---|
| Incidence of adverse events | 15 (46.9) | 23 (76.7) | 0.020 |
| Fever | 8 | 10 | |
| Skin reaction | 7 | 7 | |
| Fatigue | 2 | 4 | |
| Diarrhea | 0 | 3 | |
| Vomiting | 1 | 3 | |
| Reduction of platelet | 0 | 2 | |
| Hypertension | 2 | 2 | |
| Headache | 0 | 2 | |
| Level III or IV adverse events | 0 | 2 (6.7) | - |
| Readmission for adverse events | 0 | 0 | - |
| Death due to adverse events | 0 | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Li, C.; Liao, W.; Huang, Y.; Wang, Z. A Combination of Sorafenib, an Immune Checkpoint Inhibitor, TACE and Stereotactic Body Radiation Therapy versus Sorafenib and TACE in Advanced Hepatocellular Carcinoma Accompanied by Portal Vein Tumor Thrombus. Cancers 2022, 14, 3619. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153619
Zhang Z, Li C, Liao W, Huang Y, Wang Z. A Combination of Sorafenib, an Immune Checkpoint Inhibitor, TACE and Stereotactic Body Radiation Therapy versus Sorafenib and TACE in Advanced Hepatocellular Carcinoma Accompanied by Portal Vein Tumor Thrombus. Cancers. 2022; 14(15):3619. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153619
Chicago/Turabian StyleZhang, Zeyu, Chan Li, Weijun Liao, Yun Huang, and Zhiming Wang. 2022. "A Combination of Sorafenib, an Immune Checkpoint Inhibitor, TACE and Stereotactic Body Radiation Therapy versus Sorafenib and TACE in Advanced Hepatocellular Carcinoma Accompanied by Portal Vein Tumor Thrombus" Cancers 14, no. 15: 3619. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153619