
Specialist versus Primary Care Prostate Cancer Follow-Up: A Process Evaluation of a Randomized Controlled Trial

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
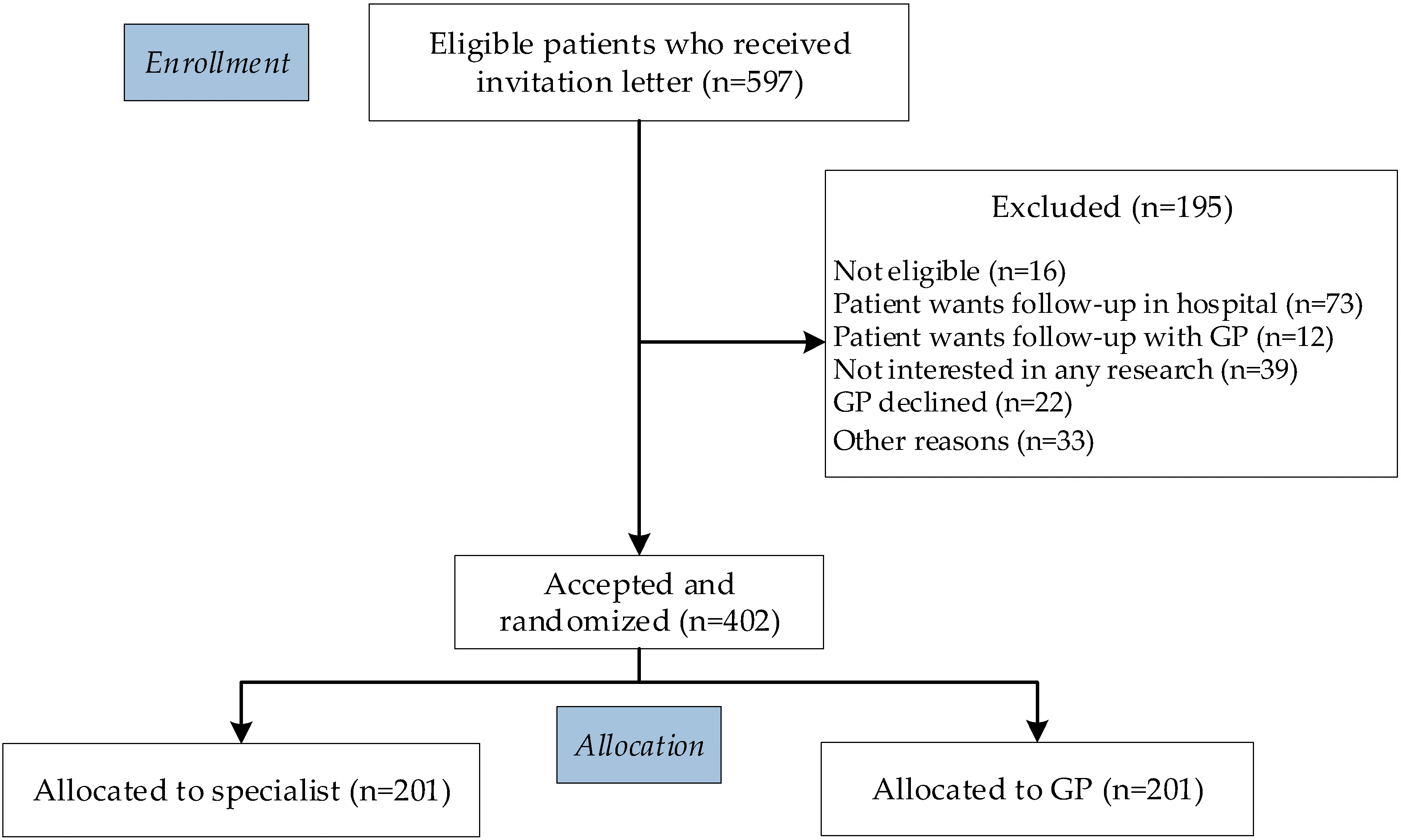
2.1. Design and Study Population
2.2. Data Collection
2.3. Study Procedures
2.4. Data Analysis
3. Results
3.1. Interviews
3.2. Structure of Prostate Cancer Follow-Up Care
3.3. Communication between Primary and Secondary Care
3.4. Clinical Competencies of Primary Care Follow-Up
3.5. Facilitators of Primary Care-Based Follow-Up
3.6. Barriers to Primary Care-Based Follow-Up
3.7. Organizational Requirements for the Implementation of Primary Care-Based Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carioli, G.; Bertuccio, P.; Boffetta, P.; Levi, F.; La Vecchia, C.; Negri, E.; Malvezzi, M. European cancer mortality predictions for the year 2020 with a focus on prostate cancer. Ann. Oncol. 2020, 31, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Urquhart, R.; Cordoba, W.; Bender, J.; Cuthbert, C.; Easley, J.; Howell, D.; Kaal, J.; Kendell, C.; Radford, S.; Sussman, J. Risk Stratification and Cancer Follow-Up: Towards More Personalized Post-Treatment Care in Canada. Curr. Oncol. 2022, 29, 3215–3223. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; van der Kwast, T.H.; Lam, T.B.; et al. Guidelines on Prostate Cancer. 2021. Available online: https://uroweb.org/guideline/prostate-cancer/ (accessed on 11 April 2022).
- Nekhlyudov, L.; Mollica, M.A.; Jacobsen, P.B.; Mayer, D.K.; Shulman, L.N.; Geiger, A.M. Developing a Quality of Cancer Survivorship Care Framework: Implications for Clinical Care, Research, and Policy. J. Natl. Cancer Inst. 2019, 111, 1120–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milonas, D.; Ruzgas, T.; Venclovas, Z.; Jievaltas, M.; Joniau, S. Impact of Grade Groups on Prostate Cancer-Specific and Other-Cause Mortality: Competing Risk Analysis from a Large Single Institution Series. Cancers 2021, 13, 1963. [Google Scholar] [CrossRef]
- Wollersheim, B.M.; van Asselt, K.M.; van der Poel, H.G.; van Weert, H.; Hauptmann, M.; Retèl, V.P.; Aaronson, N.K.; van de Poll-Franse, L.V.; Boekhout, A.H. Design of the PROstate cancer follow-up care in Secondary and Primary hEalth Care study (PROSPEC): A randomized controlled trial to evaluate the effectiveness of primary care-based follow-up of localized prostate cancer survivors. BMC Cancer 2020, 20, 635. [Google Scholar] [CrossRef]
- Hulscher, M.; Laurant, M.; Grol, R. Process evaluation of implementation strategies. In Improving Patient Care: The Implementation of Change in Health Care; Grol, R., Wensing, M., Eccles, M., Davis, D., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2013; pp. 333–349. [Google Scholar]
- Oakley, A.; Strange, V.; Bonell, C.; Allen, E.; Stephenson, J. Process evaluation in randomised controlled trials of complex interventions. BMJ 2006, 332, 413–416. [Google Scholar] [CrossRef] [Green Version]
- Grol, R.P.; Bosch, M.C.; Hulscher, M.E.; Eccles, M.P.; Wensing, M. Planning and studying improvement in patient care: The use of theoretical perspectives. Milbank Q. 2007, 85, 93–138. [Google Scholar] [CrossRef] [Green Version]
- Huibertse, L.J.; van Eenbergen, M.; de Rooij, B.H.; Bastiaens, M.T.; Fossion, L.M.; de la Fuente, R.B.; Kil, P.J.; Koldewijn, E.L.; Meier, A.H.; Mommers, R.J.; et al. Cancer survivors’ preference for follow-up care providers: A cross-sectional study from the population-based PROFILES-registry. Acta Oncol. 2017, 56, 278–287. [Google Scholar] [CrossRef] [Green Version]
- Brandenbarg, D.; Roorda, C.; Stadlander, M.; de Bock, G.H.; Berger, M.Y.; Berendsen, A.J. Patients’ views on general practitioners’ role during treatment and follow-up of colorectal cancer: A qualitative study. Fam. Pract. 2017, 34, 234–238. [Google Scholar] [CrossRef]
- Smith, T.G.; Strollo, S.; Hu, X.; Earle, C.C.; Leach, C.R.; Nekhlyudov, L. Understanding Long-Term Cancer Survivors’ Preferences for Ongoing Medical Care. J. Gen. Intern. Med. 2019, 34, 2091–2097. [Google Scholar] [CrossRef]
- Mayo, S.J.; Ajaj, R.; Drury, A. Survivors’ preferences for the organization and delivery of supportive care after treatment: An integrative review. Eur. J. Oncol. Nurs. 2021, 54, 102040. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.A.; McLoone, J.K.; Wakefield, C.E.; Cohn, R.J. Primary Care Physicians’ Perspectives of Their Role in Cancer Care: A Systematic Review. J. Gen. Intern. Med. 2016, 31, 1222–1236. [Google Scholar] [CrossRef] [PubMed]
- Fidjeland, H.L.; Brekke, M.; Vistad, I. General practitioners’ attitudes toward follow-up after cancer treatment: A cross-sectional questionnaire study. Scand. J. Prim. Health Care 2015, 33, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Wind, J.; Duineveld, L.A.; van der Heijden, R.P.; van Asselt, K.M.; Bemelman, W.A.; van Weert, H.C. Follow-up after colon cancer treatment in the Netherlands; a survey of patients, GPs, and colorectal surgeons. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2013, 39, 837–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. IS 2009, 4, 50–65. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Huang, R. RQDA: R-Based Qualitative Data Analysis. Available online: http://rqda.r-forge.r-project.org (accessed on 24 February 2021).
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 24 February 2021).
- Grunfeld, E.; Levine, M.N.; Julian, J.A.; Coyle, D.; Szechtman, B.; Mirsky, D.; Verma, S.; Dent, S.; Sawka, C.; Pritchard, K.I.; et al. Randomized trial of long-term follow-up for early-stage breast cancer: A comparison of family physician versus specialist care. J. Clin. Oncol. 2006, 24, 848–855. [Google Scholar] [CrossRef]
- Grunfeld, E.; Mant, D.; Yudkin, P.; Adewuyi-Dalton, R.; Cole, D.; Stewart, J.; Fitzpatrick, R.; Vessey, M. Routine follow up of breast cancer in primary care: Randomised trial. BMJ (Clin. Res. Ed.) 1996, 313, 665–669. [Google Scholar] [CrossRef] [Green Version]
- Wattchow, D.A.; Weller, D.P.; Esterman, A.; Pilotto, L.S.; McGorm, K.; Hammett, Z.; Platell, C.; Silagy, C. General practice vs. surgical-based follow-up for patients with colon cancer: Randomised controlled trial. Br. J. Cancer 2006, 94, 1116–1121. [Google Scholar] [CrossRef] [Green Version]
- Wollersheim, B.M.; Helweg, E.; Tillier, C.N.; van Muilekom, H.A.M.; de Blok, W.; van der Poel, H.G.; van Asselt, K.M.; Boekhout, A.H. The role of routine follow-up visits of prostate cancer survivors in addressing supportive care and information needs: A qualitative observational study. Supportive Care Cancer 2021, 29, 6449–6457. [Google Scholar] [CrossRef]
- Hudson, S.V.; Ohman-Strickland, P.A.; Bator, A.; O’Malley, D.; Gundersen, D.; Lee, H.S.; Crabtree, B.F.; Miller, S.M. Breast and prostate cancer survivors’ experiences of patient-centered cancer follow-up care from primary care physicians and oncologists. J. Cancer Surviv. Res. Pract. 2016, 10, 906–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridd, M.; Shaw, A.; Lewis, G.; Salisbury, C. The patient-doctor relationship: A synthesis of the qualitative literature on patients’ perspectives. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2009, 59, e116–e133. [Google Scholar] [CrossRef] [PubMed]
- Street, R.L., Jr.; Gordon, H.S.; Ward, M.M.; Krupat, E.; Kravitz, R.L. Patient participation in medical consultations: Why some patients are more involved than others. Med. Care 2005, 43, 960–969. [Google Scholar] [CrossRef]
- Margariti, C.; Gannon, K.N.; Walsh, J.J.; Green, J.S.A. GP experience and understandings of providing follow-up care in prostate cancer survivors in England. Health Soc. Care Community 2020, 28, 1468–1478. [Google Scholar] [CrossRef] [PubMed]
- Geramita, E.M.; Parker, I.R.; Brufsky, J.W.; Diergaarde, B.; van Londen, G.J. Primary Care Providers’ Knowledge, Attitudes, Beliefs, and Practices Regarding Their Preparedness to Provide Cancer Survivorship Care. J. Cancer Educ. 2020, 35, 1219–1226. [Google Scholar] [CrossRef]
- Taylor, S.; Johnson, H.; Peat, S.; Booker, J.; Yorke, J. Exploring the experiences of patients, general practitioners and oncologists of prostate cancer follow-up: A qualitative interview study. Eur. J. Oncol. Nurs. 2020, 48, 101820. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Components | Definition | Source |
|---|---|---|
| Reach | The number and proportion of the target population participating in this intervention | Research logbook |
| CFIR Domains | Definition | Source |
| Intervention characteristics | The characteristics of the intervention when implemented in an organization | Qualitative interview questions |
| Outer setting characteristics | The political and social context within which an organization resides | Qualitative interview questions |
| Inner setting characteristics | The structural, political and cultural context through which the implementation process will proceed | Qualitative interview questions |
| Individual characteristics | The knowledge, beliefs, attitudes and expectations of the individuals involved in the intervention | Qualitative interview questions |
| Implementation process | Processes and change that are needed for a successful implementation | Qualitative interview questions |
| Phase | Coding method | Performed by |
|---|---|---|
| 1. Familiarizing yourself with your data | BW, EA, SC | |
| 2. Generating initial codes | Inductive approach | BW, EA, SC |
| Iterative process | Consensus-based codebook | BW, EA, SC |
| Review | Consensus-based codebook | BW, EA, SC, AB |
| Data saturation | Final codebook | BW, EA, SC, AB |
| 3. Searching for themes | Using CFIR framework | BW, EA, SC |
| 4. Reviewing themes | Using CFIR framework | BW, EA, SC |
| 5. Defining and naming themes | Using CFIR framework | BW, EA, SC, AB |
| 6. Producing the report | BW, AB |
| Demographics | Patients, n = 15 (%) | GPs, n = 10 (%) | Specialists, n = 8 (%) |
|---|---|---|---|
| Age at interview in years, M (SD) | 67 (6) | 53 (10) | 47 (7) |
| Sex | -- | ||
| Female | -- | 4 (40) | 0 (0) |
| Male | 15 (100) | 6 (60) | 8 (100) |
| Marital status | -- | -- | |
| Partner | 14 (93) | ||
| No partner | 1 (7) | ||
| Educational level a | -- | -- | |
| Low | 3 (20) | ||
| Intermediate | 1 (7) | ||
| High | 11 (73) | ||
| Clinical characteristics | |||
| Primary treatment | -- | -- | |
| Radical prostatectomy | 13 (87) | ||
| Radiotherapy | 2 (13) | ||
| ADT | 1 (7) | ||
| Time since treatment in months, M (range) | 20 (17–25) | -- | -- |
| LPC risk group b | -- | -- | |
| Low | 5 (33) | ||
| Intermediate | 5 (33) | ||
| High | 5 (33) | ||
| Information healthcare professionals | |||
| Type GP practice | -- | -- | |
| Duo practice | 5 (50) | ||
| Group practice | 5 (50) | ||
| Type of healthcare professional | -- | -- | |
| Urologist | 5 (62) | ||
| Radiation Oncologist | 2 (25) | ||
| Physician Assistant | 1 (13) | ||
| Type of hospital | -- | -- | |
| Academic hospital | 1 (12) | ||
| Top clinical hospital | 3 (38) | ||
| Comprehensive cancer center | 3 (38) | ||
| Community hospital | 1 (12) |
| Theme | Quotes (Examples) |
|---|---|
| Structure of prostate cancer follow-up care | P3: ‘Once my wife was also very worried, and then I had my PSA checked because it does not help me if she gets nervous.’ |
| GP3: ‘I see this person more often for all sorts of reasons, so sometimes it happened that I just, ehm, combined it (i.e., follow-up consult) with complaints of his respiratory system or something like that.’ | |
| S8: ‘We also offer people a psychologist or social worker, if there is a need. But the physical and oncological examination are the main aspects.’ | |
| Communication between primary and secondary care | P1: ‘No, I did not experience any of that (i.e., communication).’ |
| GP9: ‘In general, it is always difficult to reach a specialist, or you will be called back but not at the moment the patient is with you.’ | |
| S6: ‘No, I have never heard anything from the GPs. That shows how redundant we really are, at least for this part (i.e., follow-up).’ | |
| Clinical competencies of primary care-based follow-up | P4: ‘What the GP did well, I must say, was covering everything…like, how is it going physically, how is it going psychologically, do you have specific questions at a physical level, about urinary incontinence or erectile dysfunction, or are you tired, or do you still have…?’ |
| GP8: ‘Especially information about prognosis, what are the chances that things can come back, I cannot of course, 1,2,3, I do not have those numbers ready of course, no.’ | |
| S2: ‘I have actually had no feedback from GPs who said, ‘’Hey, I have a patient here with erectile problems and I am not sure what to do.” Or you (i.e., study team) provide GPs with excellent information about this, or they do not have questions, or they do not call us. I am not quite sure.’ | |
| Facilitators of primary care-based follow-up | P5: ‘And compared to the hospital, you know… Emotionally that is better. Better to do this (i.e., follow-up) with your GP. And when that is an option, then that is very positive.’ |
| GP5: ‘Well, I think it is very patient-friendly when he does not have to go to the hospital, it will save costs, the effort for me is little, and it is also pleasant for me that I can speak twice a year to someone who had prostate cancer.’ | |
| S3: ‘It really results in extra time in which you can take care of people with bigger problems, who really need the hospital setting.’ | |
| Barriers to primary care-based follow-up | P13: ‘Yes, with the GP you have to undertake action yourself. That is, you know, a GP does not have a system to call people, so if you have complaints you have to go to the GP yourself.’ |
| GP1: ‘The disadvantage is that we do not get one extra penny for it. But I do believe that, uh, primary care is capable of doing this. But then we kind of need… or then we should receive compensation or extra staffing.’ | |
| S1: ‘That is my fear you know, that they (i.e., GPs) will not refer them (i.e., patients) back. Or that they are too late, or not frequently measure their PSA. And then we will lose the window of curability.’ | |
| Organizational requirement for the implementation | See text |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wollersheim, B.M.; van Asselt, K.M.; Pos, F.J.; Akdemir, E.; Crouse, S.; van der Poel, H.G.; Aaronson, N.K.; van de Poll-Franse, L.V.; Boekhout, A.H. Specialist versus Primary Care Prostate Cancer Follow-Up: A Process Evaluation of a Randomized Controlled Trial. Cancers 2022, 14, 3166. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14133166
Wollersheim BM, van Asselt KM, Pos FJ, Akdemir E, Crouse S, van der Poel HG, Aaronson NK, van de Poll-Franse LV, Boekhout AH. Specialist versus Primary Care Prostate Cancer Follow-Up: A Process Evaluation of a Randomized Controlled Trial. Cancers. 2022; 14(13):3166. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14133166
Chicago/Turabian StyleWollersheim, Barbara M., Kristel M. van Asselt, Floris J. Pos, Emine Akdemir, Shifra Crouse, Henk G. van der Poel, Neil K. Aaronson, Lonneke V. van de Poll-Franse, and Annelies H. Boekhout. 2022. "Specialist versus Primary Care Prostate Cancer Follow-Up: A Process Evaluation of a Randomized Controlled Trial" Cancers 14, no. 13: 3166. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14133166