
Trimodal Therapy in Esophageal Squamous Cell Carcinoma: Role of Adjuvant Therapy Following Neoadjuvant Chemoradiation and Surgery

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Neoadjuvant Therapy
2.3. Surgical Procedure and Pathology
2.4. Adjuvant Therapy
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
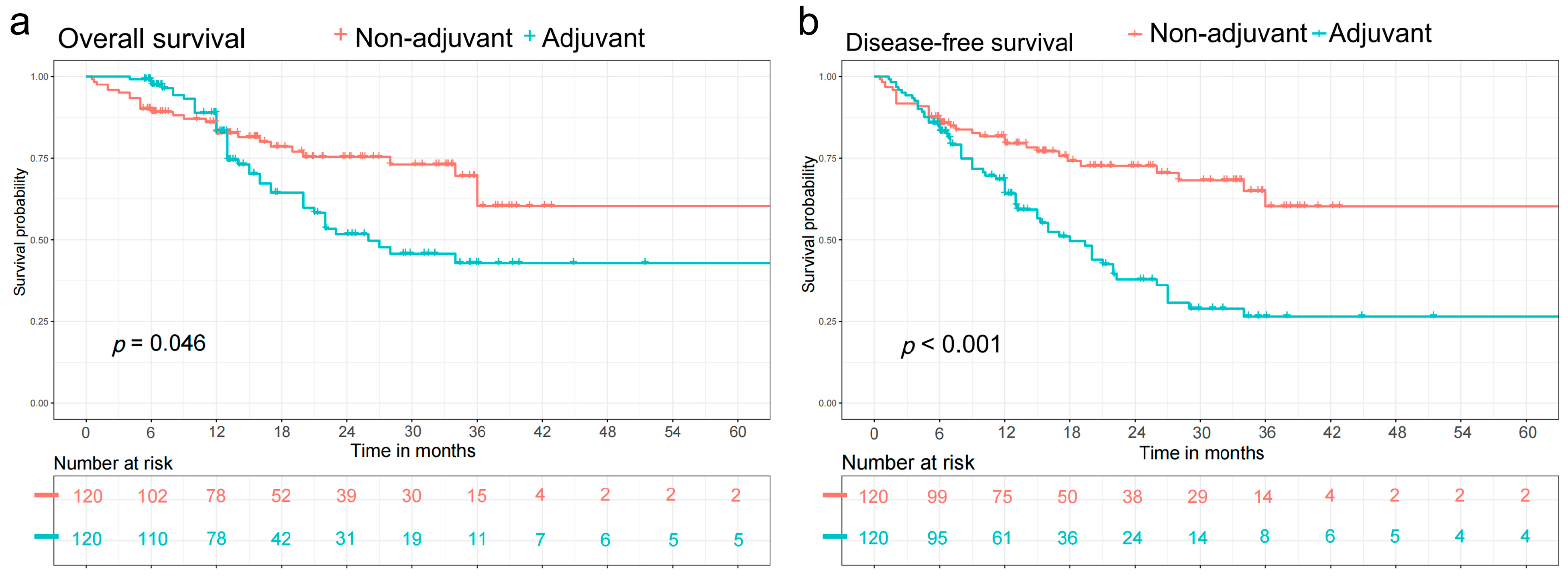
3.2. Survival Analysis
3.3. Cox Regression Analysis
3.4. Subgroup Analysis by Forest Plot
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; D’Amico, T.A.; Bentrem, D.J.; Chao, J.; Corvera, C.; Das, P.; Denlinger, C.S.; Enzinger, P.C.; Fanta, P.; Farjah, F.; et al. Esophageal and Esophagogastric Junction Cancers, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 855–883. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Samarasinghe, Y.; Lee, M.H.; Thiru, L.; Shargall, Y.; Finley, C.; Hanna, W.; Levine, O.; Juergens, R.; Agzarian, J. Role of Adjuvant Therapy in Esophageal Cancer Patients after Neoadjuvant Therapy and Esophagectomy: A Systematic Review and Meta-analysis. Ann. Surg. 2022, 275, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.A.; Yopp, A.C.; Polanco, P.M.; Mansour, J.C.; Reznik, S.I.; Heitjan, D.F.; Choti, M.A.; Minter, R.R.; Wang, S.C.; Porembka, M.R. Adjuvant Chemotherapy vs. Postoperative Observation Following Preoperative Chemoradiotherapy and Resection in Gastroesophageal Cancer: A Propensity Score-Matched Analysis. JAMA Oncol. 2018, 4, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Samson, P.; Puri, V.; Lockhart, A.C.; Robinson, C.; Broderick, S.; Patterson, G.A.; Meyers, B.; Crabtree, T. Adjuvant chemotherapy for patients with pathologic node-positive esophageal cancer after induction chemotherapy is associated with improved survival. J. Thorac. Cardiovasc. Surg. 2018, 156, 1725–1735. [Google Scholar] [CrossRef] [PubMed]
- Burt, B.M.; Groth, S.S.; Sada, Y.H.; Farjah, F.; Cornwell, L.; Sugarbaker, D.J.; Massarweh, N.N. Utility of Adjuvant Chemotherapy after Neoadjuvant Chemoradiation and Esophagectomy for Esophageal Cancer. Ann. Surg. 2017, 266, 297–304. [Google Scholar] [CrossRef]
- Sudo, N.; Ichikawa, H.; Muneoka, Y.; Hanyu, T.; Kano, Y.; Ishikawa, T.; Hirose, Y.; Miura, K.; Shimada, Y.; Nagahashi, M.; et al. Clinical Utility of ypTNM Stage Grouping in the 8th Edition of the American Joint Committee on Cancer TNM Staging System for Esophageal Squamous Cell Carcinoma. Ann. Surg. Oncol. 2021, 28, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Ando, N.; Kato, H.; Igaki, H.; Shinoda, M.; Ozawa, S.; Shimizu, H.; Nakamura, T.; Yabusaki, H.; Aoyama, N.; Kurita, A.; et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907). Ann. Surg. Oncol. 2012, 19, 68–74. [Google Scholar] [CrossRef]
- Smyth, E.C.; Cunningham, D. Adjuvant Chemotherapy Following Neoadjuvant Chemotherapy Plus Surgery for Patients after Gastroesophageal Cancer-Is There Room for Improvement? JAMA Oncol. 2018, 4, 38–39. [Google Scholar] [CrossRef]
- Takeda, F.R.; Tustumi, F.; de Almeida Obregon, C.; Yogolare, G.G.; Navarro, Y.P.; Segatelli, V.; Sallum, R.A.A.; Junior, U.R.; Cecconello, I. Prognostic Value of Tumor Regression Grade Based on Ryan Score in Squamous Cell Carcinoma and Adenocarcinoma of Esophagus. Ann. Surg. Oncol. 2020, 27, 1241–1247. [Google Scholar] [CrossRef]
- Ajani, J.A.; D’Amico, T.A.; Almhanna, K.; Bentrem, D.J.; Besh, S.; Chao, J.; Das, P.; Denlinger, C.; Fanta, P.; Fuchs, C.S.; et al. Esophageal and esophagogastric junction cancers, version 1.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 194–227. [Google Scholar] [CrossRef] [PubMed]
- Drake, J.; Tauer, K.; Portnoy, D.; Weksler, B. Adjuvant chemotherapy is associated with improved survival in patients with nodal metastases after neoadjuvant therapy and esophagectomy. J. Thorac. Dis. 2019, 11, 2546–2554. [Google Scholar] [CrossRef]
- Semenkovich, T.R.; Subramanian, M.; Yan, Y.; Hofstetter, W.L.; Correa, A.M.; Cassivi, S.D.; Inra, M.L.; Stiles, B.M.; Altorki, N.K.; Chang, A.C.; et al. Adjuvant Therapy for Node-Positive Esophageal Cancer after Induction and Surgery: A Multisite Study. Ann. Thorac. Surg. 2019, 108, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Li, S.; Yang, X.; Lu, F.; Huang, M.; Zhang, S.; Xiong, Y.; Zhang, P.; Si, J.; Ma, Y.; et al. Long-term survival of patients with locally advanced esophageal squamous cell carcinoma receiving esophagectomy following neoadjuvant chemotherapy: A cohort study. Cancer Manag. Res. 2019, 11, 1299–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquali, S.; Yim, G.; Vohra, R.S.; Mocellin, S.; Nyanhongo, D.; Marriott, P.; Geh, J.I.; Griffiths, E.A. Survival after Neoadjuvant and Adjuvant Treatments Compared to Surgery Alone for Resectable Esophageal Carcinoma: A Network Meta-analysis. Ann. Surg. 2017, 265, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Hao, D.; Wu, X.; Xing, W.; Yang, Y.; He, C.; Wang, W.; Liu, J.; Wang, J. Neoadjuvant versus adjuvant chemoradiation for stage II-III esophageal squamous cell carcinoma: A single institution experience. Dis. Esophagus 2017, 30, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, N.; Yamasaki, M.; Yamashita, K.; Tanaka, K.; Makino, T.; Saito, T.; Yamamoto, K.; Takahashi, T.; Kurokawa, Y.; Motoori, M.; et al. The role of adjuvant chemotherapy in esophageal cancer patients after neoadjuvant chemotherapy plus surgery. Esophagus 2021, 18, 559–565. [Google Scholar] [CrossRef]
- Ji, Y.; Du, X.; Zhu, W.; Yang, Y.; Ma, J.; Zhang, L.; Li, J.; Tao, H.; Xia, J.; Yang, H.; et al. Efficacy of Concurrent Chemoradiotherapy after S-1 vs. Radiotherapy Alone for Older Patients after Esophageal Cancer: A Multicenter Randomized Phase 3 Clinical Trial. JAMA Oncol. 2021, 7, 1459–1466. [Google Scholar] [CrossRef] [PubMed]
- Cheraghi, A.; Barahman, M.; Hariri, R.; Nikoofar, A.; Fadavi, P. Comparison of the Pathological Response and Adverse Effects of Oxaliplatin and Capecitabine versus Paclitaxel and Carboplatin in the Neoadjuvant Chemoradiotherapy Treatment Approach for Esophageal and Gastroesophageal Junction Cancer: A Randomized Control Trial Study. Med. J. Islamic Repub. Iran 2021, 35, 140. [Google Scholar] [CrossRef]
- Noordman, B.J.; Verdam, M.G.E.; Lagarde, S.M.; Shapiro, J.; Hulshof, M.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; Nieuwenhuijzen, G.A.P.; Bonenkamp, J.J.; Cuesta, M.A.; et al. Impact of neoadjuvant chemoradiotherapy on health-related quality of life in long-term survivors of esophageal or junctional cancer: Results from the randomized CROSS trial. Ann. Oncol. 2018, 29, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.A.; Docherty, N.G.; Eckhardt, H.G.; Doyle, S.L.; Guinan, E.M.; Ravi, N.; Reynolds, J.V.; Roux, C.W.L. Weight Loss, Satiety, and the Postprandial Gut Hormone Response after Esophagectomy: A Prospective Study. Ann. Surg. 2017, 266, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Kubo, Y.; Miyata, H.; Sugimura, K.; Shinno, N.; Asukai, K.; Hasegawa, S.; Yanagimoto, Y.; Yamada, D.; Yamamoto, K.; Nishimura, J.; et al. Prognostic Implication of Postoperative Weight Loss after Esophagectomy for Esophageal Squamous Cell Cancer. Ann. Surg. Oncol. 2021, 28, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, D.J.; Suh, J.W.; Byun, G.E. Risk Factors for Weight Loss 1 Year after Esophagectomy and Gastric Pull-up for Esophageal Cancer. J. Gastrointest. Surg. 2018, 22, 1137–1143. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | No. (%) (n = 447) | Before Propensity Score Match | After Propensity Score Match | ||||
|---|---|---|---|---|---|---|---|
| Non-Adjuvant Therapy (n = 306) | Adjuvant Therapy (n = 141) | p-Value | Non-Adjuvant Therapy (n = 120) | Adjuvant Therapy (n = 120) | p-Value | ||
| Gender | 0.155 | 0.701 | |||||
| Male | 359 (80.3%) | 274 (79.9%) | 121 (85.8%) | 106 (88.3%) | 103 (85.8%) | ||
| Female | 88 (19.7%) | 69 (20.1%) | 20 (14.2%) | 14 (11.6%) | 17 (14.2%) | ||
| Age (year) | 0.004 | 0.331 | |||||
| ≤65 | 287 (64.2%) | 183 (59.8%) | 104 (73.8%) | 78 (65.0%) | 86 (71.7%) | ||
| >65 | 160 (35.8%) | 123 (40.2%) | 37 (26.2%) | 42 (35.0%) | 34 (28.3%) | ||
| Smoke | 0.014 | 0.155 | |||||
| Yes | 230 (51.5%) | 145 (47.4%) | 85 (60.3%) | 58 (48.3%) | 70 (58.3%) | ||
| No | 217 (48.5%) | 161 (52.6%) | 56 (39.7%) | 62 (51.7%) | 50 (41.7%) | ||
| Alcohol consumption | 0.837 | 0.517 | |||||
| Yes | 187 (41.8%) | 127 (41.5%) | 60 (42.6%) | 52 (43.3%) | 57 (47.5%) | ||
| No | 260 (58.2%) | 179 (58.5%) | 81 (57.4%) | 68 (56.7%) | 63 (52.5%) | ||
| Hypertension | 0.895 | 0.869 | |||||
| Yes | 80 (17.9%) | 54 (17.6%) | 26 (18.4%) | 23 (19.2%) | 22 (18.3%) | ||
| No | 367 (82.1%) | 252 (82.4%) | 115 (81.6%) | 97 (80.8%) | 98 (81.7%) | ||
| Cardiovascular disease (n = 444) | 0.450 | 0.518 | |||||
| Yes | 19 (4.3%) | 15 (4.9%) | 4 (2.9%) | 6 (5.0%) | 4 (3.3%) | ||
| No | 425 (95.7%) | 290 (95.1%)) | 135 (97.1%) | 114 (95.0%) | 116 (96.7%) | ||
| Cerebrovascular disease (n = 442) | 0.443 | 0.999 | |||||
| Yes | 7 (1.6%) | 6 (2.0%) | 1 (0.7%) | 1 (0.8%) | 1 (0.8%) | ||
| No | 435 (98.4%) | 298 (98.0%) | 137 (99.3%) | 119 (99.2%) | 119 (99.2%) | ||
| Chronic liver disease (n = 434) | 0.853 | 0.999 | |||||
| Yes | 37 (8.5%) | 25 (8.3%) | 12 (9.0%) | 10 (8.3%) | 10 (8.3%) | ||
| No | 397 (91.5%) | 275 (91.7%) | 122 (91.0%) | 110 (91.7%) | 110 (91.7%) | ||
| COPD (n = 444) | 0.533 | 0.554 | |||||
| Yes | 28 (6.3%) | 21 (6.9%) | 7 (5.0%) | 7 (5.8%) | 5 (4.2%) | ||
| No | 416 (93.7%) | 284 (93.1%) | 132 (95.0%) | 113 (94.2%) | 115 (95.8%) | ||
| Arrhythmia (n = 446) | 0.515 | 0.651 | |||||
| Yes | 10 (2.2%) | 8 (2.6%) | 2 (1.4%) | 3 (2.5%) | 2 (1.7%) | ||
| No | 436 (97.8%) | 297 (97.4%) | 139 (98.6%) | 117 (97.5%) | 118 (98.3%) | ||
| Tumor site | 0.046 | 0.383 | |||||
| Upper | 61 (13.6%) | 34 (11.1%) | 27 (19.1%) | 11 (9.2%) | 18 (15.0%) | ||
| Middle | 229 (51.2%) | 160 (52.3%) | 69 (48.9%) | 63 (52.5%) | 59 (49.2%) | ||
| Lower | 157 (35.1%) | 112 (36.6%) | 45 (31.9%) | 46 (38.3%) | 43 (35.8%) | ||
| Tumor length (cm) | 0.001 | 0.694 | |||||
| ≤3 | 289 (64.7%) | 216 (70.6%) | 73 (51.8%) | 72 (60.0%) | 69 (57.5%) | ||
| >3 | 158 (35.3%) | 90 (29.4%) | 68 (48.2%) | 48 (40.0%) | 51 (42.5%) | ||
| ypTNM | 0.000 | 0.160 | |||||
| I | 219 (49.0%) | 174 (56.9%) | 45 (31.9%) | 57 (47.5%) | 43 (35.8%) | ||
| II | 64 (14.3%) | 40 (13.1%) | 24 (17.0%) | 19 (15.8%) | 22 (18.3%) | ||
| IIIA | 55 (12.3%) | 34 (11.1%) | 21 (14.9%) | 9 (7.5%) | 18 (15.0%) | ||
| IIIB | 96 (21.5%) | 50 (16.3%) | 46 (32.6%) | 29 (24.2%) | 34 (28.3%) | ||
| IVA | 13 (2.9%) | 8 (2.6%) | 5 (3.5%) | 6 (5.0%) | 3 (2.5%) | ||
| ypT | 0.001 | 0.493 | |||||
| Tis | 2 (0.4%) | 2 (0.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| T0 | 161 (36.0%) | 127 (41.5%) | 34 (24.1%) | 42 (35.0%) | 32 (26.6%) | ||
| T1 | 64 (14.3%) | 44 (14.4%) | 20 (14.2%) | 12 (10.0%) | 17 (14.2%) | ||
| T2 | 65 (14.5%) | 44 (14.4%) | 21 (14.9%) | 19 (15.8%) | 20 (16.7%) | ||
| T3 | 155 (34.5%) | 89 (28.8%) | 66 (46.8%) | 47 (39.2%) | 51 (42.5%) | ||
| ypN | 0.001 | 0.304 | |||||
| N0 | 284 (63.5%) | 214 (69.9%) | 70 (49.6%) | 76 (63.3%) | 66 (55.0%) | ||
| N1 | 112 (25.1%) | 67 (21.9%) | 45 (31.9%) | 26 (21.7%) | 34 (28.3%) | ||
| N2 | 39 (8.7%) | 18 (5.9%) | 21 (14.9%) | 12 (10.0%) | 17 (14.2%) | ||
| N3 | 12 (2.7%) | 8 (2.6%) | 5 (3.5%) | 6 (5.0%) | 3 (2.5%) | ||
| Tumor differentiation | 0.000 | 0.116 | |||||
| G1 | 13 (2.9%) | 10 (3.3%) | 3 (2.1%) | 5 (4.2%) | 2 (1.7%) | ||
| G2 | 108 (24.2%) | 73 (23.9%) | 35 (24.8%) | 35 (29.2%) | 25 (20.8%) | ||
| G3 | 138 (30.9%) | 77 (25.2%) | 61 (43.3%) | 37 (30.8%) | 53 (44.2%) | ||
| Gx | 188 (42.1%) | 146 (47.7%) | 42 (29.8%) | 43 (35.8%) | 40 (33.3%) | ||
| Lymphovascular invasion | 0.001 | 0.336 | |||||
| Yes | 42 (9.4%) | 19 (6.2%) | 23 (16.3%) | 13 (10.8%) | 18 (15.0%) | ||
| No | 405 (90.6%) | 287 (93.8%) | 118 (83.7%) | 107 (89.2%) | 102 (85.0%) | ||
| Peripheral nerve invasion | 0.002 | 0.525 | |||||
| Yes | 80 (17.9%) | 43 (14.1%) | 37 (26.2%) | 23 (19.2%) | 27 (22.5%) | ||
| No | 367 (82.1%) | 263 (85.9%) | 104 (73.8%) | 97 (80.8%) | 93 (77.5%) | ||
| Surgical type | 0.198 | 0.678 | |||||
| Open surgery | 45 (10.1%) | 27 (8.8%) | 18 (12.8%) | 14 (11.7%) | 12 (10.0%) | ||
| Video-assisted Thoracoscopic Surgery | 402 (89.9%) | 279 (91.2%) | 123 (87.2%) | 106 (88.3%) | 108 (90.0%) | ||
| Anastomotic method | 0.285 | 0.313 | |||||
| Stapled anastomosis | 16 (3.6%) | 9 (2.9%) | 7 (5.0%) | 3 (2.5%) | 6 (5.0%) | ||
| Hand-sewn anastomosis | 431 (96.4%) | 297 (97.1%) | 134 (95.0%) | 117 (97.5%) | 114 (95.0%) | ||
| Complications (Clavien-Dindo) | 0.606 | 0.619 | |||||
| Grade I | 73 (16.3%) | 47 (15.4%) | 26 (18.4%) | 17 (41.2%) | 22 (18.3%) | ||
| Grade II | 149 (33.3%) | 104 (34.0%) | 45 (31.9%) | 40 (33.3%) | 39 (32.5%) | ||
| Grade III | 29 (6.5%) | 21 (6.9%) | 8 (5.7%) | 12 (10.0%) | 8 (6.7%) | ||
| Grade IV | 7 (1.6%) | 6 (2.0%) | 1 (0.7%) | 2 (1.7%) | 1 (0.8%) | ||
| Tumor regression grade | 0.000 | 0.451 | |||||
| TRG 0 | 150 (33.6%) | 120 (39.2%) | 30 (21.3%) | 39 (32.5%) | 28 (23.3%) | ||
| TRG 1 | 73 (16.3%) | 55 (18.0%) | 18 (12.8%) | 15 (12.5%) | 17 (41.2%) | ||
| TRG 2 | 170 (38.0%) | 101 (33.0%) | 69 (48.9%) | 51 (42.5%) | 56 (46.7%) | ||
| TRG 3 | 54 (12.1%) | 30 (9.8%) | 24 (17.0%) | 15 (12.5%) | 19 (15.8%) | ||
| Overall Survival | Progression-Free Survival | |||||
|---|---|---|---|---|---|---|
| Multivariate Analyses | HR | 95% CI of HR | p-Value | HR | 95% CI of HR | p-Value |
| Gender | ||||||
| Male versus female | 1.034 | 0.533–2.005 | 0.921 | 1.004 | 0.562–1.794 | 0.990 |
| Smoke | ||||||
| Yes versus no | 1.505 | 0.917–2.467 | 0.106 | 1.490 | 0.961–1.924 | 0.075 |
| Tumor length | ||||||
| >3 cm versus ≤3 cm | 1.486 | 0.989–2.234 | 0.056 | 1.346 | 0.941–1.924 | 0.103 |
| ypTNM | ||||||
| III-IV versus I-II | 2.720 | 1.741–4.249 | 0.000 | 2.079 | 1.411–3.065 | 0.000 |
| Lymphovascular invasion | ||||||
| Yes versus no | 1.095 | 0.626–1.915 | 1.095 | 1.324 | 0.819–2.140 | 0.251 |
| Peripheral nerve invasion | ||||||
| Yes versus no | 0.912 | 0.558–1.490 | 0.712 | 1.409 | 0.919–2.159 | 0.115 |
| Tumor regression grade | ||||||
| TRG 3/2 versus TRG 1/0 | 1.358 | 0.839–2.198 | 0.212 | 1.074 | 0.703–1.640 | 0.743 |
| Adjuvant Therapy | ||||||
| Yes versus no | 1.270 | 0.846–1.906 | 0.249 | 2.061 | 1.436–2.958 | 0.000 |
| Study | Year | Design | Sample Size | Histological Type | ypN Stage | Hazard Ratio | p Value |
|---|---|---|---|---|---|---|---|
| Burt BM, et al. [7] | 2017 | Retrospective cohort study based on NCDB | 3592 | EAC, ESCC | Any | 0.93 (ypN0) | Not significant |
| 0.7 (ypN1–3) | Significant | ||||||
| Samson P, et al. [6] | 2018 | Retrospective cohort study based on NCDB | 3100 | EAC, ESCC | + | 0.69 | <0.001 |
| Mokdad AA, et al. [5] | 2018 | Retrospective cohort study based on NCDB | 10,086 | Gastroesophageal adenocarcinoma | Any | 0.79 | <0.001 |
| 0.68 (ypN0) | Significant | ||||||
| 0.86 (ypN1–3) | Significant | ||||||
| Drake J, et al. [13] | 2019 | Retrospective cohort study based on NCDB | 2046 | EAC | + | 0.839 | 0.0311 |
| Semenkovich TR, et al. [14] | 2019 | Multicenter retrospective cohort study | 1082 | EAC, ESCC | + | 0.76 | 0.005 |
| Huang Z, et al. [15] | 2019 | Retrospective cohort study | 228 | ESCC | Any | 1.498 | 0.052 |
| The present study | 2022 | Retrospective cohort study | 447 | ESCC | Any | 1.613 | 0.051 |
| 4.274 (ypN0) | 0.002 | ||||||
| 0.818 (ypN1–3) | 0.506 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Luan, S.; Yang, Y.; Zhou, J.; Shang, Q.; Fang, P.; Xiao, X.; Zhang, H.; Yuan, Y. Trimodal Therapy in Esophageal Squamous Cell Carcinoma: Role of Adjuvant Therapy Following Neoadjuvant Chemoradiation and Surgery. Cancers 2022, 14, 3721. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153721
Li X, Luan S, Yang Y, Zhou J, Shang Q, Fang P, Xiao X, Zhang H, Yuan Y. Trimodal Therapy in Esophageal Squamous Cell Carcinoma: Role of Adjuvant Therapy Following Neoadjuvant Chemoradiation and Surgery. Cancers. 2022; 14(15):3721. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153721
Chicago/Turabian StyleLi, Xiaokun, Siyuan Luan, Yushang Yang, Jianfeng Zhou, Qixin Shang, Pinhao Fang, Xin Xiao, Hanlu Zhang, and Yong Yuan. 2022. "Trimodal Therapy in Esophageal Squamous Cell Carcinoma: Role of Adjuvant Therapy Following Neoadjuvant Chemoradiation and Surgery" Cancers 14, no. 15: 3721. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153721