Association between Dietary Fiber Intake and Mortality among Colorectal Cancer Survivors: Results from the Newfoundland Familial Colorectal Cancer Cohort Study and a Meta-Analysis of Prospective Studies

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The Newfoundland Familial Colorectal Cancer Study
2.1.1. Study Population
2.1.2. Diet assessment and Baseline Information Collection
2.1.3. Study Outcomes
2.1.4. Statistical Analysis
2.2. Meta-Analysis
2.2.1. Literature Search Strategy and Study Selection
2.2.2. Data Extraction
2.2.3. Statistical Analysis
3. Results
3.1. The Newfoundland Familial Colorectal Cancer Cohort Study
3.1.1. Patient Characteristics
3.1.2. Dietary Fiber Intake and All-Cause Mortality
3.1.3. Dietary Fiber Intake and CRC-Specific Mortality
3.2. Meta-Analysis
3.2.1. Study Selection and Characteristics
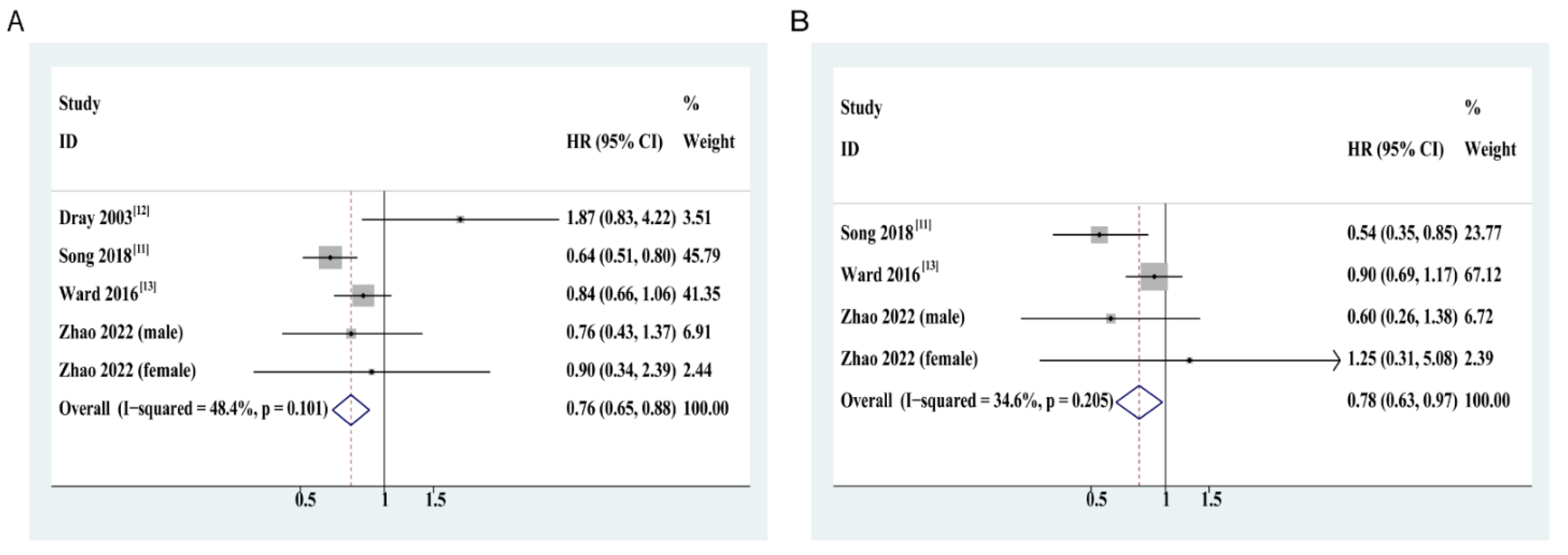
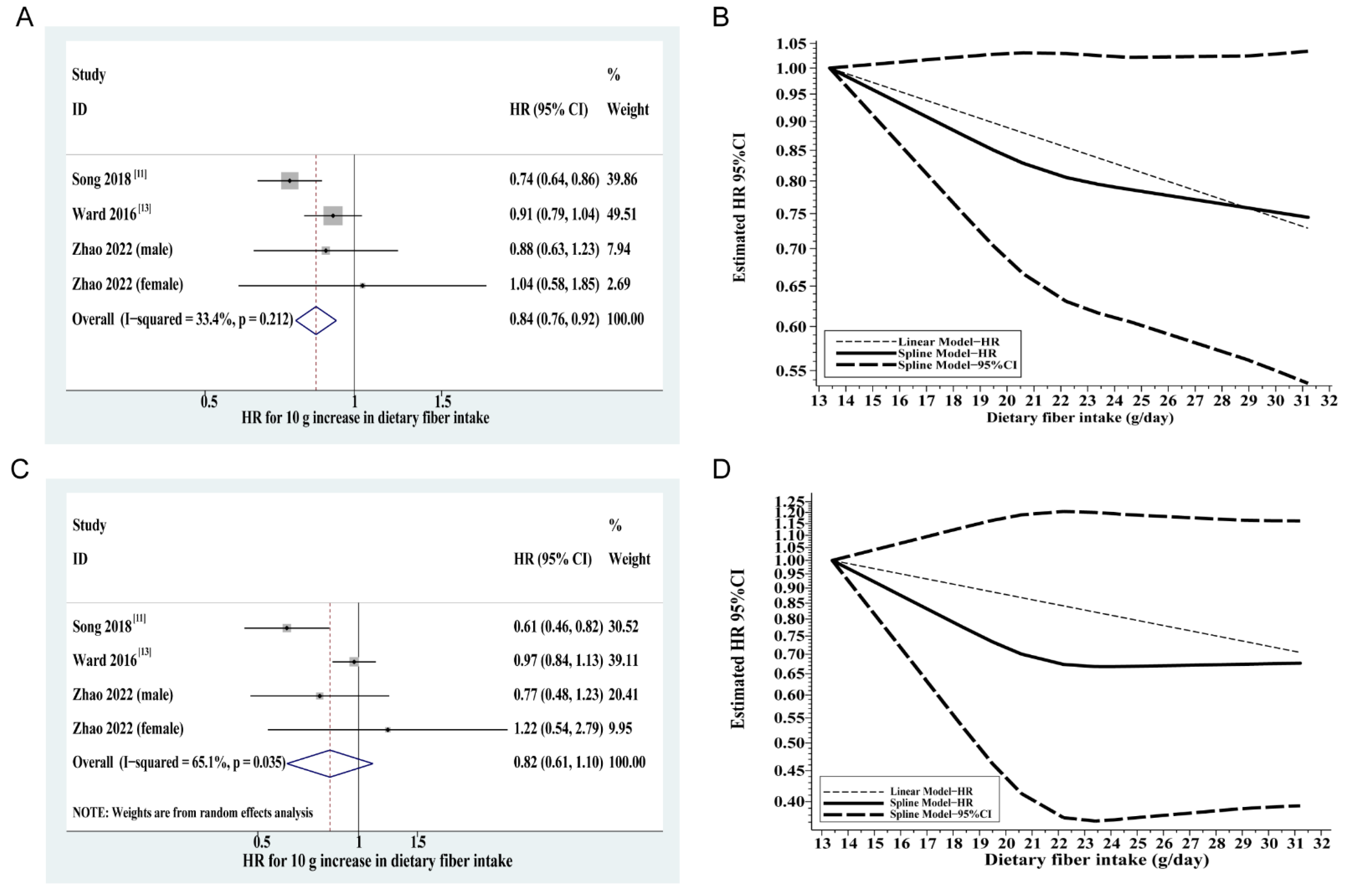
3.2.2. Association between Dietary Fiber Intake and All-Cause Mortality
3.2.3. Association between Dietary Fiber Intake and CRC-Specific Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee in Collaboration with the Canadian Cancer Society; Statistics Canada; The Public Health Agency of Canada. Canadian Cancer Statistics 2021; Canadian Cancer Society: Toronto, ON, Canada, 2021; Available online: cancer.ca/Canadian-Cancer-Statistics-2021-EN (accessed on 18 November 2021).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.W.; Demark-Wahnefried, W. Diet, exercise, and complementary therapies after primary treatment for cancer. Lancet Oncol. 2006, 7, 1017–1026. [Google Scholar] [CrossRef]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 243–274. [Google Scholar] [CrossRef] [Green Version]
- El-Shami, K.; Oeffinger, K.C.; Erb, N.L.; Willis, A.; Bretsch, J.K.; Pratt-Chapman, M.L.; Cannady, R.S.; Wong, S.L.; Rose, J.; Barbour, A.L.; et al. American Cancer Society Colorectal Cancer Survivorship Care Guidelines. CA Cancer J. Clin. 2015, 65, 428–455. [Google Scholar] [CrossRef]
- Barber, T.M.; Kabisch, S.; Pfeiffer, A.F.H.; Weickert, M.O. The Health Benefits of Dietary Fibre. Nutrients 2020, 12, 209. [Google Scholar] [CrossRef]
- Stephen, A.M.; Champ, M.M.; Cloran, S.J.; Fleith, M.; van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary fibre in Europe: Current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr. Res. Rev. 2017, 30, 149–190. [Google Scholar] [CrossRef]
- Aune, D.; Chan, D.S.; Lau, R.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Dietary fibre, whole grains, and risk of colorectal cancer: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2011, 343, d6617. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Garrett, W.S.; Chan, A.T. Nutrients, foods, and colorectal cancer prevention. Gastroenterology 2015, 148, 1244–1260.e16. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Wu, K.; Meyerhardt, J.A.; Ogino, S.; Wang, M.; Fuchs, C.S.; Giovannucci, E.L.; Chan, A.T. Fiber Intake and Survival After Colorectal Cancer Diagnosis. JAMA Oncol. 2018, 4, 71–79. [Google Scholar] [CrossRef]
- Dray, X.; Boutron-Ruault, M.C.; Bertrais, S.; Sapinho, D.; Benhamiche-Bouvier, A.M.; Faivre, J. Influence of dietary factors on colorectal cancer survival. Gut 2003, 52, 868–873. [Google Scholar] [CrossRef]
- Ward, H.A.; Norat, T.; Overvad, K.; Dahm, C.C.; Bueno-de-Mesquita, H.B.; Jenab, M.; Fedirko, V.; van Duijnhoven, F.J.; Skeie, G.; Romaguera-Bosch, D.; et al. Pre-diagnostic meat and fibre intakes in relation to colorectal cancer survival in the European Prospective Investigation into Cancer and Nutrition. Br. J. Nutr. 2016, 116, 316–325. [Google Scholar] [CrossRef] [Green Version]
- Zell, J.A.; McEligot, A.J.; Ziogas, A.; Holcombe, R.F.; Anton-Culver, H. Differential effects of wine consumption on colorectal cancer outcomes based on family history of the disease. Nutr. Cancer 2007, 59, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Slattery, M.L.; French, T.K.; Egger, M.J.; Lyon, J.L. Diet and survival of patients with colon cancer in Utah: Is there an association? Int. J. Epidemiol. 1989, 18, 792–797. [Google Scholar] [CrossRef]
- Hoang, T.; Kim, H.; Kim, J. Dietary Intake in Association with All-Cause Mortality and Colorectal Cancer Mortality among Colorectal Cancer Survivors: A Systematic Review and Meta-Analysis of Prospective Studies. Cancers 2020, 12, 3391. [Google Scholar] [CrossRef]
- Sharma, I.; Zhu, Y.; Woodrow, J.R.; Mulay, S.; Parfrey, P.S.; McLaughlin, J.R.; Hebert, J.R.; Shivappa, N.; Li, Y.; Zhou, X.; et al. Inflammatory diet and risk for colorectal cancer: A population-based case-control study in Newfoundland, Canada. Nutrition 2017, 42, 69–74. [Google Scholar] [CrossRef]
- Sun, Z.; Wang, P.P.; Roebothan, B.; Cotterchio, M.; Green, R.; Buehler, S.; Zhao, J.; Squires, J.; Zhao, J.; Zhu, Y.; et al. Calcium and Vitamin D and Risk of Colorectal Cancer: Results From a Large Population-based Case-control Study in Newfoundland and Labrador and Ontario. Can. J. Public Health 2011, 102, 382–389. [Google Scholar] [CrossRef]
- Woods, M.O.; Younghusband, H.B.; Parfrey, P.S.; Gallinger, S.; McLaughlin, J.; Dicks, E.; Stuckless, S.; Pollett, A.; Bapat, B.; Mrkonjic, M.; et al. The genetic basis of colorectal cancer in a population-based incident cohort with a high rate of familial disease. Gut 2010, 59, 1369–1377. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Wang, P.P.; Zhao, J.; Green, R.; Sun, Z.; Roebothan, B.; Squires, J.; Buehler, S.; Dicks, E.; Zhao, J.; et al. Dietary N-nitroso compounds and risk of colorectal cancer: A case-control study in Newfoundland and Labrador and Ontario, Canada. Br. J. Nutr. 2014, 111, 1109–1117. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Wu, H.; Wang, P.P.; Savas, S.; Woodrow, J.; Wish, T.; Jin, R.; Green, R.; Woods, M.; Roebothan, B.; et al. Dietary patterns and colorectal cancer recurrence and survival: A cohort study. BMJ Open 2013, 3, e002270. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.P.; Dicks, E.; Gong, X.; Buehler, S.; Zhao, J.; Squires, J.; Younghusband, B.; McLaughlin, J.R.; Parfrey, P.S. Validity of random-digit-dialing in recruiting controls in a case-control study. Am. J. Health Behav. 2009, 33, 513–520. [Google Scholar] [CrossRef]
- Liu, L.; Wang, P.P.; Roebothan, B.; Ryan, A.; Tucker, C.S.; Colbourne, J.; Baker, N.; Cotterchio, M.; Yi, Y.; Sun, G. Assessing the validity of a self-administered food-frequency questionnaire (FFQ) in the adult population of Newfoundland and Labrador, Canada. Nutr. J. 2013, 12, 49. [Google Scholar] [CrossRef] [Green Version]
- Sun, Z.; Zhu, Y.; Wang, P.P.; Roebothan, B.; Zhao, J.; Zhao, J.; Dicks, E.; Cotterchio, M.; Buehler, S.; Campbell, P.T.; et al. Reported intake of selected micronutrients and risk of colorectal cancer: Results from a large population-based case-control study in Newfoundland, Labrador and Ontario, Canada. Anticancer Res. 2012, 32, 687–696. [Google Scholar]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef]
- Loughrey, M.B.; Waring, P.M.; Tan, A.; Trivett, M.; Kovalenko, S.; Beshay, V.; Young, M.A.; McArthur, G.; Boussioutas, A.; Dobrovic, A. Incorporation of somatic BRAF mutation testing into an algorithm for the investigation of hereditary non-polyposis colorectal cancer. Fam. Cancer 2007, 6, 301–310. [Google Scholar] [CrossRef]
- Raptis, S.; Mrkonjic, M.; Green, R.C.; Pethe, V.V.; Monga, N.; Chan, Y.M.; Daftary, D.; Dicks, E.; Younghusband, B.H.; Parfrey, P.S.; et al. MLH1–93G>A promoter polymorphism and the risk of microsatellite-unstable colorectal cancer. J. Natl. Cancer Inst. 2007, 99, 463–474. [Google Scholar] [CrossRef]
- World Health Organization. MANUAL of the international statistical classification of diseases, injuries, and causes of death. Addendum 1. Supplementary interpretations and instructions for coding causes of death. Bull. World Health Org. Suppl. 1953, 7, 1–55. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Cook, N.R.; Bergström, A.; Hsieh, C.-C. A two-stage hierarchical regression model for meta-analysis of epidemiologic nonlinear dose–response data. Comput. Stat. Data Anal. 2009, 53, 4157–4167. [Google Scholar] [CrossRef]
- Desquilbet, L.; Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Durrleman, S.; Simon, R. Flexible regression models with cubic splines. Stat. Med. 1989, 8, 551–561. [Google Scholar] [CrossRef]
- Orsini, N.; Greenland, S. A Procedure to Tabulate and Plot Results after Flexible Modeling of a Quantitative Covariate. Stata J.—Promot. Commun. Stat. Stata 2011, 11, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Jackson, D.; White, I.R.; Thompson, S.G. Extending DerSimonian and Laird’s methodology to perform multivariate random effects meta-analyses. Stat. Med. 2010, 29, 1282–1297. [Google Scholar] [CrossRef]
- White, I.R. Multivariate Random-effects Meta-analysis. Stata J.—Promot. Commun. Stat. Stata 2009, 9, 40–56. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Burkitt, D.P. Epidemiology of cancer of the colon and rectum. Cancer 1971, 28, 3–13. [Google Scholar] [CrossRef]
- Bras-Goncalves, R.A.; Pocard, M.; Formento, J.L.; Poirson-Bichat, F.; De Pinieux, G.; Pandrea, I.; Arvelo, F.; Ronco, G.; Villa, P.; Coquelle, A.; et al. Synergistic efficacy of 3n-butyrate and 5-fluorouracil in human colorectal cancer xenografts via modulation of DNA synthesis. Gastroenterology 2001, 120, 874–888. [Google Scholar] [CrossRef]
- Kuefer, R.; Hofer, M.D.; Altug, V.; Zorn, C.; Genze, F.; Kunzi-Rapp, K.; Hautmann, R.E.; Gschwend, J.E. Sodium butyrate and tributyrin induce in vivo growth inhibition and apoptosis in human prostate cancer. Br. J. Cancer 2004, 90, 535–541. [Google Scholar] [CrossRef]
- Entin-Meer, M.; Rephaeli, A.; Yang, X.; Nudelman, A.; VandenBerg, S.R.; Haas-Kogan, D.A. Butyric acid prodrugs are histone deacetylase inhibitors that show antineoplastic activity and radiosensitizing capacity in the treatment of malignant gliomas. Mol. Cancer Ther. 2005, 4, 1952–1961. [Google Scholar] [CrossRef] [Green Version]
- Bultman, S.J. Molecular pathways: Gene-environment interactions regulating dietary fiber induction of proliferation and apoptosis via butyrate for cancer prevention. Clin. Cancer Res. 2014, 20, 799–803. [Google Scholar] [CrossRef] [Green Version]
- Encarnacao, J.C.; Abrantes, A.M.; Pires, A.S.; Botelho, M.F. Revisit dietary fiber on colorectal cancer: Butyrate and its role on prevention and treatment. Cancer Metastasis Rev. 2015, 34, 465–478. [Google Scholar] [CrossRef]
- Skeie, G.; Hjartaker, A.; Braaten, T.; Lund, E. Dietary change among breast and colorectal cancer survivors and cancer-free women in the Norwegian Women and Cancer cohort study. Cancer Causes Control 2009, 20, 1955–1966. [Google Scholar] [CrossRef]
- Wang, D.D.; Li, Y.; Bhupathiraju, S.N.; Rosner, B.A.; Sun, Q.; Giovannucci, E.L.; Rimm, E.B.; Manson, J.E.; Willett, W.C.; Stampfer, M.J.; et al. Fruit and Vegetable Intake and Mortality: Results From 2 Prospective Cohort Studies of US Men and Women and a Meta-Analysis of 26 Cohort Studies. Circulation 2021, 143, 1642–1654. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Patients | No. of Deaths (%) | Univariate HR (95% CI) a |
|---|---|---|---|
| Age at diagnosis (y) b | 60.9 ± 9.0 | 62.0 ± 8.9 | 1.02 (1.00–1.03) |
| Sex | |||
| Male | 306 | 106 (34.6) | 1.00 |
| Female | 198 | 53 (26.8) | 0.70 (0.50–0.98) |
| BMI (kg/m2) | |||
| <25.0 | 140 | 43 (30.7) | 1.00 |
| 25.0–29.9 | 203 | 70 (34.5) | 1.06 (0.72–1.55) |
| ≥30 | 146 | 41 (28.1) | 0.91 (0.60–1.40) |
| Marital status | |||
| Single | 109 | 40 (36.7) | 1.00 |
| Married or living as married | 395 | 119 (30.1) | 0.85 (0.60–1.22) |
| Tumor location | |||
| Colon | 328 | 97 (29.6) | 1.00 |
| Rectum | 176 | 62 (35.2) | 1.19 (0.86–1.63) |
| Stage at diagnosis | |||
| I/II | 293 | 66 (22.5) | 1.00 |
| III/IV | 211 | 93 (44.1) | 2.36 (1.72–3.24) |
| T stage | |||
| T1 | 25 | 5 (20.0) | 1.00 |
| T2 | 100 | 23 (23.0) | 1.11 (0.42–2.93) |
| T3 | 308 | 107 (34.9) | 1.74 (0.71–4.26) |
| T4 | 19 | 8 (42.1) | 1.98 (0.64–6.07) |
| N stage | |||
| NX | 9 | 2 (22.2) | 1.00 |
| N0 | 264 | 66 (25.1) | 1.29 (0.32–5.28) |
| N1 | 121 | 43 (35.5) | 2.02 (0.49–8.35) |
| N2 | 55 | 30 (54.6) | 3.74 (0.89–15.78) |
| M stage | |||
| MX | 221 | 56 (25.5) | 1.00 |
| M0 | 154 | 43 (27.9) | 1.15 (0.77–1.71) |
| M1 | 39 | 31 (79.5) | 6.84 (4.37–10.71) |
| Chemoradiotherapy | |||
| No | 100 | 38 (38.0) | 1.00 |
| Yes | 404 | 121 (30.0) | 1.36 (0.94–1.95) |
| MSI status | |||
| MSS/MSI-L | 423 | 146 (34.5) | 1.00 |
| MSI-H | 55 | 4 (7.3) | 0.17 (0.06–0.46) |
| BRAF mutation status | |||
| Wild-type | 411 | 133 (32.4) | 1.00 |
| V600E mutant | 45 | 13 (28.9) | 0.80 (0.45–1.41) |
| Smoking status | |||
| Never smokers | 138 (27.4) | 36 (26.1) | 1.00 |
| Ever smokers | 366 (72.6) | 123 (33.6) | 1.27 (0.87–1.84) |
| Total energy intake (kcal/d) b | 2455.3 ± 849.4 | 2491.53 ± 796.7 | 1.11 (0.96–1.27) |
| No. of Events a /No. at Risk | Quartiles of Dietary Fiber HR (95% CI) b | p-Value for Trend c | ||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |||
| Mean (g/day) | 14.17 | 19.74 | 24.15 | 30.35 | ||
| All-cause mortality | ||||||
| All | 159/504 | 1.00 | 0.58 (0.35–0.98) | 0.93 (0.57–1.51) | 0.80 (0.49–1.31) | 0.716 |
| Sex | ||||||
| Male | 106/306 | 1.00 | 0.65 (0.35–1.21) | 0.83 (0.46–1.50) | 0.76 (0.43–1.37) | 0.451 |
| Female | 53/198 | 1.00 | 0.53 (0.19–1.46) | 1.23 (0.49–3.11) | 0.90 (0.34–2.39) | 0.783 |
| Anatomical subsite | ||||||
| Colon cancer | 97/328 | 1.00 | 0.44 (0.22–0.88) | 0.76 (0.40–1.43) | 0.55 (0.28–1.07) | 0.264 |
| Rectal cancer | 62/176 | 1.00 | 0.78 (0.32–1.92) | 1.37 (0.58–3.21) | 1.59 (0.70–3.62) | 0.187 |
| CRC-specific mortality | ||||||
| All | 83/443 | 1.00 | 0.42 (0.21–0.87) | 0.72 (0.36–1.43) | 0.77 (0.39–1.52) | 0.568 |
| Sex | ||||||
| Male | 54/264 | 1.00 | 0.28 (0.09–0.86) | 0.70 (0.32–1.56) | 0.60 (0.26–1.38) | 0.285 |
| Female | 29/179 | 1.00 | 0.73 (0.21–2.53) | 0.93 (0.21–4.14) | 1.25 (0.31–5.08) | 0.677 |
| Anatomical subsite | ||||||
| Colon cancer | 47/288 | 1.00 | 0.31 (0.12–0.82) | 0.55 (0.21–1.45) | 0.54 (0.20–1.51) | 0.349 |
| Rectal cancer | 36/155 | 1.00 | 0.79 (0.26–2.42) | 0.80 (0.28–2.25) | 1.53 (0.55–4.29) | 0.556 |
| Author Year Country | Study Name | Study Population | Number of Cases | Follow-Up Time | Outcome | Exposure | Dose (Highest vs. Lowest Categories) | HR (95% CI) | Adjusted Variables |
|---|---|---|---|---|---|---|---|---|---|
| Dray [12] 2003 France | Influence of dietary factors on colorectal cancer survival | 148 participants | 46 deaths | 5 years | 5-year survival rate | Fiber | No dose | 1.87 (0.83–4.22) | Age, sex, tumor stage, tumor location, and energy intake |
| Song [11] 2018 US | Fiber intake and survival after colorectal cancer diagnosis | 1575 participants | 773 deaths; 174 deaths from CRC | 8 years (median) | CRC-specific mortality | Fiber | 28.9 vs. 14.4 g/day | 0.54 (0.35–0.85) | Age at diagnosis, sex, cancer stage, year of diagnosis, tumor grade of differentiation, subsite, fiber intake, post-diagnostic alcohol consumption, pack-years of smoking, BMI, physical activity, regular use of aspirin, glycemic load, and consumption of total fat, folate, calcium, and vitamin D |
| All-cause mortality | 28.9 vs. 14.4 g/day | 0.64 (0.51–0.80) | |||||||
| Ward [13] 2016 Europe | Prediagnostic meat and fibre intakes in relation to colorectal cancer survival in the European Prospective Investigation into Cancer and Nutrition | 3789 participants | 1262 deaths; 1008 deaths from CRC | 4.1 years (average) | CRC-specific mortality | Fiber | 31.2 vs. 14.5 g/day | 0.90 (0.69–1.17) | Age at diagnosis, sex, BMI, smoking status, tumor grade, tumor stage, year of tumor diagnosis, energy intake, Ca intake, folate intake, alcohol intake, and education |
| All-cause mortality | 31.2 vs. 14.5 g/day | 0.84 (0.66–1.06) | |||||||
| Zhao 2022 Canada | Association between dietary fiber intake and mortality among colorectal cancer survivors: results from the Newfoundland familial colorectal cancer cohort study and a meta-analysis of prospective studies | 504 participants | 159 deaths; 83 deaths from CRC | 6.4 years (median) | CRC-specific mortality | Fiber | 30.1 vs. 13.4 g/day (male) | 0.60 (0.26–1.38) (male) | Age at diagnosis, sex, stage at diagnosis, marital status, microsatellite instable status, BRAF mutation status, chemoradiotherapy, and total energy intake |
| 31.1 vs. 14.5 g/day (female) | 1.25 (0.31–5.08) (female) | ||||||||
| All-cause mortality | 30.1 vs. 13.4 g/day (male) | 0.76 (0.43–1.37) (male) | |||||||
| 31.1 vs. 14.5 g/day (female) | 0.90 (0.34–2.29) (female) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, J.; Zhu, Y.; Du, M.; Wang, Y.; Vallis, J.; Parfrey, P.S.; Mclaughlin, J.R.; Qi, X.; Wang, P.P. Association between Dietary Fiber Intake and Mortality among Colorectal Cancer Survivors: Results from the Newfoundland Familial Colorectal Cancer Cohort Study and a Meta-Analysis of Prospective Studies. Cancers 2022, 14, 3801. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153801
Zhao J, Zhu Y, Du M, Wang Y, Vallis J, Parfrey PS, Mclaughlin JR, Qi X, Wang PP. Association between Dietary Fiber Intake and Mortality among Colorectal Cancer Survivors: Results from the Newfoundland Familial Colorectal Cancer Cohort Study and a Meta-Analysis of Prospective Studies. Cancers. 2022; 14(15):3801. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153801
Chicago/Turabian StyleZhao, Jing, Yun Zhu, Meizhi Du, Yu Wang, Jillian Vallis, Patrick S. Parfrey, John R. Mclaughlin, Xiuying Qi, and Peizhong Peter Wang. 2022. "Association between Dietary Fiber Intake and Mortality among Colorectal Cancer Survivors: Results from the Newfoundland Familial Colorectal Cancer Cohort Study and a Meta-Analysis of Prospective Studies" Cancers 14, no. 15: 3801. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14153801