
External Validation of the Individualized Prediction of Breast Cancer Survival (IPBS) Model for Estimating Survival after Surgery for Patients with Breast Cancer in Northern Thailand
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
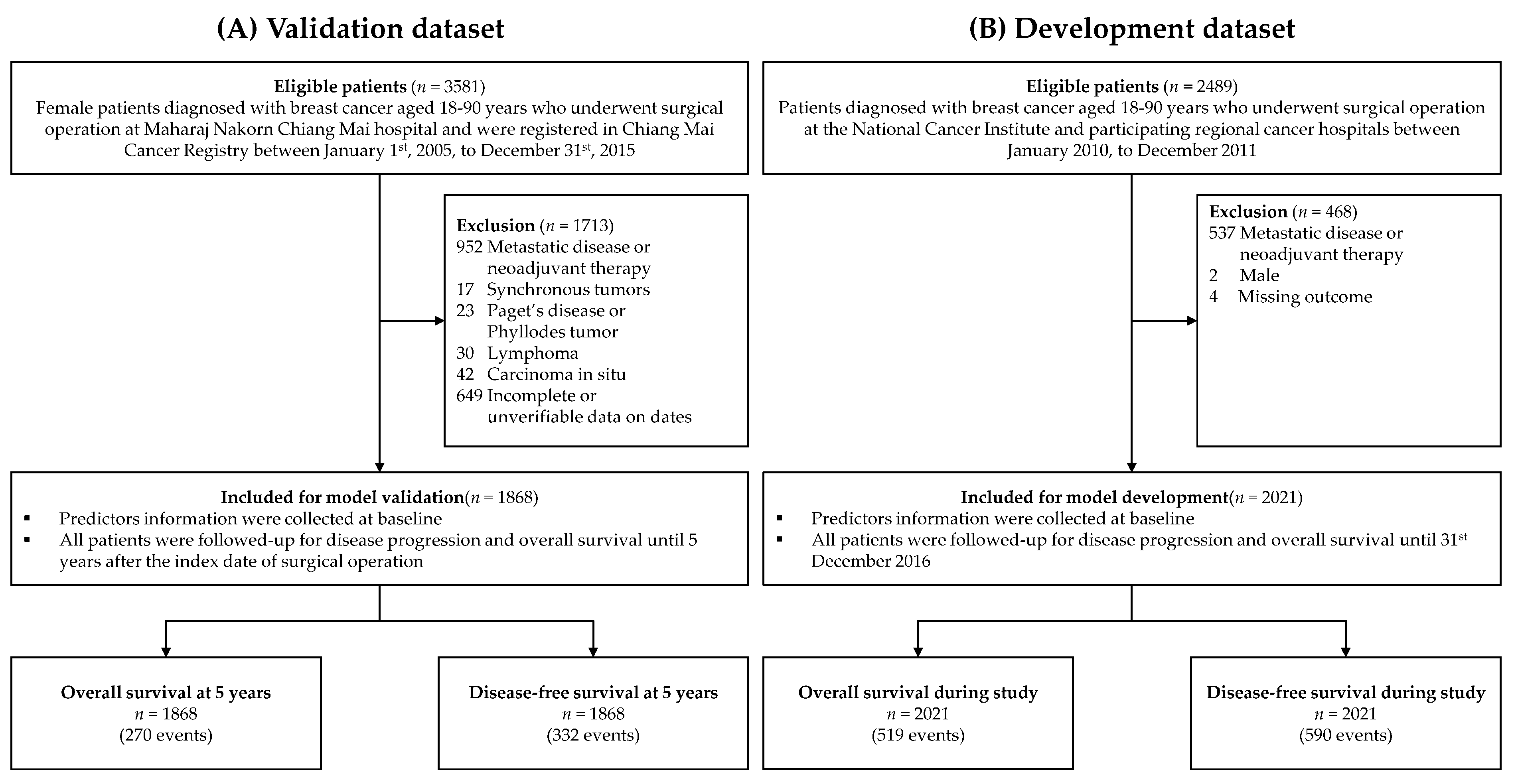
2.1. Study Design
2.2. Study Patients
2.3. Data Collection
2.4. The IPBS Model
2.5. Study Outcomes
2.6. Statistical Analyses
2.6.1. Study Size Estimation
2.6.2. Handling of Missing Data
2.6.3. Descriptive and Comparative Analysis
2.6.4. Evaluation of External Performance
3. Results
3.1. Patient Characteristics
3.2. Predictor–Outcome Associations
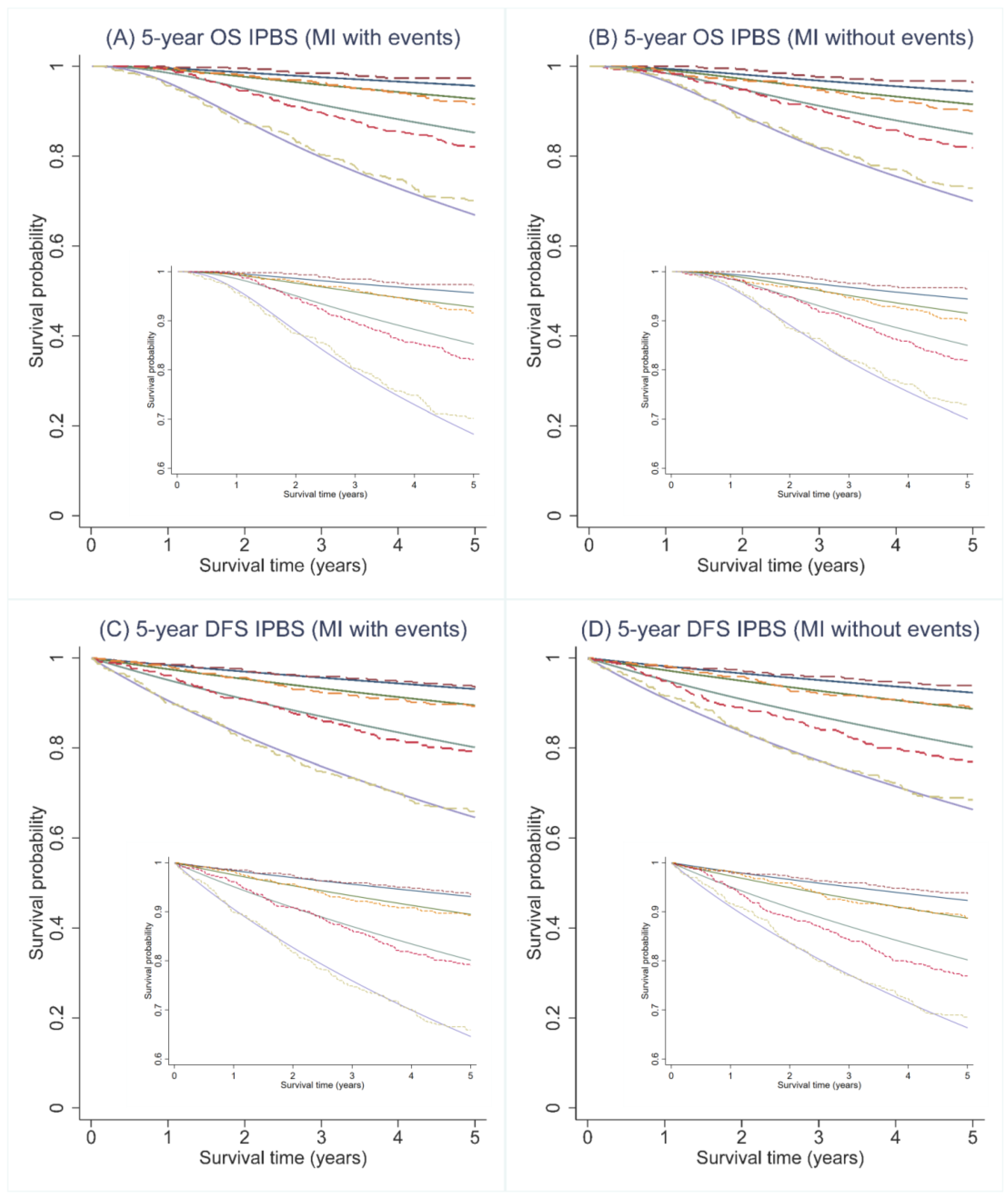
3.3. External Discrimination
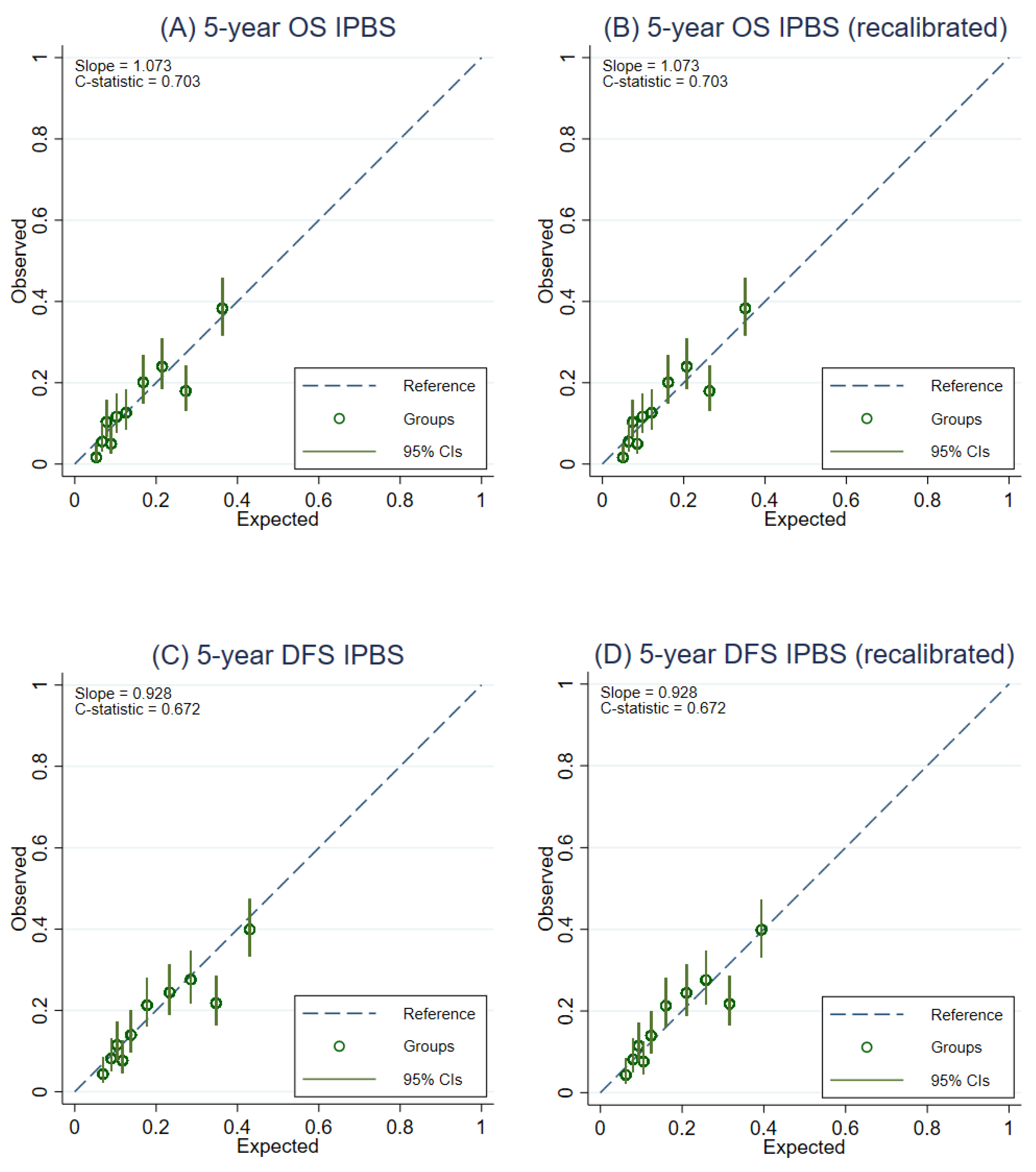
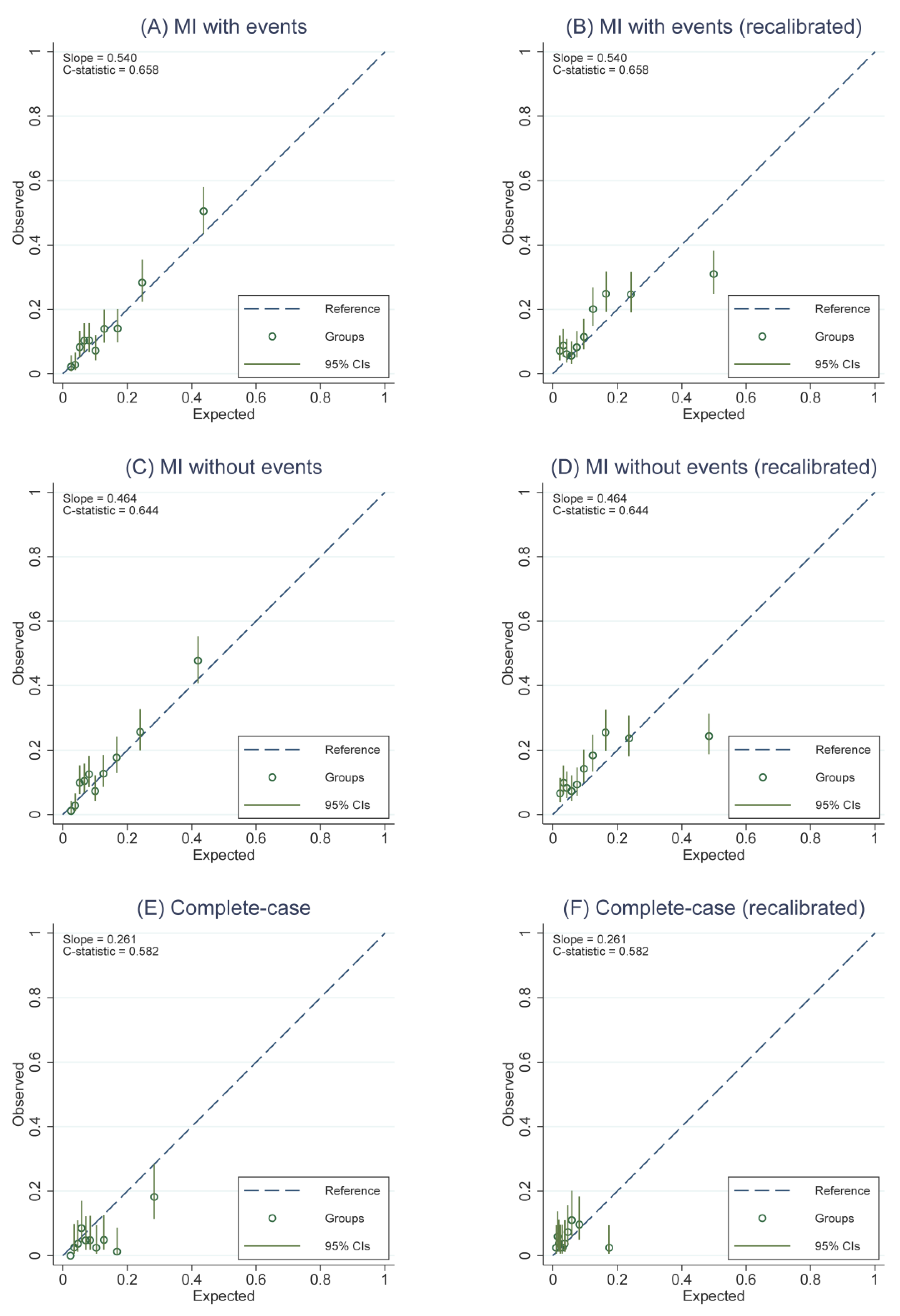
3.4. External Calibration
3.5. Model Recalibration
3.6. Exploratory Subgroup Analysis of Model Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Predictors | Detail | Input Value |
|---|---|---|---|
| AGE | Age at surgery (year) | AGE = age at surgery–50 | |
| MENO | Menopausal status | Pre-menopause | MENO = 0 |
| Post-menopause | MENO = 1 | ||
| SURG | Type of surgery | Mastectomy | SURG = 0 |
| Breast conserving surgery (BCS) | SURG = 1 | ||
| STG | Pathological stage | ||
| I | STG2 = 0, STG3 = 0 | ||
| II | STG2 = 1, STG3 = 0 | ||
| III | STG2 = 0, STG3 = 1 | ||
| HIST | Histological type | Others, | HIST = 0 |
| Ductal | HIST = 1 | ||
| GRD | Histological grade | ||
| I | GRD2 = 0, GRD3 = 0 | ||
| II | GRD2 = 1, GRD3 = 0 | ||
| III | GRD2 = 0, GRD3 = 1 | ||
| SIZE | Tumor size (mm) | SIZE = tumor size—30 | |
| LVI | Lympho-vascular invasion | No, | LVI = 0 |
| Yes | LVI = 1 | ||
| NODE | Number of positive axillary lymph nodes (node) | ||
| 0 | NODE2 = 0, NODE3 = 0 | ||
| 1–3 | NODE2 = 1, NODE3 = 0 | ||
| ≥4 | NODE2 = 0, NODE3 = 1 | ||
| ER | Estrogen receptor status | Negative | ER = 0 |
| Positive | ER = 1 | ||
| PR | Progesterone receptor status | Negative | PR = 0 |
| Positive | PR = 1 | ||
| HER2 | HER-2 status | Negative | HER2 = 0 |
| Positive | HER2 = 1 | ||
| CHEM | Chemotherapy | CHEM = 0.839 | |
| HORM | Hormonal therapy | HORM = 0.539 | |
| RADI | Radiotherapy | RADI = 0.579 | |
| OS5 | Baseline 5-year overall survival probability | 0.893 | |
| DFS5 | Baseline 5-year disease-free survival probability | 0.889 | |
| PIOS | Prognostic index of OS | 0.0001 × AGE + 0.1681 × MENO − 0.2428×SURG + 0.0398 × STG2 + 0.5962 × STG3 + 0.4004 × HIST + 0.0021 × SIZE + 0.4655 × NODE2 + 0.8066 × NODE3 + 0.2071 × LVI + 0.1737 × GRD2 + 0.3126 × GRD3 − 0.1122 × ER − 0.1037 × PR + 0.0714 × HER2 − 0.4421 × CHEM − 0.5539 × HORM − 0.0246 × RADI | |
| PIDFS | Prognostic index of DFS | 0.0018 × AGE + 0.1510 × MENO − 0.1956 × SURG + 0.2018 × STG2 + 0.6774 × STG3 + 0.3416 × HIST + 0.0016 × SIZE + 0.5409 × NODE2 + 0.7573 × NODE3 + 0.2435 × LVI + 0.3422 × GRD2 + 0.4226 × GRD3 − 0.1073 × ER − 0.0358×PR + 0.0973 × HER2 − 0.5737 × CHEM − 0.4825×HORM + 0.0050×RADI | |
| Overall survival probability at 5-year | OS5exp(PIOS) | ||
| Disease-free survival probability at 5 years | DFS5exp(PIDFS) | ||
| Variable | Predictors | Input value | Log HR |
|---|---|---|---|
| Model for breast cancer specific mortality for ER-negative breast cancer patients | |||
| AGE_ERneg | Age at surgery (year) | Age–56.325 | 0.00894 |
| SIZE_ERneg | Tumor size (mm) | (Tumor size /100)1/2 − 0.5090 | 2.109 |
| NODES_ERneg | Number of positive axillary lymph nodes (node) | 1/[(Number of nodes + 1)/10]1/2 − 1.72 | −0.705 |
| GRADE_ERneg | Histological grade | Histological grade (1,2,3) | 0.259 |
| PIOS for ER- | Prognostic index of OS for ER-negative patients | 0.00894 × AGE_ERneg + 2.109 × (SIZE_ERneg) + (−0.705 × NODES_ERneg) + 0.259 × GRADE_ERneg | |
| Model for breast cancer specific mortality for ER-positive breast cancer patients | |||
| AGE_Erpos1 | Age at surgery (year) | (Age /10)−2 − 0.0287 | 34.53 |
| AGE_Erpos2 | Age at surgery (year) | (Age /10)−2 × ln(Age/10) − 0.0510 | −34.20 |
| SIZE_Erpos | Tumor size (mm) | ln(Tumor size /100) + 1.5452 | 0.7531 |
| NODES_Erpos | Number of positive axillary lymph nodes (node) | ln((Nodes + 1)/10) + 1.3876 | 0.7069 |
| GRADE_Erpos | Histological grade | Histological grade (1,2,3) | 0.7467 |
| SCREEN | Screen-detected | Not screen detected (0) | −0.2763 |
| PIOS for ER+ | Prognostic index of OS for ER-positive patients | (34.53 × AGE_Erpos1) + (−34.20 × AGE_ERpos2) + 0.7531 × SIZE_ERpos + 0.7069 × NODES_ERpos + 0.7467×GRADE_ERpos + (−0.2763 × 0) | |
| Model for non-specific mortality | |||
| AGE_nonbreast | Age at surgery (year) | (Age/10)2 − 34.234 | 0.0698 |
| PIOS for non-breast | Prognostic index for non-specific mortality | AGE_nonbreast × 0.0698 | |
| BS5 | Breast cancer specific mortality at 5 years | ER-negative patients | 0.9805221 |
| ER-positive patients | 0.8531408 | ||
| NBS5 | Non-breast cancer specific mortality at 5 years | 0.9726993 | |
| Overall survival probability at 5-year | ER-negative patients | BS5exp(PIOS for ER-) × NBS5 exp(PIOS for non-breast) | |
| ER-positive patients | BS5exp(PIOS for ER+) × NBS5 exp(PIOS for non-breast) | ||
| IPBS Model | PREDICT v2 | |||||
|---|---|---|---|---|---|---|
| 5-Year OS | 5-Year DFS | 5-Year OS | ||||
| C-Statistics | Calibration Slope | C-Statistics | Calibration Slope | C-Statistics | Calibration Slope | |
| Overall | 0.728 (0.714–0.742) * | 1.052 | 0.689 (0.677–0.697) * | 1.112 | 0.658 (0.638–0.672) | 0.540 |
| Histological subtype | ||||||
| Others | 0.733 | 1.300 | 0.693 | 1.000 | 0.709 | 0.727 |
| Ductal | 0.735 | 1.321 | 0.695 | 1.124 | 0.659 | 0.494 |
| Pathological stage | ||||||
| I | 0.748 | 2.465 | 0.712 | 2.026 | 0.648 | 0.801 |
| II | 0.696 | 1.570 | 0.656 | 1.268 | 0.618 | 0.440 |
| III | 0.658 | 1.486 | 0.642 | 1.416 | 0.567 | 0.240 |
Appendix B




References
- Lei, S.; Zheng, R.; Zhang, S.; Wang, S.; Chen, R.; Sun, K.; Zeng, H.; Zhou, J.; Wei, W. Global Patterns of Breast Cancer Incidence and Mortality: A Population-based Cancer Registry Data Analysis from 2000 to 2020. Cancer Commun. 2021, 41, 1183–1194. [Google Scholar] [CrossRef] [PubMed]
- Soerjomataram, I.; Bray, F. Planning for Tomorrow: Global Cancer Incidence and the Role of Prevention 2020–2070. Nat. Rev. Clin. Oncol. 2021, 18, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Laversanne, M.; Brewster, D.H.; Gombe Mbalawa, C.; Kohler, B.; Piñeros, M.; Steliarova-Foucher, E.; Swaminathan, R.; Antoni, S.; et al. Cancer Incidence in Five Continents: Inclusion Criteria, Highlights from Volume X and the Global Status of Cancer Registration. Int. J. Cancer 2015, 137, 2060–2071. [Google Scholar] [CrossRef]
- Wilkinson, L.; Gathani, T. Understanding Breast Cancer as a Global Health Concern. Br. J. Radiol. 2022, 95, 20211033. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global Surveillance of Trends in Cancer Survival 2000–14 (CONCORD-3): Analysis of Individual Records for 37,513,025 Patients Diagnosed with One of 18 Cancers from 322 Population-Based Registries in 71 Countries. Lancet Lond. Engl. 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Kuo, Y.; Shih, Y.C.T.; Giordano, S.H.; Berenson, A.B. Trends in Breast Cancer Mortality by Stage at Diagnosis among US Young Women. Cancer 2018, 124, 3500–3509. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G. Prognostic Models: A Methodological Framework and Review of Models for Breast Cancer. Cancer Investing. 2009, 27, 235–243. [Google Scholar] [CrossRef]
- Steyerberg, E. Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating. In Statistics for Biology and Health; Springer: New York, NY, USA, 2009; ISBN 978-0-387-77243-1. [Google Scholar]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. BMC Med. 2015, 13, 214. [Google Scholar] [CrossRef] [Green Version]
- Haybittle, J.L.; Blamey, R.W.; Elston, C.W.; Johnson, J.; Doyle, P.J.; Campbell, F.C.; Nicholson, R.I.; Griffiths, K. A Prognostic Index in Primary Breast Cancer. Br. J. Cancer 1982, 45, 361–366. [Google Scholar] [CrossRef] [Green Version]
- Ravdin, P.M.; Siminoff, L.A.; Davis, G.J.; Mercer, M.B.; Hewlett, J.; Gerson, N.; Parker, H.L. Computer Program to Assist in Making Decisions about Adjuvant Therapy for Women with Early Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 980–991. [Google Scholar] [CrossRef]
- Campbell, H.E.; Gray, A.M.; Harris, A.L.; Briggs, A.H.; Taylor, M.A. Estimation and External Validation of a New Prognostic Model for Predicting Recurrence-Free Survival for Early Breast Cancer Patients in the UK. Br. J. Cancer 2010, 103, 776–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wishart, G.C.; Bajdik, C.D.; Azzato, E.M.; Dicks, E.; Greenberg, D.C.; Rashbass, J.; Caldas, C.; Pharoah, P.D.P. A Population-Based Validation of the Prognostic Model PREDICT for Early Breast Cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2011, 37, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Polchai, N.; Sa-nguanraksa, D.; Numprasit, W.; Thumrongtaradol, T.; O-charoenrat, E.; O-charoenrat, P. A Comparison Between the Online Prediction Models CancerMath and PREDICT as Prognostic Tools in Thai Breast Cancer Patients. Cancer Manag. Res. 2020, 12, 5549–5559. [Google Scholar] [CrossRef] [PubMed]
- Pongnikorn, D.; Phinyo, P.; Patumanond, J.; Daoprasert, K.; Phothong, P.; Siribumrungwong, B. Individualized Prediction of Breast Cancer Survival Using Flexible Parametric Survival Modeling: Analysis of a Hospital-Based National Clinical Cancer Registry. Cancers 2021, 13, 1567. [Google Scholar] [CrossRef] [PubMed]
- Gourgou-Bourgade, S.; Cameron, D.; Poortmans, P.; Asselain, B.; Azria, D.; Cardoso, F.; A’Hern, R.; Bliss, J.; Bogaerts, J.; Bonnefoi, H.; et al. Guidelines for Time-to-Event End Point Definitions in Breast Cancer Trials: Results of the DATECAN Initiative (Definition for the Assessment of Time-to-Event Endpoints in CANcer Trials)†. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Ogundimu, E.O.; Altman, D.G. Sample Size Considerations for the External Validation of a Multivariable Prognostic Model: A Resampling Study. Stat. Med. 2016, 35, 214–226. [Google Scholar] [CrossRef] [Green Version]
- von Hippel, P.T. How Many Imputations Do You Need? A Two-Stage Calculation Using a Quadratic Rule. Sociol. Methods Res. 2020, 49, 699–718. [Google Scholar] [CrossRef] [Green Version]
- Marshall, A.; Altman, D.G.; Holder, R.L.; Royston, P. Combining Estimates of Interest in Prognostic Modelling Studies after Multiple Imputation: Current Practice and Guidelines. BMC Med. Res. Methodol. 2009, 9, 57. [Google Scholar] [CrossRef] [Green Version]
- Hoogland, J.; van Barreveld, M.; Debray, T.P.A.; Reitsma, J.B.; Verstraelen, T.E.; Dijkgraaf, M.G.W.; Zwinderman, A.H. Handling Missing Predictor Values When Validating and Applying a Prediction Model to New Patients. Stat. Med. 2020, 39, 3591–3607. [Google Scholar] [CrossRef]
- Austin, P.C. Balance Diagnostics for Comparing the Distribution of Baseline Covariates between Treatment Groups in Propensity-Score Matched Samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Candido dos Reis, F.J.; Wishart, G.C.; Dicks, E.M.; Greenberg, D.; Rashbass, J.; Schmidt, M.K.; van den Broek, A.J.; Ellis, I.O.; Green, A.; Rakha, E.; et al. An Updated PREDICT Breast Cancer Prognostication and Treatment Benefit Prediction Model with Independent Validation. Breast Cancer Res. 2017, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Booth, S.; Riley, R.D.; Ensor, J.; Lambert, P.C.; Rutherford, M.J. Temporal Recalibration for Improving Prognostic Model Development and Risk Predictions in Settings Where Survival Is Improving over Time. Int. J. Epidemiol. 2020, 49, 1316–1325. [Google Scholar] [CrossRef] [Green Version]
- Van Calster, B.; McLernon, D.J.; van Smeden, M.; Wynants, L.; Steyerberg, E.W.; Bossuyt, P.; Collins, G.S.; Macaskill, P.; McLernon, D.J.; Moons, K.G.M.; et al. Calibration: The Achilles Heel of Predictive Analytics. BMC Med. 2019, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- Debray, T.P.A.; Vergouwe, Y.; Koffijberg, H.; Nieboer, D.; Steyerberg, E.W.; Moons, K.G.M. A New Framework to Enhance the Interpretation of External Validation Studies of Clinical Prediction Models. J. Clin. Epidemiol. 2015, 68, 279–289. [Google Scholar] [CrossRef] [Green Version]
- Janssen, K.J.M.; Moons, K.G.M.; Kalkman, C.J.; Grobbee, D.E.; Vergouwe, Y. Updating Methods Improved the Performance of a Clinical Prediction Model in New Patients. J. Clin. Epidemiol. 2008, 61, 76–86. [Google Scholar] [CrossRef]
- Riley, R.D.; Ensor, J.; Snell, K.I.E.; Debray, T.P.A.; Altman, D.G.; Moons, K.G.M.; Collins, G.S. External Validation of Clinical Prediction Models Using Big Datasets from E-Health Records or IPD Meta-Analysis: Opportunities and Challenges. BMJ 2016, 353, i3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steif, J.; Brant, R.; Sreepada, R.S.; West, N.; Murthy, S.; Görges, M. Prediction Model Performance With Different Imputation Strategies: A Simulation Study Using a North American ICU Registry. Pediatr. Crit. Care Med. 2022, 23, e29. [Google Scholar] [CrossRef] [PubMed]




| Characteristics | Validation Dataset | Development Dataset | STD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 1868) | 5-Year OS | p-Value | Total (n = 2021) | 5-Year OS | p-Value | ||||
| n (%) | (%) | 95% CI | n (%) | (%) | 95% CI | ||||
| Age at surgery (year, mean ± SD) | 52.9 ± 11.0 | 50.4 ± 10.6 | |||||||
| <50 | 768 (41.1) | 88.0 | 85.5–90.1 | 0.004 | 1020 (50.5) | 80.5 | NR | 0.001 | 0.189 |
| ≥50 | 1100 (58.9) | 65.0 | 59.1–70.9 | 1001 (49.5) | 75.2 | NR | |||
| Menopausal status | |||||||||
| Premenopause | 619 (33.1) | 88.7 | 85.9–91.0 | <0.001 | 903 (44.7) | 80.2 | NR | 0.012 | 0.401 |
| Postmenopause | 927 (49.6) | 82.2 | 79.5–84.5 | 996 (49.3) | 75.4 | NR | |||
| Unknown | 322 (17.2) | 112 (6.0) | |||||||
| Pathological stage | |||||||||
| I | 431 (23.1) | 97.4 | 95.4–98.6 | <0.001 | 286 (14.2) | 91.3 | NR | <0.001 | 0.933 |
| II | 580 (31.1) | 93.1 | 90.6–94.9 | 979 (48.4) | 84.9 | NR | |||
| III | 366 (19.6) | 88.5 | 84.7–91.4 | 744 (26.8) | 63.8 | NR | |||
| Unknown | 491 (26.3) | 12 (0.6) | |||||||
| Histological type | |||||||||
| Ductal | 1370 (73.3) | 89.0 | 87.2–90.6 | 0.011 | 1915 (94.8) | 77.7 | NR | 0.140 | 0.629 |
| Other types | 376 (20.1) | 93.5 | 90.5–95.6 | 106 (5.2) | 82.1 | NR | |||
| Unknown | 122 (6.5) | ||||||||
| Histological grade | |||||||||
| I | 76 (4.1) | 94.5 | 86.1–97.9 | 0.005 | 277 (13.7) | 85.2 | NR | <0.001 | 0.562 |
| II | 866 (46.4) | 91.7 | 89.6–93.4 | 955 (47.2) | 80.0 | NR | |||
| III | 638 (34.2) | 87.1 | 84.2–89.5 | 652 (47.2) | 72.2 | NR | |||
| Unknown | 288 (15.4) | 53 (2.6) | |||||||
| Tumor size (mm) | |||||||||
| <30 | 1119 (59.9) | 91.0 | 89.1–92.5 | <0.001 | 1014 (50.2) | 82.6 | NR | <0.001 | 0.349 |
| ≥30 | 649 (34.7) | 77.5 | 74.0–80.5 | 1205 (59.6) | 73.6 | NR | |||
| Unknown | 100 (5.4) | 132 (6.5) | |||||||
| LVI | |||||||||
| Yes | 739 (39.6) | 83.2 | 80.3–85.7 | <0.001 | 684 (33.9) | 70.0 | NR | <0.001 | 0.325 |
| No | 860 (46.0) | 92.6 | 90.6–94.2 | 1205 (59.6) | 82.0 | NR | |||
| Unknown | 269 (14.4) | 132 (6.5) | |||||||
| Node | |||||||||
| 0 | 950 (50.9) | 93.1 | 91.3–94.6 | <0.001 | 838 (41.5) | 88.5 | NR | <0.001 | 0.505 |
| 1–3 | 433 (23.2) | 85.7 | 82.0–88.7 | 524 (25.9) | 80.3 | NR | |||
| ≥4 | 351 (18.8) | 68.3 | 63.1–72.9 | 659 (32.6) | 62.4 | NR | |||
| Unknown | 134 (7.2) | ||||||||
| ER | |||||||||
| Positive | 1067 (57.1) | 90.5 | 88.5–92.1 | <0.001 | 1237 (61.2) | 82.7 | NR | <0.001 | 0.174 |
| Negative | 670 (35.9) | 80.1 | 76.9–83.0 | 718 (35.5) | 69.6 | NR | |||
| Unknown | 131 (7.01) | 66 (3.3) | |||||||
| PR | |||||||||
| Positive | 930 (49.8) | 91.5 | 89.5–93.1 | <0.001 | 1026 (50.8) | 84.1 | NR | <0.001 | 0.165 |
| Negative | 805 (43.1) | 80.7 | 77.8–83.3 | 925 (45.8) | 71.1 | NR | |||
| Unknown | 133 (7.1) | 70 (3.4) | |||||||
| HER-2 status | |||||||||
| Positive | 760 (40.7) | 86.0 | 83.4–88.3 | 0.417 | 687 (34.0) | 74.5 | NR | 0.001 | 0.158 |
| Negative | 960 (51.4) | 87.4 | 85.1–89.4 | 1110 (54.9) | 80.6 | NR | |||
| Unknown | 148 (7.9) | 224 (11.1) | |||||||
| Type of surgery | |||||||||
| Mastectomy | 1412 (75.6) | 89.2 | 87.4–90.7 | 0.076 | 1758 (87.0) | 76.3 | NR | <0.001 | 0.442 |
| BCS | 304 (16.3) | 92.5 | 88.9–95.0 | 263 (13.0) | 88.2 | NR | |||
| Unknown | 152 (8.1) | ||||||||
| Chemotherapy | |||||||||
| Yes | 1443 (77.3) | 84.4 | 82.4–86.1 | 0.041 | 1696 (83.9) | 78.1 | NR | 0.685 | 0.246 |
| No | 385 (20.6) | 88.7 | 85.0–91.5 | 325 (16.1) | 76.9 | NR | |||
| Unknown | 40 (2.1) | ||||||||
| Hormonal therapy | |||||||||
| Yes | 1058 (56.6) | 90.2 | 88.2–91.8 | <0.001 | 1053 (52.1) | 85.5 | NR | <0.001 | 0.137 |
| No | 717 (38.4) | 78.4 | 75.2–81.2 | 900 (44.5) | 69.8 | NR | |||
| Unknown | 93 (5.0) | 69 (3.4) | |||||||
| Targeted therapy | |||||||||
| Yes | 131 (7.0) | 85.4 | 78.1–90.4 | 0.929 | NR | NR | NR | NR | - |
| No | 1670 (89.4) | 85.3 | 83.5–87.0 | NR | NR | NR | |||
| Unknown | 67 (3.6) | ||||||||
| RT | |||||||||
| Yes | 1018 (54.5) | 81.9 | 79.4–84.2 | <0.001 | 1126 (55.7) | 75.1 | NR | <0.001 | 0.078 |
| No | 802 (42.9) | 89.7 | 87.3–91.6 | 819 (40.5) | 82.3 | NR | |||
| Unknown | 48 (2.6) | 76 (3.8) | |||||||
| Expected: Observed (E:O) Ratio | Calibration Slope | C-Statistics from Validation Dataset (Median, Range *) | C-Statistics from Development Dataset | |
|---|---|---|---|---|
| Multiple imputations including cumulative hazard of events (n = 1868) | ||||
| 5-year OS | ||||
| IPBS | 1.052 | 1.277 | 0.728 (0.714–0.742) | 0.72 |
| Recalibrated IPBS | 1.009 | 1.277 | 0.728 (0.714–0.742) | |
| PREDICT | 0.907 | 0.540 | 0.658 (0.638–0.672) | |
| Recalibrated PREDICT | 0.901 | 0.540 | 0.658 (0.638–0.672) | |
| 5-year DFS | ||||
| IPBS | 1.112 | 1.072 | 0.689 (0.677–0.697) | 0.70 |
| Recalibrated IPBS | 0.996 | 1.072 | 0.689 (0.677–0.697) | |
| Multiple imputations not including cumulative hazard of events (n = 1868) | ||||
| 5-year OS | ||||
| IPBS | 1.046 | 1.073 | 0.706 (0.693–0.722) | 0.72 |
| Recalibrated IPBS | 1.009 | 1.073 | 0.706 (0.693–0.722) | |
| PREDICT | 0.899 | 0.464 | 0.644 (0.633–0.656) | |
| Recalibrated PREDICT | 0.912 | 0.464 | 0.644 (0.633–0.656) | |
| 5-year DFS | ||||
| IPBS | 1.107 | 0.928 | 0.675 (0.663–0.685) | 0.70 |
| Recalibrated IPBS | 1.003 | 0.928 | 0.675 (0.663–0.685) | |
| Excluding patients with incomplete data on predictors (complete-case analysis) (n = 837) | ||||
| 5-year OS | ||||
| IPBS | 2.471 | 0.901 | 0.665 (0.585, 0.745) † | 0.72 |
| Recalibrated IPBS | 0.999 | 0.901 | 0.665 (0.585, 0.745) † | |
| PREDICT | 1.954 | 0.261 | 0.582 (0.499, 0.664) † | |
| Recalibrated PREDICT | 0.967 | 0.261 | 0.582 (0.499, 0.664) † | |
| 5-year DFS | ||||
| IPBS | 1.541 | 0.652 | 0.625 (0.562, 0.689) † | 0.70 |
| Recalibrated IPBS | 0.987 | 0.652 | 0.625 (0.562, 0.689) † | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charumporn, T.; Jarupanich, N.; Rinthapon, C.; Meetham, K.; Pattayakornkul, N.; Taerujjirakul, T.; Tanasombatkul, K.; Ditsatham, C.; Chongruksut, W.; Phanphaisarn, A.; et al. External Validation of the Individualized Prediction of Breast Cancer Survival (IPBS) Model for Estimating Survival after Surgery for Patients with Breast Cancer in Northern Thailand. Cancers 2022, 14, 5726. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14235726
Charumporn T, Jarupanich N, Rinthapon C, Meetham K, Pattayakornkul N, Taerujjirakul T, Tanasombatkul K, Ditsatham C, Chongruksut W, Phanphaisarn A, et al. External Validation of the Individualized Prediction of Breast Cancer Survival (IPBS) Model for Estimating Survival after Surgery for Patients with Breast Cancer in Northern Thailand. Cancers. 2022; 14(23):5726. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14235726
Chicago/Turabian StyleCharumporn, Thanapat, Nutcha Jarupanich, Chanawin Rinthapon, Kantapit Meetham, Napat Pattayakornkul, Teerapant Taerujjirakul, Krittai Tanasombatkul, Chagkrit Ditsatham, Wilaiwan Chongruksut, Areerak Phanphaisarn, and et al. 2022. "External Validation of the Individualized Prediction of Breast Cancer Survival (IPBS) Model for Estimating Survival after Surgery for Patients with Breast Cancer in Northern Thailand" Cancers 14, no. 23: 5726. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14235726