
18F-Fluorodeoxyglucose PET/CT for Early Prediction of Outcomes in Patients with Advanced Lung Adenocarcinomas and EGFR Mutations Treated with First-Line EGFR-TKIs

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials & Methods
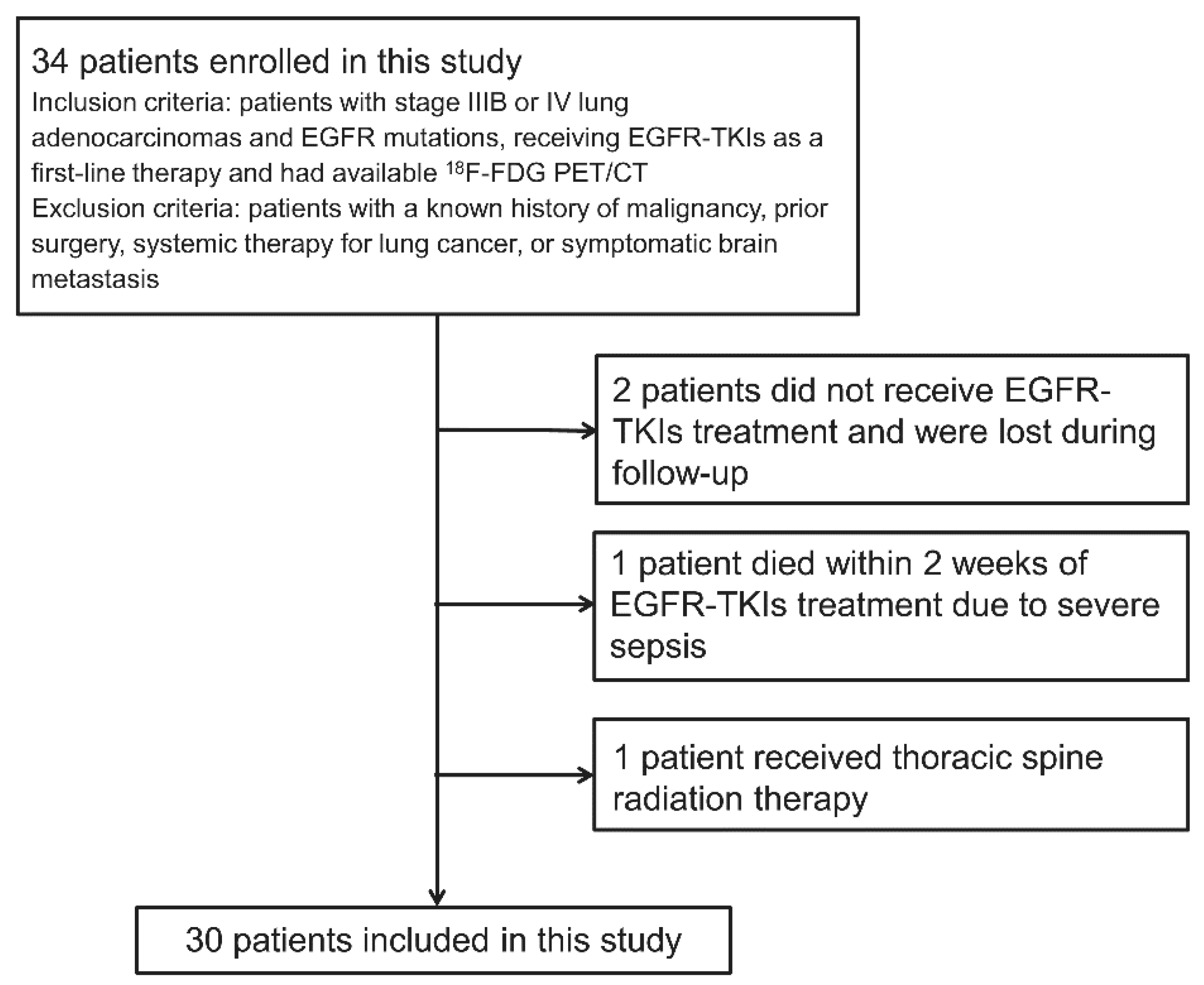
2.1. Patients
2.2. 18F-FDG PET/CT Image Acquisition
2.3. 18F-FDG PET/CT Image Analysis
2.4. Response Assessment Based on 18F-FDG PET/CT
2.5. Response Assessment Based on CT
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
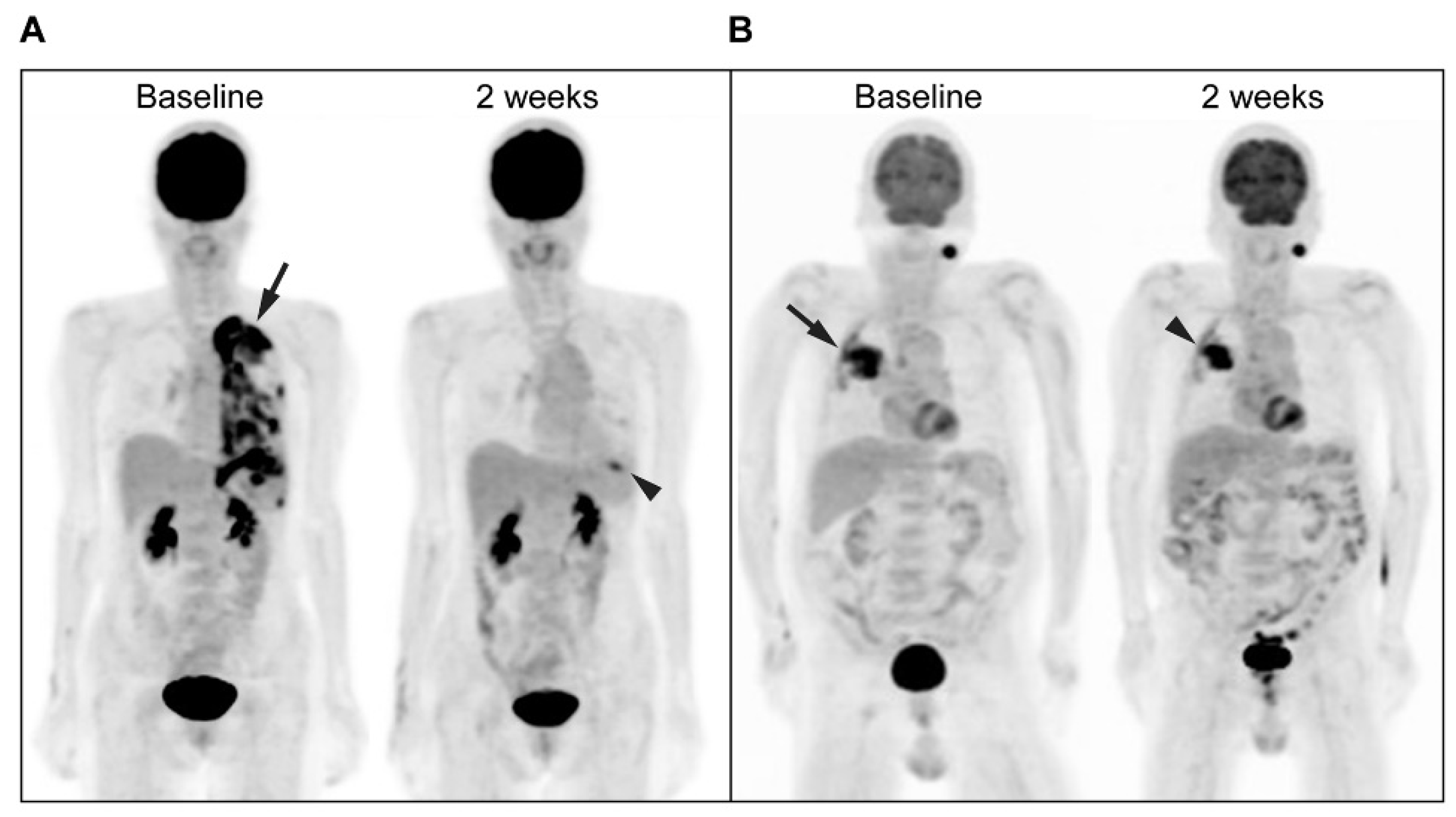
3.2. Treatment Response Evaluation
3.3. PFS Evaluation
3.4. OS Evaluation
3.5. Correlation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data availability Statement
Acknowledgments
Conflicts of Interest
References
- Arteaga, C.L. The epidermal growth factor receptor: From mutant oncogene in nonhuman cancers to therapeutic target in human neoplasia. J. Clin. Oncol. 2001, 19, 32s–40s. [Google Scholar] [PubMed]
- Yarden, Y.; Sliwkowski, M.X. Untangling the ErbB signalling network. Nat. Rev. Mol. Cell Biol. 2001, 2, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.V.; Bell, D.W.; Settleman, J.; Haber, D.A. Epidermal growth factor receptor mutations in lung cancer. Nat. Rev. Cancer 2007, 7, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Wakeling, A.E.; Guy, S.P.; Woodburn, J.R.; Ashton, S.E.; Curry, B.J.; Barker, A.J.; Gibson, K.H. ZD1839 (Iressa): An orally active inhibitor of epidermal growth factor signaling with potential for cancer therapy. Cancer Res. 2002, 62, 5749–5754. [Google Scholar]
- Ciardiello, F.; Caputo, R.; Bianco, R.; Damiano, V.; Pomatico, G.; Placido, S.D.; Bianco, A.R.; Tortora, G. Antitumor effect and potentiation of cytotoxic drugs activity in human cancer cells by ZD-1839 (Iressa), an epidermal growth factor receptor-selective tyrosine kinase inhibitor. Clin. Cancer Res. 2000, 6, 2053–2063. [Google Scholar]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Fukuoka, M.; Wu, Y.L.; Thongprasert, S.; Sunpaweravong, P.; Leong, S.S.; Sriuranpong, V.; Chao, T.Y.; Nakagawa, K.; Chu, D.T.; Saijo, N.; et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J. Clin. Oncol. 2011, 29, 2866–2874. [Google Scholar] [CrossRef]
- Chan, B.A.; Hughes, B.G. Targeted therapy for non-small cell lung cancer: Current standards and the promise of the future. Transl. Lung Cancer Res. 2015, 4, 36–54. [Google Scholar]
- Noronha, V.; Prabhash, K.; Thavamani, A.; Chougule, A.; Purandare, N.; Joshi, A.; Sharma, R.; Desai, S.; Jambekar, N.; Dutt, A.; et al. EGFR mutations in Indian lung cancer patients: Clinical correlation and outcome to EGFR targeted therapy. PLoS ONE 2013, 8, e61561. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [Green Version]
- Ladanyi, M.; Pao, W. Lung adenocarcinoma: Guiding EGFR-targeted therapy and beyond. Mod. Pathol. 2008, 21, S16–S22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Zhang, J.; Fujimoto, J.; Zhang, J.; Wedge, D.C.; Song, X.; Zhang, J.; Seth, S.; Chow, C.W.; Cao, Y.; Gumbs, C.; et al. Intratumor heterogeneity in localized lung adenocarcinomas delineated by multiregion sequencing. Science 2014, 346, 256–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruin, E.C.; McGranahan, N.; Mitter, R.; Salm, M.; Wedge, D.C.; Yates, L.; Jamal-Hanjani, M.; Shafi, S.; Murugaesu, N.; Rowan, A.J.; et al. Spatial and temporal diversity in genomic instability processes defines lung cancer evolution. Science 2014, 346, 251–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gridelli, C.; De Marinis, F.; Di Maio, M.; Cortinovis, D.; Cappuzzo, F.; Mok, T. Gefitinib as first-line treatment for patients with advanced non-small-cell lung cancer with activating epidermal growth factor receptor mutation: Implications for clinical practice and open issues. Lung Cancer 2011, 72, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Okami, J.; Kodama, K.; Higashiyama, M.; Kato, K. Intratumor heterogeneity of epidermal growth factor receptor mutations in lung cancer and its correlation to the response to gefitinib. Cancer Sci. 2008, 99, 929–935. [Google Scholar] [CrossRef]
- Tuma, R.S. Sometimes size doesn’t matter: Reevaluating RECIST and tumor response rate endpoints. J. Natl. Cancer Inst. 2006, 98, 1272–1274. [Google Scholar] [CrossRef]
- Lardinois, D.; Weder, W.; Hany, T.F.; Kamel, E.M.; Korom, S.; Seifert, B.; von Schulthess, G.K.; Steinert, H.C. Staging of non-small-cell lung cancer with integrated positron-emission tomography and computed tomography. N. Engl. J. Med. 2003, 348, 2500–2507. [Google Scholar] [CrossRef] [Green Version]
- Antoch, G.; Stattaus, J.; Nemat, A.T.; Marnitz, S.; Beyer, T.; Kuehl, H.; Bockisch, A.; Debatin, J.F.; Freudenberg, L.S. Non-small cell lung cancer: Dual-modality PET/CT in preoperative staging. Radiology 2003, 229, 526–533. [Google Scholar] [CrossRef]
- Flier, J.S.; Mueckler, M.M.; Usher, P.; Lodish, H.F. Elevated levels of glucose transport and transporter messenger RNA are induced by ras or src oncogenes. Science 1987, 235, 1492–1495. [Google Scholar] [CrossRef]
- Vansteenkiste, J.; Fischer, B.M.; Dooms, C.; Mortensen, J. Positron-emission tomography in prognostic and therapeutic assessment of lung cancer: Systematic review. Lancet Oncol. 2004, 5, 531–540. [Google Scholar] [CrossRef]
- Zander, T.; Scheffler, M.; Nogova, L.; Kobe, C.; Engel-Riedel, W.; Hellmich, M.; Papachristou, I.; Toepelt, K.; Draube, A.; Heukamp, L.; et al. Early prediction of nonprogression in advanced non-small-cell lung cancer treated with erlotinib by using [18F]fluorodeoxyglucose and [18F]fluorothymidine positron emission tomography. J. Clin. Oncol. 2011, 29, 1701–1708. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, R.; Hirata, H.; Tachibana, I.; Shimosegawa, E.; Inoue, A.; Nagatomo, I.; Takeda, Y.; Kida, H.; Goya, S.; Kijima, T.; et al. Early [18F]fluorodeoxyglucose positron emission tomography at two days of gefitinib treatment predicts clinical outcome in patients with adenocarcinoma of the lung. Clin. Cancer Res. 2012, 18, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Ho, K.C.; Fang, Y.D.; Chung, H.W.; Liu, Y.C.; Chang, J.W.; Hou, M.M.; Yang, C.T.; Cheng, N.M.; Su, T.P.; Yen, T.C. TLG-S criteria are superior to both EORTC and PERCIST for predicting outcomes in patients with metastatic lung adenocarcinoma treated with erlotinib. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 2155–2165. [Google Scholar] [CrossRef] [PubMed]
- Fledelius, J.; Winther-Larsen, A.; Khalil, A.A.; Bylov, C.M.; Hjorthaug, K.; Bertelsen, A.; Frøkiær, J.; Meldgaard, P. 18F-FDG PET/CT for very early response evaluation predicts CT response in erlotinib-treated non-small cell lung cancer patients: A comparison of assessment methods. J. Nucl. Med. 2017, 58, 1931–1937. [Google Scholar] [CrossRef]
- van Gool, M.H.; Aukema, T.S.; Hartemink, K.J.; Valdés Olmos, R.A.; van Tinteren, H.; Klomp, H.M. FDG-PET/CT response evaluation during EGFR-TKI treatment in patients with NSCLC. World J. Radiol. 2014, 6, 392–398. [Google Scholar] [CrossRef]
- van Gool, M.H.; Aukema, T.S.; Schaake, E.E.; Rijna, H.; Valdés Olmos, R.A.; van Pel, R.; Burgers, S.A.; van Tinteren, H.; Klomp, H.M. Timing of metabolic response monitoring during erlotinib treatment in non-small cell lung cancer. J. Nucl. Med. 2014, 55, 1081–1086. [Google Scholar] [CrossRef] [Green Version]
- Kahraman, D.; Holstein, A.; Scheffler, M.; Zander, T.; Nogova, L.; Lammertsma, A.A.; Boellaard, R.; Neumaier, B.; Dietlein, M.; Wolf, J.; et al. Tumor lesion glycolysis and tumor lesion proliferation for response prediction and prognostic differentiation in patients with advanced non-small cell lung cancer treated with erlotinib. Clin. Nucl. Med. 2012, 37, 1058–1064. [Google Scholar] [CrossRef]
- Cook, G.J.; O’Brien, M.E.; Siddique, M.; Chicklore, S.; Loi, H.Y.; Sharma, B.; Punwani, R.; Bassett, P.; Goh, V.; Chua, S. Non-small cell lung cancer treated with erlotinib: Heterogeneity of 18F-FDG uptake at PET-association with treatment response and prognosis. Radiology 2015, 276, 883–893. [Google Scholar] [CrossRef]
- Edge, S.B.; Bryd, D.R.; Comton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. AJCC Cancer Staging Handbook, 7th ed.; Springer: New York, NY, USA, 2010; pp. 253–270. [Google Scholar]
- Hung, M.S.; Lung, J.H.; Lin, Y.C.; Fang, Y.H.; Hsieh, M.J.; Tsai, Y.H. The content of mutant EGFR DNA correlates with response to EGFR-TKIs in lung adenocarcinoma patients with common EGFR mutations. Medicine 2016, 95, e3991. [Google Scholar] [CrossRef]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50, 122s–150s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Stroobants, S.; Goeminne, J.; Seegers, M.; Dimitrijevic, S.; Dupont, P.; Nuyts, J.; Martens, M.; van den Borne, B.; Cole, P.; Sciot, R.; et al. 18FDG-Positron emission tomography for the early prediction of response in advanced soft tissue sarcoma treated with imatinib mesylate (Glivec). Eur. J. Cancer 2003, 39, 2012–2020. [Google Scholar] [CrossRef]
- Su, H.; Bodenstein, C.; Dumont, R.A.; Seimbille, Y.; Seimbille, Y.; Dubinett, S.; Phelps, M.E.; Herschman, H.; Czernin, J.; Weber, W. Monitoring tumor glucose utilization by positron emission tomography for the prediction of treatment response to epidermal growth factor receptor kinase inhibitors. Clin. Cancer Res. 2006, 12, 5659–5667. [Google Scholar] [CrossRef] [Green Version]
- Benz, M.R.; Herrmann, K.; Walter, F.; Garon, E.B.; Reckamp, K.L.; Figlin, R.; Phelps, M.E.; Weber, W.A.; Czernin, J.; Allen-Auerbach, M.S. 18F-FDG PET/CT for monitoring treatment responses to the epidermal growth factor receptor inhibitor erlotinib. J. Nucl. Med. 2011, 52, 1684–1689. [Google Scholar] [CrossRef] [Green Version]
- Mileshkin, L.; Hicks, R.J.; Hughes, B.G.; Mitchell, P.L.; Charu, V.; Gitlitz, B.J.; Macfarlane, D.; Solomon, B.; Amler, L.C.; Yu, W.; et al. Changes in 18F-fluorodeoxyglucose and 18F-fluorodeoxythymidine positron emission tomography imaging in patients with non-small cell lung cancer treated with erlotinib. Clin. Cancer Res. 2011, 17, 3304–3315. [Google Scholar] [CrossRef] [Green Version]
- Chung, H.H.; Kwon, H.W.; Kang, K.W.; Park, N.H.; Song, Y.S.; Chung, J.K.; Kang, S.B.; Kim, J.W. Prognostic value of preoperative metabolic tumor volume and total lesion glycolysis in patients with epithelial ovarian cancer. Ann. Surg. Oncol. 2012, 19, 1966–1972. [Google Scholar] [CrossRef]
- Hyun, S.H.; Choi, J.Y.; Kim, K.; Kim, J.; Shim, Y.M.; Um, S.W.; Kim, H.; Lee, K.H.; Kim, B.T. Volume-based parameters of 18F-fluorodeoxyglucose positron emission tomography/computed tomography improve outcome prediction in early-stage non-small cell lung cancer after surgical resection. Ann. Surg. 2013, 257, 364–370. [Google Scholar] [CrossRef]
- Hyun, S.H.; Ahn, H.K.; Kim, H.; Ahn, M.J.; Park, K.; Ahn, Y.C.; Kim, J.; Shim, Y.M.; Choi, J.Y. Volume-based assessment by 18F-FDG PET/CT predicts survival in patients with stage III non-small-cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 50–58. [Google Scholar] [CrossRef]
- Makino, T.; Yamasaki, M.; Tanaka, K.; Masuike, Y.; Tatsumi, M.; Motoori, M.; Kimura, Y.; Hatazawa, J.; Mori, M.; Doki, Y. Metabolic tumor volume change predicts long-term survival and histological response to preoperative chemotherapy in locally advanced esophageal cancer. Ann. Surg. 2019, 270, 1090–1095. [Google Scholar] [CrossRef]
- Cottereau, A.S.; Becker, S.; Broussais, F.; Casasnovas, O.; Kanoun, S.; Roques, M.; Charrier, N.; Bertrand, S.; Delarue, R.; Bonnet, C.; et al. Prognostic value of baseline total metabolic tumor volume (TMTV0) measured on FDG-PET/CT in patients with peripheral T-cell lymphoma (PTCL). Ann. Oncol. 2016, 27, 719–724. [Google Scholar] [CrossRef]
- Hong, I.K.; Lee, L.M.; Hwang, I.K.; Paik, S.S.; Kim, C.; Lee, S.H. Diagnostic and predictive values of 18F-FDG PET/CT metabolic parameters in EGFR-mutated advanced lung adenocarcinoma. Cancer Manag. Res. 2020, 12, 6453–6465. [Google Scholar] [CrossRef] [PubMed]
- Jamal-Hanjani, M.; Quezada, S.A.; Larkin, J.; Swanton, C. Translational implications of tumor heterogeneity. Clin. Cancer Res. 2015, 21, 1258–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Zhang, M.; Tang, W.; Ma, J.; Wei, B.; Niu, Y.; Zhang, G.; Li, P.; Yan, X.; Ma, Z. Mutation abundance affects the therapeutic efficacy of EGFR-TKI in patients with advanced lung adenocarcinoma: A retrospective analysis. Cancer Biol. Ther. 2018, 19, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Leonetti, A.; Bola, S.; Minari, R.; Scarlattei, M.; Buti, S.; Bordi, P.; Baldari, G.; Gnetti, L.; Sammartano, A.; Migliari, S.; et al. Liquid biopsy and PET parameters as predictive factors of osimertinib treatment in advanced EGFR-mutated NSCLC. J. Thorac. Oncol. 2021, 16, S610. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (%) |
|---|---|
| Number of patients | 30 (100) |
| Age (y) | |
| Median | 71 |
| Range | 40–91 |
| Sex | |
| Female | 18 (60) |
| Male | 12 (40) |
| Smoking | |
| Never | 22 (73) |
| Ever | 8 (27) |
| ECOG performance status | |
| 0 | 1 (3) |
| 1 | 29 (97) |
| AJCC clinical stage | |
| IIIB | 1 (3) |
| IV | 29 (97) |
| EGFR mutation type | |
| Classical | 25 (83) |
| Exon 21 L858R | 13 (43) |
| Exon 19 deletion | 11 (37) |
| Both | 1 (3) |
| Others | 5 (17) |
| CEA (ng/mL) | |
| Median | 6.92 |
| Range | 0.5–1034 |
| CT response at 3 months (RECIST) | |
| PR | 23 (77) |
| SD | 1 (3) |
| PD | 6 (20) |
| PET response at 2 weeks (PERCIST) | |
| PMR | 21 (70) |
| SMD | 9 (30) |
| Parameter | Nonprogression (n = 24) | Progression (n = 6) | p Value | Odds Ratio (95% CI) |
|---|---|---|---|---|
| dCt | 3.65 | 5.22 | 0.180 | 0.66 (0.41–1.07) |
| (8.54–1.07) | (8.89–2.63) | |||
| MR (PERCIST) | 83 | 17 | 0.009 * | 25.0 (2.27–276) |
| ΔsumSUL (%) | −46.2 | −20.7 | 0.516 | 0.003 (0–0.41) |
| (−72.5 to 24.4) | (−49.7 to −3.24) | |||
| ΔsumMTV (%) | −77.0 | −35.8 | 0.191 | 0.03 (0.001–0.74) |
| (−99.8 to 5.35) | (−65.4 to 82.5) | |||
| ΔsumTLG (%) | −80.8 | −39.6 | 0.272 | 0.28 (0.001–0.79) |
| (−99.8 to 2.47) | (−72.3 to 76.7) | |||
| bsumMTV (cm3) | 63.00 | 80.60 | 0.080 | 0.99 (0.98–1.00) |
| (1.090–287.2) | (8.410–287.3) | |||
| bsumTLG (g) | 247.9 | 307.8 | 0.085 | 1.00 (0.99–1.00) |
| (2.950–1124) | (24.47–1124) |
| Parameter | Median PFS (Months) (95% CI) | p Value | Hazard Ratio (95% CI) |
|---|---|---|---|
| dCt | 0.014 * | 4.85 (1.38–17.1) | |
| ≥6 | 2.43 (0.01–4.86) | ||
| <6 | 14.3 (9.22–19.4) | ||
| PERCIST | 0.882 | 0.91 (0.26–3.19) | |
| nMR | 3.50 (0–10.2) | ||
| MR | 12.1 (2.46–7.31) | ||
| ΔsumSUL | 0.134 | 2.73 (0.77–10.2) | |
| ≥−40% | 3.50 (0–12.0) | ||
| <−40% | 15.4 (7.74–23.1) | ||
| ΔsumTLG | 0.107 | 3.36 (0.77–14.7) | |
| ≥−50% | 3.50 (0.76–6.24) | ||
| <−50% | 12.1 (8.98–15.3) | ||
| bsumMTV | 0.014 * | 5.60 (1.43–22.0) | |
| ≥40 cm3 | 8.97 (1.58–16.4) | ||
| <40 cm3 | 19.5 (9.07–30.0) | ||
| bsumTLG | 0.222 | 2.02 (0.65–6.24) | |
| ≥ 300 g | 7.59 (4.14–11.0) | ||
| < 300 g | 14.8 (11.5–18.1) |
| Parameter | Median OS (Months) (95% CI) | p Value | Hazard Ratio (95% CI) |
|---|---|---|---|
| dCt | 0.014 * | 9.84 (1.58–61.2) | |
| ≥6 | 12.8 (0–28.1) | ||
| <6 | 25.3 (20.9–29.8) | ||
| PERCIST | 0.636 | 0.64 (0.30–7.03) | |
| nMR | 20.1 (8.23–32.0) | ||
| MR | 25.3 (22.5–28.2) | ||
| ΔsumSUL | 0.106 | 0.14 (0.01–1.53) | |
| ≥−40% | 22.5 (15.1–29.9) | ||
| <−40% | 30.9 (30.9–30.9) | ||
| ΔsumMTV | 0.005 * | 13.1 (2.15–79.4) | |
| ≥−60% | 20.1 (10.3–29.9) | ||
| <−60% | 30.9 (22.4–39.4) | ||
| ΔsumTLG | 0.871 | 1.23 (0.10–14.8) | |
| ≥−50% | 22.5 (11.5–33.4) | ||
| <−50% | 30.9 (22.4–39.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-E.; Tsai, Y.-H.; Huang, Y.-J.; Lung, J.-H.; Ho, K.-W.; Yen, T.-C.; Chan, S.-C.; Chen, S.-T.; Tsai, M.-F.; Hung, M.-S. 18F-Fluorodeoxyglucose PET/CT for Early Prediction of Outcomes in Patients with Advanced Lung Adenocarcinomas and EGFR Mutations Treated with First-Line EGFR-TKIs. Cancers 2022, 14, 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061507
Huang Y-E, Tsai Y-H, Huang Y-J, Lung J-H, Ho K-W, Yen T-C, Chan S-C, Chen S-T, Tsai M-F, Hung M-S. 18F-Fluorodeoxyglucose PET/CT for Early Prediction of Outcomes in Patients with Advanced Lung Adenocarcinomas and EGFR Mutations Treated with First-Line EGFR-TKIs. Cancers. 2022; 14(6):1507. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061507
Chicago/Turabian StyleHuang, Yu-Erh, Ying-Huang Tsai, Yu-Jie Huang, Jr-Hau Lung, Kuo-Wei Ho, Tzu-Chen Yen, Sheng-Chieh Chan, Shu-Tian Chen, Ming-Feng Tsai, and Ming-Szu Hung. 2022. "18F-Fluorodeoxyglucose PET/CT for Early Prediction of Outcomes in Patients with Advanced Lung Adenocarcinomas and EGFR Mutations Treated with First-Line EGFR-TKIs" Cancers 14, no. 6: 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061507