
Is Systemic Immunosuppression a Risk Factor for Oral Cancer? A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. PICOS Question
2.2. Focused Question
2.3. Research
2.4. Manual Search
2.5. Search of Unpublished Articles
2.6. Study Selection
2.7. Extraction Data
2.8. Quality Assessment
2.9. Heterogeneity Assessment
2.10. Data Analysis
3. Results
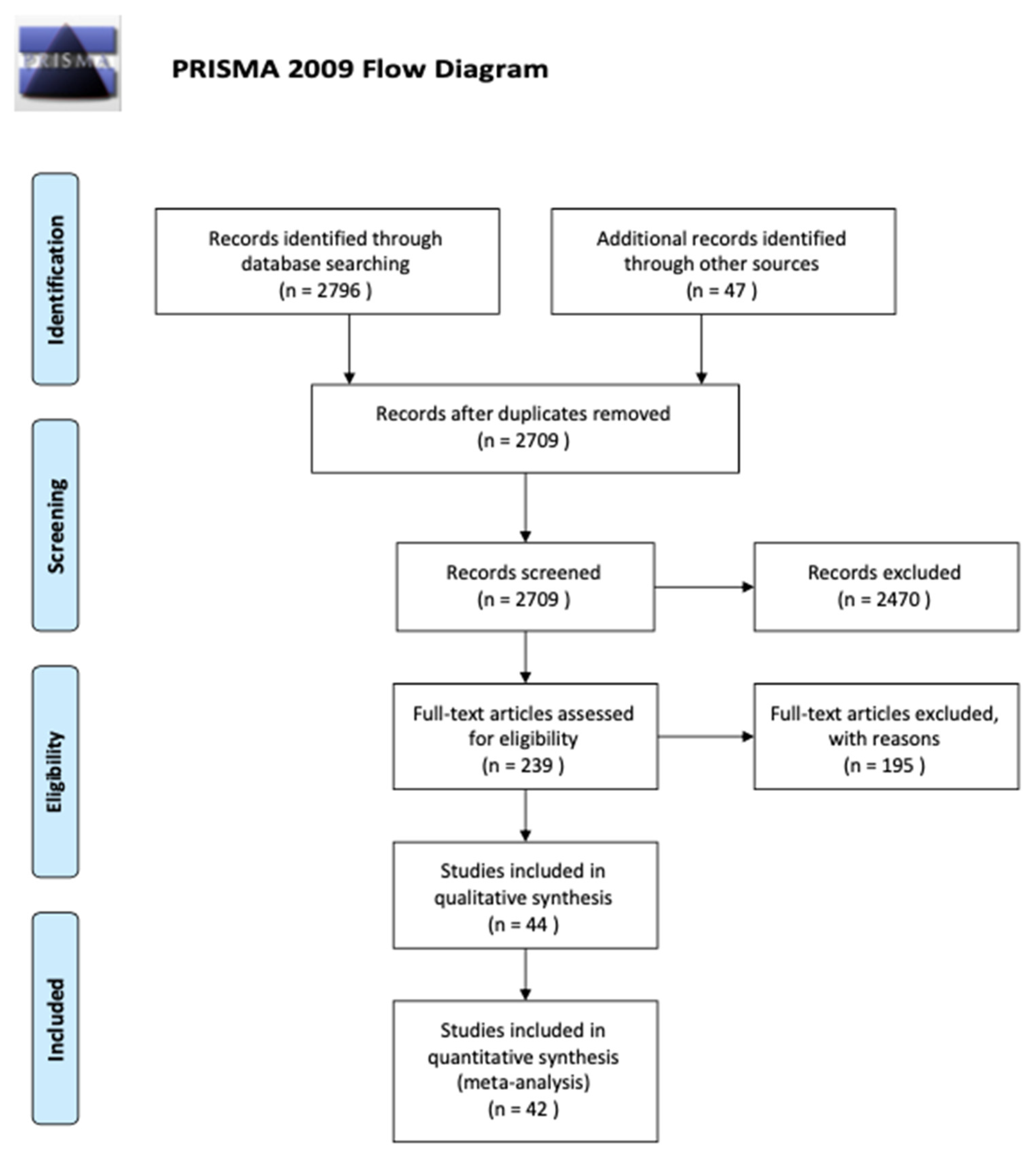
3.1. Study Selection
3.2. Study Characteristics
3.3. Assessment of the Risk of Bias
3.4. Results of the Meta-Analyses
4. Discussion
4.1. Summary of the Main Findings
4.2. Organ Transplantation
4.3. Other Cancers
4.4. Infectious Agents
4.5. Hematopoietic Stem Cell Transplantation (HSC)
4.6. Strengths and Limitations of the Present Systematic Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rivera, C. Essentials of oral cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884–11894. [Google Scholar] [PubMed]
- Liu, J.; Kaplon, A.; Blackman, E.; Miyamoto, C.; Savior, D.; Ragin, C. The Impact of the Multidisciplinary Tumor Board on Head and Neck Cancer Outcomes. Laryngoscope 2020, 130, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Shanti, R.M.; O’Malley, B.W. Surgical Management of Oral Cancer. Dent. Clin. N. Am. 2018, 86, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Burnet, M. Immunological factors in the process of carcinogenesis. Br. Med. Bull. 1964, 20, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Swann, J.B.; Smyth, M.J. Immune surveillance of tumors. J. Clin. Investig. 2007, 117, 1137–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bird, L. Innate surveillance. Nat. Rev. Immunol. 2016, 16, 132–133. [Google Scholar] [CrossRef] [PubMed]
- Lodish, H. Molecular Biology of the Cell, 5th ed.; Macmillan: New York, NY, USA, 2004. [Google Scholar]
- Chinen, J.; Shearer, W.T. Secondary immunodeficiencies, including HIV infection. J. Allergy Clin. Immunol. 2010, 125, S195–S203. [Google Scholar] [CrossRef] [PubMed]
- Notarangelo, L.D.; Bacchetta, R.; Casanova, J.L.; Su, H.C. Human inborn errors of immunity: An expanding universe. Sci. Immunol. 2020, 5, eabb1662. [Google Scholar] [CrossRef] [PubMed]
- Rice, J.M. Immunosuppression. In Tumour Site Concordance and Mechanisms of Carcinogenesis; IARC Scientific Publications (No. 165); Baan, R.A., Stewart, B.W., Straif, K., Eds.; International Agency for Research on Cancer: Lyon, France, 2019; Chapter 16. [Google Scholar]
- Geisser, E.K. Immunosuppression. Cancer Treat. Res. 2009, 146, 23–43. [Google Scholar]
- Kumar, M. Oral cancer: Etiology and risk factors: A review. J. Cancer Res. Ther. 2016, 12, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Vial, T.; Descotes, J. Immunosuppressive drugs and cancer. Toxicology 2003, 185, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised studies in Meta-Analyses. Eur. J. Epidemiol. 2014, 25, 603–605. [Google Scholar]
- Guyatt, G.H. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T. Measuring in consistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, B.C. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Spolidorio, L.C. Oral health in renal transplant recipients administered cyclosporin A or tacrolimus. Oral Dis. 2006, 12, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Villeneuve, P.J.; Wielgosz, A.; Schaubel, D.E.; Fenton, S.S.; Mao, Y. The incidence of cancer in a population-based cohort of Canadian heart transplant recipients. Am. J. Transpl. 2010, 10, 637–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derk, C.T.; Rasheed, M.; Spiegel, J.R.; Jimenez, S.A. Increased incidence of carcinoma of the tongue in patients with systemic sclerosis. J. Rheumatol. 2005, 32, 637–641. [Google Scholar]
- Da Silva, L.C.; de Almeida Freitas, R.; de Andrade, M.P., Jr.; Piva, M.R.; Martins-Filho, P.R.; de Santana Santos, T. Oral lesions in renal transplant. J. Craniofac. Surg. 2012, 23, e214–e218. [Google Scholar] [CrossRef] [PubMed]
- Öhman, J.; Rexius, H.; Mjörnstedt, L.; Gonzalez, H.; Holmberg, E.; Dellgren, G.; Hasséus, B. Oral and lip cancer in solid organ transplant patients—A cohort study from a Swedish Transplant Centre. Oral. Oncol. 2015, 51, 146–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narayan, G. Carcinoma of the Tongue in Renal Transplant Recipients: An Unusual Spectrum of De Novo Malignancy at a Tertiary Care Center in India over a Period of 26 Years. Indian J. Nephrol. 2018, 28, 119–126. [Google Scholar] [PubMed]
- Jäämaa-Holmberg, S.; Salmela, B.; Lemström, K.; Pukkala, E.; Lommi, J. Cancer incidence and mortality after heart transplantation—A population-based national cohort study. Acta. Oncol. 2019, 58, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Laprise, C.; Cahoon, E.K.; Lynch, C.F.; Kahn, A.R.; Copeland, G.; Gonsalves, L.; Madeleine, M.M.; Pfeiffer, R.M.; Engels, E.A. Risk of lip cancer after solid organ transplantation in the United States. Am. J. Transpl. 2019, 19, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, N.C.; Chen, Y.L.; Tsai, K.Y. Head and neck cancer in living donor liver transplant recipients: Single center retrospective study. Medicine 2019, 98, PMC6709202. [Google Scholar] [CrossRef]
- Johns, M.E.; Shikhani, A.H.; Kashima, H.K.; Matanoski, G.M. Multiple primary neoplasms in patients with salivary gland or thyroid gland tumors. Laryngoscope 1986, 96, 718–721. [Google Scholar] [CrossRef]
- Gutman, M. Are malignant melanoma patients at higher risk for a second cancer? Cancer 1991, 68, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Lishner, M. Second malignant neoplasms in patients with non Hodgkin’s lymphoma. Hematol. Oncol. 1991, 9, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Hiyama, T.; Hanai, A.; Fujimoto, I. Second primary cancer after diagnosis of stomach cancer in Osaka, Japan. Jpn. J. Cancer Res. 1991, 82, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Spitz, M.R.; Sider, J.G.; Schantz, S.P.; Newell, G.R. Association between malignancies of the upper aerodigestive tract and uterine cervix. Head Neck 1992, 14, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, C.S.; Biggar, R.J.; Melbye, M.; Curtis, R.E. Second primary cancers following anal and cervical carcinoma: Evidence of shared etiologic factors. Am. J. Epidemiol. 1992, 136, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Levi, F.; Randimbison, L.; La Vecchia, C.; Erler, G.; Te, V.C. Incidence of invasive cancers following squamous cell skin cancer. Am. J. Epidemiol. 1997, 146, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Levi, F.; Randimbison, L.; Te, V.C.; La Vecchia, C. Second primary cancers in patients with lung carcinoma. Cancer 1999, 86, 186–190. [Google Scholar] [CrossRef]
- Levi, F.; Randimbison, L.; Maspoli, M.; Te, V.C.; La Vecchia, C. Second neoplasms after oesophageal cancer. Int. J. Cancer 2007, 121, 694–697. [Google Scholar] [CrossRef] [PubMed]
- Chuang, S.C.; Hashibe, M.; Scelo, G.; Brewster, D.H.; Pukkala, E.; Friis, S.; Tracey, E.; Weiderpass, E.; Hemminki, K.; Tamaro, S.; et al. Risk of second primary cancer among esophageal cancer patients: A pooled analysis of 13 cancer registries. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1543–1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, A.P.; Neeley, E.S.; Werner, T.; Soisson, A.P.; Burt, R.W.; Gaffney, D.K. A population-based study of subsequent primary malignancies after endometrial cancer: Genetic, environmental, and treatment-related associations. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.; Chen, Y.; Zhu, Z.; Lu, L.; Bi, X.; Deng, Q.; Chen, X.; Su, H.; Liu, Y.; Guo, H.; et al. Risk of second primary cancer after treatment for esophageal cancer: A pooled analysis of nine cancer registries. Dis. Esophagus 2012, 25, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.H.; Huang, C.L.; Hsu, Y.H.; Iqbal, U.; Nguyen, P.A.; Jian, W.S. Co-occurrence of second primary malignancy in patients with thyroid cancer. QJM 2014, 107, 643–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robsahm, T.E.; Karagas, M.R.; Rees, J.R.; Syse, A. New malignancies after squamous cell carcinoma and melanomas: A population-based study from Norway. BMC Cancer 2014, 19, 210. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.J.; Beebe-Dimmer, J.L.; Yee, C.L.; Cooney, K.A. Risk of second primary tumors in men diagnosed with prostate cancer: A population-based cohort study. Cancer 2014, 120, 2735–2741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, S.H. Other primary systemic cancers in patients with melanoma: Analysis of balanced acral and nonacral melanomas. J. Am. Acad. Dermatol. 2016, 72, 333–340. [Google Scholar] [CrossRef]
- Krilaviciute, A.; Vincerzevskiene, I.; Smailyte, G. Basal cell skin cancer and the risk of second primary cancers: A cancer registry-based study in Lithuania. Ann. Epidemiol. 2016, 26, 511–514. [Google Scholar] [CrossRef]
- Schlieve, T.; Heidel, R.E.; Carlson, E.R. Second Primary Head and Neck Cancers after Non-Head and Neck Primary Cancers. J. Oral. Maxillofac. Surg. 2016, 74, 2515–2520. [Google Scholar] [CrossRef] [PubMed]
- Adjei Boakye, E.; Wang, M.; Sharma, A.; Jenkins, W.D.; Osazuwa-Peters, N.; Chen, B.; Lee, M.; Schootman, M. Risk of second primary cancers in individuals diagnosed with index smoking- and non-smoking- related cancers. J. Cancer Res. Clin. Oncol. 2020, 146, 1765–1779. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhang, X.; Tao, L.; Chen, P. Risk of second primary malignancy in adults with pulmonary high-grade neuroendocrine carcinoma (HGNEC). BMC Cancer 2020, 20, 719. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Lv, J.; Liu, Y.; Chen, J.G.; Ge, Z.; Zhu, J.; Dai, J.; Du, L.B.; Yu, C.; Guo, Y.; et al. Virus Infection and Risk of All Cancer Types. JAMA Netw. Open. 2019, 2, 6. [Google Scholar] [CrossRef]
- Su, T.H.; Tseng, T.C.; Liu, C.J.; Chou, S.W.; Liu, C.H.; Yang, H.C.; Chen, P.J.; Chen, D.S.; Chen, C.L.; Kao, J.H. Antiviral therapy against chronic hepatitis C is associated with a reduced risk of oral cancer. Int. J. Cancer 2020, 147, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Mahale, P.; Ugoji, C.; Engels, E.A.; Shiels, M.S.; Peprah, S.; Morton, L.M. Cancer risk following lymphoid malignancies among HIV-infected people. AIDS 2020, 34, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Yokota, A.; Ozawa, S.; Masanori, T.; Akiyama, H.; Ohshima, K.; Kanda, Y.; Takahashi, S.; Mori, T.; Nakaseko, C.; Onoda, M.; et al. Secondary solid tumors after allogeneic hematopoietic SCT in Japan. Bone Marrow Transpl. 2012, 47, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, R.E.; Metayer, C.; Rizzo, J.D.; Socié, G.; Sobocinski, K.A.; Flowers, M.E.; Travis, W.D.; Travis, L.B.; Horowitz, M.M.; Deeg, H.J. Impact of chronic GVHD therapy on the development of squamous-cell cancers after hematopoietic stem-cell transplantation: An international case-control study. Blood 2005, 105, 3802–3811. [Google Scholar] [CrossRef] [PubMed]
- Majhail, N.S.; Brazauskas, R.; Rizzo, J.D.; Sobecks, R.M.; Wang, Z.; Horowitz, M.M.; Bolwell, B.; Wingard, J.R.; Socie, G. Secondary solid cancers after allogeneic hematopoietic cell transplantation using busulfan-cyclophosphamide conditioning. Blood 2011, 117, 316–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyer, G.; Brice, L.; Schifter, M.; Gilroy, N.; Kabir, M.; Hertzberg, M.; Greenwood, M.; Larsen, S.R.; Moore, J.; Gottlieb, D.; et al. Oral health and dental morbidity in long-term allogeneic blood and marrow transplant survivors in Australia. Aust. Dent. J. 2018, 63, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Anak, S.; Yalman, N.; Bilgen, H.; Sepet, E.; Deviren, A.; Gürtekin, B.; Tunca, F.; Başaran, B. Squamous cell carcinoma development in Fanconi anemia patients who underwent hematopoietic stem cell transplantation. Pediatr. Transpl. 2020, 24, e13706. [Google Scholar] [CrossRef]
- Santarone, S.; Natale, A.; Angelini, S.; Papalinetti, G.; Vaddinelli, D.; Di Bartolomeo, A.; Di Bartolomeo, P. Secondary oral cancer following hematopoietic cell transplantation. Bone Marrow Transpl. 2021, 56, 1038–1046. [Google Scholar] [CrossRef] [PubMed]
- Bensing, S.; Brandt, L.; Tabaroj, F.; Sjöberg, O.; Nilsson, B.; Ekbom, A.; Blomqvist, P.; Kämpe, O. Increased death risk and altered cancer incidence pattern in patients with isolated or combined autoimmune primary adrenocortical insufficiency. Clin. Endocrinol. 2008, 69, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Feng, S.; Yan, S.; Zhao, Y.; Li, M.; Sun, J.; Zhang, F.C.; Cui, Q.; Dong, Y. Incidence of malignancy in primary Sjogren’s syndrome in a Chinese cohort. Rheumatology 2010, 49, 571–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsanos, K.H.; Roda, G.; McBride, R.B.; Cohen, B.; Colombel, J.F. Increased Risk of Oral Cancer in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2016, 14, 413–420. [Google Scholar] [CrossRef]
- Rautemaa, R.; Hietanen, J.; Niissalo, S.; Pirinen, S.; Perheentupa, J. Oral and oesophageal squamous cell carcinoma—A complication or component of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED, APS-I). Oral Oncol. 2007, 43, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Atsuta, Y.; Suzuki, R.; Yamashita, T.; Fukuda, T.; Miyamura, K.; Taniguchi, S.; Iida, H.; Uchida, T.; Ikegame, K.; Takahashi, S.; et al. Continuing increased risk of oral/esophageal cancer after allogeneic hematopoietic stem cell transplantation in adults in association with chronic graft-versus-host disease. Ann. Oncol. 2014, 25, 435–441. [Google Scholar] [CrossRef] [PubMed]
- López-Pintor, R.M.; Hernández, G.; de Arriba, L.; de Andrés, A. Lip cancer in renal transplant patients. Oral Oncol. 2011, 47, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Motlokwa, P.K.; Tsima, B.M.; Martei, Y.M.; Ralefala, T.; Galebole, F.; Stephens-Shields, A.J.; Grover, S.; Gross, R. Disparities in Oral Cancer Stage at Presentation in a High HIV Prevalence Setting in Sub-Saharan Africa. JCO Glob. Oncol. 2022, 8, e2100439. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, T.L. Immunobiology and immunotherapy of head and neck cancer. Curr Oncol Rep. 2001, 3, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Wen, B.W.; Tsai, C.S.; Lin, C.L.; Chang, Y.J.; Lee, C.F.; Hsu, C.H.; Kao, C.H. Cancer risk among gingivitis and periodontitis patients: A nationwide cohort study. QJM 2014, 107, 283–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, B.; Ariyawardana, A.; Johnson, N.W. Oral cancer in India continues in epidemic proportions: Evidence base and policy initiatives. Int. Dent. J. 2013, 63, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Dickenson, A.J.; Currie, W.J.; Avery, B.S. Screening for syphilis in patients with carcinoma of the tongue. Br. J. Oral Maxillofac. Surg. 1995, 33, 319–320. [Google Scholar] [CrossRef]
- Mohd Bakri, M.; Mohd Hussaini, H.; Rachel Holmes, A.; David Cannon, R.; Mary Rich, A. Revisiting the association between candidal infection and carcinoma, particularly oral squamous cell carcinoma. J. Oral Microbiol. 2010, 21, 2. [Google Scholar] [CrossRef]
- Garrote, L.F.; Herrero, R.; Reyes, R.M.; Vaccarella, S.; Anta, J.L.; Ferbeye, L.; Muñoz, N.; Franceschi, S. Risk factors for cancer of the oral cavity and oro-pharynx in Cuba. Br. J. Cancer 2001, 85, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Hassona, Y.; Scully, C.; Almangush, A.; Baqain, Z.; Sawair, F. Oral potentially malignant disorders among dental patients: A pilot study in Jordan. Asian Pac. J. Cancer Prev. 2014, 15, 10427–10431. [Google Scholar] [CrossRef] [Green Version]
- Ben-David, Y.; Leiser, Y.; Kachta, O.; El-Naaj, I.A. Does long-term treatment with Doxil® predispose patients to oral cancer? Int. J. Clin. Oncol. 2013, 18, 554–555. [Google Scholar] [CrossRef]
- Fahmy, M.S.; Sadeghi, A.; Behmard, S. Epidemiologic study of oral cancer in Fars Province, Iran. Community Dent. Oral Epidemiol. 1983, 11, 50–58. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Nair, M.K.; Mathew, B.; Balaram, P.; Sebastian, P.; Dutt, S.C. Recent results of oral cancer research in Kerala, India. Head Neck. 1992, 14, 107–112. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Kovacevic, T.; Madden, P.; Coupland, V.H.; Sperandio, M.; Odell, E.; Møller, H. Factors predicting malignant transformation in oral potentially malignant disorders among patients accrued over a 10-year period in South East England. J. Oral Pathol. Med. 2011, 40, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Túri, K.; Barabás, P.; Csurgay, K.; Léhner, G.Y.; Lőrincz, A.; Németh, Z.S. An analysis of the epidemiological and etiological factors of oral tumors of young adults in a Central-Eastern European population. Pathol. Oncol. Res. 2013, 19, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Gorsky, M.; Epstein, J.B.; Oakley, C.; Le, N.D.; Hay, J.; Stevenson-Moore, P. Carcinoma of the tongue: A case series analysis of clinical presentation, risk factors, staging, and outcome. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 98, 546–552. [Google Scholar] [CrossRef]
- Hsue, S.S.; Wang, W.C.; Chen, C.H.; Lin, C.C.; Chen, Y.K.; Lin, L.M. Malignant transformation in 1458 patients with potentially malignant oral mucosal disorders: A follow-up study based in a Taiwanese hospital. J. Oral Pathol. Med. 2007, 36, 25–29. [Google Scholar] [CrossRef]
- Saira; Ahmed, R.; Malik, S.; Khan, M.F.; Khattak, M.R. Epidemiological and clinical correlates of oral squamous cell carcinoma in patients from north-west Pakistan. J. Pak. Med. Assoc. 2019, 69, 1074–1078. [Google Scholar]
- Yao, J.G.; Gao, L.B.; Liu, Y.G.; Li, J.; Pang, G.F. Genetic variation in interleukin-10 gene and risk of oral cancer. Clin. Chim. Acta 2008, 388, 84–88. [Google Scholar] [CrossRef]
- De Benedittis, M.; Petruzzi, M.; Giardina, C.; Lo Muzio, L.; Favia, G.; Serpico, R. Oral squamous cell carcinoma during long-term treatment with hydroxyurea. Clin. Exp. Dermatol. 2004, 29, 605–607. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.W.; Chang, W.S.; Lin, K.C.; Shih, L.C.; Tsai, M.H.; Hsiao, C.L.; Yang, M.D.; Lin, C.C.; Bau, D.T. Significant association of Interleukin-10 genotypes and oral cancer susceptibility in Taiwan. Anticancer Res. 2014, 34, 3731–3737. [Google Scholar]
- Abhinav, R.P.; Williams, J.; Livingston, P.; Anjana, R.M.; Mohan, V. Burden of diabetes and oral cancer in India. J. Diabetes Complicat. 2020, 34, 107670. [Google Scholar] [CrossRef]
- Satheeshkumar, P.S.; Mohan, M.P. Oral Helicobacter pylori infection and the risk of oral cancer. Oral Oncol. 2013, 49, e20–e21. [Google Scholar] [CrossRef] [PubMed]
- Krüger, M.; Hansen, T.; Kasaj, A.; Moergel, M. The Correlation between Chronic Periodontitis and Oral Cancer. Case Rep. Dent. 2013, 2013, 262410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermsen, M.A.; Xie, Y.; Rooimans, M.A.; Meijer, G.A.; Baak, J.P.; Plukker, J.T.; Arwert, F.; Joenje, H. Cytogenetic characteristics of oral squamous cell carcinomas in Fanconi anemia. Fam. Cancer 2001, 1, 39–43. [Google Scholar] [CrossRef]
- Moura, L.K.B.; Mobin, M.; Matos, F.T.C.; Monte, T.L.; Lago, E.C.; Falcão, C.A.M.; Ferraz, M.Â.A.L.; Santos, T.C.; Tapety, F.I.; Nunes, C.M.C.L.L.; et al. Bibliometric Analysis on the Risks of Oral Cancer for People Living with HIV/AIDS. Iran J. Public Health 2017, 46, 1583–1585. [Google Scholar] [PubMed]
- Singh, P.K.; Ahmad, M.K.; Kumar, V.; Gupta, R.; Kohli, M.; Jain, A.; Mahdi, A.A.; Bogra, J.; Chandra, G. Genetic polymorphism of interleukin-10 (-A592C) among oral cancer with squamous cell carcinoma. Arch. Oral Biol. 2017, 77, 18–22. [Google Scholar] [CrossRef]
- Tarvainen, L.; Suojanen, J.; Kyyronen, P.; Lindqvist, C.; Martinsen, J.I.; Kjaerheim, K.; Lynge, E.; Sparen, P.; Tryggvadottir, L.; Weiderpass, E.; et al. Occupational Risk for Oral Cancer in Nordic Countries. Anticancer Res. 2017, 37, 3221–3228. [Google Scholar] [PubMed]
- Soulier, J. Fanconi anemia. Hematol. Am. Soc. Hematol. Educ. Program. 2011, 2011, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Hu, Z.; Zhong, Z.; Jiang, Y.; Sun, R.; Fei, J.; Xi, Y.; Li, X.; Song, M.; Li, W.; et al. Clinical and prognostic analysis of second primary squamous cell carcinoma of the tongue after radiotherapy for nasopharyngeal carcinoma. Br. J. Oral Maxillofac. Surg. 2014, 52, 715–720. [Google Scholar] [CrossRef]
- Hashibe, M.; Ritz, B.; Le, A.D.; Li, G.; Sankaranarayanan, R.; Zhang, Z.F. Radiotherapy for oral cancer as a risk factor for second primary cancers. Cancer Lett. 2005, 220, 185–195. [Google Scholar] [CrossRef]
- Santos, A.M.; Marcu, L.G.; Wong, C.M.; Bezak, E. Risk estimation of second primary cancers after breast radiotherapy. Acta Oncol. 2016, 55, 1331–1337. [Google Scholar] [CrossRef] [Green Version]
- Rafferty, M.A.; O’Dwyer, T.P. Secondary primary malignancies in head and neck squamous cell carcinoma. J. Laryngol. Otol. 2001, 115, 988–991. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.D.; Lu, C.H.; Chen, P.T.; Chan, C.H.; Lin, J.T.; Huang, C.E.; Chen, C.C.; Chen, M.C. The incidence and risk of developing a second primary esophageal cancer in patients with oral and pharyngeal carcinoma: A population-based study in Taiwan over a 25 year period. BMC Cancer 2009, 9, 373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanmugham, J.R.; Zavras, A.I.; Rosner, B.A.; Giovannucci, E.L. Alcohol-folate interactions in the risk of oral cancer in women: A prospective cohort study. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2516–2524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Araújo, R.L.; Lyko Kde, F.; Funke, V.A.; Torres-Pereira, C.C. Oral cancer after prolonged immunosuppression for multiorgan chronic graft-versus-host disease. Rev. Bras. Hematol. Hemoter. 2014, 36, 65–68. [Google Scholar] [CrossRef] [Green Version]
- Rosenquist, K.; Wennerberg, J.; Schildt, E.B.; Bladström, A.; Göran Hansson, B.; Andersson, G. Oral status, oral infections and some lifestyle factors as risk factors for oral and oropharyngeal squamous cell carcinoma. A population-based case-control study in southern Sweden. Acta Otolaryngol. 2005, 125, 1327–1336. [Google Scholar] [CrossRef]
- Douglas, C.M.; Jethwa, A.R.; Hasan, W.; Liu, A.; Gilbert, R.; Goldstein, D.; De Almedia, J.; Lipton, J.; Irish, J.C. Long-term survival of head and neck squamous cell carcinoma after bone marrow transplant. Head Neck. 2020, 42, 3389–3395. [Google Scholar] [CrossRef]
- Farrar, M.; Sandison, A.; Peston, D.; Gailani, M. Immunocytochemical analysis of AE1/AE3, CK 14, Ki-67 and p53 expression in benign, premalignant and malignant oral tissue to establish putative markers for progression of oral carcinoma. Br. J. Biomed. Sci. 2004, 61, 117–124. [Google Scholar] [CrossRef]
- Hsu, H.J.; Yang, Y.H.; Shieh, T.Y.; Chen, C.H.; Kao, Y.H.; Yang, C.F.; Ko, E.C. TGF-β1 and IL-10 single nucleotide polymorphisms as risk factors for oral cancer in Taiwanese. Kaohsiung J. Med. Sci. 2015, 31, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Danylesko, I.; Shimoni, A. Second Malignancies after Hematopoietic Stem Cell Transplantation. Curr. Treat. Options Oncol. 2018, 19, 9. [Google Scholar] [CrossRef]
- Adhikari, J.; Sharma, P.; Bhatt, V.R. Risk of secondary solid malignancies after allogeneic hematopoietic stem cell transplantation and preventive strategies. Future Oncol. 2015, 11, 3175–3185. [Google Scholar] [CrossRef]
- Demarosi, F.; Lodi, G.; Carrassi, A.; Soligo, D.; Sardella, A. Oral malignancies following HSCT: Graft versus host disease and other risk factors. Oral Oncol. 2005, 41, 865–877. [Google Scholar] [CrossRef] [PubMed]
- Manavoğlu, O.; Orhan, B.; Evrensel, T.; Karabulut, Y.; Ozkocaman, V.; Ozyardimci, C. Second primary cancer due to radiotherapy and chemotherapy. J. Environ. Pathol. Toxicol. Oncol. 1996, 15, 275–278. [Google Scholar]
- Takeuchi, Y.; Onizawa, K.; Wakatsuki, T.; Yamagata, K.; Hasegawa, Y.; Yoshida, H. Tongue cancer after bone marrow transplantation. Oral Oncol. 2006, 42, 251–254. [Google Scholar] [CrossRef] [Green Version]
- Tomihara, K.; Dehari, H.; Yamaguchi, A.; Abe, M.; Miyazaki, A.; Nakamori, K.; Hareyama, M.; Hiratsuka, H. Squamous cell carcinoma of the buccal mucosa in a young adult with history of allogeneic bone marrow transplantation for childhood acute leukemia. Head Neck 2009, 31, 565–568. [Google Scholar] [CrossRef]
- Kawano, K.; Goto, H.; Takahashi, Y.; Kaku, Y.; Oobu, K.; Yanagisawa, S. Secondary Squamous Cell Carcinoma of the Oral Cavity in Young Adults after Hematopoietic Stem Cell Transplantation for Leukemia: Report of Two Cases with Human Papillomavirus Infection. Oral Sci. Int. 2007, 4, 110–116. [Google Scholar] [CrossRef] [Green Version]
- Inamoto, Y.; Shah, N.N.; Savani, B.N.; Shaw, B.E.; Abraham, A.A.; Ahmed, I.A.; Akpek, G.; Atsuta, Y.; Baker, K.S.; Basak, G.W.; et al. Secondary solid cancer screening following hematopoietic cell transplantation. Bone Marrow Transplant. 2015, 50, 1013–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández, G.; Arriba, L.; Jiménez, C.; Bagán, J.V.; Rivera, B.; Lucas, M.; Moreno, E. Rapid progression from oral leukoplakia to carcinoma in an immunosuppressed liver transplant recipient. Oral Oncol. 2003, 39, 87–90. [Google Scholar] [CrossRef]
- Torres-Pereira, C.C.; Stramandinoli-Zanicotti, R.T.; Amenábar, J.M.; Sassi, L.M.; Galbiatti Pedruzzi, P.A.; Piazzetta, C.M.; Bonfim, C. Oral squamous cell carcinoma in two siblings with Fanconi anemia after allogeneic bone marrow transplantation. Spec. Care Dentist 2014, 34, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Alotaiby, F.; Song, F.; Boyce, B.J.; Cao, D.; Zhao, Y.; Lai, J. Unusual Papillary Squamous Cell Carcinoma of the Tip of Tongue Presenting in a Patient Status Post Heart Transplant. Anticancer Res. 2018, 38, 4203–4206. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Schmidt, B.L.; Jordan, R.C. Tongue and tonsil carcinoma: Increasing trends in the U.S. population ages 20–44 years. Cancer 2005, 103, 1843–1849. [Google Scholar] [CrossRef] [PubMed]
- Weng, X.; Xing, Y.; Cheng, B. Multiple and Recurrent Squamous Cell Carcinoma of the Oral Cavity After Graft-Versus-Host Disease. J. Oral Maxillofac. Surg. 2017, 75, 1899–1905. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.N. Oral Carcinoma: A Clinical Study Of 122 Cases. J. Indian Med. Assoc. 1964, 43, 263–268. [Google Scholar] [PubMed]
- Fu, X.; Chen, S.; Chen, W.; Yang, Z.; Song, M.; Li, H.; Zhang, H.; Yao, F.; Su, X.; Liu, T.; et al. Clinical analysis of second primary gingival squamous cell carcinoma after radiotherapy. Oral Oncol. 2018, 84, 20–24. [Google Scholar] [CrossRef]
- García-Martín, J.M.; Varela-Centelles, P.; González, M.; Seoane-Romero, J.M.; Seoane, J.; García-Pola, M.J. Epidemiology of oral cancer. In Oral Cancer Detection; Panta, P., Ed.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Tao, Y.; Sturgis, E.M.; Huang, Z.; Sun, Y.; Dahlstrom, K.R.; Wei, Q.; Li, G. A TGF-β1 genetic variant at the miRNA187 binding site significantly modifies risk of HPV16-associated oropharyngeal cancer. Int. J. Cancer 2018, 143, 1327–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madrid, C.; Scully, C. Oral cancer: Comprehending the condition, causes, controversies, control and consequences. 17. Osteonecrosis. Dent. Update 2012, 39, 377–379. [Google Scholar] [CrossRef]
- Dhanuthai, K.; Rojanawatsirivej, S.; Thosaporn, W.; Kintarak, S.; Subarnbhesaj, A.; Darling, M.; Kryshtalskyj, E.; Chiang, C.P.; Shin, H.I.; Choi, S.Y.; et al. Oral cancer: A multicenter study. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e23–e29. [Google Scholar] [CrossRef]
- Geng, F.; Wang, Q.; Li, C.; Liu, J.; Zhang, D.; Zhang, S.; Pan, Y. Identification of Potential Candidate Genes of Oral Cancer in Response to Chronic Infection With Porphyromonas gingivalis Using Bioinformatical Analyses. Front Oncol. 2019, 9, 91. [Google Scholar] [CrossRef]
- Pisani, L.P.; Estadella, D.; Ribeiro, D.A. The Role of Toll Like Receptors (TLRs) in Oral Carcinogenesis. Anticancer Res. 2017, 37, 5389–5394. [Google Scholar]
- Okubo, M.; Kioi, M.; Nakashima, H.; Sugiura, K.; Mitsudo, K.; Aoki, I.; Taniguchi, H.; Tohnai, I. M2-polarized macrophages contribute to neovasculogenesis, leading to relapse of oral cancer following radiation. Sci Rep. 2016, 6, 27548. [Google Scholar] [CrossRef] [Green Version]
- Dewan, K.; Kelly, R.D.; Bardsley, P. A national survey of consultants, specialists and specialist registrars in restorative dentistry for the assessment and treatment planning of oral cancer patients. Br. Dent. J. 2014, 216, E27. [Google Scholar] [CrossRef] [Green Version]
- Mukhopadhyaya, R.; Rao, R.S.; Fakih, A.R.; Gangal, S.G. Detection of circulating immune complexes in patients with squamous cell carcinoma of the oral cavity. J. Clin. Lab. Immunol. 1986, 21, 189–193. [Google Scholar] [PubMed]
- Adewole, R.A. Alcohol, smoking and oral cancer. A 10-year retrospective study at Base Hospital, Yaba. West Afr. J. Med. 2002, 21, 142–145. [Google Scholar]
- Kashyap, T.; Pramanik, K.K.; Nath, N.; Mishra, P.; Singh, A.K.; Nagini, S.; Rana, A.; Mishra, R. Crosstalk between Raf-MEK-ERK and PI3K-Akt-GSK3β signaling networks promotes chemoresistance, invasion/migration and stemness via expression of CD44 variants (v4 and v6) in oral cancer. Oral Oncol. 2018, 86, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Johnson, N.; Pierce, A.; Wilson, D. The epidemiology of lip cancer: A review of global incidence and aetiology. Oral Dis. 1999, 5, 185–195. [Google Scholar] [CrossRef]
- Ueda, N.; Kamata, N.; Hayashi, E.; Yokoyama, K.; Hoteiya, T.; Nagayama, M. Effects of an anti-angiogenic agent, TNP-470, on the growth of oral squamous cell carcinomas. Oral Oncol. 1999, 35, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, X.; Fang, J. Mesenchymal stem cells participate in oral mucosa carcinogenesis by regulating T cell proliferation. Clin. Immunol. 2019, 198, 46–53. [Google Scholar] [CrossRef]
- Kikuchi, K.; Noguchi, Y.; de Rivera, M.W. Detection of Epstein-Barr virus genome and latent infection gene expression in normal epithelia, epithelial dysplasia, and squamous cell carcinoma of the oral cavity. Tumour Biol. 2016, 37, 3389–3404. [Google Scholar] [CrossRef]
- Lenouvel, D.; González-Moles, M.Á.; Talbaoui, A. An update of knowledge on PD-L1 in head and neck cancers: Physiologic, prognostic and therapeutic perspectives. Oral Dis. 2020, 26, 511–526. [Google Scholar] [CrossRef]
- Brown, A.M.; Lally, E.T.; Frankel, A.; Harwick, R.; Davis, L.W.; Rominger, C.J. The association of the IGA levels of serum and whole saliva with the progression of oral cancer. Cancer 1975, 35, 1154–1162. [Google Scholar] [CrossRef]
- Johnson, N.W. Az oralis carcinomák etiológiája és rizikófaktorai, különös tekintettel a dohányzásra és az alkoholfogyasztásra [Aetiology and risk factors for oral cancer, with special reference to tobacco and alcohol use]. Magy Onkol. 2001, 45, 115–122. [Google Scholar]
- Adams, S.; Lin, J.; Brown, D.; Shriver, C.D.; Zhu, K. Ultraviolet Radiation Exposure and the Incidence of Oral, Pharyngeal and Cervical Cancer and Melanoma: An Analysis of the SEER Data. Anticancer Res. 2016, 36, 233–237. [Google Scholar] [PubMed]
- Kurokawa, H.; Tsuru, S.; Okada, M.; Nakamura, T.; Kajiyama, M. Evaluation of tumor markers in patients with squamous cell carcinoma in the oral cavity. Int. J. Oral Maxillofac. Surg. 1993, 22, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Talamini, R.; Vaccarella, S.; Barbone, F. Oral hygiene, dentition, sexual habits and risk of oral cancer. Br. J. Cancer 2000, 83, 1238–1242. [Google Scholar] [CrossRef]
- La Rosa, G.R.M.; Gattuso, G.; Pedullà, E.; Rapisarda, E.; Nicolosi, D.; Salmeri, M. Association of oral dysbiosis with oral cancer development. Oncol. Lett. 2020, 19, 3045–3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, D.; Ghosh, S.; Maitra, A. Epigenomic dysregulation-mediated alterations of key biological pathways and tumor immune evasion are hallmarks of gingivo-buccal oral cancer. Clin. Epigenetics 2019, 11, 178. [Google Scholar] [CrossRef] [Green Version]
- Rajkumar, T.; Sridhar, H.; Balaram, P. Oral cancer in Southern India: The influence of body size, diet, infections and sexual practices. Eur. J. Cancer Prev. 2003, 12, 135–143. [Google Scholar] [CrossRef]
- Khanna, S. Immunological and biochemical markers in oral carcinogenesis: The public health perspective. Int. J. Environ. Res. Public Health 2008, 5, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Engku Nasrullah Satiman, E.A.F.; Ahmad, H.; Ramzi, A.B.; Wahab, R.A.; Kaderi, M.A.; Harun, W.H.A.W.; Dashper, S. The role of Candida albicans candidalysin ECE1 gene in oral carcinogenesis. J. Oral Pathol. Med. 2020, 49, 835–841. [Google Scholar] [CrossRef]
- Wu, T.S.; Tan, C.T.; Chang, C.C. B-cell lymphoma/leukemia 10 promotes oral cancer progression through STAT1/ATF4/S100P signaling pathway. Oncogene. 2015, 34, 1207–1219. [Google Scholar] [CrossRef]
- Malinowska, K.; Morawiec-Sztandera, A.; Majsterek, I.; Kaczmarczyk, D. TC2 C776G polymorphism studies in patients with oral cancer in the Polish population. Pol. J. Pathol. 2016, 67, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Leuci, S.; Coppola, N.; Blasi, A. Oral Dysplastic Complications after HSCT: Single Case Series of Multidisciplinary Evaluation of 80 Patients. Life 2020, 10, 236. [Google Scholar] [CrossRef] [PubMed]
- Anqi, C.; Takabatake, K.; Kawai, H.; Oo, M.W.; Yoshida, S.; Fujii, M.; Omori, H.; Sukegawa, S.; Nakano, K.; Tsuijigiwa, H.; et al. Differentiation and roles of bone marrow-derived cells on the tumor microenvironment of oral squamous cell carcinoma. Oncol. Lett. 2019, 18, 6628–6638. [Google Scholar] [CrossRef] [PubMed]
- Furquim, C.P.; Pivovar, A.; Amenábar, J.M.; Bonfim, C.; Torres-Pereira, C.C. Oral cancer in Fanconi anemia: Review of 121 cases. Crit. Rev.Oncol. Hematol. 2018, 125, 35–40. [Google Scholar] [CrossRef]
- Shah, A.T.; Wu, E.; Wein, R.O. Oral squamous cell carcinoma in post-transplant patients. Am. J. Otolaryngol. 2013, 34, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Elad, S.; Zadik, Y.; Zeevi, I.; Miyazaki, A.; de Figueiredo, M.A.; Or, R. Oral cancer in patients after hematopoietic stem-cell transplantation: Long-term follow-up suggests an increased risk for recurrence. Transplantation 2010, 90, 1243–1244. [Google Scholar] [CrossRef] [PubMed]
- Abdelsayed, R.A.; Sumner, T.; Allen, C.M.; Treadway, A.; Ness, G.M.; Penza, S.L. Oral precancerous and malignant lesions associated with graft-versus-host disease: Report of 2 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 75–80. [Google Scholar] [CrossRef] [PubMed]
- González-Moles, M.Á.; Ruiz-Ávila, I.; González-Ruiz, L.; Ayén, Á.; Gil-Montoya, J.A.; Ramos-García, P. Malignant transformation risk of oral lichen planus: A systematic review and comprehensive meta-analysis. Oral Oncol. 2019, 96, 121–130. [Google Scholar] [CrossRef]
- Nagao, Y.; Sata, M.; Fukuizumi, K.; Harada, H.; Kameyama, T. Oral cancer and hepatitis C virus (HCV): Can HCV alone cause oral cancer?—A case report. Kurume Med. J. 1996, 43, 97–100. [Google Scholar] [CrossRef] [Green Version]
- Nagao, Y.; Sata, M.; Noguchi, S. Detection of hepatitis C virus RNA in oral lichen planus and oral cancer tissues. J. Oral Pathol. Med. 2000, 29, 259–266. [Google Scholar] [CrossRef]
- Nagao, Y.; Sata, M.; Tanikawa, K.; Itoh, K.; Kameyama, T. High prevalence of hepatitis C virus antibody and RNA in patients with oral cancer. J. Oral Pathol. Med. 1995, 24, 354–360. [Google Scholar] [CrossRef]
- Nagao, Y.; Sata, M. Oral verrucous carcinoma arising from lichen planus and esophageal squamous cell carcinoma in a patient with hepatitis C virus-related liver cirrhosis-hyperinsulinemia and malignant transformation: A case report. Biomed. Rep. 2013, 1, 53–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandolfo, S.; Richiardi, L.; Carrozzo, M. Risk of oral squamous cell carcinoma in 402 patients with oral lichen planus:A follow-up study in an Italian population. Oral Oncol. 2004, 40, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.Y.; You, S.L.; Lu, S.N. Risk of hepatocellular carcinoma and habits of alcohol drinking, betel quid chewing and cigarette smoking: A cohort of 2416 HBsAg-seropositive and 9421 HBsAg-seronegative male residents in Taiwan. Cancer Causes Control 2003, 14, 241–250. [Google Scholar] [CrossRef]
- Kao, C.H.; Sun, L.M.; Liang, J.A.; Chang, S.N.; Sung, F.C.; Muo, C.H. Relationship of zolpidem and cancer risk: A Taiwanese population-based cohort study. Mayo Clin. Proc. 2012, 87, 430–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tandle, A.T.; Sanghvi, V.; Saranath, D. Determination of p53 genotypes in oral cancer patients from India. Br. J. Cancer 2001, 84, 739–742. [Google Scholar] [CrossRef] [Green Version]
- Shih, L.C.; Li, C.H.; Sun, K.T. Association of Matrix Metalloproteinase-7 Genotypes to the Risk of Oral Cancer in Taiwan. Anticancer Res. 2018, 38, 2087–2092. [Google Scholar]
- Chiu, C.F.; Tsai, M.H.; Tseng, H.C.; Wang, C.L.; Tsai, F.J.; Lin, C.C.; Bau, D.T. A novel single nucleotide polymorphism in ERCC6 gene is associated with oral cancer susceptibility in Taiwanese patients. Oral Oncol. 2008, 44, 582–586. [Google Scholar] [CrossRef]
- Park, J.Y.; Schantz, S.P.; Stern, J.C.; Kaur, T.; Lazarus, P. Association between glutathione S-transferase pi genetic polymorphisms and oral cancer risk. Pharmacogenetics 1999, 9, 497–504. [Google Scholar]
- Hatagima, A.; Costa, E.C.; Marques, C.F.; Koifman, R.J.; Boffetta, P.; Koifman, S. Glutathione S-transferase polymorphisms and oral cancer: A case-control study in Rio de Janeiro, Brazil. Oral Oncol. 2008, 44, 200–207. [Google Scholar] [CrossRef]
- Misra, C.; Majumder, M.; Bajaj, S.; Ghosh, S.; Roy, B.; Roychoudhury, S. Polymorphisms at p53, p73, and MDM2 loci modulate the risk of tobacco associated leukoplakia and oral cancer. Mol Carcinog. 2009, 48, 790–800. [Google Scholar] [CrossRef]
- Sartor, M.; Steingrimsdottir, H.; Elamin, F. Role of p16/MTS1, cyclin D1 and RB in primary oral cancer and oral cancer cell lines. Br. J. Cancer 1999, 80, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, C.T.; Chang, T.K.; Hwang, Y.H. A critical exploration of blood and environmental chromium concentration among oral cancer patients in an oral cancer prevalent area of Taiwan. Environ. Geochem. Health 2011, 33, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Chen, M.F.; Lin, P.Y. Significance of DNMT3b in oral cancer. PLoS ONE 2014, 9, e89956. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Gridley, G.; Huang, W.Y. Microsatellite polymorphisms in the epidermal growth factor receptor (EGFR) gene and the transforming growth factor-alpha (TGFA) gene and risk of oral cancer in Puerto Rico. Pharmacogenet. Genom. 2005, 15, 343–347. [Google Scholar] [CrossRef]
- Rao, A.K.D.M.; Manikandan, M.; Arunkumar, G.; Revathidevi, S.; Vinothkumar, V.; Arun, K.; Tiwary, B.K.; Rajkumar, K.S. Prevalence of p53 codon 72, p73 G4C14-A4T14 and MDM2 T309G polymorphisms and its association with the risk of oral cancer in South Indians. Gene Rep. 2017, 7, 106–112. [Google Scholar] [CrossRef]
- Yen, C.Y.; Liu, S.Y.; Chen, C.H.; Tseng, H.F.; Chuang, L.Y.; Yang, C.H.; Lin, Y.C.; Wen, C.H.; Chiang, W.F.; Ho, C.H. Combinational polymorphisms of four DNA repair genes XRCC1, XRCC2, XRCC3, and XRCC4 and their association with oral cancer in Taiwan. J. Oral Pathol. Med. 2008, 37, 271–277. [Google Scholar] [CrossRef]
- Ramachandran, S.; Ramadas, K.; Hariharan, R.; Rejnish Kumar, R.; Radhakrishna Pillai, M. Single nucleotide polymorphisms of DNA repair genes XRCC1 and XPD and its molecular mapping in Indian oral cancer. Oral Oncol. 2006, 42, 350–362. [Google Scholar] [CrossRef]
- Shukla, D.; Dinesh Kale, A.; Hallikerimath, S.; Vivekanandhan, S.; Venkatakanthaiah, Y. Genetic polymorphism of drug metabolizing enzymes (GSTM1 and CYP1A1) as risk factors for oral premalignant lesions and oral cancer. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2012, 156, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Park, J.Y.; Muscat, J.E.; Ren, Q. CYP1A1 and GSTM1 polymorphisms and oral cancer risk. Cancer Epidemiol. Biomark. Prev. 1997, 6, 791–797. [Google Scholar]
- Cha, I.H.; Park, J.Y.; Chung, W.Y.; Choi, M.A.; Kim, H.J.; Park, K.K. Polymorphisms of CYP1A1 and GSTM1 genes and susceptibility to oral cancer. Yonsei Med. J. 2007, 48, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Carneiro, N.K.; Oda, J.M.; Losi Guembarovski, R.; Ramos, G.; Oliveira, B.V.; Cavalli, I.J.; Ribeiro, E.M.d.S.F.; Goncalves, M.S.B.; Watanabe, M.A.E. Possible association between TGF-β1 polymorphism and oral cancer. Int. J. Immunogenet. 2013, 40, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-H.; Ting, S.-C.; Chen, C.-H.; Tsai, C.-C.; Lung, O.; Liu, T.-C.; Lee, C.-W.; Wang, Y.-Y.; Tsai, C.-L.; Lin, Y.-C. Polymorphisms in the apoptosis-associated genes FAS and FASL and risk of oral cancer and malignant potential of oral premalignant lesions in a Taiwanese population. J. Oral Pathol. Med. 2010, 39, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Chung, T.T.; Pan, M.S.; Kuo, C.L. Impact of RECK gene polymorphisms and environmental factors on oral cancer susceptibility and clinicopathologic characteristics in Taiwan. Carcinogenesis 2011, 32, 1063–1068. [Google Scholar] [CrossRef] [Green Version]
- Shukla, D.; Dinesh Kale, A.; Hallikerimath, S.; Yerramalla, V.; Subbiah, V.; Mishra, S. Association between GSTM1 and CYP1A1 polymorphisms and survival in oral cancer patients. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2013, 157, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Gunduz, E.; Gunduz, M.; Ouchida, M. Genetic and epigenetic alterations of BRG1 promote oral cancer development. Int. J. Oncol. 2005, 26, 201–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merrill, R.M.; Isakson, R.T.; Beck, R.E. The association between allergies and cancer: What is currently known? Ann. Allergy Asthma Immunol. 2007, 99, 102–150. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Sturgis, E.M.; Wang, L.E. Association of a p73 exon 2 G4C14-to-A4T14 polymorphism with risk of squamous cell carcinoma of the head and neck. Carcinogenesis 2004, 25, 1911–1916. [Google Scholar] [CrossRef]
- Twu, C.W.; Jiang, R.S.; Shu, C.H.; Lin, J.C. Association of p53 codon 72 polymorphism with risk of hypopharyngeal squamous cell carcinoma in Taiwan. J. Formos. Med. Assoc. 2006, 105, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Katoh, T. The frequency of glutathione-S-transferase M1 (GSTM1) gene deletion in patients with lung and oral cancer. Sangyo Igaku. 1994, 36, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z. The role of COX-2 in oral cancer development, and chemoprevention/ treatment of oral cancer by selective COX-2 inhibitors. Curr. Pharm. Des. 2005, 11, 1771–1777. [Google Scholar] [CrossRef]
- Liu, F.; Liu, L.; Li, B. p73 G4C14-A4T14 polymorphism and cancer risk: A meta-analysis based on 27 case-control studies. Mutagenesis 2011, 26, 573–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.P.; Shah, P.P.; Ruwali, M.; Mathur, N.; Pant, M.C.; Parmar, D. Polymorphism in cytochrome P4501A1 is significantly associated with head and neck cancer risk. Cancer Investig. 2009, 27, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Shillitoe, E.J. The role of viruses in squamous cell carcinoma of the oropharyngeal mucosa. Oral Oncol. 2009, 45, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Beppu, M.; Ikebe, T.; Shirasuna, K. The inhibitory effects of immunosuppressive factors, dexamethasone and interleukin-4, on NF-kappaB-mediated protease production by oral cancer. Biochim. Biophys. Acta 2002, 1586, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Van der Meij, E.H.; Epstein, J.B.; Hay, J.; Ho, V.; Lerner, K. Sweet’s syndrome in a patient with oral cancer associated with radiotherapy. Eur. J. Cancer B Oral Oncol. 1996, 32B, 133–136. [Google Scholar] [CrossRef]
- Uittamo, J.; Siikala, E.; Kaihovaara, P.; Salaspuro, M.; Rautemaa, R. Chronic candidosis and oral cancer in APECED-patients: Production of carcinogenic acetaldehyde from glucose and ethanol by Candida albicans. Int. J. Cancer 2009, 124, 754–756. [Google Scholar] [CrossRef]
- Shillitoe, E.J. The role of immunology in the diagnosis, prognosis and treatment planning of oral cancer. Proc. R. Soc. Med. 1976, 69, 747–749. [Google Scholar]
- Meurman, J.H. Infectious and dietary risk factors of oral cancer. Oral Oncol. 2010, 46, 411–413. [Google Scholar] [CrossRef]
- Sanjaya, P.R.; Gokul, S.; Gururaj Patil, B.; Raju, R. Candida in oral pre-cancer and oral cancer. Med. Hypotheses 2011, 77, 1125–1128. [Google Scholar] [CrossRef]
- Morris, L.G.; Patel, S.G.; Shah, J.P.; Ganly, I. Squamous cell carcinoma of the oral tongue in the pediatric age group: A matched-pair analysis of survival. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 697–701. [Google Scholar] [CrossRef] [Green Version]
- Hara, H.; Ozeki, S.; Nagata, T.; Okamoto, M.; Sasaguri, M.; Tashiro, H.; Jingu, K. Pulmonary tuberculosis in patients with oral cancer. Gan No Rinsho. 1988, 34, 1647–1653. [Google Scholar] [PubMed]
- Laprise, C.; Shahul, H.P.; Madathil, S.A. Periodontal diseases and risk of oral cancer in Southern India: Results from the HeNCe Life study. Int. J. Cancer. 2016, 139, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Arantes, D.A.; Costa, N.L.; Mendonça, E.F.; Silva, T.A.; Batista, A.C. Overexpression of immunosuppressive cytokines is associated with poorer clinical stage of oral squamous cell carcinoma. Arch. Oral Biol. 2016, 61, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Hwang, P.H.; Lian, L.; Zavras, A.I. Alcohol intake and folate antagonism via CYP2E1 and ALDH1: Effects on oral carcinogenesis. Med. Hypotheses 2012, 78, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Mun, M.; Yap, T.; Alnuaimi, A.D.; Adams, G.G.; McCullough, M.J. Oral candidal carriage in asymptomatic patients. Aust. Dent. J. 2016, 61, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Krogh, P.; Hald, B.; Holmstrup, P. Possible mycological etiology of oral mucosal cancer: Catalytic potential of infecting Candida albicans and other yeasts in production of N-nitrosobenzylmethylamine. Carcinogenesis 1987, 8, 1543–1548. [Google Scholar] [CrossRef]
- Yakin, M.; Gavidi, R.O.; Cox, B.; Rich, A. Oral cancer risk factors in New Zealand. N. Z. Med. J. 2017, 130, 30–38. [Google Scholar]
- Sheu, J.J.; Keller, J.J.; Lin, H.C. Increased risk of cancer after Bell’s palsy: A 5-year follow-up study. J. Neurooncol. 2012, 110, 215–220. [Google Scholar] [CrossRef]
- Ma’aita, J.K. Oral cancer in Jordan: A retrospective study of 118 patients. Croat. Med. J. 2000, 41, 64–69. [Google Scholar]
- Mäkinen, A.; Nawaz, A.; Mäkitie, A.; Meurman, J.H. Role of Non-Albicans Candida and Candida Albicans in Oral Squamous Cell Cancer Patients. J. Oral Maxillofac. Surg. 2018, 76, 2564–2571. [Google Scholar] [CrossRef] [Green Version]
- Menicagli, R.; Bolla, G.; Menicagli, L.; Esseridou, A. The Possible Role of Diabetes in the Etiology of Laryngeal Cancer. Gulf. J. Oncolog. 2017, 1, 44–51. [Google Scholar]
- Bhattathiri, N.V.; Bindu, L.; Remani, P.; Chandralekha, B.; Nair, K.M. Radiation-induced acute immediate nuclear abnormalities in oral cancer cells: Serial cytologic evaluation. Acta Cytol. 1998, 42, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- D’Costa, J.; Saranath, D.; Sanghvi, V.; Mehta, A.R. Epstein-Barr virus in tobacco-induced oral cancers and oral lesions in patients from India. J. Oral Pathol. Med. 1998, 27, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Lu, S.; Xing, X.; Wang, L.; Mu, D.; He, M.; Huang, H.; Zeng, X.; Chen, Q. Thalidomide: Features and potential significance in oral precancerous conditions and oral cancer. J. Oral Pathol. Med. 2013, 42, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Gall, F.; Colella, G.; Di Onofrio, V.; Rossiello, R.; Angelillo, I.F.; Liguori, G. Candida spp. in oral cancer and oral precancerous lesions. New Microbiol. 2013, 36, 283–288. [Google Scholar]
- Vijayakumar, T.; Sasidharan, V.K.; Ankathil, R.; Remani, P.; Kumari, T.V.; Vasudevan, D.M. Incidence of hepatitis B surface antigen (HBsAg) in oral cancer and carcinoma of uterine cervix. Indian J. Cancer 1984, 21, 7–10. [Google Scholar]
- Li, M.H.; Ito, D.; Sanada, M.; Odani, T.; Hatori, M.; Iwase, M.; Nagumo, M. Effect of 5-fluorouracil on G1 phase cell cycle regulation in oral cancer cell lines. Oral Oncol. 2004, 40, 63–70. [Google Scholar] [CrossRef]
- Mawardi, H.; Elad, S.; Correa, M.E.; Stevenson, K.; Woo, S.B.; Almazrooa, S.; Haddad, R.; Antin, H.J.; Soiffer, R.; Treister, H. Oral epithelial dysplasia and squamous cell carcinoma following allogeneic hematopoietic stem cell transplantation: Clinical presentation and treatment outcomes. Bone Marrow Transplant. 2011, 46, 884–891. [Google Scholar] [CrossRef] [Green Version]
- Gruter, M.O.; Brand, H.S. Oral health complications after a heart transplant: A review. Br. Dent. J. 2020, 228, 177–182. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Dinshaw, K.; Nene, B.M. Cervical and oral cancer screening in India. J. Med. Screen. 2006, 13 (Suppl. 1), S35–S38. [Google Scholar]
- Nagasaka, M.; Zaki, M.; Kim, H. PD1/PD-L1 inhibition as a potential radiosensitizer in head and neck squamous cell carcinoma: A case report. J. Immunother. Cancer 2016, 4, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapoor, V.; Aggarwal, S.; Das, S.N. 6-Gingerol Mediates its Anti- Tumor Activities in Human Oral and Cervical Cancer Cell Lines through Apoptosis and Cell Cycle Arrest. Phytother. Res. 2016, 30, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Ha, N.H.; Park, D.G.; Woo, B.H. Porphyromonas gingivalis increases the invasiveness of oral cancer cells by upregulating IL-8 and MMPs. Cytokine 2016, 86, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.G. Aetiology of oral cancer in the Sudan. J. Oral Maxillofac. Res. 2013, 4, e3. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A. Viruses and Oral Cancer: Crossreactivity as a Potential Link. Anticancer Agents Med. Chem. 2015, 15, 1224–1229. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors-Year | Study Setting | Study Design | No. Patients (Gender) | Cause of Immunodepression | No. Patients Who Delevoped Oral Cancer | % of Oral Cancer (Cancer/Tot) | Age (Mean) | Gender | Aim | Oral Cancer Site | Follow Up (Years) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Organ Transplant | |||||||||||
| Spolidorio, 2006 [19] | São Paulo Hospital | P | 155 (120 M, 35 F) | Cyclosporin A or tacrolimus | 3 | 1.93% | Unknown | NR | To determine the oral status of renal transplant recipients receiving cyclosporin A or tacrolimus as immunosuppressant | Lip | unknown |
| Jiang, 2010 [20] | Canadian Organ Replacement Register | R | 1703 (1405 M, 298 F) | Heart transplantation | 10 | 0.58% | 54.4 | NR | To assess the long-term risk of developing cancer among heart transplant recipients compared to the Canadian general population | NR | 6.08 years |
| Lòpez-Pintor, 2010 [21] | Hospital Universitario 12 de Octubre, Madrid, Spain | R | 500 (193 F, 307 M) | Renal transplantation | 6 | 1.2% | 57.33 | M | To establish the incidence of lip cancer (LC) in a population of renal transplant patients (RTPs) | lip | 18 |
| Ferreira da Silva, 2012 [22] | Department of the federal university of Sergipe, Brazil | R | 21 (7 F, 14 M) | Kidney transplantation | 1 | 4.76% | 42 | M | To investigate oral lesions in kidney transplant patients | lip | 2.5 (mean) |
| Ohman, 2014 [23] | Sahlgrenska University Hospital Register | R | 4590 (2839 M, 1751 F) | Transplantation | 51 | 1.11% | 62 | NR | To verify an increased risk of oral and lip cancer in solid organ transplantation patients | 4 tongue, 5 salivary glands, 3 floor of mouth, 3 gingiva, palate, bucca, 34 lip | Median 6.3 years |
| Narayan, 2018 [24] | Medwin Hospitals, Telangana, India | P | 332 | Renal transplantation | 5 | 1.50% | NR | NR | To identify the number of patients with renal transplant who developed second cancer | tongue | 26 |
| Jaamaa-Holmberg, 2019 [25] | NA | R | 479 (381 M, 98 F) | Heart transplantation | 13 | 2.71% | Unknown | NR | To demonstrate that cancer incidence in Finnish HTx-recipients is six times higher than in general Finnish population | 7 lip, 4 tongue, 1 salivary glands, 1 non specified | Median 7.8 years |
| Laprise, 2019 [26] | The scientific Registry of transplant recipients | R | 261,500 (174,475 M, 109,357 F) | Transplantation | 231 | 0.09% | 50 | NR | To evaluate the incidence of lip cancer after solid organ transplantation | 231 lip | Median 3.96 years |
| Lin, 2019 [27] | Changhua Christian Hospital | R | 455-2 (453) | Liver transplantation | 5 | 1.10% | 56 | 1 F, 4 M | To identify the number of head and neck cancer in liver transplant recipients | 3 tongue, 1 retromolar trigone, 1 buccal mucosa, 1 parotid gland | NR |
| Other Cancers | |||||||||||
| Johns, 1986 [28] | Johns Hopkins Medical Istitutions, Baltimore | R | 384 (206 F, 178 M) | Salivary gland or thyroid gland malignancies | 3 | 0.78% | NR | 1 F, 2 M | To determine the exact risk of multiple primary neoplasms in patients with salivary gland or thyroid gland malignancies | 3 salivary glands | 10 |
| Gutman, 1991 [29] | Tel Aviv Medical Center | P | 370 (133 M, 237 F) | Melanoma | 3 | 0.81% | 60.5 | F | To identify the number of patients with GVHD who developed second cancer | NR | Different based on stages |
| Lishner, 1991 [30] | Princess Margaret Hospital, Toronto | R | 321 | Non-Hodgkin’s lymphoma | 4 | 1.24% | 48 | 3 M, 1 unknown | To evaluate the incidence of second malignant tumors in patients with Non-Hodgkin’s lymphoma | 3 tongue, 1 gingiva | At least 6 months |
| Hiyama, 1991 [31] | Department of field research, Osaka | R | 61,168 (22,391 F, 38,777 M) | Stomach cancer | 51 | 0.08% | NR | NR | To determine the risk of second primary cancer after diagnosis of stomach cancer in Osaka | NR | 30 |
| Spitz, 1992 [32] | National Cancer Institute | R | 48,940 (F) | Cervix cancer | 34 | 0.07% | NR | F | To evaluate the association between malignancies of the upper aerodigestive tract and uterine cervix | NR | 11 years |
| Rabkin, 1992 [33] | National cancer institute, Belthesda | R | 28,160 (25,295 F, 2865 M) | Anal and cervical carcinoma | 51 | 0.18% | NR | NR | To determine the risk of second primary cancer following anal and cervical carcinoma | NR | NR |
| Levi, 1997 [34] | The Cancer Registries, Switzerland | R | 4639 | Skin Cancer | 16 | 0.34% | 74 | NR | To evaluate the incidence of second primary cancers in patients with skin cancer | 5 lip, 3 salivary gland, 8 mouth | 23 years |
| Levi, 1999 [35] | University of Milan, Italy | R | 5794 | Lung carcinoma | 15 | 0.26% | NR | NR | To determine the risk of second primary cancer in patients with lung carcinoma | NR | 22 |
| Levi, 2007 [36] | Universitè de Lausanne | R | 1672 (424 F, 1248 M) | Esophageal cancer | 67 | 4.00% | 55 | NR | To determine the risk of second neoplasms after esophageal cancer | NR | 30 |
| Chuang, 2008 [37] | Lyon, France | R | 52,589 (19,110 F, 33,479 M) | Esophageal cancer | 92 | 0.18% | NR | NR | To assess the risk of second primary cancers following a first primary esophageal cancer | NR | 10 |
| Brown, 2010 [38] | The National Cancer Institute’s Survival | R | 69,739 (F) | Endometrial cancer | 143 | 0.20% | 62 | F | To examine the risk of subsequent primary malignancies (SPMs) in women diagnosed with endometrial cancer. | NR | 11.2 years |
| Zhu, 2011 [39] | Academy of Medical Sciences, Gansu, China | R | 24,557 (6253 F, 18,304 M) | Treatment of esophageal cancer | 162 | 0.66% | NR | NR | To determine the risk of second primary cancer after treatment for esophageal cancer | NR | 34 |
| Hsu, 2014 [40] | Taiwan’s National Health Insurance | R | 9423 (1940 M, 7483 F) | Thyroid cancer | 53 | 0.56% | NR | NR | To determine the association of thyroid cancer with other malignancies in Taiwan. | 40 mouth, 13 salivary glands | NR |
| Robsahm, 2014 [41] | Cancer Registry of Norway | R | 52,689 (28,069 CMM, 24,620 SCC) | Squamous cell carcinoma and melanomas | 47 (CMM), 152 (SCC) | 0.37% | NR | 33 M, 14 F (CMM)/114 M, 38 F (SCC) | To examine the risk of a new primary cancer following an initial skin cancer | NR | 10.1 |
| Davis, 2014 [42] | University of Michigan Medical school | R | 441,504 (M) | Prostate cancer | 1251 | 0.28% | NR | NR | To determine the risk of second primary tumors in men with prostate cancer | NR | 10 |
| Hyeon Bae, 2015 [43] | Chonnam National University Hospital, Hwasun, Korea | R | 452 (208 M, 244 F) | Melanoma | 1 | 0.22% | Unknown | NR | To assess the presence of other primary cancer in patients with acral and non-acral melanomas | NR | No |
| Krilaviciute, 2016 [44] | National cancer institute, Vilnius, Lithuania | R | 12,584 (8074 F, 4510 M) | Basal cell carcinoma | 39 | 0.31% | NR | NR | To determine the risk of second primary cancer in basal cell carcinoma patients in Lithuania | 14 lip, 25 other in oral cavity | 14 |
| Schlieve, 2016 [45] | University of Tennessee | R | 19,406/849 | Primary Non-head-neck cancer | 32 | 80%/ | 67 | NR | To determine the rate of second primary head and neck cancer development among patients with a primary cancer diagnosed outside of the head and neck region, to present the clinical characteristics of this population, and to determine if any variables are associated with survival. | 11 gingiva, 7 tongue, 4 base of tongue, 4 buccal, 3 floor of mouth, 2 palate, 1 parotid | 10 years |
| Boakye, 2020 [46] | National Cancer Institute’s Surveillance | R | 2,903,241 | First primary cancers | 1877 | 0.064 | 63.1 | 1303 M, 574 F | To describe the risk of developing a second primary cancer among survivors of 10 cancer sites with the highest survival rates in the United States | 1462 tongue, 343 floor, 72 salivary glands | 3.8 years |
| Wu, 2020 [47] | People’s hospital of Nanjing, China | R | 1161 (542 F, 619 M) | Pulmonary high-grade neuroendocrine carcinoma | 13 | 1.12% | NR | NR | To determine the risk of second primary cancer in patients with pulmonary high-grade neuroendocrine carcinoma | floor of mouth, and gum and other mouth | 16 |
| Infectious Diseases | |||||||||||
| Song, 2019 [48] | The China Kadoorie Biobank | R | (a) 496,732 (203,660 M, 294,072 F) (b)37,336 (c) 97 (73 M, 24 F) | HBV | (a) 415 (b) no cases c) NR | (a) 1.98%/0.08% (b) no c) NR | (a) 51.5 (b) | NR | To assess the association between chronic HBV infection and risk of all cancer types | NR | (a) 8.85 (b) |
| Su, 2020 [49] | National Health insurance Research Database | P | 100,058 (50,029 HCV-50,029 NO HCV) + 47,904 (23 952 therapy-23,952 no therapy) | HCV and anti-HCV therapy | 229 (NO-HCV) 265 (HCV) + 146 (no therapy) 58 (therapy) | 0.47% | 59 (1 group)- 51 (2 group) | NR | To investigate the association between chronic hepatitis C and oral cancer, and the development of oral cancer after anti-hepatitis C virus (HCV) therapy | NR | 7.9 years non-HCV/5.1 years HCV + 4.9 years no therapy/3.4 years therapy |
| Mahale, 2020 [50] | Surveillance, Epidemiology, and End Results (SEER) | R | 531,460 (384,777 M, 146,683 F) | HIV+/lymphoid malignancies | 511 | 0.01% | NR | NR | To describe the risk of cancers following lymphoid malignancies among HIV-infected people. | NR | NR |
| HSC | |||||||||||
| Yokota, 2010 [51] | Kanto Study Group for Cell Therapy | R | 2062 (1225 M, 837 F) | Allogeneic hematopoietic SCT | 10 | 35.7%/0.48% | 42 | 5 M, 4 F, 1 Unknown | To evaluate the incidence and risk factors for secondary solid tumors in Japan after hematopoietic SCT | 5 tongue, 3 gingiva, 2 oral mucosa | Median 5.7 years |
| Curtis, 2016 [52] | Center for International Blood and Marrow Transplant Research | P | 24011 | GVHD | 24 | 13.11%/0.1% | NR | NR | To identify the number of patients with GVHD who developed second cancer | NR | 30 |
| Majhail, 2016 [53] | Center for International Blood and Marrow Transplant Research | R | 4318 (2415 M, 1903 F) | Hematopoietic cell transplant | 11 | 16.6%/0.25% | 44 | NR | To evaluate the risk of secondary solid cancers among allogeneic hematopoietic cell transplant recipients | NR | NR |
| Dyer, 2018 [54] | Blood and Marrow Transplant Network, Australia. | P | 441 (191 F, 250 M) | Blood and marrow transplant | 4 | 1.5% | NR | NR | To investigate oral health in blood and marrow transplant recipients | NR | 12 |
| Anak, 2018 [55] | Istanbul University Faculty of Istanbul Medicine, Our Children Leukemia Foundation BMT Center | P | 24 (12 M, 12 F) | Hematopoietic cell transplantation in Fanconi Anemia patients | 4 | 21 | NR | To investigate SCC development after HSCT and examine features of the follow-up patients | 4 retromolar trigone | NR | NR |
| Santarone, 2020 [56] | Bone marrow transplant center, Ospedale civile, Pescara, Italy | R | 908 (498 M, 410 F) | Hematopoietic cell transplantation | 12 | 100%/1.32% | 47 | 8 M, 4 F | To demonstrate that oral cGVHD and a diagnosis of non-malignant hematologic disease are strong risk factors in the SOC development | 6 tongue, 1 lower lip, 3 cheek mucosa, 1 gingival fornix, 1 hard palate | Unknown |
| Inflammatory Diseases | |||||||||||
| Bensing, 2008 [57] | National Death Register/Swedish Cancer Register | R | 3299 (1359 M, 1940 F) | Autoimmune primary adrenocortical insufficiency | 10 | 0.30% | NR | To assess the increased death risk and altered cancer incidence in patients with autoimmune primary adrenocortical insufficiency | NR | 29 years | |
| Zhang, 2009 [58] | Peking Union Medical College Hospital | R | 1320 (1201 F, 119 M) | Sjögren’s syndrome | 3 | 10% | 50.7 | NR | To identify the incidence of malignancy in primary Sjögren’s syndrome | 2 tongue, 1 parotid gland | 4.4 (mean) |
| Katsanos KH, 2015 [59] | Clinical Gastroenterology and Hepatology, NT.; USA | R | 7294 (3785 F, 3509 M) | Inflammatory bowel disease (IBD) | 11 | 0.15% | 44.6 | 4 F, 7 M | To identify the number of patients with IBD that developed oral cancer | 6 tongue, 2 hard palate, 3 buccal | NR |
| Rautemaa, 2016 [60] | Helsinki Hospital, Finland | R | 92 (47 F, 45 M) | APECED | 6 | 6.52% | 37 | 2 F, 4 M | To study the possible association of APECED with oral and esophageal carcinoma. | buccal mucosa | NR |
| Derk, 2019 [21] | Thomas Jefferson University Philadelphia, Pennsylvania, USA | P | 769 | Systemic sclerosis | 9 | 1.17% | 49.2 | NR | To describe the incidence of carcinoma of the tongue in a cohort of patients with systemic sclerosis | tongue | 16 |
| NR | |||||||||||
| Atsuta, 2014 [61] | Transplant Registry Unified Management Program | R | 17545 (10,386 M, 7149 F) | NR | 64 | 23.80% | NR | NR | To determine the incidence and the risk factors for secondary solid tumors after allogenic stem cell transplantation | NR | NR |
| Quality Assessment, Outcome: Oral Cancer Incidence in Patients with Immunosuppression | ||||||
|---|---|---|---|---|---|---|
| Question: Does the Immunosuppression Condition Have Influence on Oral Cancer Incidence? | ||||||
| Number of Studies according to meta-analysis | Study design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication bias |
| Meta-analysis on data from national registers (Figure 7): 23 studies | Cohort studies | Serious | Serious a | Not Serious | Serious b | Detected (1 study) |
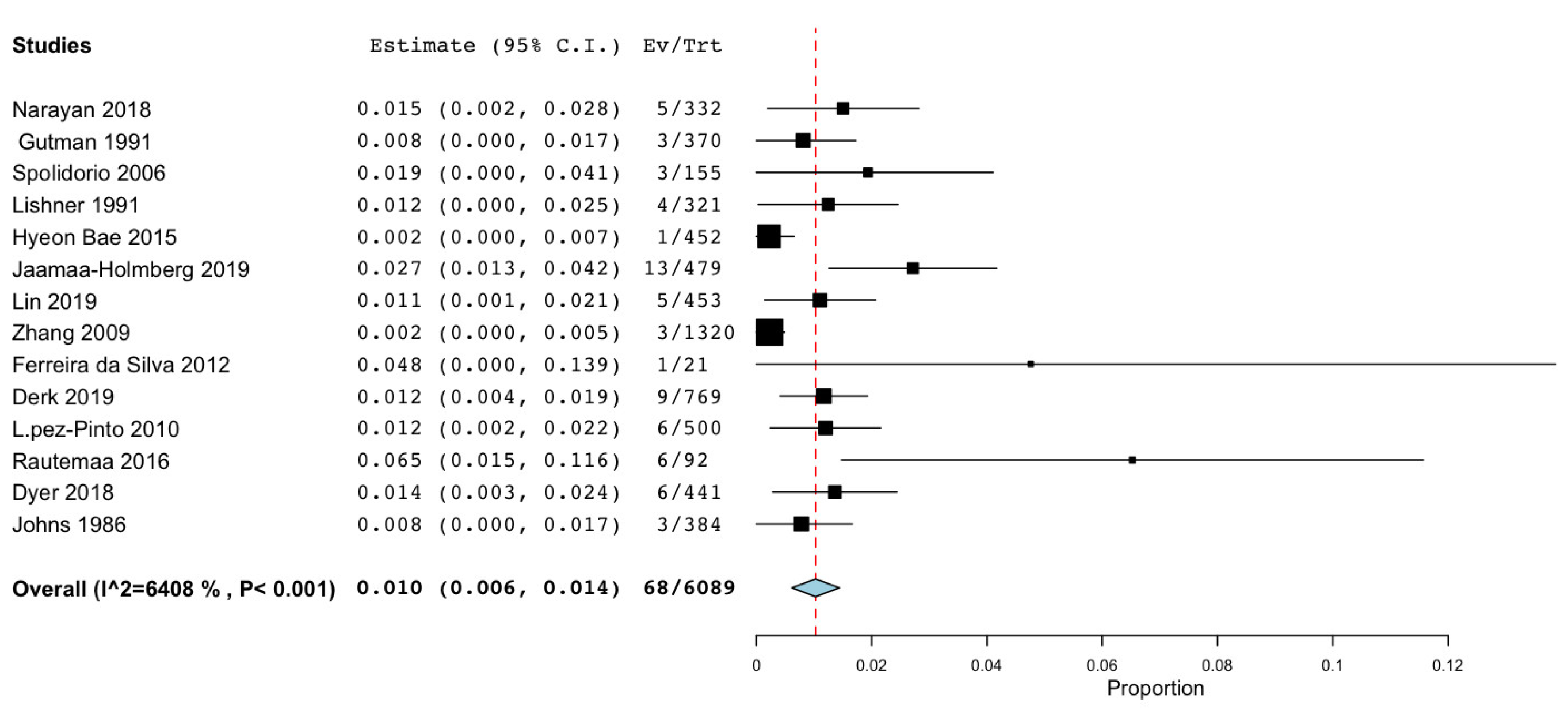
| Meta-analysis on data not from national registers (Figure 8): 14 studies | Cohort studies | Serious | Not Serious | Not Serious | Serious b | Undetected |
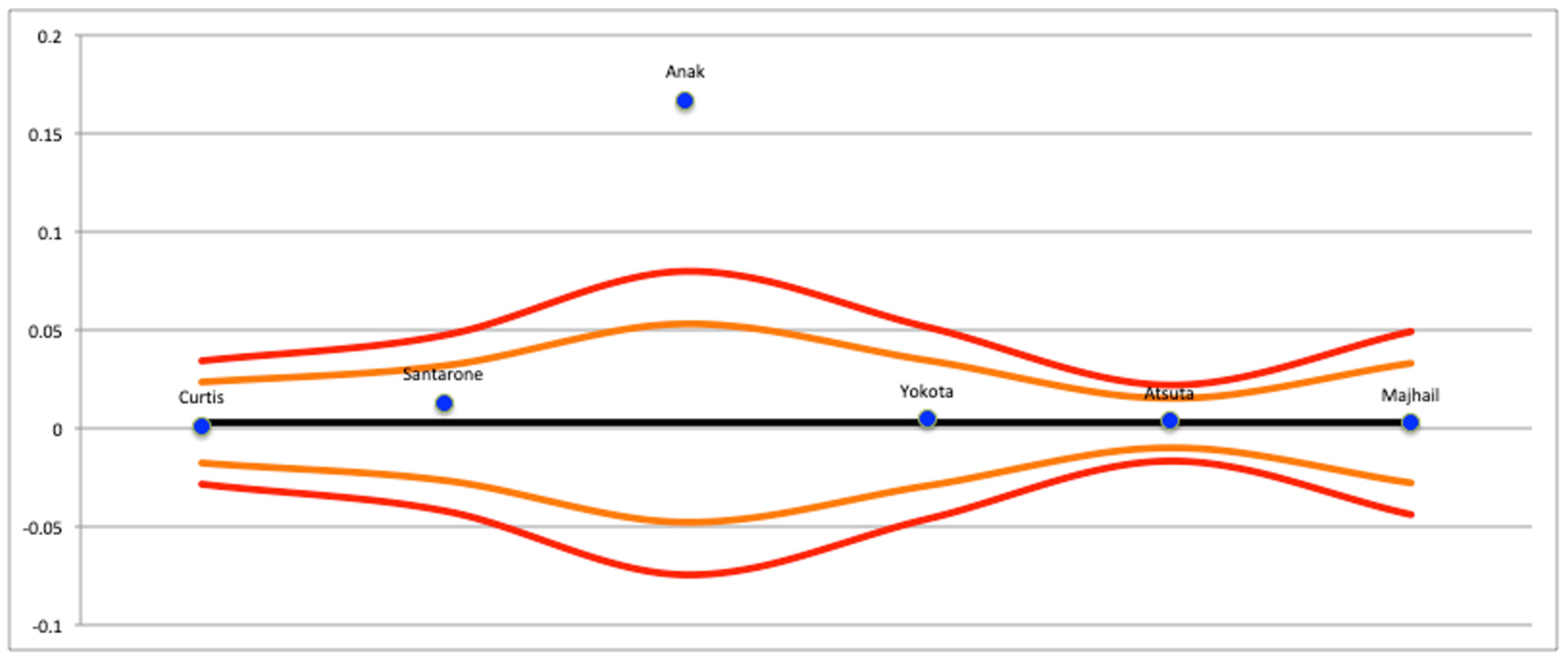
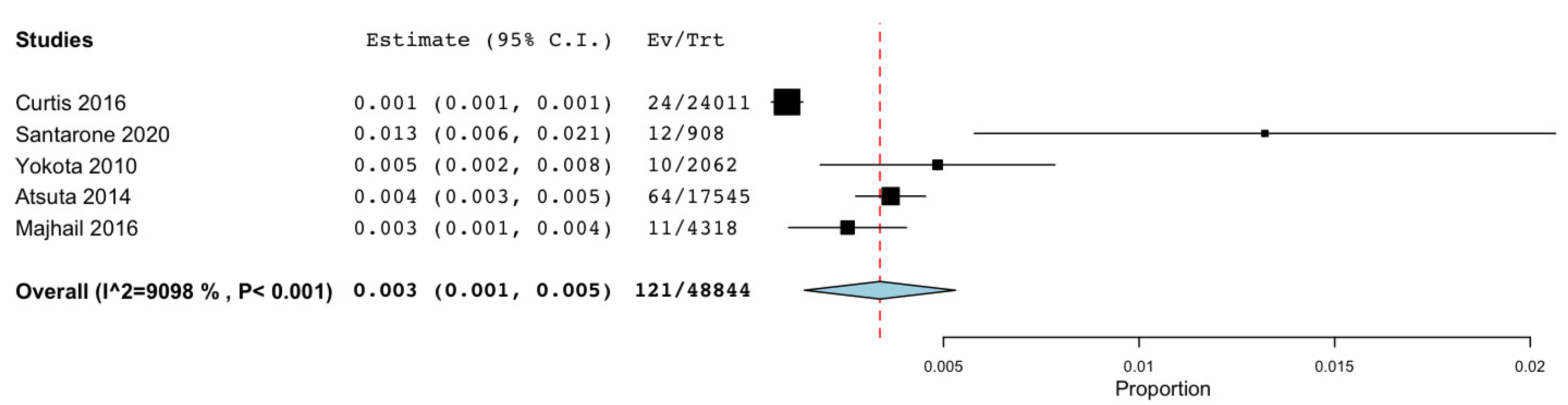
| Meta-analysis on GVHD patients (Figure 9): 5 studies | Cohort studies | Serious | Serious a | Not Serious | Serious b | Detected (1 study) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patini, R.; Cordaro, M.; Marchesini, D.; Scilla, F.; Gioco, G.; Rupe, C.; D’Agostino, M.A.; Lajolo, C. Is Systemic Immunosuppression a Risk Factor for Oral Cancer? A Systematic Review and Meta-Analysis. Cancers 2023, 15, 3077. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15123077
Patini R, Cordaro M, Marchesini D, Scilla F, Gioco G, Rupe C, D’Agostino MA, Lajolo C. Is Systemic Immunosuppression a Risk Factor for Oral Cancer? A Systematic Review and Meta-Analysis. Cancers. 2023; 15(12):3077. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15123077
Chicago/Turabian StylePatini, Romeo, Massimo Cordaro, Denise Marchesini, Francesco Scilla, Gioele Gioco, Cosimo Rupe, Maria Antonietta D’Agostino, and Carlo Lajolo. 2023. "Is Systemic Immunosuppression a Risk Factor for Oral Cancer? A Systematic Review and Meta-Analysis" Cancers 15, no. 12: 3077. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15123077