
Vascular and Urinary Tract Anatomic Variants Relevant to Para-Aortic Lymphadenectomy in Women with Gynecological Cancers

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
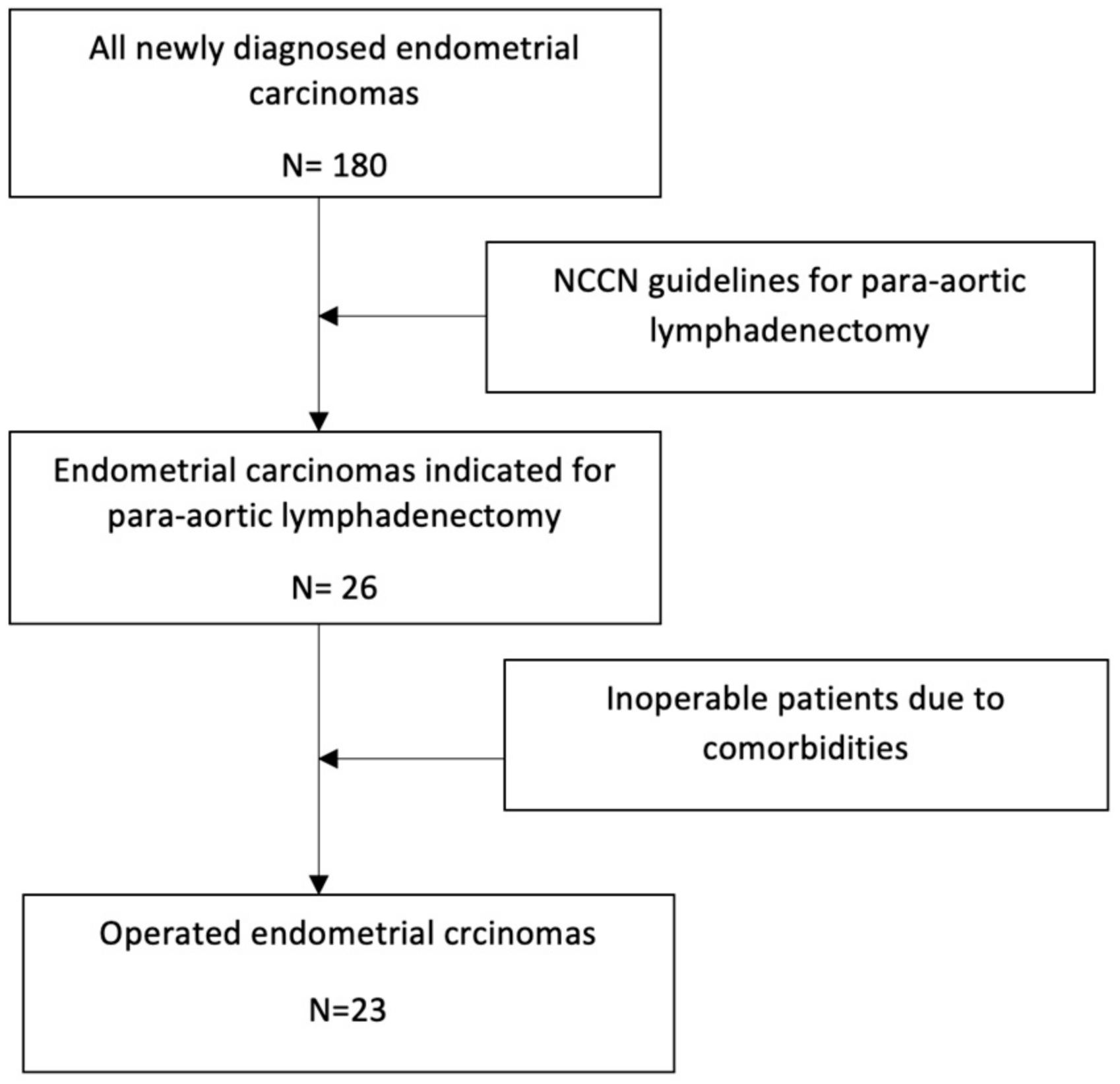
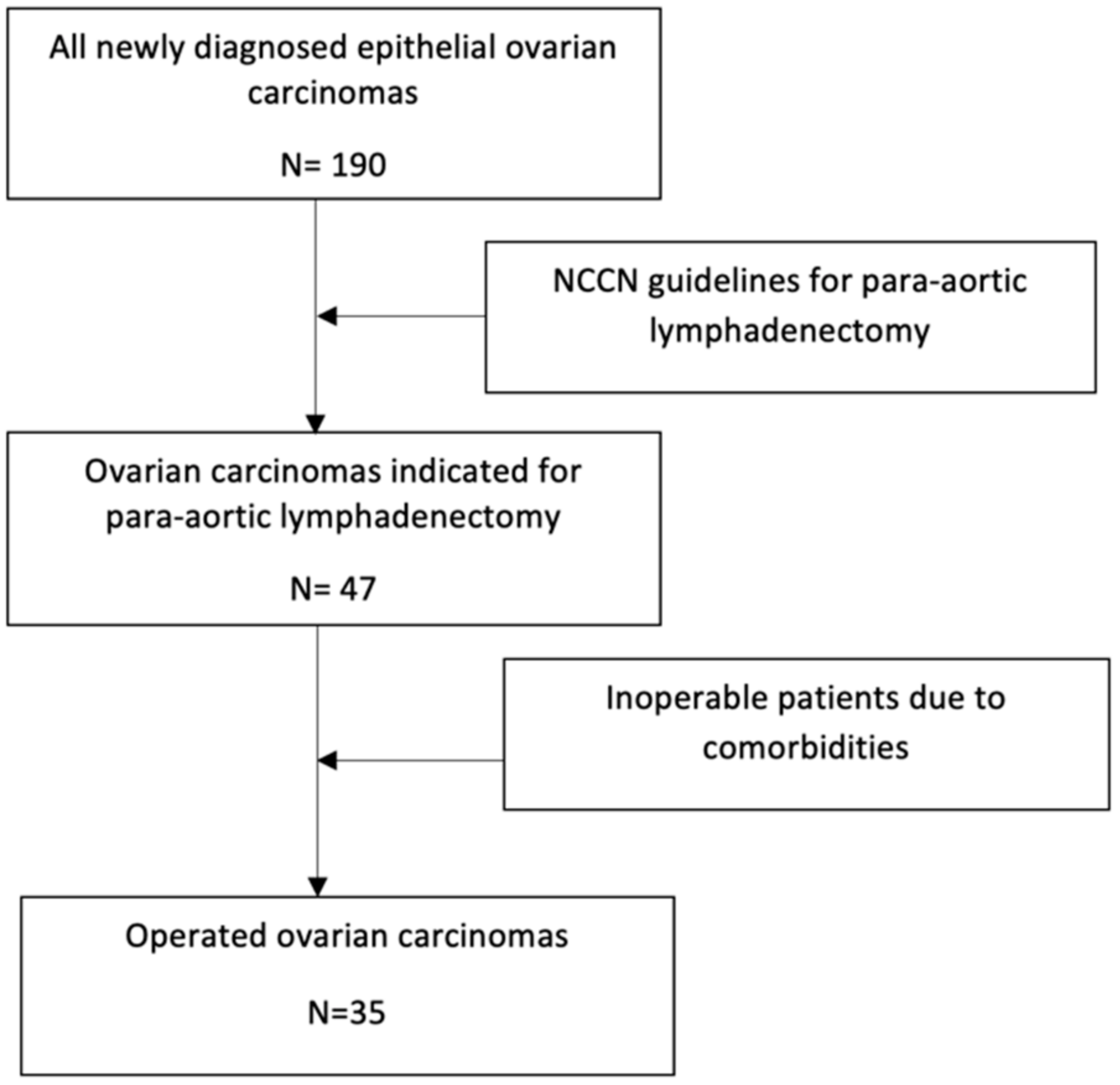
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Golia D’Augè, T.; Giannini, A.; Bogani, G.; Di Dio, C.; Laganà, A.S.; Di Donato, V.; Salerno, M.G.; Caserta, D.; Chiantera, V.; Vizza, E.; et al. Prevention, Screening, Treatment and Follow-Up of Gynecological Cancers: State of Art and Future Perspectives. Clin. Exp. Obstet. Gynecol. 2023, 50, 160. [Google Scholar] [CrossRef]
- Armstrong, D.K.; Alvarez, R.D.; Backes, F.J.; Bakkum-Gamez, J.N.; Barroilhet, L.; Behbakht, K.; Berchuck, A.; Chen, L.-M.; Chitiyo, V.C.; Cristea, M.; et al. NCCN Guidelines® Insights: Ovarian Cancer, Version 3.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Zikan, M.; Fischerova, D.; Kocian, R.; Germanova, A.; Burgetova, A.; Dusek, L.; Fartáková, Z.; Schneiderová, M.; Nemejcová, K.; et al. Pelvic Floor Reconstruction by Modified Rectus Abdominis Myoperitoneal (MRAM) Flap after Pelvic Exenterations. Gynecol. Oncol. 2017, 144, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the Management of Patients with Endometrial Carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer; National Comprehensive Cancer Network: Plymouth, PA, USA, 2023. [Google Scholar]
- Kovačević, N.; Šegedin, B.; Merlo, S.; Bebar, S.; Blatnik, A.; Cokan, A.; Cvjetićanin, B. Priporočila za Obravnavo Bolnic z Rakom Jajčnikov, Jajcevodov in s Primarnim Peritonealnim Seroznim Rakom v Sloveniji; Onkološki inštitut Ljubljana: Ljubljana, Slovenia, 2022. [Google Scholar]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Uterine Neoplasms; National Comprehensive Cancer Network: Plymouth, PA, USA, 2023. [Google Scholar]
- Šegedin, B.; Merlo, S.; Smrkolj, Š.; Bebar, S.; Blatnik, A.; Cerar, O.; Cvjetičanin, B.; Gazić, B.; Gornjac, A. Priporočila za Obravnavo Bolnic z Rakom Materničnega Telesa; Onkološki inštitut Ljubljana: Ljubljana, Slovenia, 2018. [Google Scholar]
- Bakkum-Gamez, J.N. Lymphadenectomy in the Management of Gynecologic Cancer. Clin. Obstet. Gynecol. 2019, 62, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Leborne, P.; Néron, M.; Colombo, P.E. An Anatomical Variation during Para-Aortic Lymphadenectomy. J. Visc. Surg. 2022, 159, 528–530. [Google Scholar] [CrossRef]
- White, H.J.; Bordes, S.J.; Borger, J. Anatomy, Abdomen and Pelvis: Aorta. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Baranski, A. Right-Sided Medial Visceral Rotation: The Cattel–Braasch Manoeuvre. In Surgical Technique of the Abdominal Organ Procurement: Step by Step; Baranski, A., Ed.; Springer: London, UK, 2009; pp. 45–53. ISBN 978-1-84800-251-7. [Google Scholar]
- Tobe, A.; Shirasu, T.; Furuya, T.; Nagai, M.; Nomura, Y. Cattell-Braasch Maneuver: A Gadget to Manipulate Abdominal Aortic Aneurysm in a Patient with a Left-Sided Inferior Vena Cava. Case Rep. Surg. 2019, 2019, 9789670. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, M.; Ohata, T.; Yamada, Y.; Yamana, F.; Nakahira, S. The Cattell-Braasch Maneuver Might Be a Good Option for a Huge Abdominal Aortic Aneurysm. J. Vasc. Surg. Cases Innov. Tech. 2019, 5, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Pomel, C.; Naik, R.; Martinez, A.; Ferron, G.; Nassif, J.; Dauplat, J.; Jeyarajah, A. Systematic (Complete) Para-Aortic Lymphadenectomy: Description of a Novel Surgical Classification with Technical and Anatomical Considerations: Complete Para-Aortic Lymphadenectomy. BJOG An. Int. J. Obstet. Gynaecol. 2012, 119, 249–253. [Google Scholar] [CrossRef]
- Zivanovic, O.; Sheinfeld, J.; Abu-Rustum, N.R. Retroperitoneal Lymph Node Dissection (RPLND). Gynecol. Oncol. 2008, 111, S66–S69. [Google Scholar] [CrossRef]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Haie Meder, C.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients with Cervical Cancer. Radiother. Oncol. 2018, 127, 404–416. [Google Scholar] [CrossRef]
- Aljabri, B.; MacDonald, P.S.; Satin, R.; Stein, L.S.; Obrand, D.I.; Steinmetz, O.K. Incidence of Major Venous and Renal Anomalies Relevant to Aortoiliac Surgery as Demonstrated by Computed Tomography. Ann. Vasc. Surg. 2001, 15, 615–618. [Google Scholar] [CrossRef]
- Jiménez Gil, R.; Morant Gimeno, F. Major Venous Anomalies and Abdominal Aortic Surgery. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 631–633. [Google Scholar] [CrossRef] [PubMed]
- Haładaj, R.; Polguj, M.; Wysiadecki, G.; Żytkowski, A.; Topol, M. Circumaortic Left Renal Vein (Circumaortic Renal Collar) Associated with the Presence of Vascular Anomalies: A Case Series and Review of Literature. Folia Morphol. 2019, 78, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Di Donato, V.; Di Pinto, A.; Giannini, A.; Caruso, G.; D’Oria, O.; Tomao, F.; Fischetti, M.; Perniola, G.; Palaia, I.; Muzii, L.; et al. Modified Fragility Index and Surgical Complexity Score Are Able to Predict Postoperative Morbidity and Mortality after Cytoreductive Surgery for Advanced Ovarian Cancer. Gynecol. Oncol. 2021, 161, 4–10. [Google Scholar] [CrossRef]
- Gopal, K.; Singh, O.; Anugar. Abnormal Pattern of Renal and Gonadal Veins and Its Developmental Correlation. Int. J. Anat. Res. 2017, 5, 4295–4298. [Google Scholar] [CrossRef]
- Hassan, S.S.; El-Shaarawy, E.A.; Johnson, J.C.; Youakim, M.F.; Ettarh, R. Incidence of Variations in Human Cadaveric Renal Vessels. Folia Morphol. 2017, 76, 394–407. [Google Scholar] [CrossRef]
- Namburu, B.S.P. A Study of Renal Veins. Int. J. Anat. Res. 2017, 5, 4463–4468. [Google Scholar] [CrossRef]
- Sośnik, H.; Sośnik, K. Renal Vascularization Anomalies in the Polish Population. Pol. Przegl. Chir. 2017, 89, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Pandya, V.; Patel, A.; Sutariya, H.; Gandhi, S. Evaluation of Renal Vascular Anatomy in Live Renal Donors: Role of Multi Detector Computed Tomography. Urol. Ann. 2016, 8, 270. [Google Scholar] [CrossRef]
- Zhu, J.; Zhang, L.; Yang, Z.; Zhou, H.; Tang, G. Classification of the Renal Vein Variations: A Study with Multidetector Computed Tomography. Surg. Radiol. Anat. 2015, 37, 667–675. [Google Scholar] [CrossRef]
- Hostiuc, S.; Minoiu, C.; Negoi, I.; Rusu, M.C.; Hostiuc, M. Duplication and Transposition of Inferior Vena Cava: A Meta-Analysis of Prevalence. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 7, 742–755. [Google Scholar] [CrossRef]
- Li, S.J.; Lee, J.; Hall, J.; Sutherland, T.R. The Inferior Vena Cava: Anatomical Variants and Acquired Pathologies. Insights Imaging 2021, 12, 123. [Google Scholar] [CrossRef] [PubMed]
- Kostov, S.; Selçuk, I.; Yordanov, A.; Kornovski, Y.; Yalçın, H.; Slavchev, S.; Ivanova, Y.; Dineva, S.; Dzhenkov, D.; Watrowski, R. Paraaortic Lymphadenectomy in Gynecologic Oncology-Significance of Vessels Variations. J. Clin. Med. 2022, 11, 953. [Google Scholar] [CrossRef] [PubMed]
- VonAchen, P.; Hamann, J.; Houghland, T.; Lesser, J.R.; Wang, Y.; Caye, D.; Rosenthal, K.; Garberich, R.F.; Daniels, M.; Schwartz, R.S. Accessory Renal Arteries: Prevalence in Resistant Hypertension and an Important Role in Nonresponse to Radiofrequency Renal Denervation. Cardiovasc. Revasc. Med. 2016, 17, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Gulas, E.; Wysiadecki, G.; Cecot, T.; Majos, A.; Stefańczyk, L.; Topol, M.; Polguj, M. Accessory (Multiple) Renal Arteries—Differences in Frequency According to Population, Visualizing Techniques and Stage of Morphological Development. Vascular 2016, 24, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Dogra, A.; Chauhan, R.S.; Sharma, S.; Partap, A.; Diwan, Y.; Chawla, K.; Negi, K.; Rana, S.; Diwan, D. Variations of Renal Arteries on 64 Slice Multidetector Computed Tomography. J. Anat. Soc. India 2017, 66, 20–25. [Google Scholar] [CrossRef]
- Gulas, E.; Wysiadecki, G.; Szymański, J.; Majos, A.; Stefańczyk, L.; Topol, M.; Polguj, M. Morphological and Clinical Aspects of the Occurrence of Accessory (Multiple) Renal Arteries. Arch. Med. Sci. 2018, 14, 442–453. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, J.; Mohanty, S.K.; Kim, T.; Sexton, W.J.; Powsang, J.; Spiess, P.E. Spectrum of Renal Pathology in Adult Patients with Congenital Renal Anomalies—A Series from a Tertiary Cancer Center. Ann. Diagn. Pathol. 2014, 18, 14–17. [Google Scholar] [CrossRef]
- Abou-El-Ghar, M.; Refaie, H.; Sharaf, D.; El-Diasty, T. Diagnosing Urinary Tract Abnormalities: Intravenous Urography or CT Urography? Rep. Med. Imaging 2014, 7, 55–63. [Google Scholar] [CrossRef]
- Dervishi, B.; Hyseni, F.; Musa, J.; Saliaj, K.; Vokshi, V.; Rakovica, L.; Nasiri, F.; Decka, A.; Ahsan, E.; Boshnjaku, I.; et al. The Importance of CT Urography in Early Diagnosis of Anatomical Variations in Urogenital Tract: Case Presentation. Radiol. Case Rep. 2022, 17, 4025–4029. [Google Scholar] [CrossRef] [PubMed]
- Muttarak, M.; Sriburi, T. Congenital Renal Anomalies Detected in Adulthood. Biomed. Imaging Interv. J. 2012, 8, e7. [Google Scholar] [CrossRef]
- Singh, J.; Singh, N.; Kapoor, K.; Sharma, M. Bilateral Malrotation and a Congenital Pelvic Kidney with Varied Vasculature and Altered Hilar Anatomy. Case Rep. Med. 2015, 2015, 848949. [Google Scholar] [CrossRef] [PubMed]
- Houat, A.P.; Guimarães, C.T.S.; Takahashi, M.S.; Rodi, G.P.; Gasparetto, T.P.D.; Blasbalg, R.; Velloni, F.G. Congenital Anomalies of the Upper Urinary Tract: A Comprehensive Review. Radiographics 2021, 41, 462–486. [Google Scholar] [CrossRef]
- Dorko, F.; Tokarčík, J.; Výborná, E. Congenital Malformations of the Ureter: Anatomical Studies. Anat. Sci. Int. 2016, 91, 290–294. [Google Scholar] [CrossRef]
- Didier, R.A.; Chow, J.S.; Kwatra, N.S.; Retik, A.B.; Lebowitz, R.L. The Duplicated Collecting System of the Urinary Tract: Embryology, Imaging Appearances and Clinical Considerations. Pediatr. Radiol. 2017, 47, 1526–1538. [Google Scholar] [CrossRef] [PubMed]
- Loftus, T.J.; Altieri, M.S.; Balch, J.A.; Abbott, K.L.; Choi, J.; Marwaha, J.S.; Hashimoto, D.A.; Brat, G.A.; Raftopoulos, Y.; Evans, H.L.; et al. Artificial Intelligence–Enabled Decision Support in Surgery: State-of-the-Art and Future Directions. Ann. Surg. 2023, 278, 51–58. [Google Scholar] [CrossRef]
- Sim, J.; Fong, Q.; Huang, W.; Tan, C. Machine Learning in Medicine: What Clinicians Should Know. Singap. Med. J. 2023, 64, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Bodenstedt, S.; Wagner, M.; Müller-Stich, B.P.; Weitz, J.; Speidel, S. Artificial Intelligence-Assisted Surgery: Potential and Challenges. Visc. Med. 2020, 36, 450–455. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number/Median Values (IQR) |
|---|---|
| Total number of patients | 58 |
| Endometrial cancer | 23 |
| Ovarian cancer | 35 |
| Age in years | 65 (21–83) (5–72) |
| Body mass index | 25.8 (19.3–41.3) (22.1–29.8) |
| Removed para-aortic lymph nodes | 31 (6–58) (28–37) |
| Removed pelvic lymph nodes | 13 (2–31) (10–19) |
| Anatomic Variants | Our Results | Literature | |
|---|---|---|---|
| Double inferior vena cava | 1/58 (1.7%) | 0.7% [15] | |
| Retro-aortic left renal vein | 2/58 (3.4%) | 2.1% [20] | |
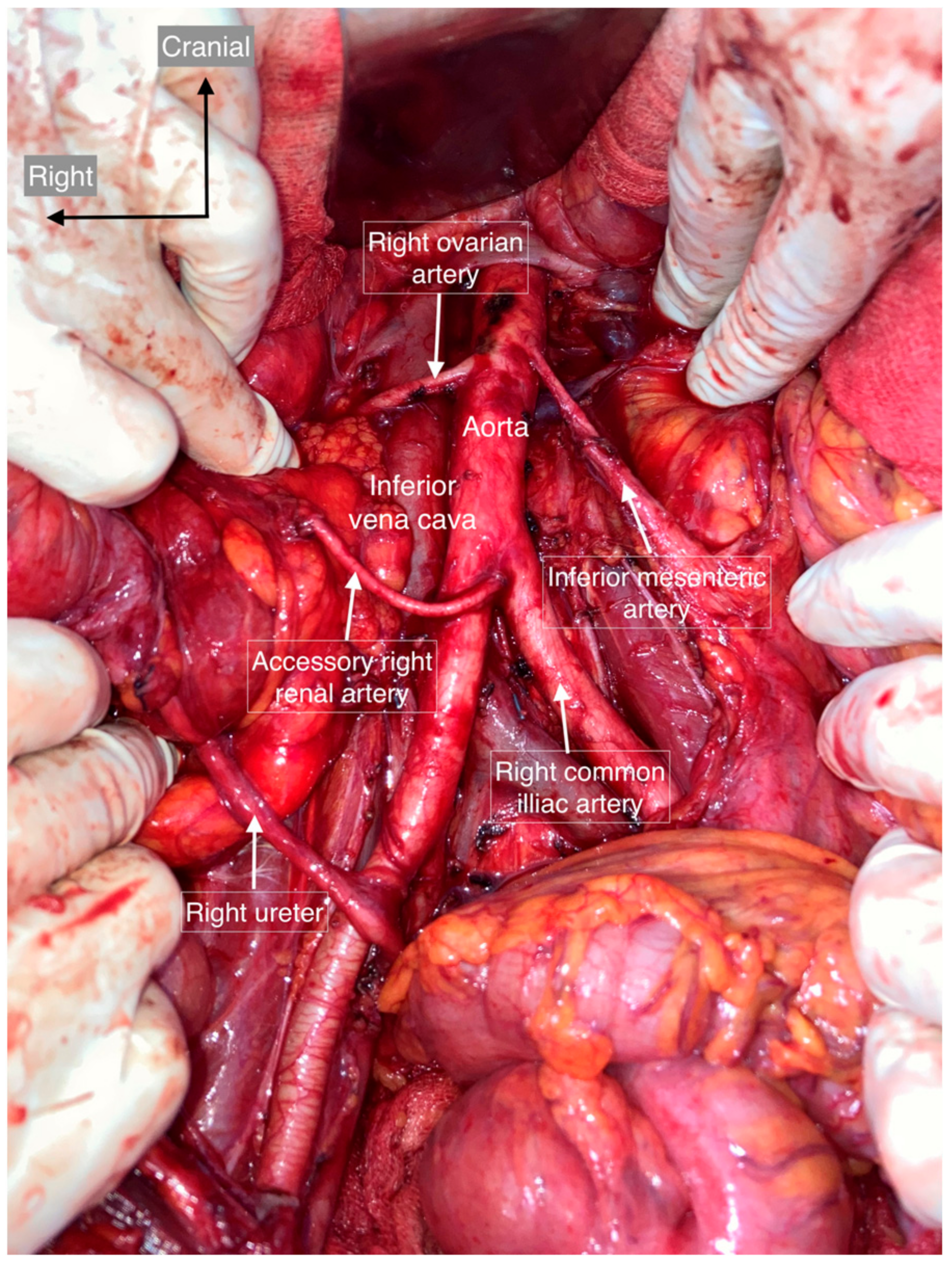
| Accessory renal arteries | 4/58 (6.8%) | 20–30% [16] | |
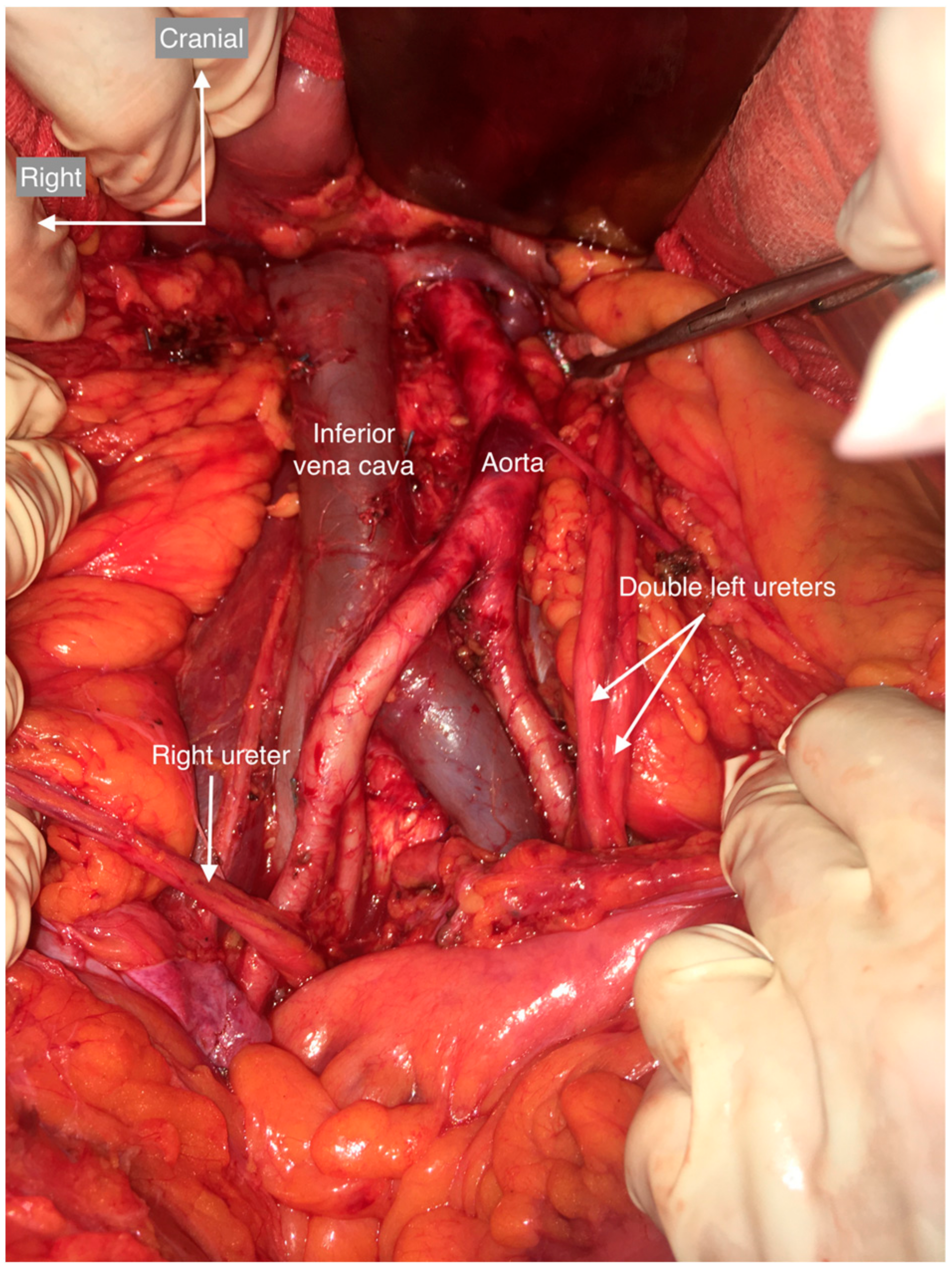
| Kidneys and urinary tract | Double left ureter | 2/58 (3.4%) | 3.3–11.1% [19] |
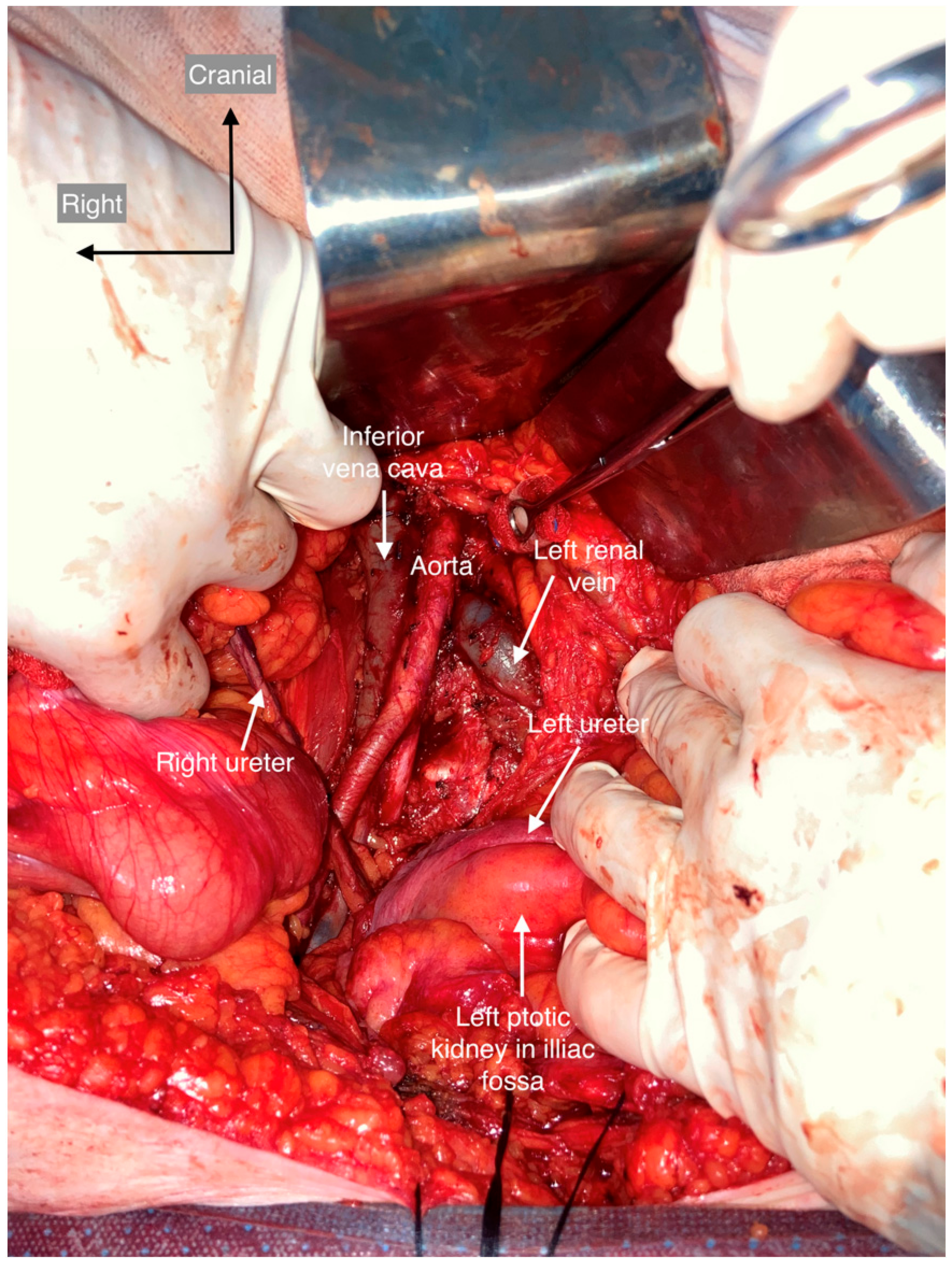
| Ptotic kidney | 1/58 (1.7%) | ||
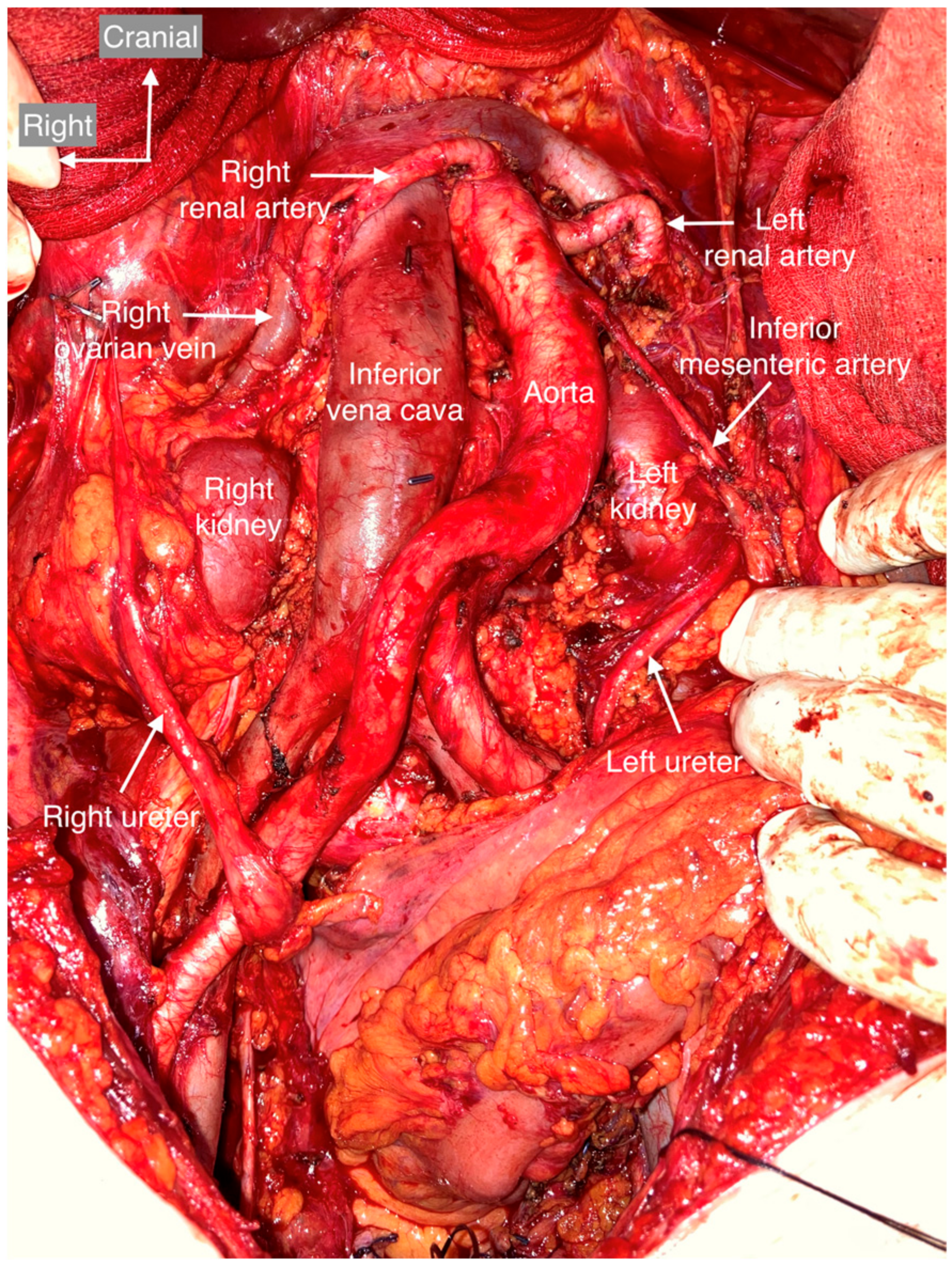
| Renal malrotation | 1/58 (1.7%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovačević, N.; Hočevar, M.; Vivod, G.; Merlo, S. Vascular and Urinary Tract Anatomic Variants Relevant to Para-Aortic Lymphadenectomy in Women with Gynecological Cancers. Cancers 2023, 15, 4959. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15204959
Kovačević N, Hočevar M, Vivod G, Merlo S. Vascular and Urinary Tract Anatomic Variants Relevant to Para-Aortic Lymphadenectomy in Women with Gynecological Cancers. Cancers. 2023; 15(20):4959. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15204959
Chicago/Turabian StyleKovačević, Nina, Marko Hočevar, Gregor Vivod, and Sebastjan Merlo. 2023. "Vascular and Urinary Tract Anatomic Variants Relevant to Para-Aortic Lymphadenectomy in Women with Gynecological Cancers" Cancers 15, no. 20: 4959. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15204959