
A Novel Methylation Marker NRN1 plus TERT and FGFR3 Mutation Using Urine Sediment Enables the Detection of Urothelial Bladder Carcinoma

 ,
,
Abstract
:Simple Summary
Abstract
1. Background
2. Materials and Methods
2.1. Study Cohort and Ethics Statement
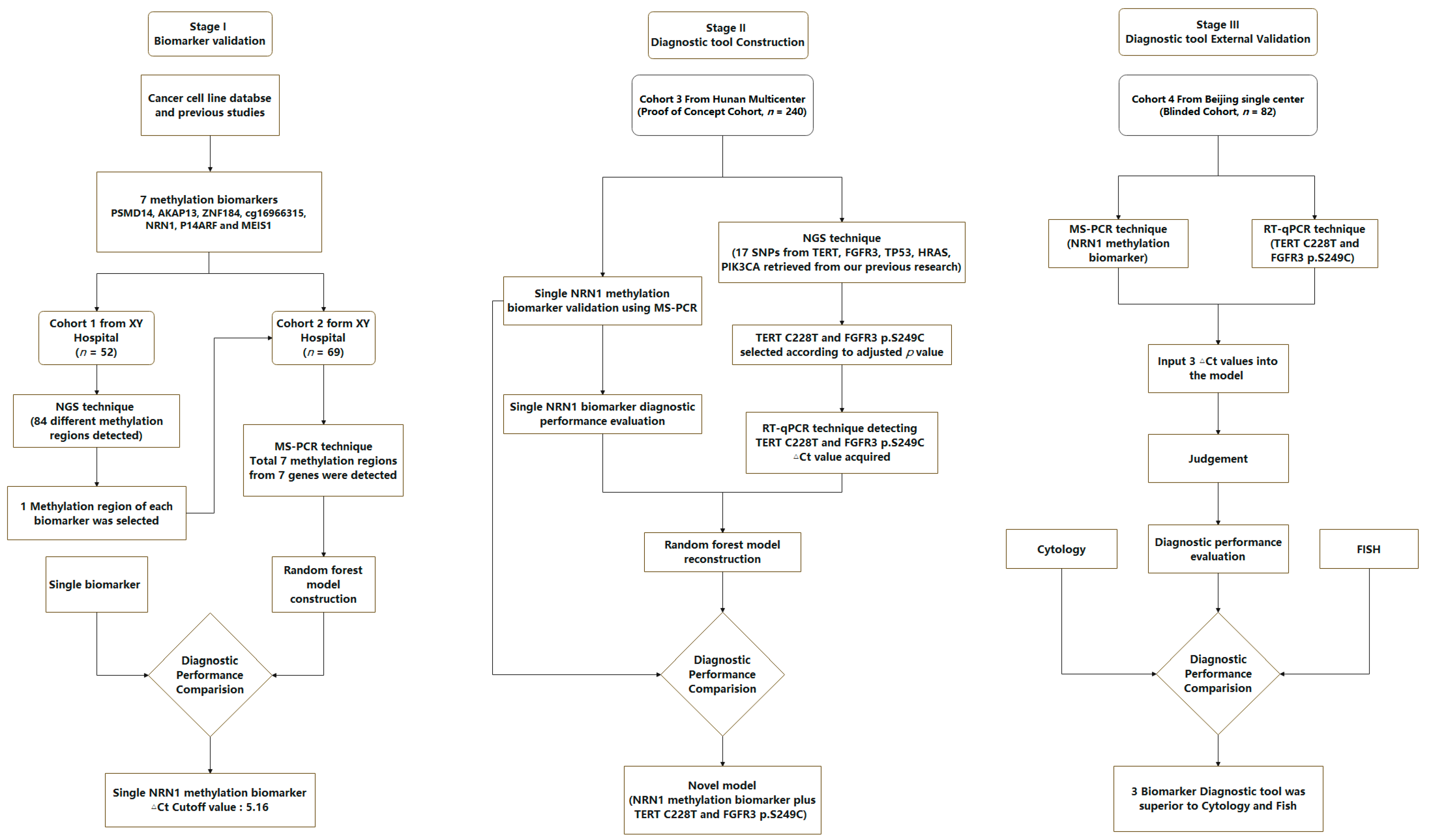
2.2. Study Design
2.3. Sample Collection, DNA Isolation and Sodium Bisulfite Conversion
2.4. Library Preparation and Sequencing
2.5. MS-PCR
2.6. RT-qPCR
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Flow Chart
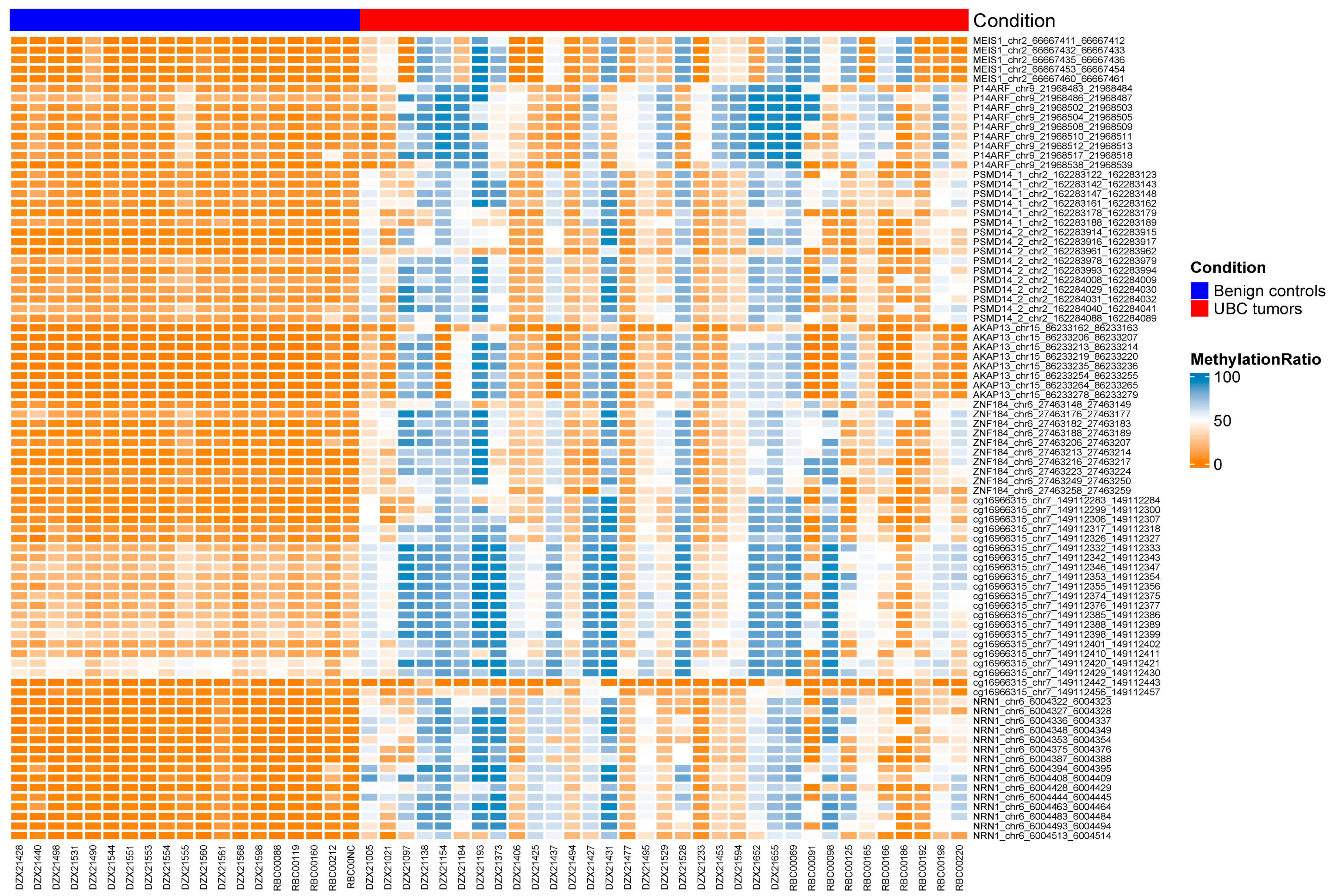
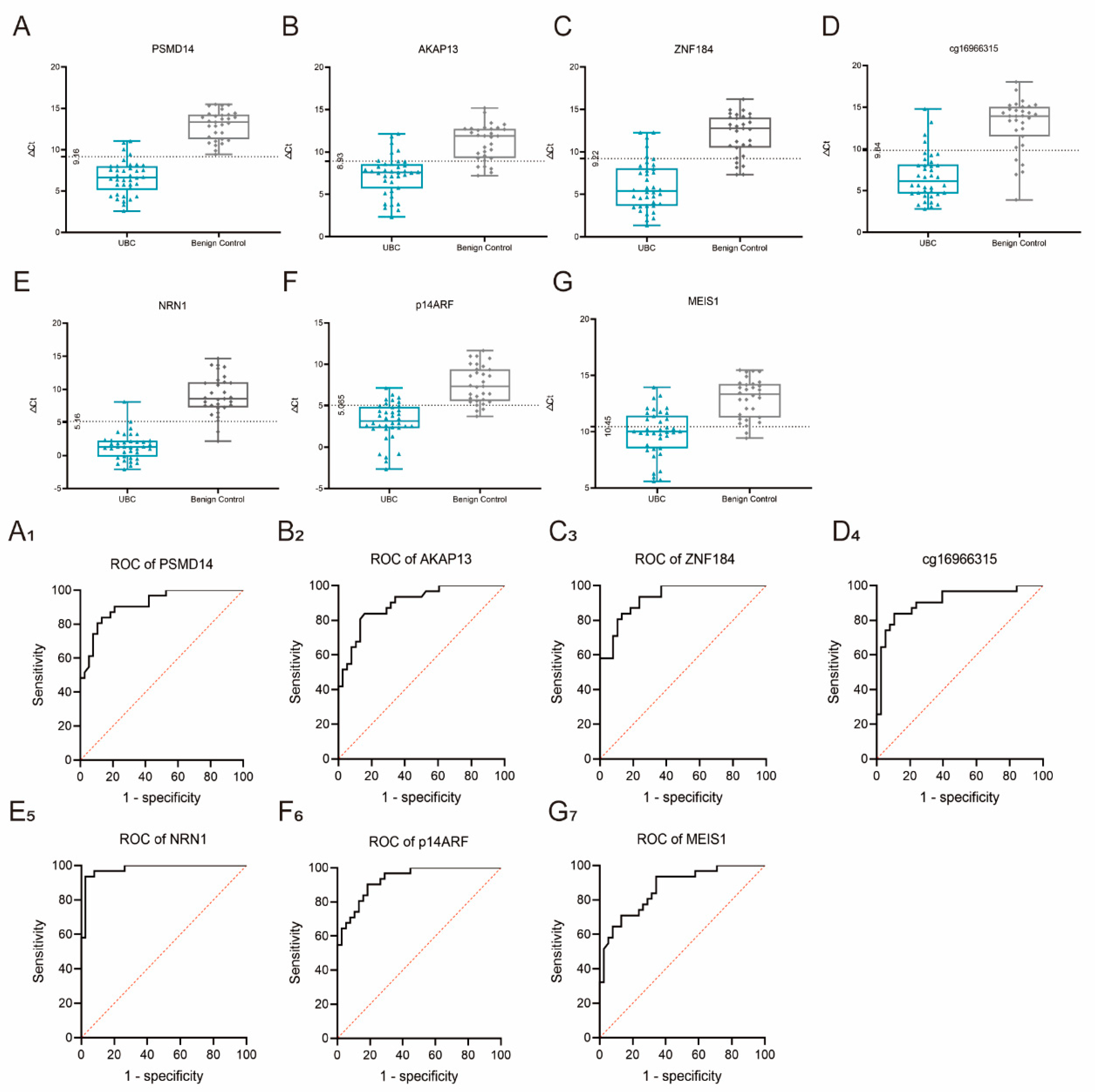
3.2. Validation of the Seven Methylation Biomarkers Using NGS and MS-PCR
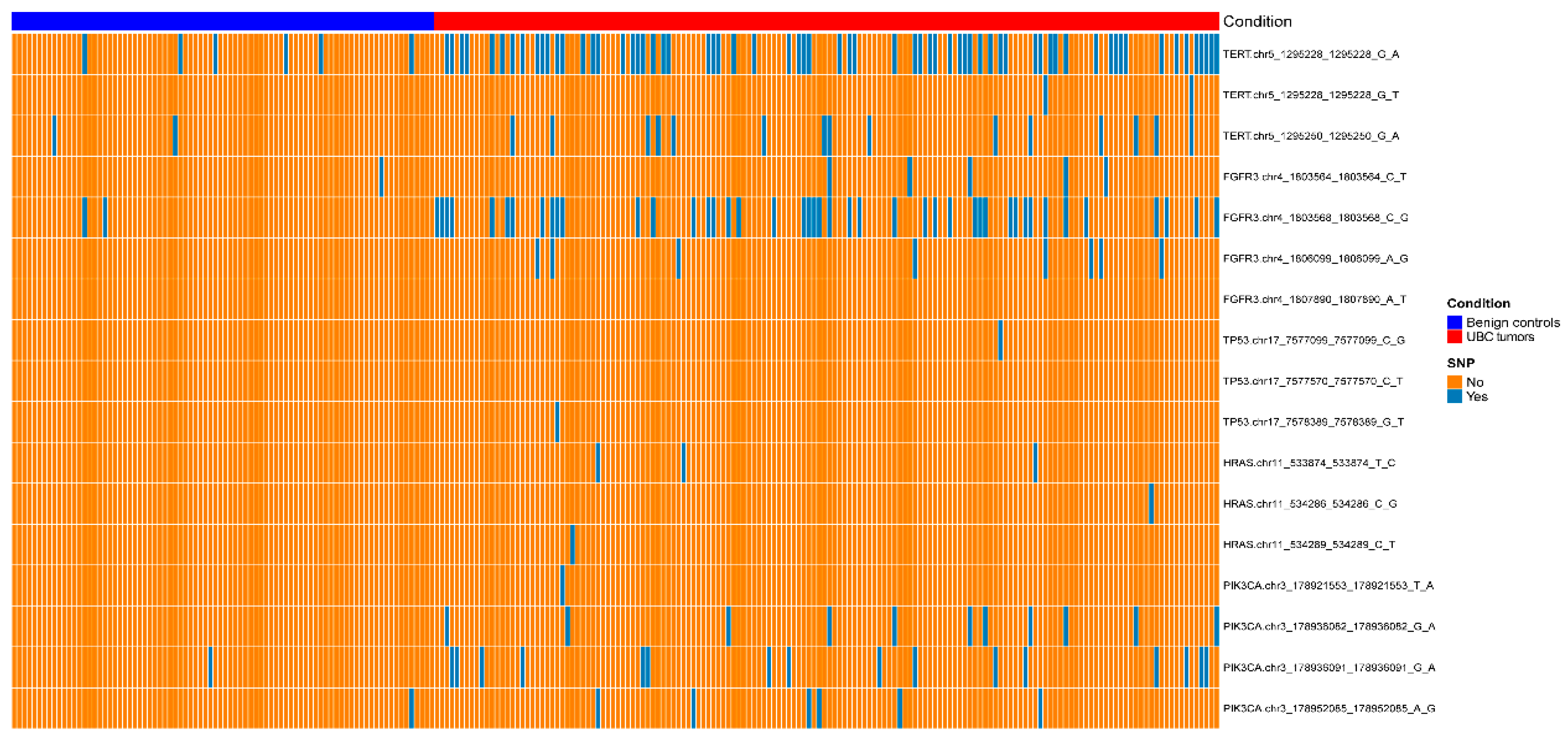
3.3. NRN1 Methylation Biomarker plus TERT C228T and FGFR3 p.S249C. as a Diagnostic Tool to Differentiate UBC from Benign Controls
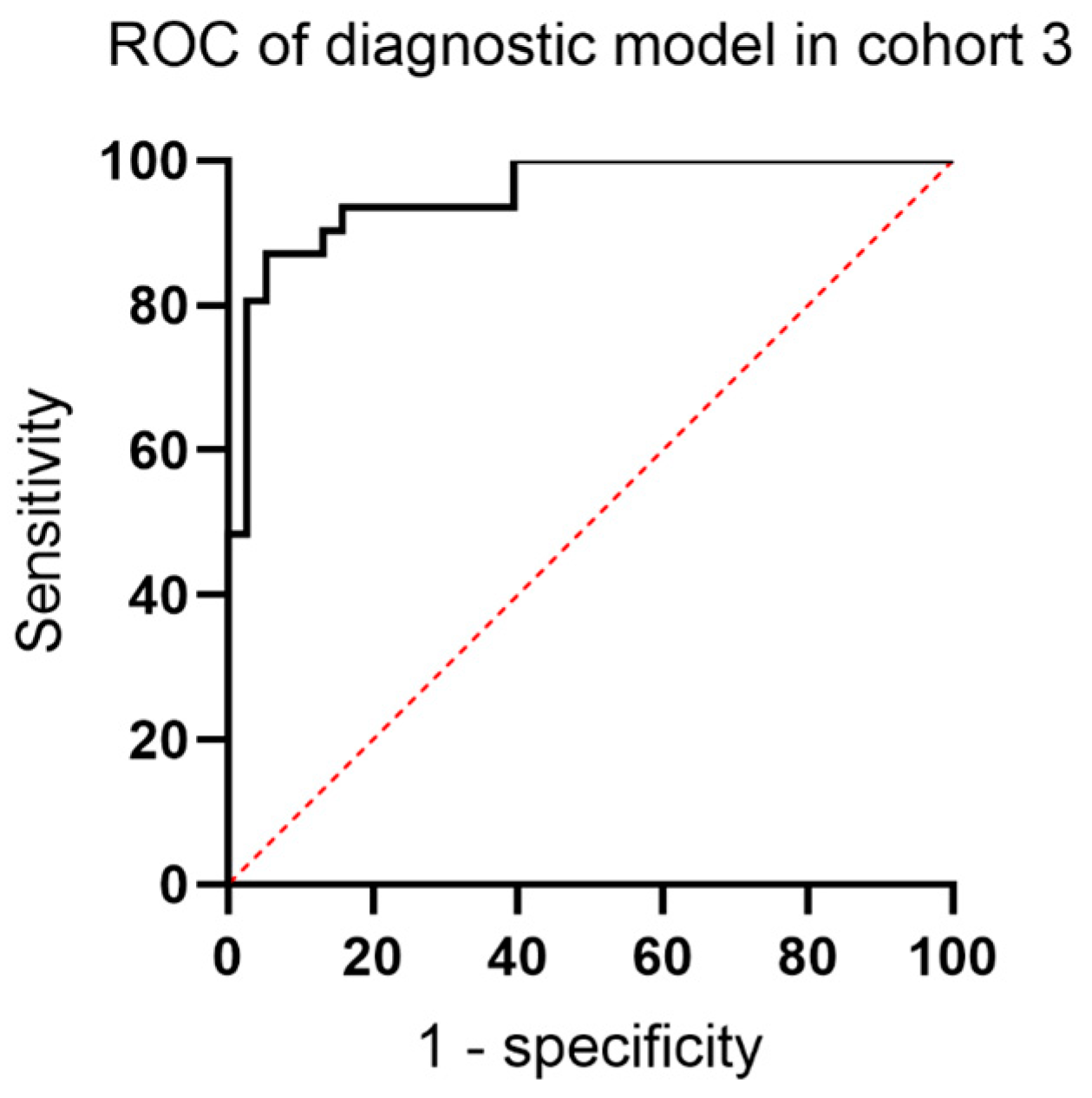
3.4. External Validation of the Model and Comparison with FISH and Cytology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sbizzera, M.; Descotes, F.; Arber, T.; Neuville, P.; Ruffion, A. Bladder cancer detection in patients with neurogenic bladder: Are cystoscopy and cytology effective, and are biomarkers pertinent as future diagnostic tools? A scoping review. World J. Urol. 2022, 40, 1897–1913. [Google Scholar] [CrossRef] [PubMed]
- Shang, D.; Liu, Y.; Xu, X.; Chen, Z.; Wang, D. Diagnostic value comparison of CellDetect, fluorescent in situ hybridization (FISH), and cytology in urothelial carcinoma. Cancer Cell Int. 2021, 21, 465. [Google Scholar] [CrossRef] [PubMed]
- Ge, G.; Peng, D.; Guan, B.; Zhou, Y.; Gong, Y.; Shi, Y.; Hao, X.; Xu, Z.; Qi, J.; Lu, H.; et al. Urothelial Carcinoma Detection Based on Copy Number Profiles of Urinary Cell-Free DNA by Shallow Whole-Genome Sequencing. Clin. Chem. 2020, 66, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Hentschel, A.; Beijert, I.; Bosschieter, J.; Kauer, P.; Vis, A.; Lissenberg-Witte, B.; van Moorselaar, R.; Steenbergen, R.; Nieuwenhuijzen, J. Bladder cancer detection in urine using DNA methylation markers: A technical and prospective preclinical validation. Clin. Epigenetics 2022, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Shivakumar, M.; Han, S.; Lee, Y.; Kim, D. Epigenetic interplay between methylation and miRNA in bladder cancer: Focus on isoform expression. BMC Genom. 2021, 22, 754. [Google Scholar] [CrossRef]
- Constancio, V.; Nunes, S.P.; Moreira-Barbosa, C.; Freitas, R.; Oliveira, J.; Pousa, I.; Oliveira, J.; Soares, M.; Dias, C.G.; Dias, T.; et al. Early detection of the major male cancer types in blood-based liquid biopsies using a DNA methylation panel. Clin. Epigenetics 2019, 11, 175. [Google Scholar] [CrossRef] [Green Version]
- Ahlquist, D.; Zou, H.; Domanico, M.; Mahoney, D.; Yab, T.; Taylor, W.; Butz, M.; Thibodeau, S.; Rabeneck, L.; Paszat, L.; et al. Next-generation stool DNA test accurately detects colorectal cancer and large adenomas. Gastroenterology 2012, 142, 248–256. [Google Scholar] [CrossRef] [Green Version]
- Witjes, J.; Morote, J.; Cornel, E.; Gakis, G.; van Valenberg, F.; Lozano, F.; Sternberg, I.; Willemsen, E.; Hegemann, M.; Paitan, Y.; et al. Performance of the Bladder EpiCheck™ Methylation Test for Patients Under Surveillance for Non-muscle-invasive Bladder Cancer: Results of a Multicenter, Prospective, Blinded Clinical Trial. Eur. Urol. Oncol. 2018, 1, 307–313. [Google Scholar] [CrossRef]
- Pietrusiński, M.; Kȩpczyński, Ƚ.; Jȩdrzejczyk, A.; Borkowska, E.; Traczyk-Borszyńska, M.; Constantinou, M.; Kaƚużewski, B.; Borowiec, M. Detection of bladder cancer in urine sediments by a hypermethylation panel of selected tumor suppressor genes. Cancer Biomark. Sect. A Dis. Markers 2017, 18, 47–59. [Google Scholar] [CrossRef]
- Beukers, W.; Kandimalla, R.; van Houwelingen, D.; Kovacic, H.; Chin, J.; Lingsma, H.; Dyrskjot, L.; Zwarthoff, E. The use of molecular analyses in voided urine for the assessment of patients with hematuria. PLoS ONE 2013, 8, e77657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.; Ke, H.; Wu, W.; Lee, Y.; Chang, L. Hypermethylation of E-cadherin, p16, p14, and RASSF1A genes in pathologically normal urothelium predict bladder recurrence of bladder cancer after transurethral resection. Urol. Oncol. 2012, 30, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Ou, Z.; Li, K.; Yang, T.; Dai, Y.; Chandra, M.; Ning, J.; Wang, Y.; Xu, R.; Gao, T.; Xie, Y.; et al. Detection of bladder cancer using urinary cell-free DNA and cellular DNA. Clin. Transl. Med. 2020, 9, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oeda, T.; Manabe, D. [The usefulness of urinary FDP in the diagnosis of bladder cancer: Comparison with NMP22, BTA and cytology]. Nihon Hinyokika Gakkai Zasshi. Jpn. J. Urol. 2001, 92, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Del Nero, A.; Esposito, N.; Currò, A.; Biasoni, D.; Montanari, E.; Mangiarotti, B.; Trinchieri, A.; Zanetti, G.; Serrago, M.; Pisani, E. Evaluation of urinary level of NMP22 as a diagnostic marker for stage pTa-pT1 bladder cancer: Comparison with urinary cytology and BTA test. Eur. Urol. 1999, 35, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Kandimalla, R.; Masius, R.; Beukers, W.; Bangma, C.; Orntoft, T.; Dyrskjot, L.; van Leeuwen, N.; Lingsma, H.; van Tilborg, A.; Zwarthoff, E. A 3-plex methylation assay combined with the FGFR3 mutation assay sensitively detects recurrent bladder cancer in voided urine. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2013, 19, 4760–4769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Kessel, K.; Van Neste, L.; Lurkin, I.; Zwarthoff, E.; Van Criekinge, W. Evaluation of an Epigenetic Profile for the Detection of Bladder Cancer in Patients with Hematuria. J. Urol. 2016, 195, 601–607. [Google Scholar] [CrossRef] [PubMed]
- van Kessel, K.E.M.; de Jong, J.J.; Ziel-van der Made, A.C.J.; Roshani, H.; Haensel, S.M.; Wolterbeek, J.H.; Boeve, E.R.; Oomens, E.; van Casteren, N.J.; Krispin, M.; et al. A Urine Based Genomic Assay to Triage Patients with Hematuria for Cystoscopy. J. Urol. 2020, 204, 50–57. [Google Scholar] [CrossRef]
- van Kessel, K.E.; Beukers, W.; Lurkin, I.; Ziel-van der Made, A.; van der Keur, K.A.; Boormans, J.L.; Dyrskjot, L.; Marquez, M.; Orntoft, T.F.; Real, F.X.; et al. Validation of a DNA Methylation-Mutation Urine Assay to Select Patients with Hematuria for Cystoscopy. J. Urol. 2017, 197, 590–595. [Google Scholar] [CrossRef]
- Li, P.; Ning, J.; Luo, X.; Du, H.; Zhang, Q.; Zhou, G.; Du, Q.; Ou, Z.; Wang, L.; Wang, Y. New method to preserve the original proportion and integrity of urinary cell-free DNA. J. Clin. Lab. Anal. 2019, 33, e22668. [Google Scholar] [CrossRef]
- Zito, A.; Cartelli, D.; Cappelletti, G.; Cariboni, A.; Andrews, W.; Parnavelas, J.; Poletti, A.; Galbiati, M. Neuritin 1 promotes neuronal migration. Brain Struct. Funct. 2014, 219, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Fatjó-Vilas, M.; Prats, C.; Pomarol-Clotet, E.; Lázaro, L.; Moreno, C.; González-Ortega, I.; Lera-Miguel, S.; Miret, S.; Muñoz, M.; Ibáñez, I.; et al. Involvement of NRN1 gene in schizophrenia-spectrum and bipolar disorders and its impact on age at onset and cognitive functioning. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2016, 17, 129–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prats, C.; Arias, B.; Ortet, G.; Ibáñez, M.; Moya, J.; Pomarol-Clotet, E.; Fañanás, L.; Fatjó-Vilas, M. Neurotrophins role in depressive symptoms and executive function performance: Association analysis of NRN1 gene and its interaction with BDNF gene in a non-clinical sample. J. Affect. Disord. 2017, 211, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Bosserhoff, A.; Schneider, N.; Ellmann, L.; Heinzerling, L.; Kuphal, S. The neurotrophin Neuritin1 (cpg15) is involved in melanoma migration, attachment independent growth, and vascular mimicry. Oncotarget 2017, 8, 1117–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisnieski, F.; Santos, L.; Calcagno, D.; Geraldis, J.; Gigek, C.; Anauate, A.; Chen, E.; Rasmussen, L.; Payão, S.; Artigiani, R.; et al. The impact of DNA demethylation on the upregulation of the NRN1 and TNFAIP3 genes associated with advanced gastric cancer. J. Mol. Med. 2020, 98, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, Y.; Fujita, K.; Nojima, S.; Tomiyama, E.; Matsushita, M.; Koh, Y.; Nakano, K.; Wang, C.; Ishizuya, Y.; Kato, T.; et al. TERT C228T mutation in non-malignant bladder urothelium is associated with intravesical recurrence for patients with non-muscle invasive bladder cancer. Mol. Oncol. 2020, 14, 2375–2383. [Google Scholar] [CrossRef]
- Springer, S.; Chen, C.; Rodriguez Pena, M.; Li, L.; Douville, C.; Wang, Y.; Cohen, J.; Taheri, D.; Silliman, N.; Schaefer, J.; et al. Non-invasive detection of urothelial cancer through the analysis of driver gene mutations and aneuploidy. eLife 2018, 7, e32143. [Google Scholar] [CrossRef]
- Min, J.; Shay, J. TERT Promoter Mutations Enhance Telomerase Activation by Long-Range Chromatin Interactions. Cancer Discov. 2016, 6, 1212–1214. [Google Scholar] [CrossRef] [Green Version]
- Chiba, K.; Lorbeer, F.; Shain, A.; McSwiggen, D.; Schruf, E.; Oh, A.; Ryu, J.; Darzacq, X.; Bastian, B.; Hockemeyer, D. TERTMutations in the promoter of the telomerase gene contribute to tumorigenesis by a two-step mechanism. Science 2017, 357, 1416–1420. [Google Scholar] [CrossRef] [Green Version]
- van Rhijn, B.; Mertens, L.; Mayr, R.; Bostrom, P.; Real, F.; Zwarthoff, E.; Boormans, J.; Abas, C.; van Leenders, G.; Götz, S.; et al. FGFR3 Mutation Status and FGFR3 Expression in a Large Bladder Cancer Cohort Treated by Radical Cystectomy: Implications for Anti-FGFR3 Treatment? Eur. Urol. 2020, 78, 682–687. [Google Scholar] [CrossRef]
- Roperch, J.; Hennion, C. A novel ultra-sensitive method for the detection of FGFR3 mutations in urine of bladder cancer patients—Design of the Urodiag® PCR kit for surveillance of patients with non-muscle-invasive bladder cancer (NMIBC). BMC Med. Genet. 2020, 21, 112. [Google Scholar] [CrossRef] [PubMed]
- Dodurga, Y.; Tataroglu, C.; Kesen, Z.; Satiroglu-Tufan, N. Incidence of fibroblast growth factor receptor 3 gene (FGFR3) A248C, S249C, G372C, and T375C mutations in bladder cancer. Genet. Mol. Res. GMR 2011, 10, 86–95. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Cohort 3 (Hunan Multicenter Cohort) | Cohort 4 (Beijing Cohort) | ||
|---|---|---|---|---|
| UBC | Control | UBC | Control | |
| Sample Size | 156 | 84 | 44 | 38 |
| Age, Years, Median (IQR) | 63 (54–70) | 58 (43–69) | 64(56.5–70) | 57 (47–62) |
| Gender | ||||
| Male | 114 | 64 | 34 | 35 |
| Female | 42 | 20 | 10 | 3 |
| Smoking History | ||||
| Smoker | 120 | 48 | 25 | 4 |
| Non-smokers | 36 | 36 | 19 | 34 |
| Stage | ||||
| pTa | 83 | / | 24 | / |
| pT1 | 40 | 7 | ||
| pT2 | 20 | / | 18 | / |
| pT3 | 8 | 4 | ||
| pT4 | 5 | 1 | ||
| Grade | ||||
| PUNLMP | 2 | / | 0 | / |
| Low grade | 53 | / | 15 | / |
| High grade | 101 | / | 29 | / |
| Tumor Type | ||||
| Primary | 147 | / | 44 | / |
| Recurrent | 9 | / | 0 | |
| Control Group | / | 84 | / | 38 |
| Urolithiasis | / | 57 | / | 28 |
| Infection | / | 21 | / | 10 |
| BPH | / | 4 | / | 0 |
| Renal cyst | / | 2 | / | 0 |
| TERT C228T | ||||
| Yes | 66 | 6 | 20 | 1 |
| No | 90 | 78 | 24 | 37 |
| FGFR3 p.S249C | ||||
| Yes | 44 | 2 | 7 | 0 |
| No | 112 | 82 | 37 | 38 |
| NRN1 methylation | ||||
| >5.16 | 133 | 12 | 37 | 5 |
| <5.16 | 23 | 72 | 7 | 33 |
| Cpg Site | AUC | Adjusted p Value |
|---|---|---|
| PSMD14_1_chr2_162283188_162283189 | 0.903508771929825 | 0.00000201 |
| PSMD14_2_chr2_162283978_162283979 | 0.87719298245614 | 0.0000024 |
| PSMD14_2_chr2_162284029_162284030 | 0.91786283891547 | 0.000000838 |
| PSMD14_2_chr2_162284031_162284032 | 0.896331738437002 | 0.0000079 |
| PSMD14_2_chr2_162284040_162284041 | 0.879585326953748 | 0.00000264 |
| PSMD14_2_chr2_162284088_162284089 | 0.883078152324325 | 0.00000201 |
| AKAP13_chr15_86233162_86233163 | 0.894736842105263 | 0.000319 |
| AKAP13_chr15_86233206_86233207 | 0.891547049441786 | 0.0000163 |
| AKAP13_chr15_86233213_86233214 | 0.90829346092504 | 0.0000165 |
| AKAP13_chr15_86233219_86233220 | 0.909888357256778 | 0.0000135 |
| AKAP13_chr15_86233264_86233265 | 0.893939393939394 | 0.0000288 |
| AKAP13_chr15_86233278_86233279 | 0.890255183675756 | 0.0000198 |
| ZNF184_chr6_27463148_27463149 | 0.968102073365231 | 2.91 × 10−8 |
| ZNF184_chr6_27463176_27463177 | 0.9792663476874 | 6.48 × 10−11 |
| ZNF184_chr6_27463206_27463207 | 0.984848484848485 | 1.76 × 10−9 |
| ZNF184_chr6_27463216_27463217 | 0.986443381180223 | 2.91 × 10−8 |
| ZNF184_chr6_27463223_27463224 | 0.985645933014354 | 1.68 × 10−9 |
| ZNF184_chr6_27463258_27463259 | 0.976076555435456 | 0.000000115 |
| cg16966315_chr7_149112306_149112307 | 0.910685805422648 | 0.000000831 |
| cg16966315_chr7_149112317_149112318 | 0.937799043062201 | 7.71 × 10−9 |
| cg16966315_chr7_149112376_149112377 | 0.923444976076555 | 1.89 × 10−8 |
| cg16966315_chr7_149112410_149112411 | 0.90829346092504 | 0.000000471 |
| cg16966315_chr7_149112420_149112421 | 0.87799043062201 | 0.00000552 |
| cg16966315_chr7_149112429_149112430 | 0.84051036765397 | 0.0000242 |
| NRN1_chr6_6004322_6004323 | 0.992025518341308 | 8.24 × 10−10 |
| NRN1_chr6_6004375_6004376 | 0.983253588516746 | 4.81 × 10−9 |
| NRN1_chr6_6004428_6004429 | 0.982456140350877 | 2.35 × 10−9 |
| NRN1_chr6_6004444_6004445 | 0.988038277511962 | 5.4 × 10−11 |
| NRN1_chr6_6004463_6004464 | 0.994417862838915 | 7.46 × 10−12 |
| NRN1_chr6_6004483_6004484 | 0.992025518767341 | 2.88 × 10−11 |
| P14ARF_chr9_21968483_21968484 | 0.933811802232855 | 0.00000128 |
| P14ARF_chr9_21968504_21968505 | 0.937001594896332 | 0.000000174 |
| P14ARF_chr9_21968508_21968509 | 0.931419457735247 | 0.000000115 |
| P14ARF_chr9_21968510_21968511 | 0.888357256778309 | 0.00000193 |
| P14ARF_chr9_21968512_21968513 | 0.934609250398724 | 0.000000286 |
| P14ARF_chr9_21968538_21968539 | 0.921850083230121 | 0.0000222 |
| MEIS1_chr2_66667411_66667412 | 0.88755980861244 | 0.0000143 |
| MEIS1_chr2_66667432_66667433 | 0.868421052631579 | 0.0000118 |
| MEIS1_chr2_66667435_66667436 | 0.878787878787879 | 0.0000102 |
| MEIS1_chr2_66667453_66667454 | 0.890749601275917 | 0.00000876 |
| MEIS1_chr2_66667460_66667461 | 0.891547049234238 | 0.00000827 |
| Variables | Diagnostic Tool | Cytology | Fish | |||
|---|---|---|---|---|---|---|
| + | − | + | − | + | − | |
| UBC + | 38 | 6 | 16 | 28 | 30 | 14 |
| UBC − | 4 | 34 | 4 | 34 | 3 | 35 |
| Sensitivity | 0.864 | 0.364 | 0.682 | |||
| Specificity | 0.895 | 0.895 | 0.921 | |||
| PPV | 0.905 | 0.800 | 0.909 | |||
| NPV | 0.850 | 0.548 | 0.714 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Xu, R.; Lu, Q.; Xu, Z.; Liu, J.; Li, P.; Zhang, Y.; Zhou, C.; Luo, L.; Tang, W.; et al. A Novel Methylation Marker NRN1 plus TERT and FGFR3 Mutation Using Urine Sediment Enables the Detection of Urothelial Bladder Carcinoma. Cancers 2023, 15, 615. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030615
Zhang J, Xu R, Lu Q, Xu Z, Liu J, Li P, Zhang Y, Zhou C, Luo L, Tang W, et al. A Novel Methylation Marker NRN1 plus TERT and FGFR3 Mutation Using Urine Sediment Enables the Detection of Urothelial Bladder Carcinoma. Cancers. 2023; 15(3):615. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030615
Chicago/Turabian StyleZhang, Junjie, Ran Xu, Qiang Lu, Zhenzhou Xu, Jianye Liu, Pei Li, Yaqun Zhang, Chuanchi Zhou, Lufeng Luo, Wei Tang, and et al. 2023. "A Novel Methylation Marker NRN1 plus TERT and FGFR3 Mutation Using Urine Sediment Enables the Detection of Urothelial Bladder Carcinoma" Cancers 15, no. 3: 615. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030615