
Phase I Trial of [99mTc]Tc-maSSS-PEG2-RM26, a Bombesin Analogue Antagonistic to Gastrin-Releasing Peptide Receptors (GRPRs), for SPECT Imaging of GRPR Expression in Malignant Tumors
 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
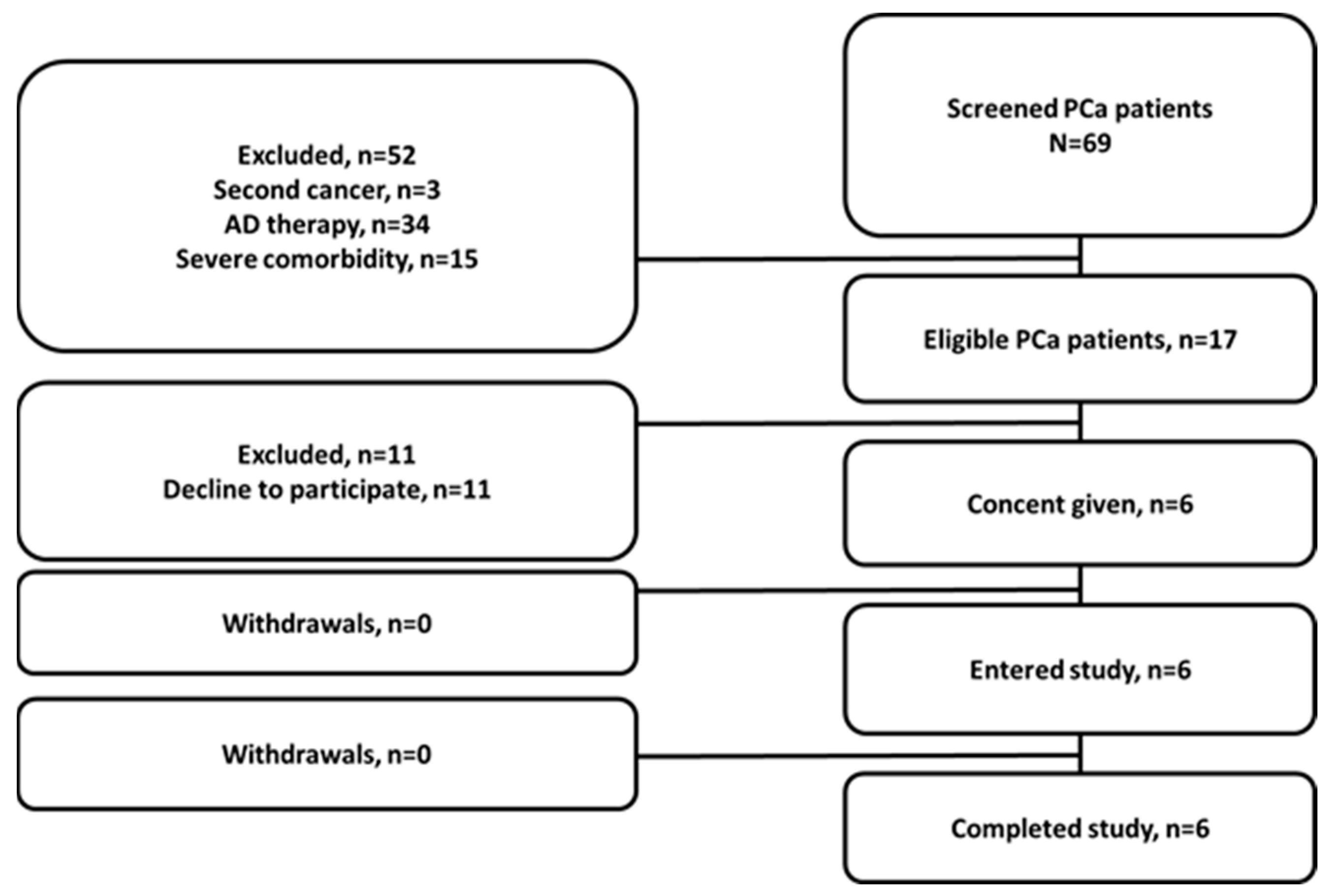
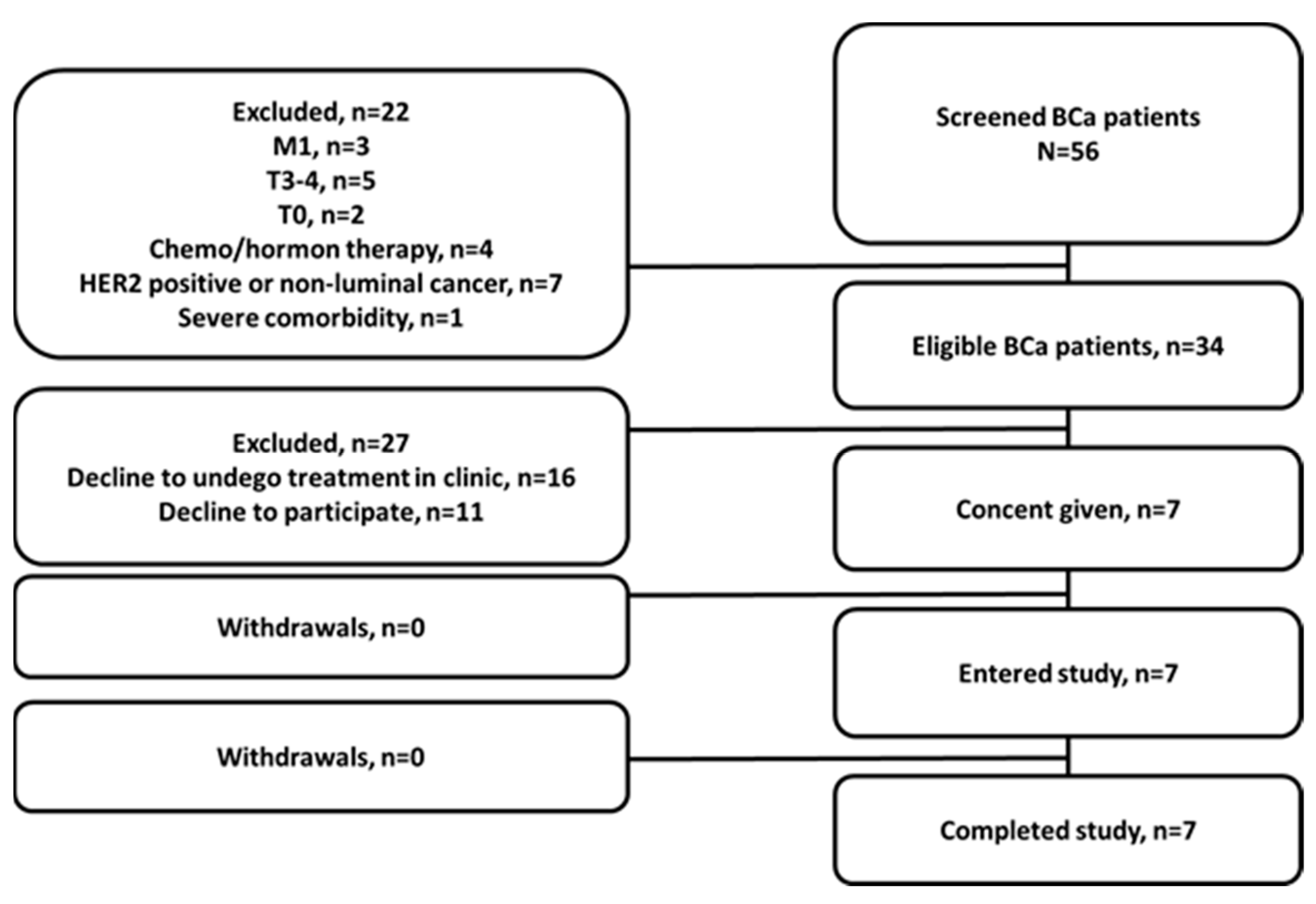
2.1. Patients
2.2. Imaging Protocol
2.3. Immunohistochemical Evaluation of Patient Material on GRPR Expression
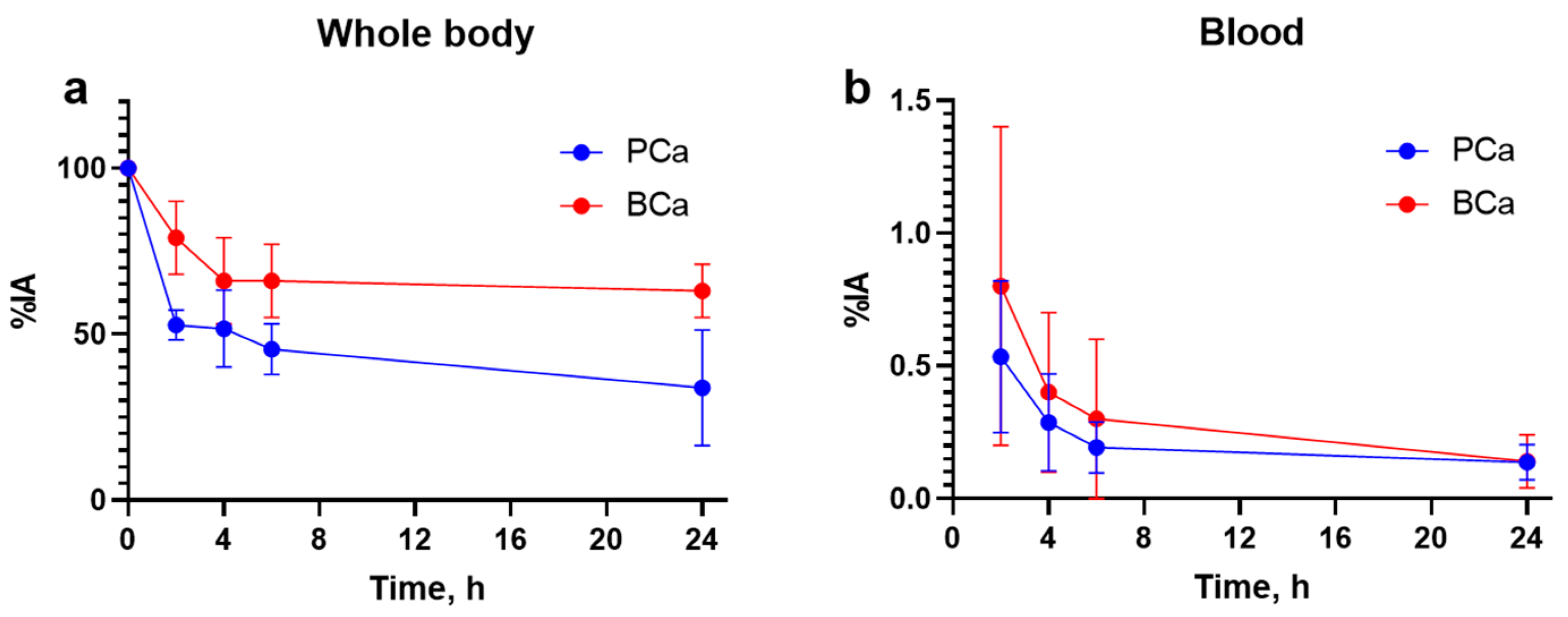
2.4. Analysis of Biodistribution and Assessment of Dosimetry
2.5. Statistical Analysis
3. Results
3.1. Patients
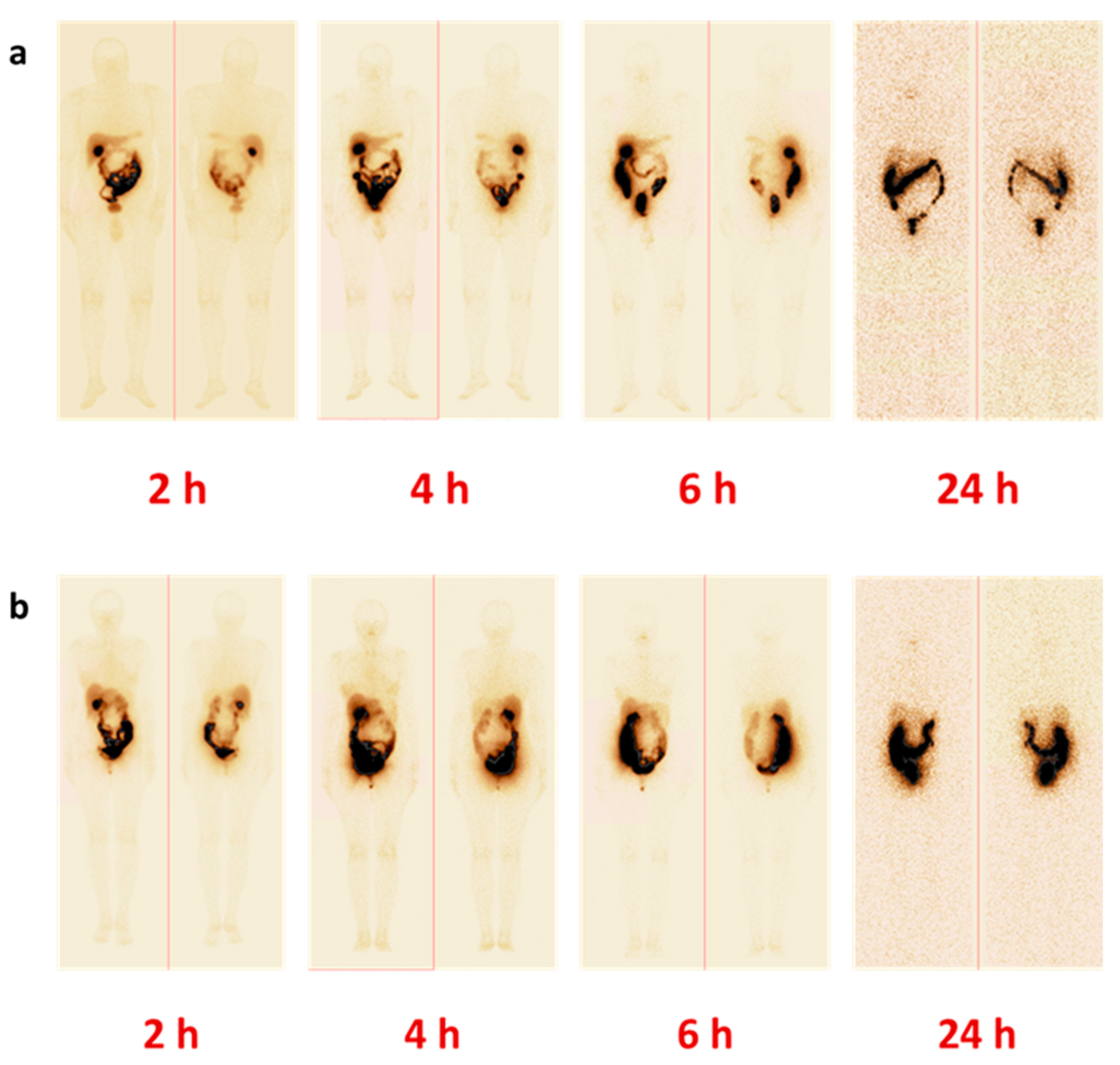
3.2. Safety, Tolerability, and Distribution of [99mTc]Tc-maSSS-PEG2-RM26
3.3. Assessment of Dosimetry
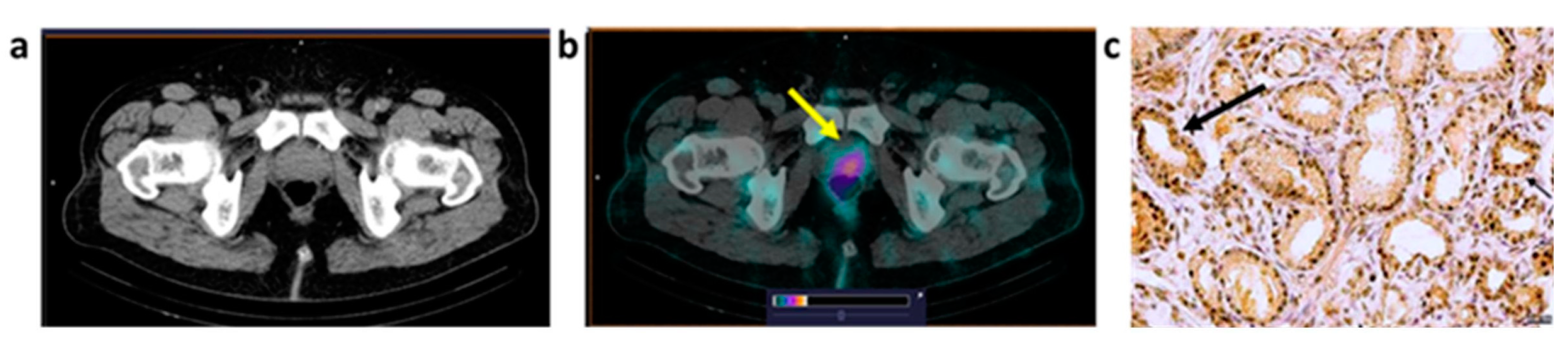
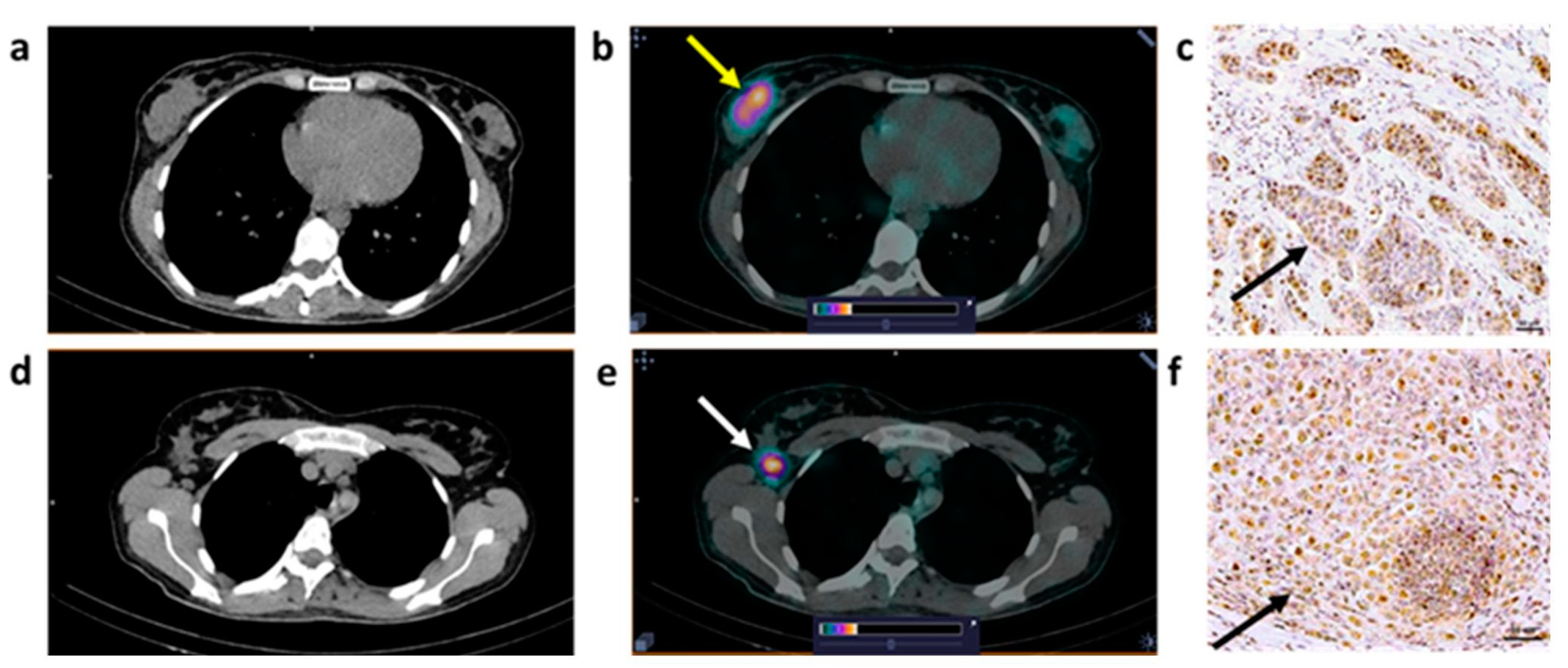
3.4. Imaging Data Analysis
3.5. Immunohistochemical Staining
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male/PCa | 2 h | 4 h | 6 h | 24 h |
| Kidney | 2.9 ± 0.9 | 3 ± 3 | 3 ± 1 | 2.4 ± 0.9 |
| Urinary bladder | 4 ± 6 | 2 ± 1 | 0.6 ± 0.4 | 0.16 ± 0.07 |
| Liver | 4 ± 2 | 2.2 ± 0.8 | 1.8 ± 0.6 | 2 ± 1 |
| Gall bladder | 2 ± 2 | 2 ± 2 | 2 ± 2 | 2.2 ± 0.3 |
| Jejunum | 12 ± 12 | 9 ± 9 | 9 ± 19 | 10 ± 1 |
| Upper colon | 1.1 ± 1.0 | 8 ± 3 | 20 ± 13 | 7 ± 8 |
| Lower colon | 0.6 ± 0.5 | 0.2 ± 0.2 | 0.5 ± 0.4 | 0.4 ± 0.2 |
| Female/BCa | 2 h | 4 h | 6 h | 24 h |
| Kidney | 5 ± 3 | 3 ± 3 | 3 ± 3 | 5 ± 5 |
| Urinary bladder | 4 ± 7 | 1 ± 2 | 0.3 ± 0.3 | 0.2 ± 0.2 |
| Liver | 6 ± 2 | 3.0 ± 1.0 | 3 ± 2 | 2 ± 2 |
| Gall bladder | 5 ± 5 | 5 ± 4 | 4 ± 3 | 0.3 ± 0.1 |
| Jejunum | 21 ± 9 | 25 ± 17 | 13 ± 10 | 3 ± 2 |
| Upper colon | 1.1 ± 0.6 | 6 ± 12 | 19 ± 17 | 15 ± 10 |
| Lower colon | 1.4 ± 0.8 | 1.0 ± 0.9 | 0.8 ± 0.7 | 20 ± 15 |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Nogueira, L.; Devasia, T.; Mariotto, A.B.; Yabroff, K.R.; Jemal, A.; Kramer, J.; Siegel, R.L. Cancer treatment and survivorship statistics. CA Cancer J Clin. 2022, 72, 409–436. [Google Scholar] [CrossRef] [PubMed]
- Von Eyben, F.E.; Picchio, M.; von Eyben, R.; Rhee, H.; Bauman, G. 68Ga-labeled prostate-specific membrane antigen ligand positron emission tomography/computed tomography for prostate cancer: A systematic review and meta-analysis. Eur. Urol. Focus 2018, 4, 686–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, A.; Han, J.; Nakano, A.; Konno, H.; Moriwaki, H.; Abe, H.; Izawa, K.; Soloshonok, V.A. New pharmaceuticals approved by FDA in 2020: Small-molecule drugs derived from amino acids and related compounds. Chirality 2022, 34, 86–103. [Google Scholar] [CrossRef]
- Keam, S.J. Piflufolastat F 18: Diagnostic first approval. Mol. Diagn. Ther. 2021, 25, 647–656. [Google Scholar] [CrossRef]
- Deandreis, D.; Guarneri, A.; Ceci, F.; Lillaz, B.; Bartoncini, S.; Oderda, M.; Nicolotti, D.G.; Pilati, E.; Passera, R.; Zitella, A.; et al. 68Ga-PSMA-11 PET/CT in recurrent hormone-sensitive prostate cancer (HSPCA): A prospective single-centre study in patients eligible for salvage therapy. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2804–2815. [Google Scholar] [CrossRef]
- Pienta, K.J.; Gorin, M.A.; Rowe, S.P.; Carroll, P.R.; Pouliot, F.; Probst, S.; Saperstein, L.; Preston, M.A.; Alva, A.S.; Patnaik, A.; et al. A phase 2/3 prospective multicenter study of the diagnostic accuracy of prostate specific membrane antigen PET/CT with 18F-DCFPyL in prostate cancer patients (OSPREY). J. Urol. 2021, 206, 52–61. [Google Scholar] [CrossRef]
- Ananias, H.J.; van den Heuvel, M.C.; Helfrich, W.; de Jong, I.J. Expression of the gastrin-releasing peptide receptor, the prostate stem cell antigen and the prostate-specific membrane antigen in lymph node and bone metastases of prostate cancer. Prostate 2009, 69, 1101–1108. [Google Scholar] [CrossRef]
- Markwalder, R.; Reubi, J.C. Gastrin-releasing peptide receptors in the human prostate: Relation to neoplastic transformation. Cancer Res. 1999, 59, 1152–1159. [Google Scholar]
- Beer, M.; Montani, M.; Gerhardt, J.; Wild, P.J.; Hany, T.F.; Hermanns, T.; Müntener, M.; Kristiansen, G. Profiling gastrin-releasing peptide receptor in prostate tissues: Clinical implications and molecular correlates. Prostate 2012, 72, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Cornelio, D.B.; Roesler, R.; Schwartsmann, G. Gastrin-releasing peptide receptor as a molecular target in experimental anticancer therapy. Ann. Oncol. 2007, 18, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Dalm, S.U.; Martens, J.W.; Sieuwerts, A.M.; van Deurzen, C.H.; Koelewijn, S.J.; de Blois, E.; Maina, T.; Nock, B.A.; Brunel, L.; Fehrentz, J.-A.; et al. In vitro and in vivo application of radiolabeled gastrin-releasing peptide receptor ligands in breast cancer. J. Nucl. Med. 2015, 56, 752–757. [Google Scholar] [CrossRef] [Green Version]
- Morgat, C.; MacGrogan, G.; Brouste, V.; Vélasco, V.; Sévenet, N.; Bonnefoi, H.; Fernandez, P.; Debled, M.; Hindié, E. Expression of gastrin-releasing peptide receptor in breast cancer and its association with pathologic, biologic and clinical parameters: A study of 1.432 primary tumors. J. Nucl. Med. 2017, 58, 1401–1407. [Google Scholar] [CrossRef]
- Ceci, F.; Castellucci, P.; Polverari, G.; Iagaru, A. Clinical application of Fluciclovine PET. choline PET and gastrin-releasing polypeptide receptor (bombesin) targeting PET in prostate cancer. Curr. Opin. Urol. 2020, 30, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Bodei, L.; Ferrari, M.; Nunn, A.; Llull, J.; Cremonesi, M.; Martano, L.; Laurora, G.; Scardino, E.; Tiberini, S.; Bufi, G.; et al. 177Lu-AMBA bombesin analogue in hormone refractory prostate cancer patients: A phase I escalation study with single-cycle administrations [abstract]. Eur. J. Nucl. Med. Mol. Imaging 2007, 34 (Suppl. S2), S221. [Google Scholar]
- Schally, A.V.; Comaru-Schally, A.M.; Nagy, A.; Kovacs, M.; Szepeshazi, K.; Plonowski, A.; Varga, J.L.; Halmos, G. Hypothalamic hormones and cancer. Front. Neuroendocrinol. 2001, 22, 248–291. [Google Scholar] [CrossRef]
- Millar, J.B.; Rozengurt, E. Chronic desensitization to bombesin by progressive down-regulation of bombesin receptors in Swiss 3T3 cells. Distinction from acute desensitization. J. Biol. Chem. 1990, 265, 12052–12058. [Google Scholar] [CrossRef]
- Schwartsmann, G.; DiLeone, L.P.; Horowitz, M.; Schunemann, D.; Cancella, A.; Pereira, A.S.; Richter, M.; Souza, F.; da Rocha, A.B.; Souza, F.H.; et al. A phase I trial of the bombesin/gastrin-releasing peptide (BN/GRP) antagonist RC3095 in patients with advanced solid malignancies. Invest. New Drugs 2006, 24, 403–412. [Google Scholar] [CrossRef]
- Mansi, R.; Nock, B.A.; Dalm, S.U.; Busstra, M.B.; van Weerden, W.M.; Maina, T. Radiolabeled bombesin analogs. Cancers 2021, 13, 5766. [Google Scholar] [CrossRef]
- Nock, B.A.; Kaloudi, A.; Kanellopoulos, P.; Janota, B.; Bromińska, B.; Iżycki, D.; Mikołajczak, R.; Czepczynski, R.; Maina, T. [99mTc]Tc-DB15 in GRPR-targeted tumor imaging with SPECT: From preclinical evaluation to the first clinical outcomes. Cancers 2021, 13, 5093. [Google Scholar] [CrossRef]
- Abouzayed, A.; Rinne, S.S.; Sabahnoo, H.; Sörensen, J.; Chernov, V.; Tolmachev, V.; Orlova, A. Preclinical evaluation of 99mTc-labeled GRPR antagonists maSSS/SES-PEG2-RM26 for imaging of prostate cancer. Pharmaceutics 2021, 13, 182. [Google Scholar] [CrossRef] [PubMed]
- Bragina, O.; Chernov, V.; Schulga, A.; Konovalova, E.; Garbukov, E.; Vorobyeva, A.; Orlova, A.; Tashireva, L.; Sörensen, J.; Zelchan, R.; et al. Phase I trial of 99mTc-(HE)3-G3. a DARPin-based probe for imaging of HER2 expression in breast cancer. J. Nucl. Med. 2022, 63, 528–535. [Google Scholar] [CrossRef]
- Bertacinni, G.; Impicciatore, M.; Molina, E.; Zappia, L. Action of bombesin on human gastrointestinal motility. Italian J. Gastroent. 1974, 6, 45–51. [Google Scholar]
- Stoykow, C.; Erbes, T.; Maecke, H.R.; Bulla, S.; Bartholomä, M.; Mayer, S.; Drendel, V.; Bronsert, P.; Werner, M.; Gitsch, G.; et al. Gastrin-releasing peptide receptor imaging in breast cancer using the receptor antagonist 68Ga-RM2 And PET. Theranostics 2016, 6, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Wieser, G.; Mansi, R.; Grosu, A.L.; Schultze-Seemann, W.; Dumont-Walter, R.A.; Meyer, P.T.; Maecke, H.R.; Reubi, J.C.; Weber, W.A. Positron emission tomography (PET) imaging of prostate cancer with a gastrin releasing peptide receptor antagonist—From mice to men. Theranostics 2014, 4, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Van de Wiele, C.; Dumont, F.; Dierckx, R.A.; Peers, S.H.; Thornback, J.R.; Slegers, G.; Thierens, H. Biodistribution and dosimetry of 99mTc-RP527. a gastrin-releasing peptide (GRP) agonist for the visualization of GRP receptor-expressing malignancies. J. Nucl. Med. 2001, 42, 1722–1727. [Google Scholar]
- Kähkönen, E.; Jambor, I.; Kemppainen, J.; Lehtiö, K.; Grönroos, T.J.; Kuisma, A.; Luoto, P.; Sipilä, H.J.; Tolvanen, T.; Alanen, K.; et al. In Vivo imaging of prostate cancer using [68Ga]-labeled bombesin analog BAY86-7548. Clin. Cancer Res. 2013, 19, 5434–5443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maina, T.; Bergsma, H.; Kulkarni, H.R.; Mueller, D.; Charalambidis, D.; Krenning, E.P.; Nock, B.A.; de Jong, M.; Baum, R.P. Preclinical and first clinical experience with the gastrin-releasing peptide receptor-antagonist [68Ga]SB3 and PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Kurth, J.; Krause, B.J.; Schwarzenböck, S.M.; Bergner, C.; Hakenberg, O.W.; Heuschkel, M. First-in-human dosimetry of gastrin-releasing peptide receptor antagonist [177Lu]Lu-RM2: A radiopharmaceutical for the treatment of metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 123–135. [Google Scholar] [CrossRef]
- Gruber, L.; Jiménez-Franco, L.D.; Decristoforo, C.; Uprimny, C.; Glatting, G.; Hohenberger, P.; Schoenberg, S.O.; Reindl, W.; Orlandi, F.; Mariani, M.; et al. MITIGATE-NeoBOMB1, a phase I/IIa study to evaluate safety, pharmacokinetics, and preliminary imaging of 68Ga-NeoBOMB1, a gastrin-releasing peptide receptor antagonist, in GIST patients. J. Nucl. Med. 2020, 61, 1749–1755. [Google Scholar] [CrossRef]
- Roivainen, A.; Kähkönen, E.; Luoto, P.; Borkowski, S.; Hofmann, B.; Jambor, I.; Lehtiö, K.; Rantala, T.; Rottmann, A.; Sipilä, H.; et al. Plasma pharmacokinetics, whole-body distribution, metabolism, and radiation dosimetry of 68Ga bombesin antagonist BAY 86-7548 in healthy men. J. Nucl. Med. 2013, 54, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Varasteh, Z.; Rosenström, U.; Velikyan, I.; Mitran, B.; Altai, M.; Honarvar, H.; Rosestedt, M.; Lindeberg, G.; Sörensen, J.; Larhed, M.; et al. The effect of mini-PEG-based spacer length on binding and pharmacokinetic properties of a 68Ga-labeled NOTA-conjugated antagonistic analog of bombesin. Molecules 2014, 19, 10455–10472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Niu, G.; Fan, X.; Lang, L.; Hou, G.; Chen, L.; Wu, H.; Zhu, Z.; Li, F.; Chen, X. PET using a GRPR antagonist 68Ga-RM26 in healthy volunteers and prostate cancer patients. J. Nucl. Med. 2018, 59, 922–928. [Google Scholar] [CrossRef] [Green Version]
- Kwee, S.A.; Wei, H.; Sesterhenn, I.; Yun, D.; Coel, M.N. Localization of primary prostate cancer with dual-phase 18F-fluorocholine PET. J. Nucl. Med. 2006, 47, 262–269. [Google Scholar] [PubMed]
- Mather, S.J.; Nock, B.A.; Maina, T.; Gibson, V.; Ellison, D.; Murray, I.; Sobnack, R.; Colebrook, S.; Wan, S.; Halberrt, C.; et al. GRP receptor imaging of prostate cancer using [99mTc]Demobesin 4: A first-in-man study. Mol. Imaging Biol. 2014, 16, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Bakker, I.L.; Fröberg, A.C.; Busstra, M.B.; Verzijlbergen, J.F.; Konijnenberg, M.; van Leenders, G.J.L.H.; Schoots, I.G.; de Blois, E.; van Weerden, W.M.; Dalm, S.U.; et al. GRPr antagonist 68Ga-SB3 PET/CT imaging of primary prostate cancer in therapy-naïve patients. J. Nucl. Med. 2021, 62, 1517–1523. [Google Scholar] [CrossRef]
- den Wyngaert, T.V.; Elvas, F.; De Schepper, S.; Kennedy, J.A.; Israel, O. SPECT/CT: Standing on the shoulders of giants. It is time to reach for the sky! J. Nucl. Med. 2020, 61, 1284–1291. [Google Scholar] [CrossRef]
- Kooij, P.P.M.; Kwekkeboom, D.J.; Breeman, W.A.P.; Reijs, A.E.M.; Bakker, W.H.; Lamberts, S.W.J.; Visser, T.J.; Krenning, E.P. The effects of specific activity on tissue distribution of [111In-DTPA-D-Phe1]octreotide in humans [abstract]. J. Nucl. Med. 1994, 35, 226P. [Google Scholar]
- Kwekkeboom, D.; Krenning, E.P.; de Jong, M. Peptide receptor imaging and therapy. J. Nucl. Med. 2000, 41, 1704–1713. [Google Scholar]
- Schuhmacher, J.; Zhang, H.; Doll, J.; Mäcke, H.R.; Matys, R.; Hauser, H.; Henze, M.; Haberkorn, U.; Eisenhut, M. GRP receptor-targeted PET of a rat pancreas carcinoma xenograft in nude mice with a 68Ga-labeled bombesin(6-14) analog. J. Nucl. Med. 2005, 46, 691–699. [Google Scholar]
- Varasteh, Z.; Velikyan, I.; Lindeberg, G.; Sörensen, J.; Larhed, M.; Sandström, M.; Selvaraju, R.K.; Malmberg, J.; Tolmachev, V.; Orlova, A. Synthesis and characterization of a high-affinity NOTA-conjugated bombesin antagonist for GRPR-targeted tumor imaging. Bioconjugate Chem. 2013, 24, 1144–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bragina, O.; von Witting, E.; Garousi, J.; Zelchan, R.; Sandström, M.; Orlova, A.; Medvedeva, A.; Doroshenko, A.; Vorobyeva, A.; Lindbo, S.; et al. Phase I study of 99mTc-ADAPT6, a scaffold protein-based probe for visualization of HER2 expression in breast cancer. J. Nucl. Med. 2021, 62, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Sörensen, J.; Velikyan, I.; Sandberg, D.; Wennborg, A.; Feldwisch, J.; Tolmachev, V.; Orlova, A.; Sandström, M.; Lubberink, M.; Olofsson, H.; et al. Measuring HER2-receptor expression in metastatic breast cancer using [68Ga]ABY-025 affibody PET/CT. Theranostics 2016, 6, 262–271. [Google Scholar] [CrossRef] [PubMed]






| Patient No | Age, y | Histotype PSA 1 | Clinical Stage | SUVmax (Lesion Size, cm) 2 | Ratio SUVmax in Tumor to Background | IHC GRPR Status 3 |
|---|---|---|---|---|---|---|
| P1 | 68 | PAA G2 GS 7 (3+4) PSA = 11.4 | T2N0M0 | 1.67 (1.6 × 2.5) | 7.3 | 2+ |
| P2 | 56 | PAA G2 GS 7 (3+4) PSA = 9 | T2aN0M0 | 0.78 (1.7 × 2) | 6.5 | 0 |
| P3 | 68 | PAA G5 GS 9 (4+5) PSA = 207.6 | T3aN0M0 | 1.21 (4.1 × 2.8) | 10.9 | No material |
| P4 | 65 | PAA G1 GS 6 (3+3) PSA = 9.25 | T1bN0M0 | 1.14 (1.8 × 2.0) | 4.2 | 1+ |
| P5 | 66 | PAA G1 GS 6 (3+3) PSA = 11 | T2N0M0 | No accumulation | 3+ | |
| P6 | 70 | PAA G2 GS 7 (4+3) PSA = 7.93 | T2aN0M0 | No accumulation | 0 | |
| Patient No | Age, y | Histotype 1 | Clinical Stage | SUVmax (Lesion Size. cm) 2 | Ratio SUVmax in Tumor to Background | IHC GRPR Status 3 | Pathologic Stage |
|---|---|---|---|---|---|---|---|
| B1 | 34 | IC NST G2 | T2N0M0 | T: 1.41 (2.8 × 2.2) | 2.2 | T: 3+ | T2N0M0 |
| B2 | 41 | IC NST G2 | T2N2M0 | T: 1.75 (3.8 × 2.2) LNM: 1.8 (1.3) | T: 35 LNM: 16.3 | T: 1+ LNM: 2+ | T2N3M0 |
| B3 | 40 | IC NST G2 | T2N0M0 | T: 0.87 (5.1 × 2.2) LNM: 1.8 (1.4) | T: 10.8 LNM: 7.1 | T: 0 LNM:1+ | T3N3M0 |
| B4 | 69 | ILC G1 | T2N0M0 | T: 0.57 (6.8 × 3.2) LNM: 0.58 (2.5) | T: 7.8 LNM: 6 | T: 1+ LNM: 1+ | T2N1M0 |
| B5 | 56 | IC NST G2 | T2N1M0 | T: 0.87 (4.0 × 1.7) LNM: 1.8 (2.3) | T: 14.5 LNM: 11.3 | T: 0 LNM: 0 | T2N1M0 |
| B6 | 50 | IC NST G1 | T1N0M0 | T: 0.43 (1.5 × 1.5) | T: 4.3 | T: 3+ | T1N0M0 |
| B7 | 62 | IC NST G2 | T1N0M0 | T: 0.50 (1.5 × 1.4) | T: 2.7 | T: 1+ | T1N0M0 |
| Organ | Males (n = 6) | Females (n = 7) |
|---|---|---|
| Adrenals | 0.005 ± 0.002 | 0.006 ± 0.001 |
| Brain | 0.0006 ± 0.0002 | 0.0005 ± 0.0002 |
| Breasts | 0.0006 ± 0.0002 | 0.0007 ± 0.0002 |
| Gallbladder wall | 0.011 ± 0.004 | 0.06 ± 0.03 1 |
| Lower large intestine wall | 0.008 ± 0.001 | 0.013 ± 0.007 |
| Small intestine | 0.014 ± 0.005 | 0.03 ± 0.02 |
| Stomach wall | 0.004 ± 0.001 | 0.005 ± 0.002 |
| Upper large intestine wall | 0.05 ± 0.02 | 0.04 ± 0.03 |
| Heart wall | 0.0021 ± 0.0006 | 0.0026 ± 0.0009 |
| Kidneys | 0.014 ± 0.007 | 0.012 ± 0.004 |
| Liver | 0.004 ± 0.001 | 0.0074 ± 0.0016 1 |
| Lungs | 0.0015 ± 0.0003 | 0.0018 ± 0.0005 |
| Muscle | 0.0018 ± 0.0006 | 0.0022 ± 0.0006 |
| Ovaries | N/A 2 | 0.018 ± 0.008 |
| Pancreas | 0.003 ± 0.001 | 0.0058 ± 0.0005 1 |
| Red marrow | 0.0026 ± 0.0009 | 0.0030 ± 0.0009 |
| Osteogenic cells | 0.005 ± 0.002 | 0.005 ± 0.001 |
| Skin | 0.0011 ± 0.0005 | 0.0010 ± 0.0003 |
| Spleen | 0.004 ± 0.002 | 0.005 ± 0.001 |
| Testes | 0.004 ± 0.005 | N/A |
| Thymus | 0.0017 ± 0.0005 | 0.0023 ± 0.0010 |
| Thyroid | 0.0014 ± 0.0005 | 0.0016 ± 0.0009 |
| Urinary bladder wall | 0.006 ± 0.004 | 0.008 ± 0.006 |
| Uterus | N/A | 0.020 ± 0.008 |
| Total body | 0.0026 ± 0.0009 | 0.0031 ± 0.0009 |
| Effective dose equivalent (mSv/MBq) | 0.009 ± 0.002 | 0.015 ± 0.003 1 |
| Effective dose (mSv/MBq) | 0.0053 ± 0.0007 | 0.008 ± 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chernov, V.; Rybina, A.; Zelchan, R.; Medvedeva, A.; Bragina, O.; Lushnikova, N.; Doroshenko, A.; Usynin, E.; Tashireva, L.; Vtorushin, S.; et al. Phase I Trial of [99mTc]Tc-maSSS-PEG2-RM26, a Bombesin Analogue Antagonistic to Gastrin-Releasing Peptide Receptors (GRPRs), for SPECT Imaging of GRPR Expression in Malignant Tumors. Cancers 2023, 15, 1631. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15061631
Chernov V, Rybina A, Zelchan R, Medvedeva A, Bragina O, Lushnikova N, Doroshenko A, Usynin E, Tashireva L, Vtorushin S, et al. Phase I Trial of [99mTc]Tc-maSSS-PEG2-RM26, a Bombesin Analogue Antagonistic to Gastrin-Releasing Peptide Receptors (GRPRs), for SPECT Imaging of GRPR Expression in Malignant Tumors. Cancers. 2023; 15(6):1631. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15061631
Chicago/Turabian StyleChernov, Vladimir, Anastasiya Rybina, Roman Zelchan, Anna Medvedeva, Olga Bragina, Nadejda Lushnikova, Artem Doroshenko, Evgeniy Usynin, Liubov Tashireva, Sergey Vtorushin, and et al. 2023. "Phase I Trial of [99mTc]Tc-maSSS-PEG2-RM26, a Bombesin Analogue Antagonistic to Gastrin-Releasing Peptide Receptors (GRPRs), for SPECT Imaging of GRPR Expression in Malignant Tumors" Cancers 15, no. 6: 1631. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15061631