
Autoimmune and Metabolic Diseases and the Risk of Early-Onset Colorectal Cancer, a Nationwide Nested Case–Control Study
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
Objectives
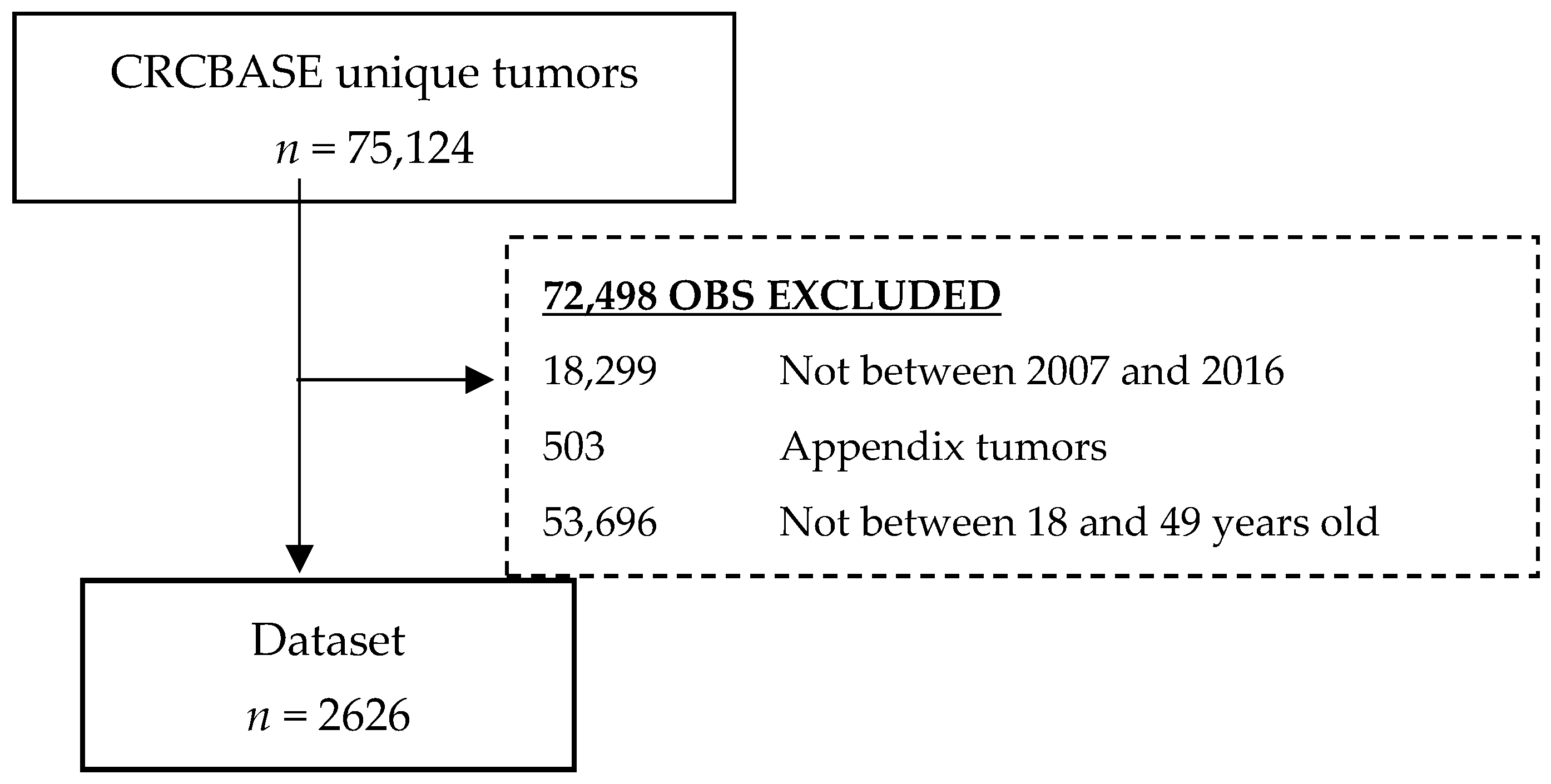
2. Materials and Methods
2.1. Data Source
2.2. Study Design
2.3. Exposure
2.4. Statistical Analyses
2.5. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Cancer i Siffror 2018: The National Board of Health and Welfare, The Swedish Cancer Society. 2021. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2018-6-10.pdf (accessed on 29 October 2022).
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahnen, D.J.; Wade, S.W.; Jones, W.F.; Sifri, R.; Mendoza Silveiras, J.; Greenamyer, J.; Spiegel, A.; You, Y.N. The increasing incidence of young-onset colorectal cancer: A call to action. Mayo Clin. Proc. 2014, 89, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Petersson, J.; Bock, D.; Martling, A.; Smedby, K.E.; Angenete, E.; Saraste, D. Increasing incidence of colorectal cancer among the younger population in Sweden. BJS Open 2020, 4, 645–658. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.E.; Hu, C.Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975-2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Saraste, D.; Järås, J.; Martling, A. Population-based analysis of outcomes with early-age colorectal cancer. Br. J. Surg. 2020, 107, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Vatandoust, S.; Price, T.J.; Ullah, S.; Roy, A.C.; Beeke, C.; Young, J.P.; Townsend, A.; Padbury, R.; Roder, D.; Karapetis, C.S. Metastatic Colorectal Cancer in Young Adults: A Study From the South Australian Population-Based Registry. Clin. Colorect. Cancer 2016, 15, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K.E. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef]
- Tjock-Och Ändtarmscancer, Nationellt Vårdprogram: Regional Cancer Centres (RCC). 2020. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/tjock-och-andtarmscancer/vardprogram/ (accessed on 29 October 2022).
- Thanikachalam, K.; Khan, G. Colorectal Cancer and Nutrition. Nutrients 2019, 11, 164. [Google Scholar] [CrossRef] [Green Version]
- Stoffel, E.M.; Murphy, C.C. Epidemiology and Mechanisms of the Increasing Incidence of Colon and Rectal Cancers in Young Adults. Gastroenterology 2020, 158, 341–353. [Google Scholar] [CrossRef]
- Moskal, A.; Freisling, H.; Byrnes, G.; Assi, N.; Fahey, M.T.; Jenab, M.; Ferrari, P.; Tjønneland, A.; Petersen, K.E.; Dahm, C.C.; et al. Main nutrient patterns and colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition study. Br. J. Cancer 2016, 115, 1430–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, K.H.; Kuo, C.F.; Huang, L.H.; Huang, W.K.; See, L.C. Cancer Risk in Patients With Inflammatory Systemic Autoimmune Rheumatic Diseases: A Nationwide Population-Based Dynamic Cohort Study in Taiwan. Medicine 2016, 95, e3540. [Google Scholar] [CrossRef] [PubMed]
- Dinse, G.E.; Parks, C.G.; Weinberg, C.R.; Co, C.A.; Wilkerson, J.; Zeldin, D.C.; Chan, E.K.; Miller, F.W. Increasing Prevalence of Antinuclear Antibodies in the United States. Arthritis Rheumatol. 2020, 72, 1026–1035. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.R. Prediction and Prevention of Autoimmune Disease in the 21st Century: A Review and Preview. Am. J. Epidemiol. 2016, 183, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Olén, O.; Erichsen, R.; Sachs, M.C.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Sørensen, H.T.; Ludvigsson, J.F. Colorectal cancer in Crohn’s disease: A Scandinavian population-based cohort study. Lancet Gastroenterol. Hepatol. 2020, 5, 475–484. [Google Scholar] [CrossRef]
- Olén, O.; Erichsen, R.; Sachs, M.C.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Sørensen, H.T.; Ludvigsson, J.F. Colorectal cancer in ulcerative colitis: A Scandinavian population-based cohort study. Lancet 2020, 395, 123–131. [Google Scholar] [CrossRef]
- Fu, Y.; Lee, C.H.; Chi, C.C. Association of psoriasis with colorectal cancer. J. Am. Acad. Dermatol. 2021, 85, 1429–1436. [Google Scholar] [CrossRef]
- Zendehdel, K.; Nyrén, O.; Ostenson, C.G.; Adami, H.O.; Ekbom, A.; Ye, W. Cancer incidence in patients with type 1 diabetes mellitus: A population-based cohort study in Sweden. J. Natl. Cancer Inst. 2003, 95, 1797–1800. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, T.M.; Andersen, N.H.; Torp-Pedersen, C.; Søgaard, P.; Kragholm, K.H. Kawasaki disease, autoimmune disorders, and cancer: A register-based study. Eur. J. Pediatr. 2021, 180, 717–723. [Google Scholar] [CrossRef]
- Gutiérrez-Salmerón, M.; Lucena, S.R.; Chocarro-Calvo, A.; García-Martínez, J.M.; Martín Orozco, R.M.; García-Jiménez, C. Remodelling of colorectal cancer cell signalling by microbiota and immunity in diabetes. Endocr. Relat. Cancer 2021, 28, R173–R190. [Google Scholar] [CrossRef]
- O’Sullivan, D.E.; Sutherland, R.L.; Town, S.; Chow, K.; Fan, J.; Forbes, N.; Heitman, S.J.; Hilsden, R.J.; Brenner, D.R. Risk Factors for Early-Onset Colorectal Cancer: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 1229–1240.e5. [Google Scholar] [CrossRef]
- Chen, H.; Zheng, X.; Zong, X.; Li, Z.; Li, N.; Hur, J.; Fritz, C.D.; Chapman, W., Jr.; Nickel, K.B.; Tipping, A.; et al. Metabolic syndrome, metabolic comorbid conditions and risk of early-onset colorectal cancer. Gut 2021, 70, 1147–1154. [Google Scholar] [CrossRef]
- Shaukat, A.; Kahi, C.J.; Burke, C.A.; Rabeneck, L.; Sauer, B.G.; Rex, D.K. ACG Clinical Guidelines: Colorectal Cancer Screening 2021. Am. J. Gastroenterol. 2021, 116, 458–479. [Google Scholar] [CrossRef] [PubMed]
- Shahrivar, M.; Weibull, C.E.; Ekström Smedby, K.; Glimelius, B.; Syk, I.; Matthiessen, P.; Nordenvall, C.; Martling, A. Low-dose aspirin use and colorectal cancer survival in 32,195 patients-A national cohort study. Cancer Med. 2022, 12, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Otterblad-Olausson, P.; Pettersson, B.U.; Ekbom, A. The Swedish personal identity number: Possibilities and pitfalls in healthcare and medical research. Eur. J. Epidemiol. 2009, 24, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Ludvigsson, J.F.; Svedberg, P.; Olén, O.; Bruze, G.; Neovius, M. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur. J. Epidemiol. 2019, 34, 423–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moberger, P.; Sköldberg, F.; Birgisson, H. Evaluation of the Swedish Colorectal Cancer Registry: An overview of completeness, timeliness, comparability and validity. Acta. Oncol. 2018, 57, 1611–1621. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Andersson, E.; Ekbom, A.; Feychting, M.; Kim, J.L.; Reuterwall, C.; Heurgren, M.; Olausson, P.O. External review and validation of the Swedish national inpatient register. BMC Public Health 2011, 11, 450. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004; Available online: https://apps.who.int/iris/handle/10665/42980 (accessed on 29 October 2022).
- Wettermark, B.; Hammar, N.; Fored, C.M.; Leimanis, A.; Otterblad Olausson, P.; Bergman, U.; Persson, I.; Sundström, A.; Westerholm, B.; Rosén, M. The new Swedish Prescribed Drug Register—Opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol. Drug Saf. 2007, 16, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Hofseth, L.J.; Hebert, J.R.; Chanda, A.; Chen, H.; Love, B.L.; Pena, M.M.; Murphy, E.A.; Sajish, M.; Sheth, A.; Buckhaults, P.J.; et al. Early-onset colorectal cancer: Initial clues and current views. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 352–364. [Google Scholar] [CrossRef]
- Danial, D.; Youssef, E.D.; Maryam, B.M.; Mohammad, A.; Moein, B.M.; Liliane, D. Risk Factors of Young-Onset Colorectal Cancer: Analysis of a Large Population-Based Registry. Can. J. Gastroenterol. Hepatol. 2022, 2022, 3582443. [Google Scholar] [CrossRef] [PubMed]
- Everhov Å., H.; Ludvigsson, J.F.; Järås, J.; Erichsen, R.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Sørensen, H.T.; Olén, O. Colorectal Cancer in Childhood-onset Inflammatory Bowel Disease: A Scandinavian Register-based Cohort Study, 1969–2017. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Syed, A.R.; Thakkar, P.; Horne, Z.D.; Abdul-Baki, H.; Kochhar, G.; Farah, K.; Thakkar, S. Old vs new: Risk factors predicting early onset colorectal cancer. World J. Gastrointest. Oncol. 2019, 11, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Wijnands, A.M.; de Jong, M.E.; Lutgens, M.; Hoentjen, F.; Elias, S.G.; Oldenburg, B. Prognostic Factors for Advanced Colorectal Neoplasia in Inflammatory Bowel Disease: Systematic Review and Meta-analysis. Gastroenterology 2021, 160, 1584–1598. [Google Scholar] [CrossRef]
- Li, H.; Boakye, D.; Chen, X.; Jansen, L.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Associations of Body Mass Index at Different Ages With Early-Onset Colorectal Cancer. Gastroenterology 2022, 162, 1088–1097.e3. [Google Scholar] [CrossRef]
- Rosato, V.; Bosetti, C.; Levi, F.; Polesel, J.; Zucchetto, A.; Negri, E.; La Vecchia, C. Risk factors for young-onset colorectal cancer. Cancer Causes Control. 2013, 24, 335–341. [Google Scholar] [CrossRef]
- Elangovan, A.; Skeans, J.; Landsman, M.; Ali, S.M.J.; Elangovan, A.G.; Kaelber, D.C.; Sandhu, D.S.; Cooper, G.S. Colorectal Cancer, Age, and Obesity-Related Comorbidities: A Large Database Study. Dig. Dis. Sci. 2021, 66, 3156–3163. [Google Scholar] [CrossRef]
- Schumacher, A.J.; Chen, Q.; Attaluri, V.; McLemore, E.C.; Chao, C.R. Metabolic Risk Factors Associated with Early-Onset Colorectal Adenocarcinoma: A Case-Control Study at Kaiser Permanente Southern California. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1792–1798. [Google Scholar] [CrossRef]
- Fung, B.M.; Lindor, K.D.; Tabibian, J.H. Cancer risk in primary sclerosing cholangitis: Epidemiology, prevention, and surveillance strategies. World J. Gastroenterol. 2019, 25, 659–671. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Leong, R.W. Primary sclerosing cholangitis as an independent risk factor for colorectal cancer in the context of inflammatory bowel disease: A review of the literature. World J. Gastroenterol. 2014, 20, 8783–8789. [Google Scholar]
- Wolf, A.M.D.; Fontham, E.T.H.; Church, T.R.; Flowers, C.R.; Guerra, C.E.; LaMonte, S.J.; Etzioni, R.; McKenna, M.T.; Oeffinger, K.C.; Shih, Y.C.T.; et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J. Clin. 2018, 68, 250–281. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics- | - | Controls | Patients | Total | |||
|---|---|---|---|---|---|---|---|
| (n = 15,756) | (n = 2626) | (n = 18,382) | |||||
| n | (%) | n | (%) | n | (%) | ||
| Age at CRC diagnosis (SCRCR), years (mean (SD)) | 42.5 | (5.9) | 42.5 | (5.9) | - | - | |
| Sex | |||||||
| Female | 7290 | (46.3) | 1215 | (46.3) | 8505 | (46.3) | |
| Male | 8466 | (53.7) | 1411 | (53.7) | 9877 | (53.7) | |
| Duration of education | |||||||
| >12 years | 6139 | (39.0) | 973 | (37.1) | 7112 | (38.7) | |
| 10–12 years | 7611 | (48.3) | 1331 | (50.7) | 8942 | (48.6) | |
| <9 years | 1855 | (11.8) | 298 | (11.3) | 2153 | (11.7) | |
| Missing | 151 | (1.0) | 24 | (0.9) | 175 | (9.5) | |
| Income group | |||||||
| Upper quartile | 3827 | (24.3) | 637 | (24.4) | 4464 | (24.3) | |
| Middle two quartiles | 7979 | (50.6) | 1339 | (51.0) | 9318 | (50.7) | |
| Lower quartile | 3863 | (24.5) | 641 | (24.3) | 4504 | (24.5) | |
| Missing | 87 | (0.6) | 9 | (0.3) | 96 | (0.5) | |
| Comorbid conditions | |||||||
| Metabolic disease | 4163 | (26.4) | 1017 | (38.7) | 5180 | (28.2) | |
| Diabetes mellitus type 2 | 770 | (4.9) | 189 | (7.2) | 959 | (5.2) | |
| Primary hypertension | 3484 | (22.1) | 854 | (32.5) | 4338 | (23.6) | |
| Hyperlipidemia | 1426 | (9.1) | 281 | (10.7) | 1707 | (9.3) | |
| Obesity | 233 | (1.5) | 41 | (1.6) | 274 | (1.5) | |
| Fatty liver | <10 | - | <10 | - | 10 | (0.1) | |
| Autoimmune disease | 956 | (6.1) | 290 | (11.0) | 1246 | (6.8) | |
| IBD | 169 | (1.1) | 158 | (6.0) | 327 | (1.8) | |
| Crohn’s disease | 49 | (0.3) | 32 | (1.2) | 81 | (0.4) | |
| Ulcerative colitis | 61 | (0.4) | 74 | (2.8) | 135 | (0.7) | |
| IBD-unclassified | 59 | (0.4) | 52 | (2.0) | 111 | (0.6) | |
| PSC | 7 | - | 27 | (1.0) | 34 | (0.2) | |
| Autoimmune diseases ** | 956 | (6.1) | 290 | (11.0) | 1246 | (6.8) | |
| Diseases of the blood and blood-forming organs | 41 | (0.3) | 8 | (0.3) | 49 | (0.3) | |
| Endocrine diseases | 348 | (2.2) | 73 | (2.8) | 421 | (2.3) | |
| Diseases of the nervous system | 51 | (0.3) | 9 | (0.3) | 60 | (0.3) | |
| Diseases of the eye | 68 | (0.4) | 12 | (0.5) | 80 | (0.4) | |
| Circulatory disease | <10 | - | <10 | - | <10 | - | |
| Diseases of the digestive system, excluding IBD | 28 | (0.2) | 14 | (0.5) | 42 | (0.2) | |
| Diseases of the skin | 151 | (1.1) | 21 | (0.8) | 172 | (0.9) | |
| Diseases of the musculoskeletal system and connective tissue | 178 | (0.2) | 29 | (1.1) | 207 | (1.1) | |
| Diseases of the genitourinary system | 29 | (0.2) | 7 | (0.3) | 36 | (0.2) | |
| No Comorbid Conditions (n = 1465) n (%) | Autoimmune Disease without IBD or Metabolic (n = 47) n (%) | Metabolic Disease without IBD (n = 956) n (%) | IBD without Metabolic Disease (n = 97) n (%) | IBD with Metabolic Disease (n = 61) n (%) | Total (n = 2626) n (%) | |
|---|---|---|---|---|---|---|
| Age | ||||||
| Median, years [min, max] | 43.0 (19.0, 49.0) | 44.0 (27.0, 49.0) | 45.0 (21.0, 49.0) | 38.0 (21.0, 49.0) | 42.0 (30.0, 49.0) | 44.0 (19.0, 49.0) |
| Weight | ||||||
| Mean, kg (SD) | 75.1 (16.1) | 79.3 (17.2) | 81.9 (18.3) | 74.4 (14.6) | 91.3 (22.0) | 77.9 (17.5) |
| Missing | 275 (18.8) | 9 (19.1) | 221 (23.1) | 14 (14.4) | 8 (13.1) | 527 (20.1) |
| Height | ||||||
| Mean, cm (SD) | 174 (9.8) | 175 (11.6) | 174 (9.8) | 176 (7.4) | 177 (8.2) | 174 (9.7) |
| Missing | 304 (20.8) | 9 (19.1) | 243 (25.4) | 17 (17.5) | 9 (14.8) | 582 (22.2) |
| BMI | ||||||
| Mean, kg/m2 (SD) | 24.8 (4.3) | 25.9 (4.5) | 27.1 (5.2) | 24.0 (4.1) | 29.0 (7.0) | 25.7 (4.9) |
| Missing | 309 (21.1) | 9 (19.1) | 245 (25.6) | 17 (17.5) | 9 (14.8) | 589 (22.4) |
| Sex | ||||||
| Male | 763 (52.1) | 21 (44.7) | 508 (53.1) | 73 (75.3) | 46 (75.4) | 1411 (53.7) |
| Female | 702 (47.9) | 26 (55.3) | 448 (46.9) | 24 (24.7) | 15 (24.6) | 1215 (46.3) |
| Duration of education | ||||||
| <9 years | 150 (10.2) | 2 (4.3) | 126 (13.2) | 14 (14.4) | 6 (9.8) | 298 (11.3) |
| 10–12 years | 717 (48.9) | 26 (55.3) | 512 (53.6) | 46 (47.4) | 30 (49.2) | 1331 (50.7) |
| 12> years | 589 (40.2) | 19 (40.4) | 304 (31.8) | 36 (37.1) | 25 (41.0) | 973 (37.1) |
| Missing | 9 (0.6) | - | 14 (1.5) | 1 (1.0) | - | 24 (0.9) |
| Income group | ||||||
| Lower quartile | 352 (24.0) | 13 (27.7) | 223 (23.3) | 35 (36.1) | 18 (29.5) | 641 (24.4) |
| Middle two quartiles | 744 (50.8) | 21 (44.7) | 498 (52.1) | 41 (42.3) | 35 (57.4) | 1339 (51.0) |
| Upper quartile | 362 (24.7) | 13 (27.7) | 234 (24.5) | 21 (21.6) | 7 (11.5) | 637 (24.3) |
| Missing | 7 (0.5) | - | 1 (0.1) | - | 1 (1.6) | 9 (0.3) |
| ASA Class | ||||||
| 1 | 729 (49.8) | 13 (27.7) | 314 (32.8) | 21 (21.6) | 9 (14.8) | 1086 (41.4) |
| 2 | 443 (30.2) | 22 (46.8) | 371 (38.8) | 56 (57.7) | 28 (45.9) | 920 (35.0) |
| 3 | 71 (4.8) | 4 (8.5) | 95 (9.9) | 7 (7.2) | 16 (26.2) | 193 (7.3) |
| 4 | 8 (0.5) | - | <5 | <5 | - | 12 (0.5) |
| Missing | 214 (14.6) | 8 (17.0) | 173 (18.1) | 12 (12.4) | 8 (13.1) | 415 (15.8) |
| Cancer location | ||||||
| Right-side colon cancer | 402 (27.4) | 14 (29.8) | 251 (26.3) | 37 (38.1) | 31 (50.8) | 735 (28.0) |
| Left-side colon cancer | 490 (33.4) | 18 (38.3) | 327 (34.2) | 28 (28.9) | 17 (27.9) | 880 (33.5) |
| Rectal cancer | 569 (38.8) | 15 (31.9) | 372 (38.9) | 32 (33.0) | 12 (19.7) | 1000 (38.1) |
| Missing | 4 (0.3) | - | 6 (0.6) | - | 1 (1.6) | 11 (0.4) |
| Tumor stage | ||||||
| I | 220 (15.0) | 9 (19.1) | 117 (12.3) | 17 (17.5) | 10 (16.4) | 373 (14.2) |
| II | 334 (22.8) | 13 (27.7) | 170 (17.8) | 15 (15.5) | 17 (27.9) | 549 (20.9) |
| III | 442 (30.2) | 12 (25.5) | 273 (28.6) | 36 (37.1) | 19 (31.1) | 782 (29.8) |
| IV | 428 (29.2) | 10 (21.3) | 360 (37.7) | 25 (25.8) | 12 (19.7) | 835 (31.8) |
| Missing | 41 (2.8) | 3 (6.4) | 36 (3.8) | 4 (4.1) | 3 (4.9) | 87 (3.3) |
| Metabolic disease | ||||||
| Type 2 diabetes | - | - | 178 (18.6) | - | 11 (18.0) | 189 (7.2) |
| Hypertension | - | - | 807 (84.4) | - | 47 (77.0) | 854 (32.5) |
| Lipidemia | - | - | 254 (26.6) | - | 27 (44.3) | 281 (10.7) |
| Obesity | - | - | 35 (3.7) | - | 6 (9.8) | 11 (0.4) |
| Fatty liver | - | - | <5 | - | <5 | <5 |
| Two or more of the above | - | - | 238 (24.9) | - | 19 (31.1) | 257 (9.8) |
| IBD condition | ||||||
| Ulcerative colitis | - | - | - | 46 (47.4) | 28 (45.9) | 74 (2.8) |
| Crohn’s disease | - | - | - | 19 (19.6) | 13 (21.3) | 32 (1.2) |
| IBD-unclassified | - | - | - | 32 (33.0) | 20 (32.8) | 52 (2.0) |
| Comparison | Cases (Yes/No) | Controls (Yes/No) | Main Effect Model HR (95% CI) | Interaction Model HR (95% CI) |
|---|---|---|---|---|
| Non-IBD autoimmune disease | 172/2454 | 816/14,940 | 1.28 (1.08–1.52) | 0.97 (0.81–1.16) |
| Metabolic disease | 1017/1609 | 4163/11,593 | 1.82 (1.67–1.99) | - |
| without IBD | 956/1512 | 4092/11,495 | - | 1.82 (1.66–2.00) |
| IBD | 158/2468 | 169/15,587 | 5.98 (4.78–7.48) | - |
| with metabolic disease | 61 | 71 | - | 3.65 (2.57–5.19) |
| without metabolic disease | 97 | 98 | - | 7.52 (5.62–10.06) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lundqvist, E.; Myrberg, I.H.; Boman, S.E.; Saraste, D.; Weibull, C.E.; Landerholm, K.; Haapaniemi, S.; Martling, A.; Myrelid, P.; Nordenvall, C. Autoimmune and Metabolic Diseases and the Risk of Early-Onset Colorectal Cancer, a Nationwide Nested Case–Control Study. Cancers 2023, 15, 688. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030688
Lundqvist E, Myrberg IH, Boman SE, Saraste D, Weibull CE, Landerholm K, Haapaniemi S, Martling A, Myrelid P, Nordenvall C. Autoimmune and Metabolic Diseases and the Risk of Early-Onset Colorectal Cancer, a Nationwide Nested Case–Control Study. Cancers. 2023; 15(3):688. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030688
Chicago/Turabian StyleLundqvist, Erik, Ida Hed Myrberg, Sol Erika Boman, Deborah Saraste, Caroline E. Weibull, Kalle Landerholm, Staffan Haapaniemi, Anna Martling, Pär Myrelid, and Caroline Nordenvall. 2023. "Autoimmune and Metabolic Diseases and the Risk of Early-Onset Colorectal Cancer, a Nationwide Nested Case–Control Study" Cancers 15, no. 3: 688. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030688