
Early Onset Colorectal Cancer in Arabs, Are We Dealing with a Distinct Disease?
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Material and Methods
2.2. Samples
2.3. Definitions
3. Results
3.1. Demographics
3.2. Disease Stage and the Anatomical Location at Diagnosis
3.3. Tumor Location and Histopathology
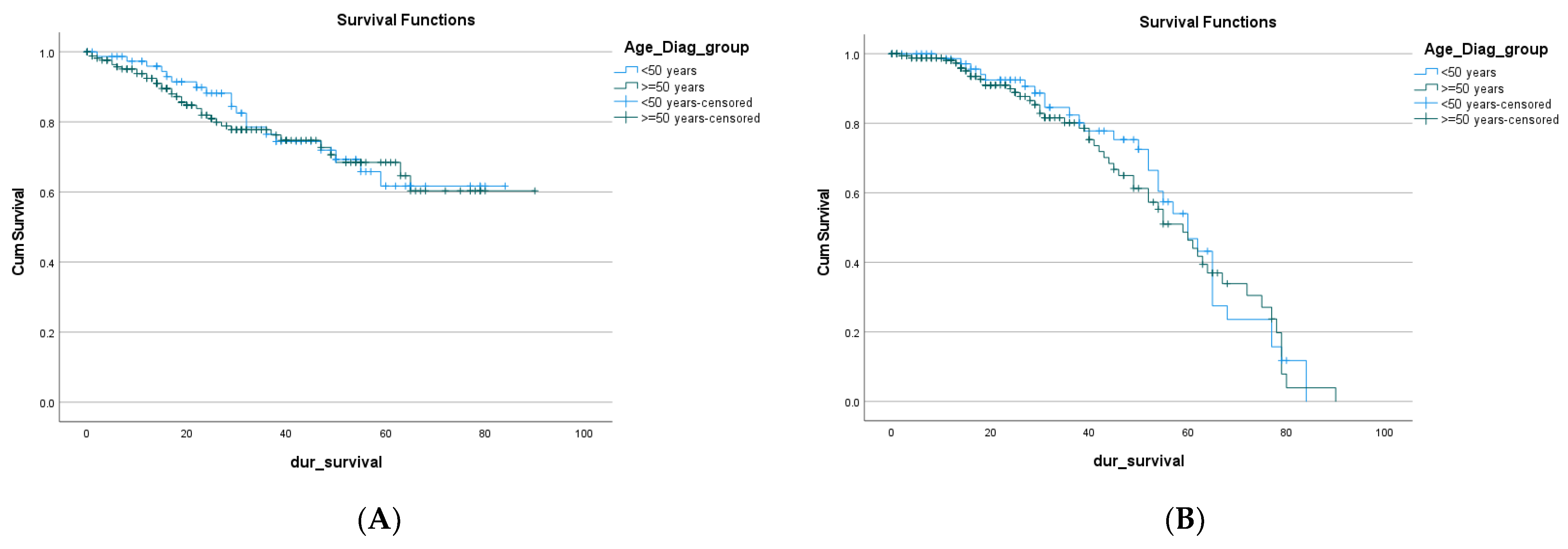
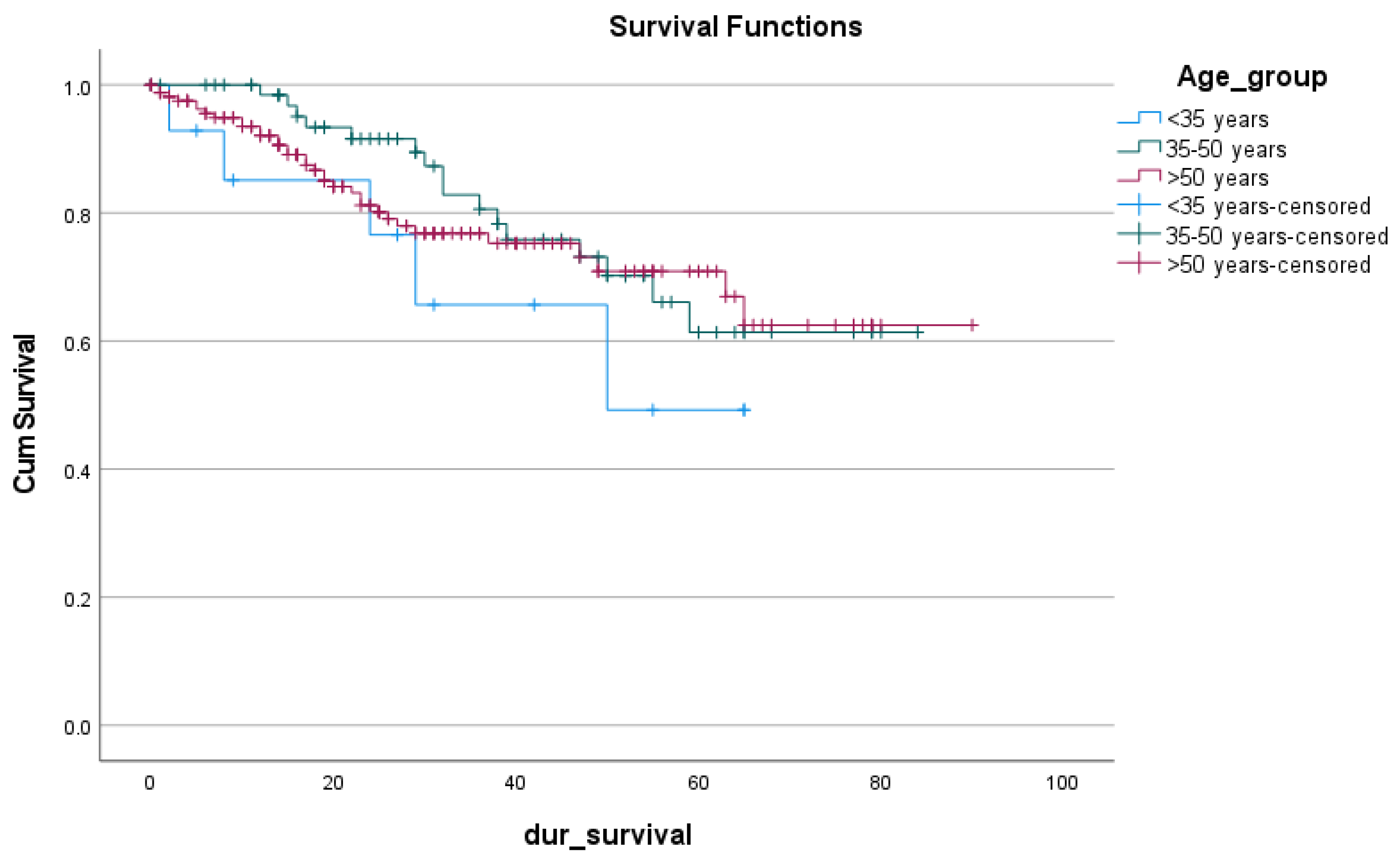
3.4. Remission and Survival
3.5. Subcategories of EOCRC
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frostberg, E.; Rahr, H.B. Clinical characteristics and a rising incidence of early-onset colorectal cancer in a nationwide cohort of 521 patients aged 18–40 years. Cancer Epidemiol. 2020, 66, 101704. [Google Scholar] [CrossRef] [PubMed]
- Troeung, L.; Sodhi-Berry, N.; Martini, A.; Malacova, E.; Ee, H.; O’Leary, P.; Lansdorp-Vogelaar, I.; Preen, D.B. Increasing Incidence of Colorectal Cancer in Adolescents and Young Adults Aged 15–39 Years in Western Australia 1982–2007: Examination of Colonoscopy History. Front. Public Health 2017, 5, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhandari, A.; Woodhouse, M.; Gupta, S. Colorectal cancer is a leading cause of cancer incidence and mortality among adults younger than 50 years in the USA: A SEER-based analysis with comparison to other young-onset cancers. J. Investig. Med. 2017, 65, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuik, F.E.R.; Nieuwenburg, S.A.V.; Bardou, M.; Lansdorp-Vogelaar, I.; Dinis-Ribeiro, M.; Bento, M.J.; Zadnik, V.; Pellisé, M.; Esteban, L.; Kaminski, M.; et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut 2019, 68, 1820–1826. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.E.; Narang, T.; Schnoll-Sussman, F.H.; Pochapin, M.B.; Christos, P.J.; Sherr, D.L. Increasing incidence of rectal cancer in patients aged younger than 40 years: An analysis of the surveillance, epidemiology, and end results database. Cancer 2010, 116, 4354–4359. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Sauer, A.G.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109, djw322. [Google Scholar] [CrossRef] [Green Version]
- Dozois, E.J.; Boardman, L.A.; Suwanthanma, W.; Limburg, P.J.; Cima, R.R.; Bakken, J.L.; Vierkant, R.A.; Aakre, J.A.; Larson, D.W. Young-onset colorectal cancer in patients with no known genetic predisposition: Can we increase early recognition and improve outcome? Medicine 2008, 87, 259–263. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Jemal, A.; Ward, E.M. Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1695–1698. [Google Scholar] [CrossRef] [Green Version]
- Abualkhair, W.H.; Zhou, M.; Ahnen, D.; Yu, Q.; Wu, X.-C.; Karlitz, J.J. Trends in Incidence of Early-Onset Colorectal Cancer in the United States Among Those Approaching Screening Age. JAMA Netw. Open 2020, 3, e1920407. [Google Scholar] [CrossRef]
- Nancy You, Y.; Xing, Y.; Feig, B.W.; Chang, G.J.; Cormier, J.N. Young-onset colorectal cancer: Is it time to pay attention? Arch. Intern. Med. 2012, 172, 287–289. [Google Scholar] [CrossRef]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.G.; Marsoni, S.; Bardelli, A.; Siena, S. Early-onset colorectal cancer in young individuals. Mol. Oncol. 2019, 13, 109–131. [Google Scholar] [CrossRef] [Green Version]
- Welch, H.G.; Robertson, D.J. Colorectal Cancer on the Decline—Why Screening Can’t Explain It All. N. Engl. J. Med. 2016, 374, 1605–1607. [Google Scholar] [CrossRef]
- Kumar, S.; Burney, I.A.; Zahid, K.F.; Souza, P.C.D.; AL Belushi, M.; Mufti, T.D.; AL Meki, W.; Furrukh, M.; AL Moundhri, M.S. Colorectal cancer patient characteristics, treatment and survival in Oman—A single center study. Asian Pac. J. Cancer Prev. 2015, 16, 4853–4858. [Google Scholar] [CrossRef] [Green Version]
- Al-Shamsi, H.O.; Abdullah Alzaabi, A.; Hassan, A.; Abu-Gheida, I.; Alrawi, S. Early Onset Colorectal Cancer in the United Arab Emirates, Where do we Stand? Acta Sci. Cancer Biol. 2020, 4, 24–27. [Google Scholar] [CrossRef]
- Nikbakht, H.A.; Hassanipour, S.; Shojaie, L.; Vali, M.; Ghaffari-Fam, S.; Ghelichi-Ghojogh, M.; Maleki, Z.; Arab-Zozani, M.; Abdzadeh, E.; Delam, H.; et al. Survival Rate of Colorectal Cancer in Eastern Mediterranean Region Countries: A Systematic Review and Meta-Analysis. Cancer Control. 2020, 27. [Google Scholar] [CrossRef]
- Amin, T.T.; Suleman, W.; Al Taissan, A.A.; Al Joher, A.L.; Al Mulhim, O.; Al Yousef, A.H. Patients’ profile, clinical presentations and histopathological features of colo-rectal cancer in Al Hassa region, Saudi Arabia. Asian Pac. J. Cancer Prev. 2012, 13, 211–216. [Google Scholar] [CrossRef] [Green Version]
- Al-Lawati, J.; Al-Zakwani, I.; Fadhil, I.; Al-Bahrani, B. Cancer Incidence in Oman. Oman Med. J. 2019, 34, 271. [Google Scholar] [CrossRef]
- Cercek, A.; Chatila, W.K.; Yaeger, R.; Walch, H.; Fernandes, G.D.S.; Krishnan, A.; Palmaira, L.; Maio, A.; Kemel, Y.; Srinivasan, P.; et al. A Comprehensive Comparison of Early-Onset and Average-Onset Colorectal Cancers. JNCI J. Natl. Cancer Inst. 2021, 113, 1683–1692. [Google Scholar] [CrossRef]
- Ahnen, D.J.; Wade, S.W.; Jones, W.F.; Sifri, R.; Silveiras, J.M.; Greenamyer, J.; Guiffre, S.; Axilbund, J.; Spiegel, A.; You, Y.N. The increasing incidence of young-onset colorectal cancer: A call to action. Mayo. Clin. Proc. 2014, 89, 216–224. [Google Scholar] [CrossRef]
- Yeo, S.A.; Chew, M.H.; Koh, P.K.; Tang, C.L. Young colorectal carcinoma patients do not have a poorer prognosis: A comparative review of 2426 cases. Tech. Coloproctol. 2013, 17, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Abualkhair, W.H.; Zhou, M.; Ochoa, C.O.; Lacayo, L.; Murphy, C.; Wu, X.; Karlitz, J.J. Geographic and intra-racial disparities in early-onset colorectal cancer in the SEER 18 registries of the United States. Cancer Med. 2020, 9, 9150–9159. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.D.; Ferrari, A.; Ries, L.; Whelan, J.; Bleyer, W.A. Cancer in adolescents and young adults: A narrative review of the current status and a view of the future. JAMA Pediatr. 2016, 170, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.E.; Hu, C.Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Abou-Zeid, A.A.; Jumuah, W.A.; Ebied, E.F.; Abd El Samee Atia, K.S.; El Ghamrini, Y.; Somaie, D.A. Hereditary factors are unlikely behind unusual pattern of early—Onset colorectal cancer in Egyptians: A study of family history and pathology features in Egyptians with large bowel cancer (cross-sectional study). Int. J. Surg. 2017, 44, 71–75. [Google Scholar] [CrossRef]
- Alyabsi, M.; Algarni, M.; Alshammari, K. Trends in Colorectal Cancer Incidence Rates in Saudi Arabia (2001–2016) Using Saudi National Registry: Early- Versus Late-Onset Disease. Front. Oncol. 2021, 11, 730689. [Google Scholar] [CrossRef]
- Glover, M.; Mansoor, E.; Panhwar, M.; Parasa, S.; Cooper, G.S. Epidemiology of Colorectal Cancer in Average Risk Adults 20–39 Years of Age: A Population-Based National Study. Dig. Dis. Sci. 2019, 64, 3602–3609. [Google Scholar] [CrossRef]
- Myers, E.A.; Feingold, D.L.; Forde, K.A.; Arnell, T.; Jang, J.H.; Whelan, R.L. Colorectal cancer in patients under 50 years of age: A retrospective analysis of two institutions’ experience. World J. Gastroenterol. 2013, 19, 5651–5657. [Google Scholar] [CrossRef]
- Surveillance Epidemiology. Colorectal Cancer—Cancer Stat. Facts. 2019. Available online: https://seer.cancer.gov/statfacts/html/colorect.html (accessed on 23 April 2022).
- Patel, S.G.; Ahnen, D.J. Colorectal Cancer in the Young. Curr. Gastroenterol. Rep. 2018, 20, 15. [Google Scholar] [CrossRef]
- Fu, J.; Yang, J.; Tan, Y.; Jiang, M.; Wen, F.; Huang, Y.; Chen, H.; Yi, C.; Zheng, S.; Yuan, Y. Young patients (≤35 years old) with colorectal cancer have worse outcomes due to more advanced disease: A 30-Year Retrospective Review. Medicine 2014, 93, e135. [Google Scholar] [CrossRef]
- Yantiss, R.K.; Goodarzi, M.; Zhou, X.K.; Rennert, H.; Pirog, E.C.; Banner, B.F.; Chen, Y.-T. Clinical, pathologic, and molecular features of early-onset colorectal carcinoma. Am. J. Surg. Pathol. 2009, 33, 572–582. [Google Scholar] [CrossRef]
- Kirzin, S.; Marisa, L.; Guimbaud, R.; De Reynies, A.; Legrain, M.; Laurent-Puig, P.; Cordelier, P.; Pradère, B.; Bonnet, D.; Meggetto, F.; et al. Sporadic early onset colorectal cancer is a specific sub-type of cancer: A morphological, molecular and genetics study. PloS ONE 2014, 9, e103159. [Google Scholar] [CrossRef] [Green Version]
- Al-Shamsi, H.O.; Abu-Gheida, I.H.; Iqbal, F.; Al-Awadhi, A. Cancer in the Arab World; Springer Nature: The Hague, The Netherlands, 2022; p. 476. [Google Scholar]
- AlZaabi, A.; AlHarrasi, A.; AlMusalami, A.; AlMahyijari, N.; Al Hinai, K.; ALAdawi, H.; Al-Shamsi, H.O. Early onset colorectal cancer: Challenges across the cancer care continuum. Ann. Med. Surg. 2022, 82, 104453. [Google Scholar] [CrossRef]
- Kneuertz, P.J.; Chang, G.J.; Hu, C.Y.; Rodriguez-Bigas, M.A.; Eng, C.; Vilar, E.; Skibber, J.M.; Feig, B.W.; Cormier, J.N.; You, Y.N. Overtreatment of young adults with colon cancer: More intense treatments with unmatched survival gains. JAMA Surg. 2015, 150, 402–409. [Google Scholar] [CrossRef]
- Manjelievskaia, J.; Brown, D.; McGlynn, K.A.; Anderson, W.; Shriver, C.D.; Zhu, K. Chemotherapy use and survival among young and middle-aged patients with colon cancer. JAMA Surg. 2017, 152, 452–459. [Google Scholar] [CrossRef]
- Khan, S.A.; Morris, M.; Idrees, K.; Gimbel, M.I.; Rosenberg, S.; Zeng, Z.; Li, F.; Gan, G.; Shia, J.; LaQuaglia, M.P.; et al. Colorectal cancer in the very young: A comparative study of tumor markers, pathology and survival in early onset and adult onset patients. J. Pediatr. Surg. 2016, 51, 1812–1817. [Google Scholar] [CrossRef] [Green Version]
- Sultan, I.; Rodriguez-Galindo, C.; El-Taani, H.; Pastore, G.; Casanova, M.; Gallino, G.; Ferrari, A. Distinct features of colorectal cancer in children and adolescents: A population-based study of 159 cases. Cancer 2010, 116, 758–765. [Google Scholar] [CrossRef]
- O’Connell, J.B.; Maggard, M.A.; Liu, J.H.; Etzioni, D.A.; Livingston, E.H.; Ko, C. Rates of colon and rectal cancers are increasing in young adults. Am. Surg. 2003, 69, 866–872. [Google Scholar] [CrossRef]
- Chang, D.T.; Pai, R.K.; Rybicki, L.A.; Dimaio, M.; Limaye, M.; Jayachandran, P.; Koong, A.C.; A Kunz, P.; A Fisher, G.; Ford, J.M.; et al. Clinicopathologic and molecular features of sporadic early-onset colorectal adenocarcinoma: An adenocarcinoma with frequent signet ring cell differentiation, rectal and sigmoid involvement, and adverse morphologic features. Mod. Pathol. 2012, 25, 1128–1139. [Google Scholar] [CrossRef] [Green Version]
- Silla, I.O.; Rueda, D.; Rodríguez, Y.; García, J.L.; De La Cruz Vigo, F.; Perea, J. Early-onset colorectal cancer: A separate subset of colorectal cancer. World J. Gastroenterol. 2014, 20, 17288–17296. [Google Scholar] [CrossRef]
- Gandhi, J.; Davidson, C.; Hall, C.; Pearson, J.; Eglinton, T.; Wakeman, C.; Frizelle, F. Population-based study demonstrating an increase in colorectal cancer in young patients. Br. J. Surg. 2017, 104, 1063–1068. [Google Scholar] [CrossRef] [PubMed]
- Exarchakou, A.; Donaldson, L.; Coleman, M.P. Increasing colorectal cancer incidence among young adults in England diagnosed during 2001–2014. Ann. Oncol. 2018, 29, viii562–viii563. [Google Scholar] [CrossRef]
- Hessami Arani, S.; Kerachian, M.A. Rising rates of colorectal cancer among younger iranians: Is diet to blame? Curr. Oncol. 2017, 24, e131–e137. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.R.; Ruan, Y.; Shaw, E.; De, P.; Heitman, S.J.; Hilsden, R.J. Increasing colorectal cancer incidence trends among younger adults in Canada. Prev. Med. 2017, 105, 345–349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Year of Diagnosis | Number of Patients Diagnosed with CRC per Year | EOCRC < 50 Years | LOCRC ≥ 50 Years Old | Percentage of EOCRC Diagnosed per Year (%) |
|---|---|---|---|---|
| 2015 | 39 | 14 | 25 | 36 |
| 2016 | 43 | 16 | 27 | 37 |
| 2017 | 45 | 13 | 32 | 29 |
| 2018 | 44 | 15 | 29 | 34 |
| 2019 | 41 | 11 | 30 | 27 |
| 2020 | 42 | 10 | 32 | 24 |
| Total | 254 | 79 | 175 | 31 |
| Variables | Diagnosis Age | p-Value | ||
|---|---|---|---|---|
| <50 Years n (%) | ≥50 Years n (%) | |||
| Gender (CRC) | Male | 40 (50.6) | 98 (56.3) | 0.417 |
| Female | 39 (49.4) | 77 (43.7) | ||
| Gender (Rectal cancer) | Male | 21 (58) | 46 (62) | 0.065 |
| Female | 15 (42) | 28 (38) | ||
| Family History | No | 53 (67.9 | 119 (68.4) | 0.707 |
| Yes | 12 (15.4) | 21 (12.1) | ||
| Unknown | 13 (167) | 34 (19.5) | ||
| BMI | Missing | 45 (57.0) | 117 (67.2) | 0.271 |
| <20 | 5 (6.3) | 7 (4.0) | ||
| ≥20 | 29 (36.7) | 50 (28.7) | ||
| DM | Absent | 66 (83.5) | 116 (66.7) | 0.011 |
| Present | 13 (16.5) | 57 (32.2) | ||
| Not mentioned | - | 2 (1.1) | ||
| HTN | Absent | 70 (88.6) | 103 (59.2) | <0.001 |
| Present | 8 (10.1) | 68 (39.1) | ||
| Not mentioned | 1 (1.3) | 3 (1.7) | ||
| Heart disease | Absent | 76 (97.4) | 142 (82.6) | 0.001 |
| Present | 2 (2.6) | 27 (15.7) | ||
| Not mentioned | - | 3 (1.7) | ||
| Medication | Metformin | 0.055 | ||
| Not given | 69 (87.3) | 132 (76.3) | ||
| Given | 10 (12.7) | 33 (19.1) | ||
| Not mentioned | - | 8 (4.6) | ||
| Aspirin | <0.001 | |||
| Not given | 76 (96.2) | 145 (83.3) | ||
| Given | - | 16 (9.2) | ||
| Not mentioned | 3 (3.8) | 13 (7.5) | ||
| (A) Colorectal cancer | Stage | Overall Stage of CRC | Stage of EOCRC | Stage of LOCRC | p Value | |||
| n | % | n | % | n | % | 0.158 | ||
| in situ | 1 | 0 | 1 | 1 | 0 | 0 | ||
| Stage 1 | 10 | 4 | 6 | 8 | 4 | 2 | ||
| Stage 2 | 55 | 22 | 15 | 19 | 40 | 23 | ||
| Stage 3 | 49 | 19 | 12 | 15 | 37 | 21 | ||
| Stage 4 | 112 | 44 | 38 | 48 | 74 | 42 | ||
| unknown | 27 | 11 | 7 | 9 | 20 | 11 | ||
| Total | 254 | 100 | 79 | 100 | 175 | 100 | ||
| (B) Rectal cancer | Stage | Overall stage of rectal cancer | EOCRC | LOCRC | p value | |||
| n | % | n | % | n | % | 0.080 | ||
| in situ | 0 | 0 | 0 | 0 | 0 | 0 | ||
| Stage 1 | 5 | 5 | 4 | 11 | 1 | 1 | ||
| Stage 2 | 17 | 15 | 5 | 14 | 12 | 16 | ||
| Stage 3 | 24 | 22 | 5 | 14 | 19 | 26 | ||
| Stage 4 | 52 | 47 | 20 | 56 | 32 | 43 | ||
| unknown | 12 | 11 | 2 | 6 | 10 | 14 | ||
| Total | 110 | 100 | 36 | 100 | 74 | 100 | ||
| Variables | Diagnosis Age | p-Value | |
|---|---|---|---|
| <50 Years | ≥50 Years | ||
| n (%) | n (%) | ||
| Right | 19 (25%) | 43 (25%) | 1.00 |
| Left | 57 (75%) | 130 (75%) | |
| Rectum involvement | |||
| No | 42 (53.8) | 99 (57.2) | 0.681 |
| Yes | 36 (46.2) | 74 (42.8) | |
| Mets by no. of involved organs | |||
| Non-Mets/missing | 42 (53.2) | 10 (58.0) | 0.766 |
| Single organ Mets | 20 (25.3) | 40 (23.0) | |
| Metastatic | 17 (21.5) | 33 (19.0) | |
| Histology type | |||
| Histology type (n = 209) | |||
| Adenocarcinoma (NOS) | 60 (83.3) | 129 (94.2) | 0.045 |
| Mucinous adenocarcinoma | 6 (8.3) | 4 (2.9) | |
| Signet-ring cell carcinoma | 6 (8.3) | 3 (2.2) | |
| Squamous cell carcinoma | - | 1 (0.7) | |
| Grade (n = 188) | |||
| 1 | 4 (6.8) | 6 (4.7) | 0.064 |
| 2 | 49 (83.1) | 120 (93.0) | |
| 3 | 6 (10.2) | 3 (2.3) | |
| pT (n = 137) | |||
| IS | 1 (2.1) | - | 0.293 |
| T1 | 2 (4.2) | - | |
| T2 | 3 (6.3) | 9 (10.3) | |
| T3 | 30 (62.5) | 59 (66.3) | |
| T4 | 3 (6.3) | 6 (6.7) | |
| T4a | 7 (14.6) | 13 (14.6) | |
| T4b | 2 (4.2) | 2 (2.2) | |
| pN (n = 123) | |||
| No | 13 (34.2) | 35 (41.2) | 0.146 |
| N1 | 3 (7.9) | 19 (22.4) | |
| N2a | 7 (18.4) | 8 (9.4) | |
| N1a | 2 (5.3) | 4 (4.7) | |
| N1b | 8 (21.1) | 7 (8.2) | |
| N2 | 1 (2.6) | 6 (7.1) | |
| N2b | 3 (7.9) | 3 (3.5) | |
| Nx | 1 (2.6) | 3 (3.5) | |
| MLH1 Immunohistochemistry (n = 182) | |||
| Intact | 61 (95.3) | 111 (94.1) | 1.000 |
| Lost | 3 (4.7) | 7 (5.9) | |
| PMS2 Immunohistochemistry (n = 182) | 1.000 | ||
| Intact | 61 (95.3) | 111 (94.1) | |
| Lost | 3 (4.7) | 7 (5.9) | |
| MSH2 Immunohistochemistry | |||
| Intact | 62 (96.8) | 114 (98.3) | |
| Lost | 1 (1.5) | 2 (1.7) | |
| MSH6 Immunohistochemistry | |||
| Proficient | 61 (96.8) | 113 (97.4) | >0.05 |
| Deficient | 2 (3.2) | 3 (2.5) | |
| MMR (n = 182) | |||
| Deficient | 5 (7.8) | 9 (7.6) | 1.000 |
| Proficient | 59 (92.2) | 109 (92.4) | |
| MSI (n = 21) | |||
| Positive | 2 (16.7) | 1 (11.1) | 1.000 |
| Negative | 10 (83.3) | 8 (88.9) | |
| KRAS (n = 105) | |||
| Wild type | 24 (58.5) | 37 (57.8) | 1.000 |
| Mutant | 17 (41.5) | 27 (42.2) | |
| BRAF (n = 60) | |||
| Wild type | 17 (94.4) | 40 (95.2) | 0.824 |
| Mutant | 1 (5.9) | 2 (4.8) | |
| CEAugL_group (n = 224) | |||
| Normal (<2.5) | 45 (60.8) | 70 (46.4) | 0.047 |
| Abnormal | 29 (39.2) | 81 (53.6) | |
| EOCRC | p-Value | LOCRC | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | |||||||
| N | % | N | % | N | % | N | % | |||
| Male | 14 | 18 | 26 | 33 | 0.369 | 18 | 10 | 80 | 46 | 0.016 |
| Female | 10 | 13 | 29 | 37 | 25 | 15 | 52 | 30 | ||
| Total | 24 | 30 | 55 | 70 | 43 | 25 | 132 | 75 | ||
| Estimate (95% C.I.) | Standard Error | p-Value | |
|---|---|---|---|
| Mortality | 0.684 | ||
| <50 years | 64.88 (57.79–71.97) | 3.62 | |
| ≥50 years | 67.24 (60.86–73.63) | 3.26 | |
| Remission | 0.653 | ||
| <50 years | 57.06 (51.34–62.78) | 2.92 | |
| ≥50 years | 55.58 (50.64–60.52) | 2.52 |
| Variables | <35 Years | 35–50 Years | >50 Years | p-Value |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Stage | 0.252 | |||
| Carcinoma in situ | - | 1 (1.5) | - | |
| Stage 1 | - | 6 (9.2) | 4 (2.7) | |
| Stage 2 | 4 (28.6) | 12 (18.5) | 39 (26.4) | |
| Stage 3 | 3 (21.4) | 11 (16.9) | 35 (23.6) | |
| Stage 4 | 7 (50.0) | 35 (53.8) | 70 (47.3) | |
| Location | 0.17 | |||
| Right | 6 (46.2) | 14 (20.3) | 42 (25.1) | |
| Left | 2 (15.4) | 36 (52.2) | 86 (51.5) | |
| Rectum | 5 (38.5) | 19 (27.5) | 39 (22.8) | |
| Anal canal | - | - | ||
| Gender | 0.811 | |||
| Male | 7 (50.0) | 37 (52.1) | 94 (56.0) | |
| Female | 7 (50.0) | 34 (47.9) | 74 (44.0) | |
| Grade | 0.051 | |||
| 1 | - | 4 (7.4) | 6 (4.9) | |
| 2 | 8 (72.7) | 47 (87.0) | 114 (92.7) | |
| 3 | 3 (27.3) | 3 (5.6) | 3 (2.4) | |
| Status | 0.433 | |||
| Alive | 9 (64.3) | 55 (77.5) | 134 (79.8) | |
| Dead | 5 (35.7) | 16 (22.5) | 34 (20.2) |
| Chi-Square | df | Sig. | |
|---|---|---|---|
| Log Rank (Mantel-Cox) | 1.411 | 2 | 0.494 |
| Breslow (Generalized Wilcoxon) | 3.192 | 2 | 0.203 |
| Tarone-Ware | 2.297 | 2 | 0.317 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Zaabi, A.; Al Shehhi, A.; Sayed, S.; Al Adawi, H.; Al Faris, F.; Al Alyani, O.; Al Asmi, M.; Al-Mirza, A.; Panchatcharam, S.; Al-Shaibi, M. Early Onset Colorectal Cancer in Arabs, Are We Dealing with a Distinct Disease? Cancers 2023, 15, 889. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030889
Al Zaabi A, Al Shehhi A, Sayed S, Al Adawi H, Al Faris F, Al Alyani O, Al Asmi M, Al-Mirza A, Panchatcharam S, Al-Shaibi M. Early Onset Colorectal Cancer in Arabs, Are We Dealing with a Distinct Disease? Cancers. 2023; 15(3):889. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030889
Chicago/Turabian StyleAl Zaabi, Adhari, Asmaa Al Shehhi, Shaymaa Sayed, Humaid Al Adawi, Faris Al Faris, Omaima Al Alyani, Maitha Al Asmi, Abdulrahman Al-Mirza, Sathiya Panchatcharam, and Maha Al-Shaibi. 2023. "Early Onset Colorectal Cancer in Arabs, Are We Dealing with a Distinct Disease?" Cancers 15, no. 3: 889. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15030889