

The Ability of Biodegradable Thermosensitive Hydrogel Composite Calcium-Silicon-Based Bioactive Bone Cement in Promoting Osteogenesis and Repairing Rabbit Distal Femoral Defects
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of PLGA-PEG-PLGA/C3S/C2S/POP
2.2. Characterization of Physical and Chemical Properties
2.2.1. Hydration Product Analysis
2.2.2. Setting Time
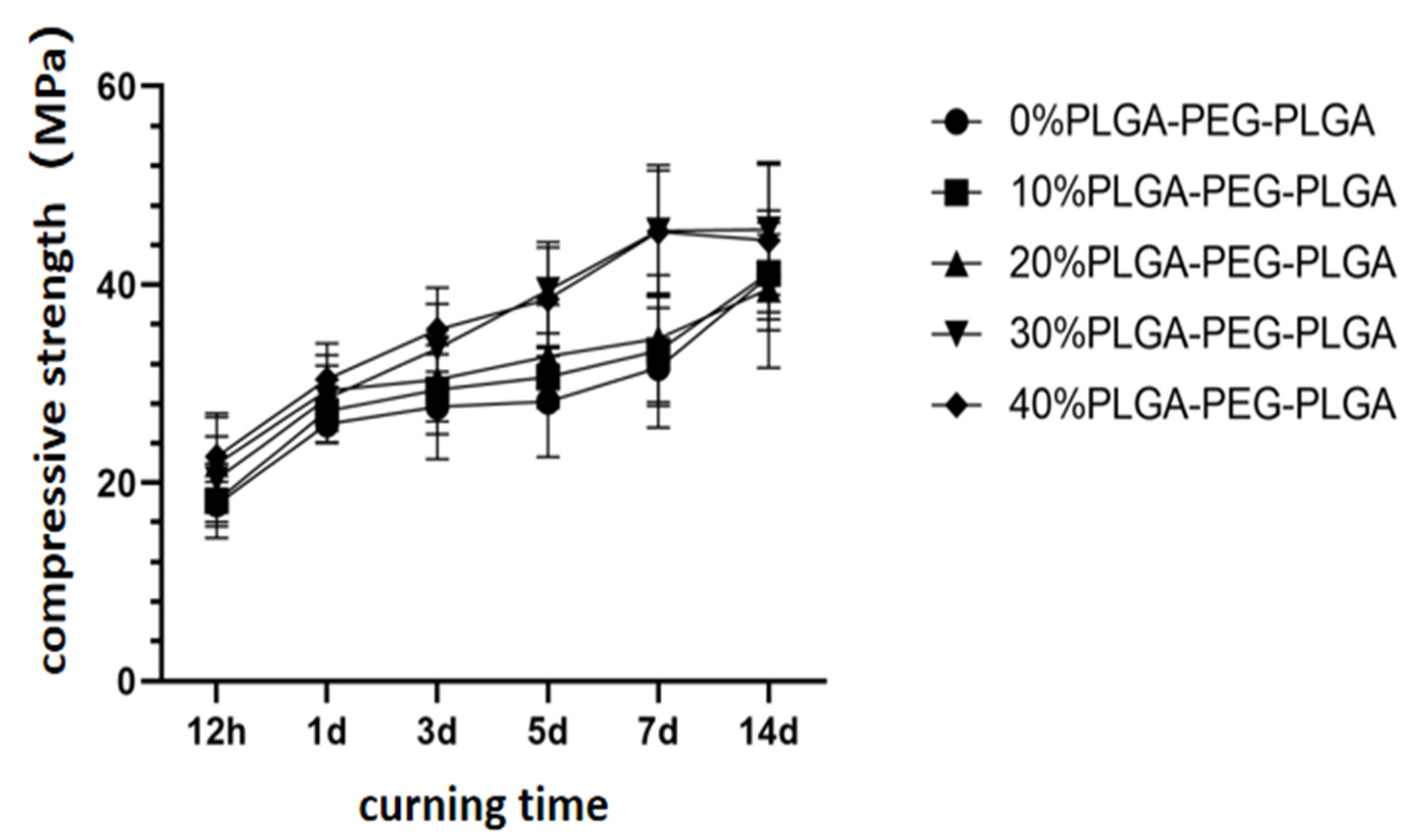
2.2.3. Compressive Strength
2.2.4. Injectability
2.2.5. Anti-Washout Properties
2.2.6. In Vitro Degradation
2.3. In Vitro Experimental Studies
2.3.1. In Vitro Cell Compatibility Evaluation
2.3.2. Alizarin Red Staining and Quantitative Detection
2.3.3. Quantitative Detection of Alkaline Phosphatase (ALP) Activity
2.4. Establishment of Animal Models and Material Implantation
2.5. Statistical Analysis
3. Results
3.1. Physical and Chemical Properties of the PLGA-PEG-PLGA/C3S/C2S/POP Composite Bone Cement
3.2. Cell Proliferation Activity and Osteoinductive Properties of the PLGA-PEG-PLGA/C3S/C2S/POP Composite Bone Cement
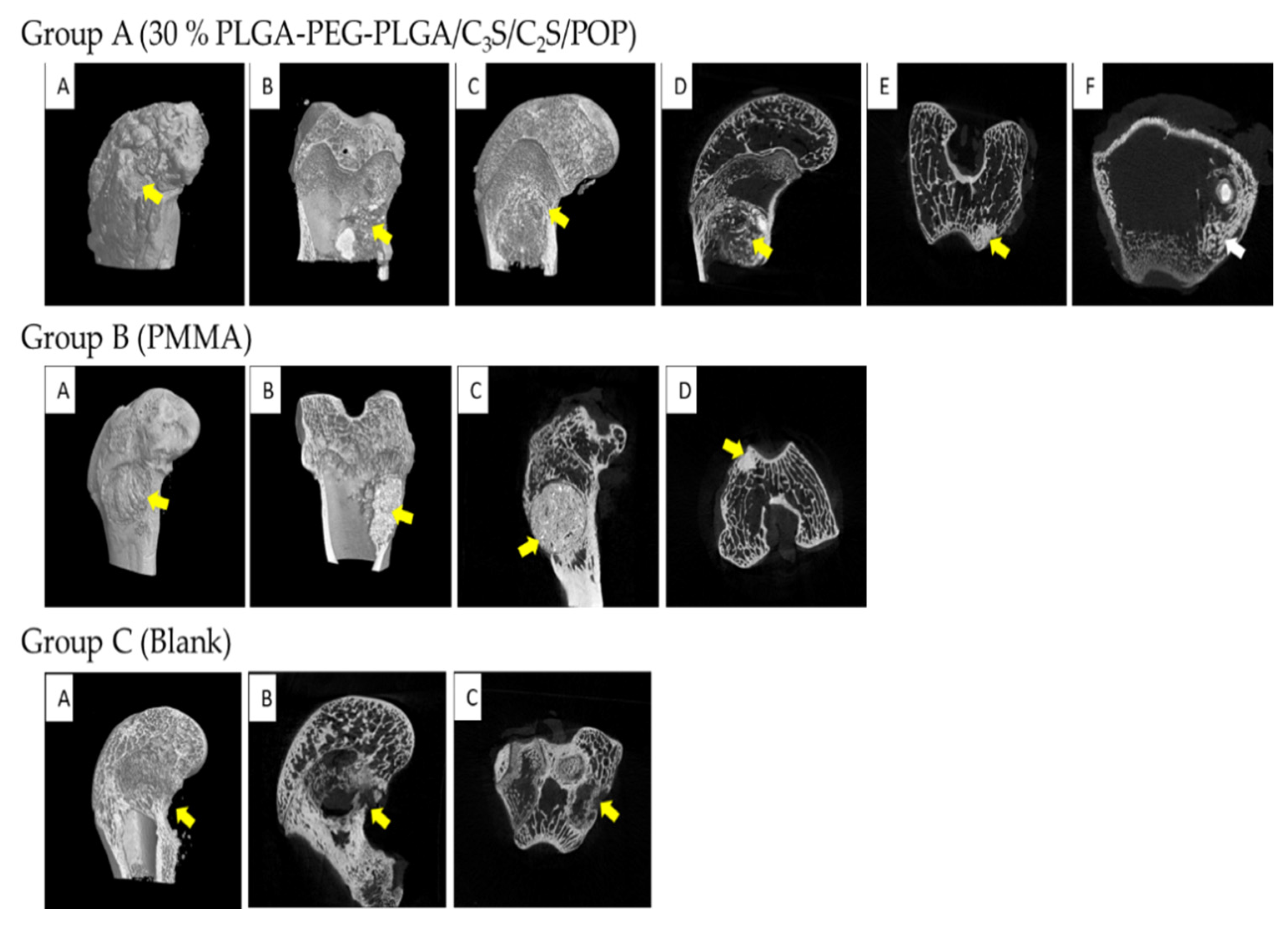
3.3. Animal Experiment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gao, C.; Feng, P.; Peng, S.; Shuai, C. Carbon Nanotube, Graphene and Boron Nitride Nanotube Reinforced Bioactive Ceramics for Bone Repair. Acta Biomater. 2017, 61, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Kadhim, M.; Holmes, L.; Gesheff, M.G.; Conway, J.D. Treatment Options for Nonunion with Segmental Bone Defects: Systematic Review and Quantitative Evidence Synthesis. J. Orthop. Trauma 2017, 31, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Wan, Q.; Pei, X. Graphene Family Materials in Bone Tissue Regeneration: Perspectives and Challenges. Nanoscale Res. Lett. 2018, 13, 289. [Google Scholar] [CrossRef]
- Spin-Neto, R.; Landazuri Del Barrio, R.A.; Pereira, L.A.V.D.; Marcantonio, R.A.C.; Marcantonio, E.; Marcantonio, E., Jr. Clinical Similarities and Histological Diversity Comparing Fresh Frozen Onlay Bone Blocks Allografts and Autografts in Human Maxillary Reconstruction. Clin. Implant. Dent. Relat. Res. 2013, 15, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.T.; Rosenbaum, A.J. Bone Grafts, Bone Substitutes and Orthobiologics: The Bridge between Basic Science and Clinical Advancements in Fracture Healing. Organogenesis 2012, 8, 114–124. [Google Scholar] [CrossRef]
- Lin, Q.; Zhang, X.; Liang, D. The in Vivo Dissolution of Tricalcium Silicate Bone Cement. J. Biomed. Mater. Res. Part A 2021, 109, 2527–2535. [Google Scholar] [CrossRef]
- Peng, W.; Liu, W.; Zhai, W.; Jiang, L.; Li, L.; Chang, J.; Zhu, Y. Effect of Tricalcium Silicate on the Proliferation and Odontogenic Differentiation of Human Dental Pulp Cells. J. Endod. 2011, 37, 1240–1246. [Google Scholar] [CrossRef]
- Huan, Z.; Chang, J. Self-Setting Properties and in Vitro Bioactivity of Calcium Sulfate Hemihydrate-Tricalcium Silicate Composite Bone Cements. Acta Biomater. 2007, 3, 952–960. [Google Scholar] [CrossRef]
- Huan, Z.; Chang, J.; Huang, X.H. Self-Setting Properties and in Vitro Bioactivity of Ca2SiO4/CaSO4.1/2H2O Composite Bone Cement. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 87, 387–394. [Google Scholar] [CrossRef]
- Ding, Z.; Li, H.; Wei, J.; Li, R.; Yan, Y. Developing a Novel Magnesium Glycerophosphate/Silicate-Based Organic-Inorganic Composite Cement for Bone Repair. Mater. Sci. Eng. C Mater. Biol. Appl. 2018, 87, 104–111. [Google Scholar] [CrossRef]
- Xiang, H.; Wang, Y.; Chang, H.; Yang, S.; Tu, M.; Zhang, X. Cerium-Containing A-Calcium Sulfate Hemihydrate Bone Substitute Promotes Osteogenesis. J. Biomater. Appl. 2019, 34, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Xiang, H.; Yao, Z.; Yang, S.; Tu, M.; Zhang, X. Strontium-Substituted Calcium Sulfate Hemihydrate/Hydroxyapatite Scaffold Enhances Bone Regeneration by Recruiting Bone Mesenchymal Stromal Cells. J. Biomater. Appl. 2020, 35, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Xu, D.; Liu, Z.; Jiang, Y.; Ren, M.; Xiang, H.; Yu, B. Physicochemical and Biological Properties of Carboxymethyl Chitosan Zinc (Cmcs-Zn)/A-Calcium Sulfate Hemihydrate (A-Csh) Composites. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 131, 112496. [Google Scholar] [CrossRef] [PubMed]
- Sha, S.; Qiu, F.; Li, S.; Liu, J.; Xu, H.; Tang, J.; Zhang, Y. A modified calcium silicate composite bone cement prepared from polyethylene glycol and graphene oxide for biomaterials. Mater. Today Commun. 2021, 27, 102431. [Google Scholar] [CrossRef]
- Vázquez, B.; Ginebra, M.P.; Gil, X.; Planell, J.A.; Román, J.S. Acrylic Bone Cements Modified with Beta-Tcp Particles Encapsulated with Poly(Ethylene Glycol). Biomaterials 2005, 26, 4309–4316. [Google Scholar] [CrossRef]
- Ross, M.; Hicks, E.A.; Rambarran, T.; Sheardown, H. Thermo-Sensitivity and Erosion of Chitosan Crosslinked Poly[N-Isopropylacrylamide-Co-(Acrylic Acid)-Co-(Methyl Methacrylate)] Hydrogels for Application to the Inferior Fornix. Acta Biomater. 2022, 141, 151–163. [Google Scholar] [CrossRef]
- Zhao, W.; Chang, J. Sol–Gel Synthesis and in Vitro Bioactivity of Tricalcium Silicate Powders. Mater. Lett. 2004, 58, 2350–2353. [Google Scholar] [CrossRef]
- Lewry, A.J.; Williamson, J. The Setting of Gypsum Plaster. J. Mater. Sci. 1994, 29, 6085–6090. [Google Scholar] [CrossRef]
- Aslan, T.; Dönmez Özkan, H. The Effect of Two Calcium Silicate-Based and One Epoxy Resin-Based Root Canal Sealer on Postoperative Pain: A Randomized Controlled Trial. Int. Endod. J. 2021, 54, 190–197. [Google Scholar] [CrossRef]
- Vojtova, L.; Michlovska, L.; Valova, K.; Zboncak, M.; Trunec, M.; Castkova, K.; Krticka, M.; Pavlinakova, V.; Polacek, P.; Dzurov, M.; et al. The Effect of the Thermosensitive Biodegradable PLGA-PEG-PLGA Copolymer on the Rheological, Structural and Mechanical Properties of Thixotropic Self-Hardening Tricalcium Phosphate Cement. Int. J. Mol. Sci. 2019, 20, 391. [Google Scholar] [CrossRef] [Green Version]
- ISO 9597:1989; Cements Test Methods—Determination of Setting Time and Soundness. ISO: London, UK, 1989.
- Kirby, D.M.; Biernacki, J.J. The Effect of Water-to-Cement Ratio on the Hydration Kinetics of Tricalcium Silicate Cements: Testing the Two-Step Hydration Hypothesis. Cem. Concr. Res. 2012, 42, 1147–1156. [Google Scholar] [CrossRef]
- Richardson, I.G. The Nature of Csh in Hardened Cements. Cem. Concr. Res. 1999, 29, 1131–1147. [Google Scholar] [CrossRef]
- Richardson, I.G. The Nature of the Hydration Products in Hardened Cement Pastes. Cem. Concr. Compos. 2000, 22, 97–113. [Google Scholar] [CrossRef]
- Liu, Z.; Yu, Z.; Chang, H.; Wang, Y.; Xiang, H.; Zhang, X.; Yu, B. Strontium-Containing A-Calcium Sulfate Hemihydrate Promotes Bone Repair Via the Tgf-Β/Smad Signaling Pathway. Mol. Med. Rep. 2019, 20, 3555–3564. [Google Scholar] [CrossRef]
- Cheng, K.; Zhu, W.; Weng, X.; Zhang, L.; Liu, Y.; Han, C.; Xia, W. Injectable Tricalcium Phosphate/Calcium Sulfate Granule Enhances Bone Repair by Reversible Setting Reaction. Biochem. Biophys. Res. Commun. 2021, 557, 151–158. [Google Scholar] [CrossRef]
- Wasupalli, G.K.; Verma, D. Injectable and Thermosensitive Nanofibrous Hydrogel for Bone Tissue Engineering. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 107, 110343. [Google Scholar] [CrossRef]
- Omer, R.A.; Hughes, A.; Hama, J.R.; Wang, W.; Tai, H. Hydrogels from dextran and soybean oil by UV photo-polymerization. J. Appl. Polym. Sci. 2015, 132, 1493–1502. [Google Scholar] [CrossRef]
- Wekwejt, M.; Chen, S.; Kaczmarek-Szczepańska, B. Nanosilver-Loaded Pmma Bone Cement Doped with Different Bioactive Glasses—Evaluation of Cytocompatibility, Antibacterial Activity, and Mechanical Properties. Biomater. Sci. 2021, 9, 3112–3126. [Google Scholar] [CrossRef]
- Tadier, S.; Galea, L.; Charbonnier, B.; Baroud, G.; Bohner, M. Phase and Size Separations Occurring During the Injection of Model Pastes Composed of Β-Tricalcium Phosphate Powder, Glass Beads and Aqueous Solutions. Acta Biomater. 2014, 10, 2259–2268. [Google Scholar] [CrossRef]
- Komath, M.; Varma, H.K. Development of a Fully Injectable Calcium Phosphate Cement for Orthopedic and Dental Applications. Bull. Mater. Sci. 2003, 26, 415–422. [Google Scholar] [CrossRef]
- Lee, Y.; Kwon, J.; Khang, G.; Lee, D. Reduction of Inflammatory Responses and Enhancement of Extracellular Matrix Formation by Vanillin-Incorporated Poly (Lactic-Co-Glycolic Acid) Scaffolds. Tissue Eng. Part A 2012, 18, 1967–1978. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, J.; Ye, J. Construction and Properties of Poly (Lactic-Co-Glycolic Acid)/Calcium Phosphate Cement Composite Pellets with Microspheres-in-Pellet Structure for Bone Repair. Ceram. Int. 2016, 42, 5587–5592. [Google Scholar] [CrossRef]
- Lodoso-Torrecilla, I.; van den Beucken, J.J.; Jansen, J.A. Calcium Phosphate Cements: Optimization toward Biodegradability. Acta Biomater. 2021, 119, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Marongiu, G.; Verona, M.; Cardoni, G.; Capone, A. Synthetic Bone Substitutes and Mechanical Devices for the Augmentation of Osteoporotic Proximal Humeral Fractures: A Systematic Review of Clinical Studies. J. Funct. Biomater. 2020, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Kenny, S.M.; Buggy, M. Bone Cements and Fillers: A Review. J. Mater. Sci. Mater. Med. 2003, 14, 923–938. [Google Scholar] [CrossRef] [PubMed]
- Hatton, P.V.; Hurrell-Gillingham, K.; Brook, I.M. Biocompatibility of Glass-Ionomer Bone Cements. J. Dent. 2006, 34, 598–601. [Google Scholar] [CrossRef]
- Urrutia, J.; Bono, C.M.; Mery, P.; Rojas, C. Early Histologic Changes Following Polymethylmethacrylate Injection (Vertebroplasty) in Rabbit Lumbar Vertebrae. Spine 2008, 33, 877–882. [Google Scholar] [CrossRef]
- Hench, L.L.; Polak, J.M. Third-Generation Biomedical Materials. Science 2002, 295, 1014–1017. [Google Scholar] [CrossRef]
- Chen, J.; Liu, Y.; Cheng, G.; Guo, J.; Du, S.; Qiu, J.; Wang, C.; Li, C.; Yang, X.; Chen, T.; et al. Tailored Hydrogel Delivering Niobium Carbide Boosts Ros-Scavenging and Antimicrobial Activities for Diabetic Wound Healing. Small 2022, 18, e2201300. [Google Scholar] [CrossRef]
- Osman, R.B.; Swain, M.V. A Critical Review of Dental Implant Materials with an Emphasis on Titanium Versus Zirconia. Materials 2015, 8, 932–958. [Google Scholar] [CrossRef] [Green Version]
- Shao, H.; Sun, M.; Zhang, F.; Liu, A.; He, Y.; Fu, J.; Yang, X.; Wang, H.; Gou, Z. Custom Repair of Mandibular Bone Defects with 3d Printed Bioceramic Scaffolds. J. Dent. Res. 2018, 97, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Zhai, X.; Ruan, C. Clay-Based Nanocomposite Hydrogel with Attractive Mechanical Properties and Sustained Bioactive Ion Release for Bone Defect Repair. J. Mater. Chem. B 2021, 9, 2394–2406. [Google Scholar] [CrossRef] [PubMed]
- Scholz, M.S.; Blanchfield, J.P.; Bloom, L.D.; Coburn, B.H.; Elkington, M.; Fuller, J.D.; Gilbert, M.E.; Muflahi, S.A.; Pernice, M.F.; Rae, S.I.; et al. The Use of Composite Materials in Modern Orthopaedic Medicine and Prosthetic Devices: A Review. Compos. Sci. Technol. 2011, 71, 1791–1803. [Google Scholar] [CrossRef]
- Eliades, T. Orthodontic Materials Research and Applications: Part 2. Current Status and Projected Future Developments in Materials and Biocompatibility. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 253–262. [Google Scholar] [CrossRef]
- Gumpert, R.; Bodo, K.; Spuller, E.; Poglitsch, T.; Bindl, R.; Ignatius, A.; Puchwein, P. Demineralization after Balloon Kyphoplasty with Calcium Phosphate Cement: A Histological Evaluation in Ten Patients. Eur. Spine J. 2014, 23, 1361–1368. [Google Scholar] [CrossRef]
- Maestretti, G.; Sutter, P.; Monnard, E.; Ciarpaglini, R.; Wahl, P.; Hoogewoud, H.; Gautier, E. A Prospective Study of Percutaneous Balloon Kyphoplasty with Calcium Phosphate Cement in Traumatic Vertebral Fractures: 10-Year Results. Eur. Spine J. 2014, 23, 1354–1360. [Google Scholar] [CrossRef]
- Hurle, K.; Christel, T.; Gbureck, U.; Moseke, C.; Neubauer, J.; Goetz-Neunhoeffer, F. Reaction Kinetics of Dual Setting A-Tricalcium Phosphate Cements. J. Mater. Sci. Mater. Med. 2016, 27, 1–13. [Google Scholar] [CrossRef]
- Ogasawara, T.; Sawamura, T.; Maeda, H.; Obata, A.; Hirata, H.; Kasuga, T. Enhancing the Mechanical Properties of Calcium Phosphate Cements Using Short-Length Polyhydroxyalkanoate Fibers. J. Ceram. Soc. Jpn. 2016, 124, 180–183. [Google Scholar] [CrossRef]
- Chiang, C.C.; Hsieh, M.K.; Wang, C.Y.; Tuan, W.H.; Lai, P.L. Cytotoxicity and Cell Response of Preosteoblast in Calcium Sulfate-Augmented Pmma Bone Cement. Biomed. Mater. 2021, 16, 055014. [Google Scholar] [CrossRef]
















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, C.; Qi, J.; Liu, J.; Wang, H.; Liu, Y.; Feng, Y.; Xu, G. The Ability of Biodegradable Thermosensitive Hydrogel Composite Calcium-Silicon-Based Bioactive Bone Cement in Promoting Osteogenesis and Repairing Rabbit Distal Femoral Defects. Polymers 2022, 14, 3852. https://0-doi-org.brum.beds.ac.uk/10.3390/polym14183852
Guo C, Qi J, Liu J, Wang H, Liu Y, Feng Y, Xu G. The Ability of Biodegradable Thermosensitive Hydrogel Composite Calcium-Silicon-Based Bioactive Bone Cement in Promoting Osteogenesis and Repairing Rabbit Distal Femoral Defects. Polymers. 2022; 14(18):3852. https://0-doi-org.brum.beds.ac.uk/10.3390/polym14183852
Chicago/Turabian StyleGuo, Chao, Junqiang Qi, Jia Liu, Haotian Wang, Yifei Liu, Yingying Feng, and Guohua Xu. 2022. "The Ability of Biodegradable Thermosensitive Hydrogel Composite Calcium-Silicon-Based Bioactive Bone Cement in Promoting Osteogenesis and Repairing Rabbit Distal Femoral Defects" Polymers 14, no. 18: 3852. https://0-doi-org.brum.beds.ac.uk/10.3390/polym14183852