

Cytotoxicity Assessment of a New Design for a Biodegradable Ureteral Mitomycin Drug-Eluting Stent in Urothelial Carcinoma Cell Culture
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. BraidStent-SF-MMC
2.1.1. Materials for Biodegradable Ureteral Stent Preparation
2.1.2. Materials for Stent SF and MMC Coating
2.1.3. Determination and Assessment of the MMC Release from BraidStent-SF-MMC
2.2. T24 Cell Culture Line
2.3. In vitro Cytotoxicity of the BraidStent-SF-MMC
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Yates, D.R.; Comperat, E.; Cussenot, O. Upper urinary tract urothelial cell carcinomas and other urological malignancies involved in the hereditary nonpolyposis colorectal cancer (lynch syndrome) tumor spectrum. Eur. Urol. 2008, 54, 1226–1236. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Liu, Z.; Tan, T.W.; Lee, Y.M.; Yeo, E.K.; Chong, Y.L. Optimal Management of Upper Tract Urothelial Carcinoma: Current Perspectives. Onco. Targets 2020, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Margulis, V.; Shariat, S.F.; Matin, S.F.; Kamat, A.M.; Zigeuner, R.; Kikuchi, E.; Lotan, Y.; Weizer, A.; Raman, J.D.; Wood, C.G. Upper Tract Urothelial Carcinoma CollaborationThe Upper Tract Urothelial Carcinoma Collaboration. Outcomes of radical nephroureterectomy: A series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer 2009, 115, 1224–1233. [Google Scholar] [CrossRef]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Hugh Mostafid, A.; et al. European association of urology guidelines on upper urinary tract urothelial carcinoma: 2020 Update. Eur. Urol. 2021, 79, 62–79. [Google Scholar] [CrossRef]
- Petros, F.G.; Li, R.; Matin, S.F. Endoscopic Approaches to Upper Tract Urothelial Carcinoma. Urol. Clin. North. Am. 2018, 45, 267–286. [Google Scholar] [CrossRef]
- Knoedler, J.J.; Raman, J.D. Intracavitary therapies for upper tract urothelial carcinoma. Expert Rev. Clin. Pharmacol. 2018, 11, 487–493. [Google Scholar] [CrossRef]
- Gallioli, A.; Boissier, R.; Territo, A.; Vila Reyes, H.; Sanguedolce, F.; Gaya, J.M.; Regis, F.; Subiela, J.D.; Palou, J.; Breda, A. Adjuvant Single-Dose Upper Urinary Tract Instillation of Mitomycin C After Therapeutic Ureteroscopy for Upper Tract Urothelial Carcinoma: A Single-Centre Prospective Non-Randomized Trial. J. Endourol. 2020, 34, 573–580. [Google Scholar] [CrossRef]
- Foerster, B.; D’Andrea, D.; Abufaraj, M.; Broenimann, S.; Karakiewicz, P.I.; Rouprêt, M.; Gontero, P.; Lerner, S.P.; Shariat, S.F.; Soria, F. Endocavitary treatment for upper tract urothelial carcinoma: A meta-analysis of the current literature. Urol. Oncol. 2019, 37, 430–436. [Google Scholar] [CrossRef]
- Matin, S.F.; Pierorazio, P.M.; Kleinmann, N.; Gore, J.L.; Shabsigh, A.; Hu, B.; Chamie, K.; Godoy, G.; Hubosky, S.G.; Rivera, M.; et al. Durability of response to primary chemoablation of low-grade upper tract urothelial carcinoma using UGN-101, a mitomycin-containing reverse thermal gel: OLYMPUS Trial Final Report. J. Urol 2022, 207, 779–788. [Google Scholar] [CrossRef]
- Qi, Y.; Wang, H.; Wei, K.; Yang, Y.; Zheng, R.Y.; Kim, I.S.; Zhang, K.Q. A review of structure construction of silk fibroin biomaterials from single structures to multi-level structures. Int. J. Mol. Sci. 2017, 18, 237. [Google Scholar] [CrossRef]
- Soria, F.; de La Cruz, J.E.; Fernandez, T.; Budia, A.; Serrano, Á.; Sanchez-Margallo, F.M. Heparin coating in biodegradable ureteral stents does not decrease bacterial colonization-assessment in ureteral stricture endourological treatment in animal model. Transl. Androl. Urol. 2021, 10, 1700–1710. [Google Scholar] [CrossRef]
- Soria, F.; de La Cruz, J.E.; Caballero-Romeu, J.P.; Pamplona, M.; Pérez-Fentes, D.; Resel-Folskerma, L.; Sanchez-Margallo, F.M. Comparative assessment of biodegradable-antireflux heparine coated ureteral stent: Animal model study. BMC Urol. 2021, 21, 32. [Google Scholar] [CrossRef]
- Soria, F.; de La Cruz, J.E.; Budia, A.; Cepeda, M.; Álvarez, S.; Serrano, Á.; Sanchez-Margallo, F.M. Iatrogenic ureteral injury treatment with biodegradable antireflux heparin-coated ureteral stent-animal model comparative study. J. Endourol. 2021, 35, 1244–1249. [Google Scholar] [CrossRef]
- Aznar-Cervantes, S.D.; Pagan, A.; Monteagudo Santesteban, B.; Cenis, J.L. Effect of different cocoon stifling methods on the properties of silk fibroin biomaterials. Sci. Rep. 2019, 9, 6703. [Google Scholar] [CrossRef]
- Rockwood, D.N.; Preda, R.C.; Yücel, T.; Wang, X.; Lovett, M.L.; Kaplan, D.L. Materials fabrication from Bombyx mori silk fibroin. Nat. Protoc. 2011, 22, 1612–1631. [Google Scholar] [CrossRef]
- Soria, F.; Aznar-Cervantes, S.D.; de la Cruz, J.E.; Budia, A.; Aranda, J.; Caballero, J.P.; Serrano, Á.; Sánchez Margallo, F.M. Assessment of a coated mitomycin-releasing biodegradable ureteral stent as an adjuvant therapy in upper urothelial carcinoma: A Comparative in vitro study. Polymers 2022, 14, 3059. [Google Scholar] [CrossRef]
- Wang, J.; Wang, G.; Shan, H.; Wang, X.; Wang, C.; Zhuang, X.; Ding, J.; Chen, X. Gradiently degraded electrospun polyester scaffolds with cytostatic for urothelial carcinoma therapy. Biomater. Sci. 2019, 7, 963–974. [Google Scholar] [CrossRef]
- Barros, A.A.; Browne, S.; Oliveira, C.; Lima, E.; Duarte, A.R.; Healy, K.E.; Reis, R.L. Drug-eluting biodegradable ureteral stent: New approach for urothelial tumors of upper urinary tract cancer. Int. J. Pharm. 2016, 513, 227–237. [Google Scholar] [CrossRef]
- Pinto-Leite, R.; Botelho, P.; Ribeiro, E.; Oliveira, P.A.; Santos, L. Effect of sirolimus on urinary bladder cancer T24 cell line. J. Exp. Clin. Cancer Res. 2009, 28, 3. [Google Scholar] [CrossRef] [Green Version]
- Marinaro, F.; Silva, J.M.; Barros, A.A.; Aroso, I.M.; Gómez-Blanco, J.C.; Jardin, I.; Lopez, J.J.; Pulido, M.; de Pedro, M.Á.; Reis, R.L.; et al. A fibrin coating method of polypropylene meshes enables the adhesion of menstrual blood-derived mesenchymal stromal cells: A new delivery strategy for stem cell-based therapies. Int. J. Mol. Sci. 2021, 22, 13385. [Google Scholar] [CrossRef]
- Iqbal, H.; Razzaq, A.; Uzair, B.; Ul Ain, N.; Sajjad, S.; Althobaiti, N.A.; Albalawi, A.E.; Menaa, B.; Haroon, M.; Khan, M.; et al. Breast cancer inhibition by biosynthesized titanium dioxide nanoparticles is comparable to free doxorubicin but appeared safer in Balb/c Mice. Materials 2021, 14, 3155. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, X.; Castellot, J.; Herman, I.; Iafrati, M.; Kaplan, D.L. Controlled release from multilayer silk biomaterial coatings to modulate vascular cell responses. Biomaterials 2008, 29, 894–903. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
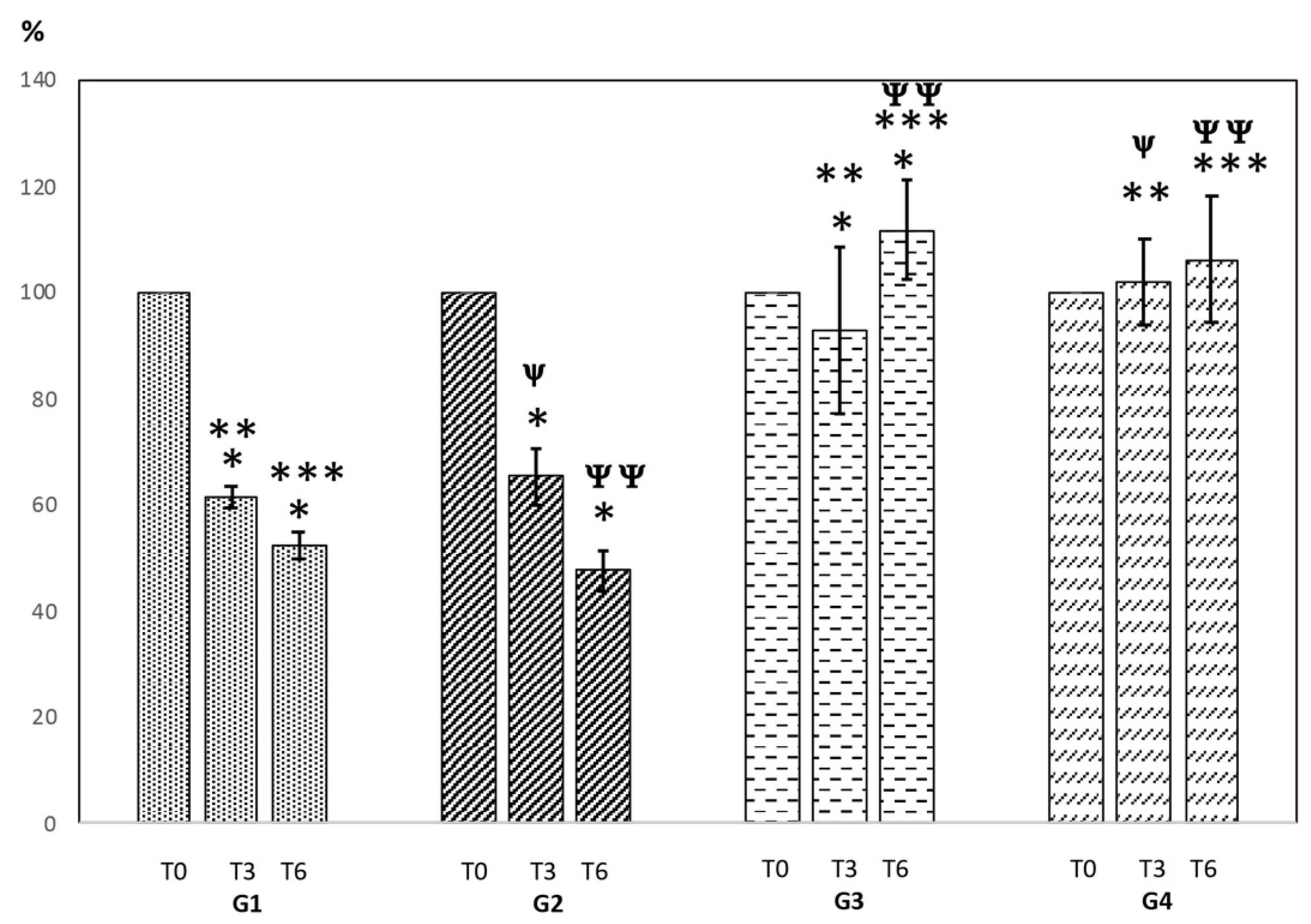
| Groups | |
|---|---|
| G1 (3 h-G13; 6 h-G16) | T24 cell culture + Recommended MMC oce in UTUC (0.66 mg/mL) [8]. No stent. Positive control. |
| G2 (3 h-G23; 6 h-G26) | T24 cell culture + BraidStent-SF-MMC. |
| G3 (3 h-G33; 6 h-G36) | T24 cell culture + BraidStent-SF. Negative control. |
| G4 (3 h-G43; 6 h-G46) | T24 cell culture. No stent. Untreated cells were used as negative control. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soria, F.; Martínez-Pla, L.; Aznar-Cervantes, S.D.; de la Cruz, J.E.; Fernández, T.; Pérez-Fentes, D.; Llanes, L.; Sánchez-Margallo, F.M. Cytotoxicity Assessment of a New Design for a Biodegradable Ureteral Mitomycin Drug-Eluting Stent in Urothelial Carcinoma Cell Culture. Polymers 2022, 14, 4081. https://0-doi-org.brum.beds.ac.uk/10.3390/polym14194081
Soria F, Martínez-Pla L, Aznar-Cervantes SD, de la Cruz JE, Fernández T, Pérez-Fentes D, Llanes L, Sánchez-Margallo FM. Cytotoxicity Assessment of a New Design for a Biodegradable Ureteral Mitomycin Drug-Eluting Stent in Urothelial Carcinoma Cell Culture. Polymers. 2022; 14(19):4081. https://0-doi-org.brum.beds.ac.uk/10.3390/polym14194081
Chicago/Turabian StyleSoria, Federico, Luna Martínez-Pla, Salvador D. Aznar-Cervantes, Julia E. de la Cruz, Tomás Fernández, Daniel Pérez-Fentes, Luis Llanes, and Francisco Miguel Sánchez-Margallo. 2022. "Cytotoxicity Assessment of a New Design for a Biodegradable Ureteral Mitomycin Drug-Eluting Stent in Urothelial Carcinoma Cell Culture" Polymers 14, no. 19: 4081. https://0-doi-org.brum.beds.ac.uk/10.3390/polym14194081