Effect of Lifestyle Intervention in the Concentration of Adipoquines and Branched Chain Amino Acids in Subjects with High Risk of Developing Type 2 Diabetes: Feel4Diabetes Study

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population and Design
2.2. Anthropometric, Clinical, and Biochemical Parameters
2.3. Dietary and Physical Parameters
2.4. Branched Amino Acid and Retinol-Binding Protein 4 Quantification
2.5. Statistical Analysis
3. Results
3.1. Baseline and Anthropometric Characteristics
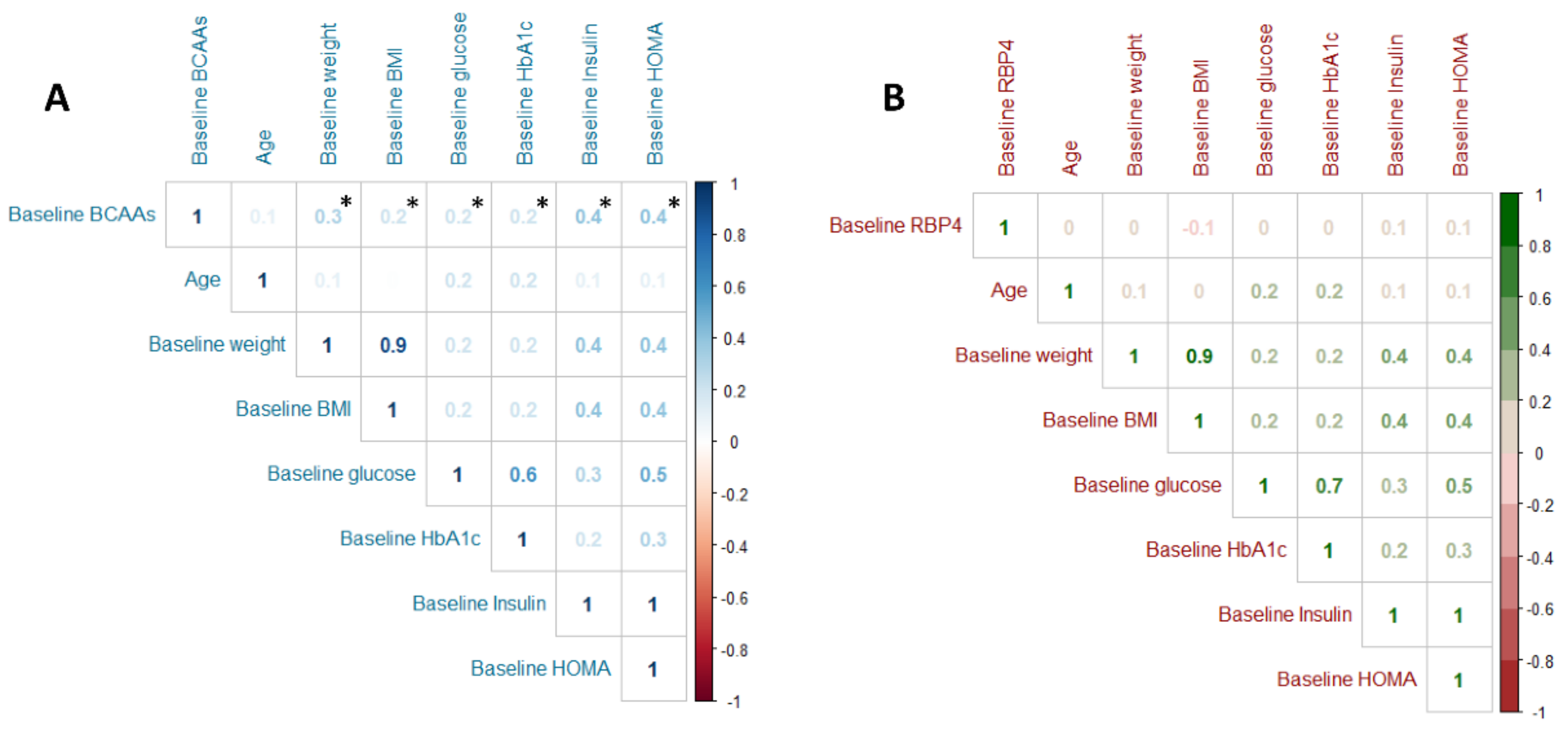
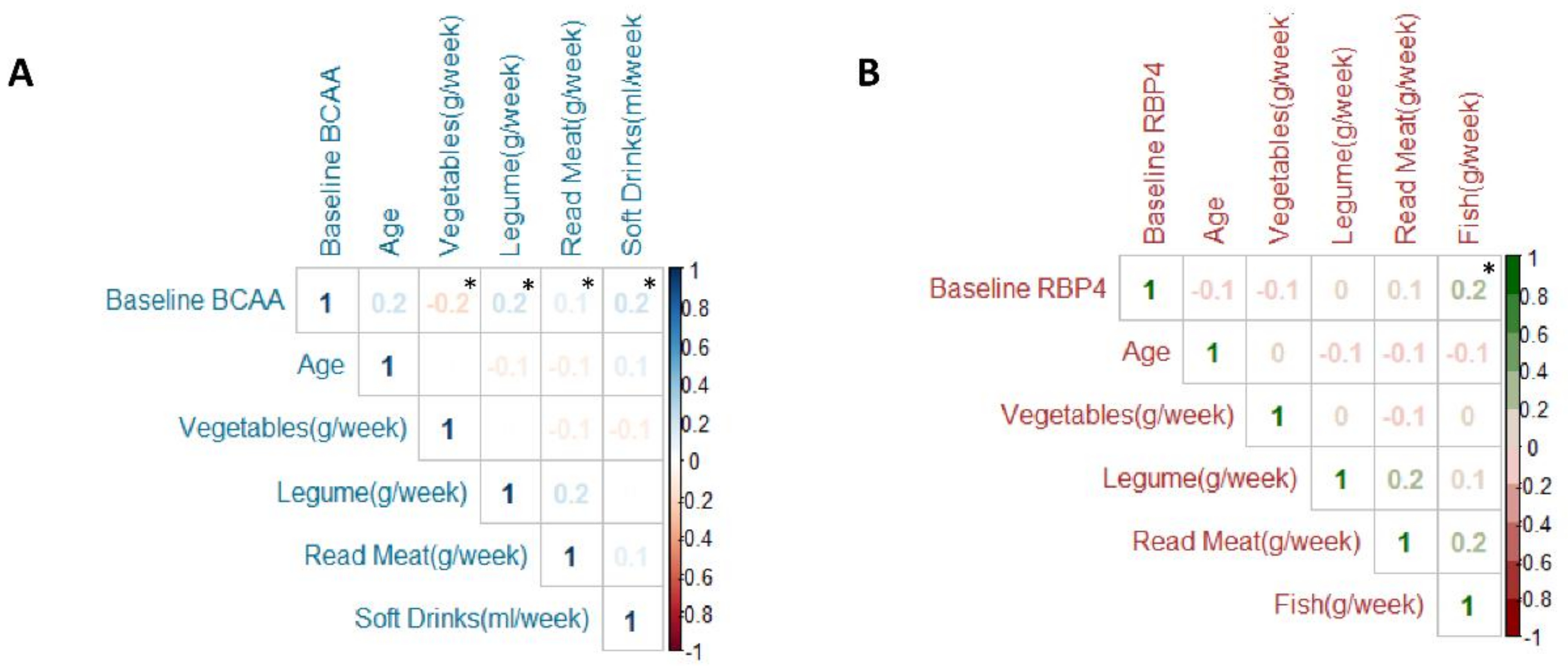
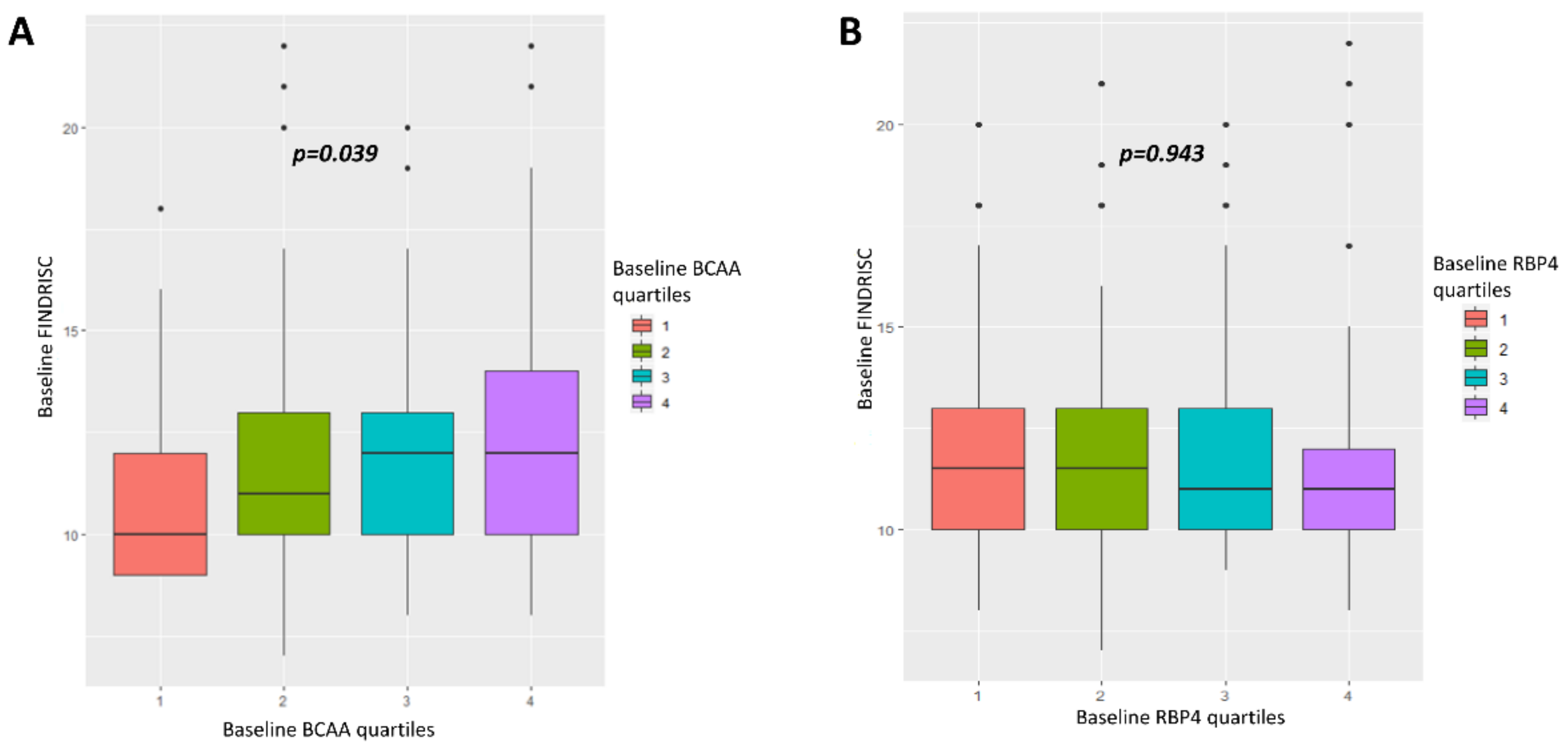
3.2. Relationship between BCAA and RBP4 with Clinical, Anthropometrics, Glucose Metabolism, Lifestyle and T2D Risk at Baseline
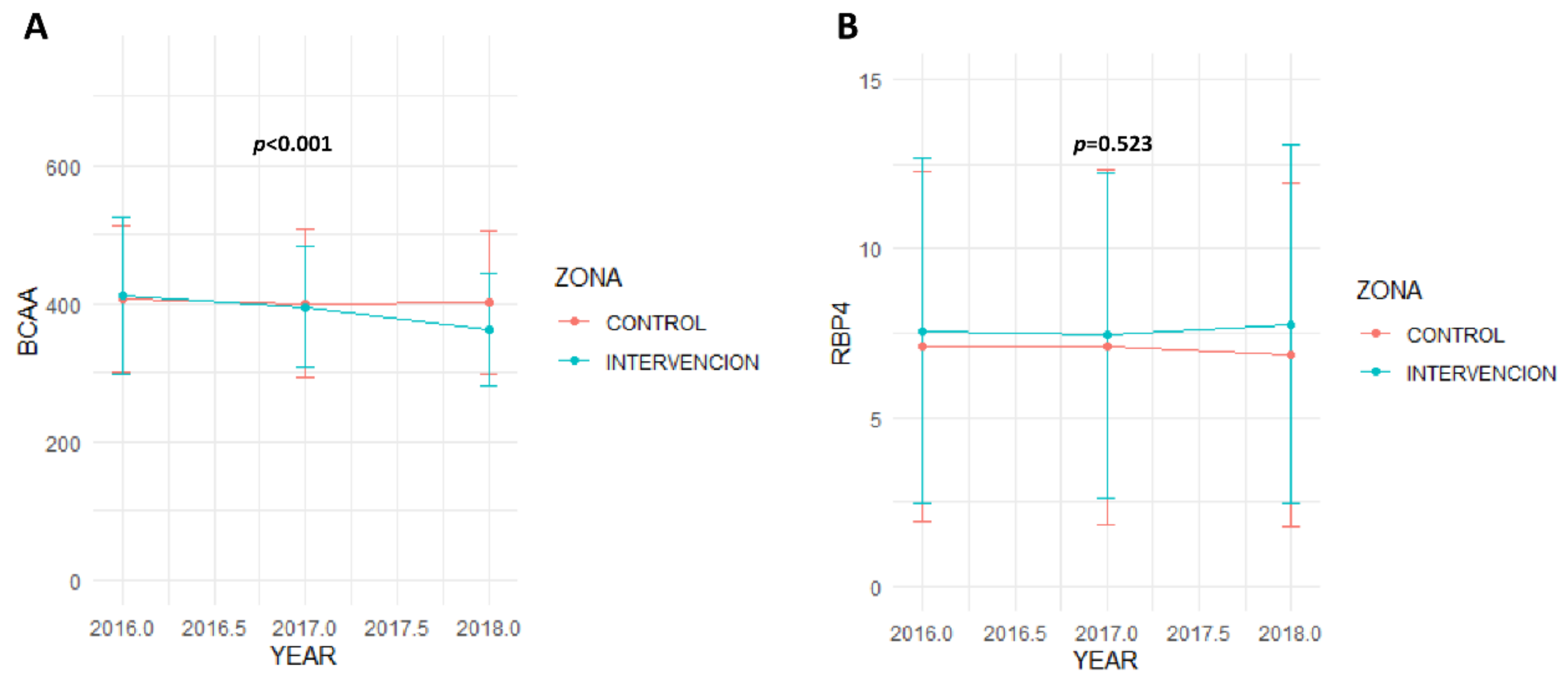
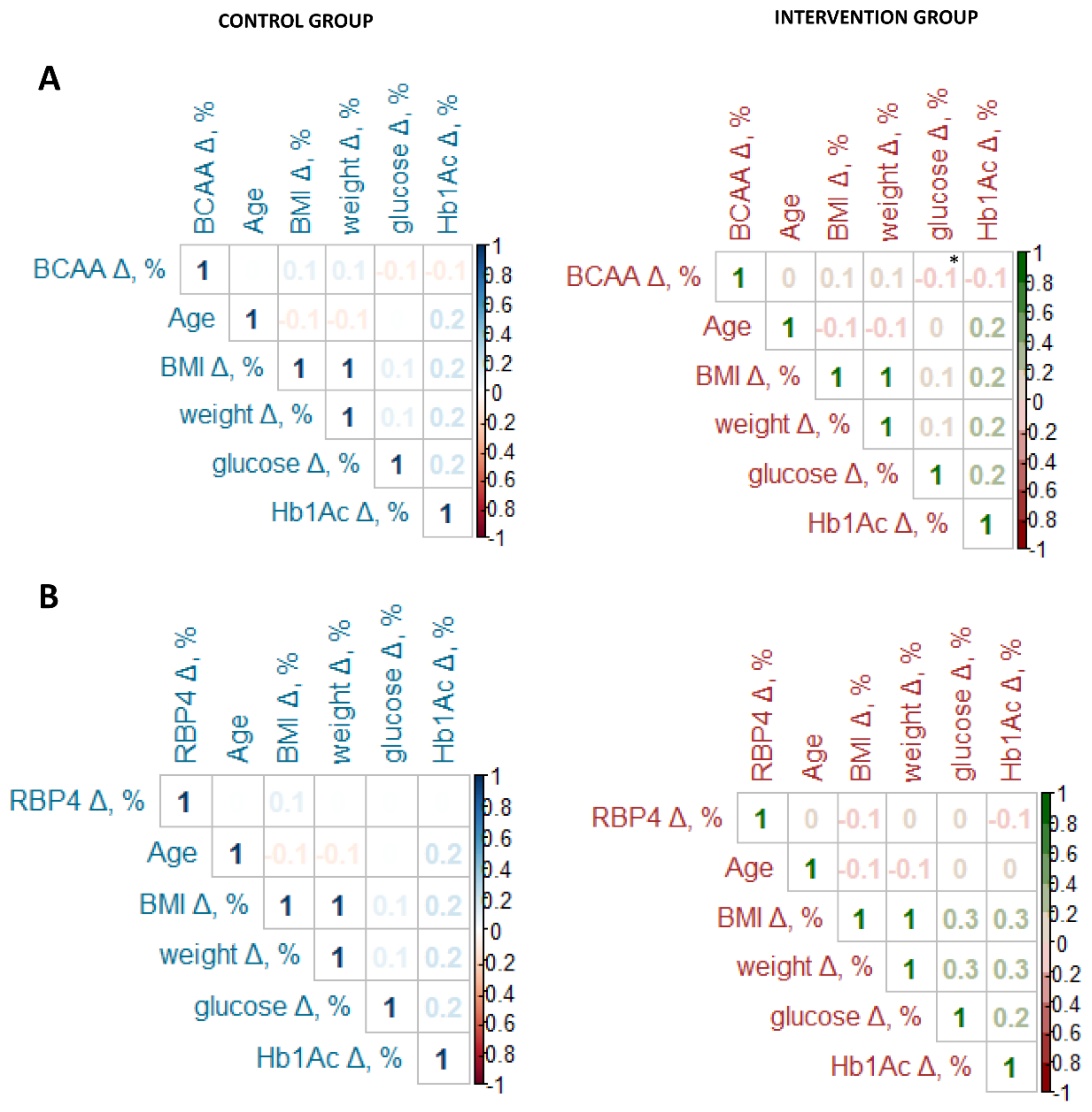
3.3. Clinical, Anthropometric, Biochemical, and Lifestyle Parameters across the Study
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Emerging Risk Factors Collaboration; Sarwar, N.; Gao, P.; Seshasai, S.R.K.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [PubMed] [Green Version]
- Low Wang, C.C.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Clinical Update: Cardiovascular Disease in Diabetes Mellitus: Atherosclerotic Cardiovascular Disease and Heart Failure in Type 2 Diabetes Mellitus - Mechanisms, Management, and Clinical Considerations. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef] [PubMed]
- Muilwijk, M.; Ho, F.; Waddell, H.; Sillars, A.; Welsh, P.; Iliodromiti, S.; Brown, R.; Ferguson, L.; Stronks, K.; van Valkengoed, I.; et al. Contribution of type 2 diabetes to all-cause mortality, cardiovascular disease incidence and cancer incidence in white Europeans and South Asians: Findings from the UK Biobank population-based cohort study. BMJ Open Diabetes Res. Care 2019, 7, e000765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeks, K.A.C.; Freitas-Da-Silva, D.; Adeyemo, A.; Beune, E.J.A.J.; Modesti, P.A.; Stronks, K.; Zafarmand, M.H.; Agyemang, C. Disparities in type 2 diabetes prevalence among ethnic minority groups resident in Europe: A systematic review and meta-analysis. Intern. Emerg. Med. 2016, 11, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Larson, M.G.; Vasan, R.S.; Cheng, S.; Rhee, E.P.; McCabe, E.; Lewis, G.D.; Fox, C.S.; Jacques, P.F.; Fernandez, C.; et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 2011, 17, 448–453. [Google Scholar] [CrossRef]
- Ahola-Olli, A.V.; Mustelin, L.; Kalimeri, M.; Kettunen, J.; Jokelainen, J.; Auvinen, J.; Puukka, K.; Havulinna, A.S.; Lehtimäki, T.; Kähönen, M.; et al. Circulating metabolites and the risk of type 2 diabetes: A prospective study of 11,896 young adults from four Finnish cohorts. Diabetologia 2019, 62, 2298–2309. [Google Scholar] [CrossRef] [Green Version]
- Isanejad, M.; LaCroix, A.; Thomson, C.A.; Tinker, L.; Larson, J.C.; Qi, Q.; Qi, L.; Cooper-DeHoff, R.M.; Phillips, L.S.; Prentice, R.L.; et al. Branched Chain Amino Acid, Meat Intake and Risk of Type 2 Diabetes in the Women’s Health Initiative. Br. J. Nutr. 2017, 117, 1523–1530. [Google Scholar] [CrossRef] [Green Version]
- Huffman, K.M.; Shah, S.H.; Stevens, R.D.; Bain, J.R.; Muehlbauer, M.; Slentz, C.A.; Tanner, C.J.; Kuchibhatla, M.; Houmard, J.A.; Newgard, C.B.; et al. Relationships between circulating metabolic intermediates and insulin action in overweight to obese, inactive men and women. Diabetes Care 2009, 32, 1678–1683. [Google Scholar] [CrossRef] [Green Version]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef] [Green Version]
- Um, S.H.; D’Alessio, D.; Thomas, G. Nutrient overload, insulin resistance, and ribosomal protein S6 kinase 1, S6K1. Cell Metab. 2006, 3, 393–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoneshiro, T.; Wang, Q.; Tajima, K.; Matsushita, M.; Maki, H.; Igarashi, K.; Dai, Z.; White, P.J.; McGarrah, R.W.; Ilkayeva, O.R.; et al. BCAA catabolism in brown fat controls energy homeostasis through SLC25A44. Nature 2019, 572, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M.; Mantzoros, C.S. From leptin to other adipokines in health and disease: Facts and expectations at the beginning of the 21st century. Metab. Clin. Exp. 2015, 64, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.; Blomhoff, R. Retinol, Retinoic Acid, and Retinol-Binding Protein 4 are Differentially Associated with Cardiovascular Disease, Type 2 Diabetes, and Obesity: An Overview of Human Studies. Adv. Nutr. 2019. [Google Scholar] [CrossRef]
- Fan, J.; Yin, S.; Lin, D.; Liu, Y.; Chen, N.; Bai, X.; Ke, Q.; Shen, J.; You, L.; Lin, X.; et al. Association of Serum Retinol-Binding Protein 4 Levels and the Risk of Incident Type 2 Diabetes in Subjects With Prediabetes. Diabetes Care 2019, 42, 1574–1581. [Google Scholar] [CrossRef]
- Mateo-Gallego, R.; Lamiquiz-Moneo, I.; Perez-Calahorra, S.; Marco-Benedí, V.; Bea, A.M.; Baila-Rueda, L.; Laclaustra, M.; Peñalvo, J.L.; Civeira, F.; Cenarro, A. Different protein composition of low-calorie diet differently impacts adipokine profile irrespective of weight loss in overweight and obese women. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 133–142. [Google Scholar] [CrossRef]
- Manios, Y.; Androutsos, O.; Lambrinou, C.-P.; Cardon, G.; Lindstrom, J.; Annemans, L.; Mateo-Gallego, R.; de Sabata, M.S.; Iotova, V.; Kivela, J.; et al. A school- and community-based intervention to promote healthy lifestyle and prevent type 2 diabetes in vulnerable families across Europe: Design and implementation of the Feel4Diabetes-study. Public Health Nutr. 2018, 21, 3281–3290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindström, J.; Tuomilehto, J. The diabetes risk score: A practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef] [Green Version]
- Mavrogianni, C.; Lambrinou, C.-P.; Androutsos, O.; Lindström, J.; Kivelä, J.; Cardon, G.; Huys, N.; Tsochev, K.; Iotova, V.; Chakarova, N.; et al. Evaluation of the Finnish Diabetes Risk Score as a screening tool for undiagnosed type 2 diabetes and dysglycaemia among early middle-aged adults in a large-scale European cohort. The Feel4Diabetes-study. Diabetes Res. Clin. Pract. 2019, 150, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Jølle, A.; Midthjell, K.; Holmen, J.; Carlsen, S.M.; Tuomilehto, J.; Bjørngaard, J.H.; Åsvold, B.O. Validity of the FINDRISC as a prediction tool for diabetes in a contemporary Norwegian population: A 10-year follow-up of the HUNT study. BMJ Open Diabetes Res. Care 2019, 7, e000769. [Google Scholar] [CrossRef] [Green Version]
- R.C. Team. R: A Language and Environment for Statistical Computing 2013; R Foundation for Statistical Computing: Vienna, Austria, 2015; Available online: https://www.r-project.org/.
- Karusheva, Y.; Koessler, T.; Strassburger, K.; Markgraf, D.; Mastrototaro, L.; Jelenik, T.; Simon, M.-C.; Pesta, D.; Zaharia, O.-P.; Bódis, K.; et al. Short-term dietary reduction of branched-chain amino acids reduces meal-induced insulin secretion and modifies microbiome composition in type 2 diabetes: A randomized controlled crossover trial. Am. J. Clin. Nutr. 2019, 110, 1098–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goffredo, M.; Santoro, N.; Tricò, D.; Giannini, C.; D’Adamo, E.; Zhao, H.; Peng, G.; Yu, X.; Lam, T.T.; Pierpont, B.; et al. A Branched-Chain Amino Acid-Related Metabolic Signature Characterizes Obese Adolescents with Non-Alcoholic Fatty Liver Disease. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, S.E.; Shaham, O.; McCarthy, M.A.; Deik, A.A.; Wang, T.J.; Gerszten, R.E.; Clish, C.B.; Mootha, V.K.; Grinspoon, S.K.; Fleischman, A. Circulating Branched-chain Amino Acid Concentrations Are Associated with Obesity and Future Insulin Resistance in Children and Adolescents. Pediatr Obes. 2013, 8, 52–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association 8. Obesity Management for the Treatment of Type 2 Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S89–S97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennings, A.; MacGregor, A.; Pallister, T.; Spector, T.; Cassidy, A. Associations between branched chain amino acid intake and biomarkers of adiposity and cardiometabolic health independent of genetic factors: A twin study. Int. J. Cardiol. 2016, 223, 992–998. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Canela, M.; Guasch-Ferré, M.; Toledo, E.; Clish, C.B.; Razquin, C.; Liang, L.; Wang, D.D.; Corella, D.; Estruch, R.; Hernáez, Á.; et al. Plasma branched chain/aromatic amino acids, enriched Mediterranean diet and risk of type 2 diabetes: Case-cohort study within the PREDIMED Trial. Diabetologia 2018, 61, 1560–1571. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Ceglarek, U.; Huang, T.; Li, L.; Rood, J.; Ryan, D.H.; Bray, G.A.; Sacks, F.M.; Schwarzfuchs, D.; Thiery, J.; et al. Weight-loss diets and 2-y changes in circulating amino acids in 2 randomized intervention trials. Am. J. Clin. Nutr. 2016, 103, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.H.; Crosslin, D.R.; Haynes, C.S.; Nelson, S.; Turer, C.B.; Stevens, R.D.; Muehlbauer, M.J.; Wenner, B.R.; Bain, J.R.; Laferrère, B.; et al. Branched-chain amino acid levels are associated with improvement in insulin resistance with weight loss. Diabetologia 2012, 55, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Magkos, F.; Zhou, D.; Eagon, J.C.; Fabbrini, E.; Okunade, A.L.; Klein, S. Adipose tissue monomethyl branched-chain fatty acids and insulin sensitivity: Effects of obesity and weight loss. Obesity (Silver Spring) 2015, 23, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Pakiet, A.; Wilczynski, M.; Rostkowska, O.; Korczynska, J.; Jabłonska, P.; Kaska, L.; Proczko-Stepaniak, M.; Sobczak, E.; Stepnowski, P.; Magkos, F.; et al. The Effect of One Anastomosis Gastric Bypass on Branched-Chain Fatty Acid and Branched-Chain Amino Acid Metabolism in Subjects with Morbid Obesity. Obes. Surg. 2020, 30, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Takashina, C.; Tsujino, I.; Watanabe, T.; Sakaue, S.; Ikeda, D.; Yamada, A.; Sato, T.; Ohira, H.; Otsuka, Y.; Oyama-Manabe, N.; et al. Associations among the plasma amino acid profile, obesity, and glucose metabolism in Japanese adults with normal glucose tolerance. Nutr. Metab. 2016, 13, 5. [Google Scholar] [CrossRef] [PubMed]
- Fukagawa, N.K.; Minaker, K.L.; Rowe, J.W.; Goodman, M.N.; Matthews, D.E.; Bier, D.M.; Young, V.R. Insulin-mediated reduction of whole body protein breakdown. Dose-response effects on leucine metabolism in postabsorptive men. J. Clin. Invest. 1985, 76, 2306–2311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández-Alvarez, M.I.; Díaz-Ramos, A.; Berdasco, M.; Cobb, J.; Planet, E.; Cooper, D.; Pazderska, A.; Wanic, K.; O’Hanlon, D.; Gomez, A.; et al. Early-onset and classical forms of type 2 diabetes show impaired expression of genes involved in muscle branched-chain amino acids metabolism. Sci. Rep. 2017, 7, 1–12. [Google Scholar]
- Newgard, C.B. Interplay between lipids and branched-chain amino acids in development of insulin resistance. Cell Metab. 2012, 15, 606–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zabetian-Targhi, F.; Mahmoudi, M.J.; Rezaei, N.; Mahmoudi, M. Retinol Binding Protein 4 in Relation to Diet, Inflammation, Immunity, and Cardiovascular Diseases. Adv. Nutr. 2015, 6, 748. [Google Scholar] [CrossRef] [Green Version]
- Moraes-Vieira, P.M.; Yore, M.M.; Dwyer, P.M.; Syed, I.; Aryal, P.; Kahn, B.B. RBP4 activates antigen-presenting cells, leading to adipose tissue inflammation and systemic insulin resistance. Cell Metab. 2014, 19, 512–526. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Graham, T.E.; Mody, N.; Preitner, F.; Peroni, O.D.; Zabolotny, J.M.; Kotani, K.; Quadro, L.; Kahn, B.B. Serum retinol binding protein 4 contributes to insulin resistance in obesity and type 2 diabetes. Nature 2005, 436, 356–362. [Google Scholar] [CrossRef]
- Haider, D.G.; Schindler, K.; Prager, G.; Bohdjalian, A.; Luger, A.; Wolzt, M.; Ludvik, B. Serum retinol-binding protein 4 is reduced after weight loss in morbidly obese subjects. J. Clin. Endocrinol. Metab. 2007, 92, 1168–1171. [Google Scholar] [CrossRef] [Green Version]
- American Heart Association Committee on Atherosclerosis Hypertension and Obesity in Youth of the Council on Cardiovascular Disease in the Young; Balagopal, P.B.; de Ferranti, S.D.; Cook, S.; Daniels, S.R.; Gidding, S.S.; Hayman, L.L.; McCrindle, B.W.; Mietus-Snyder, M.L.; Steinberger, J.; et al. Nontraditional risk factors and biomarkers for cardiovascular disease: Mechanistic, research, and clinical considerations for youth: A scientific statement from the American Heart Association. Circulation 2011, 123, 2749–2769. [Google Scholar] [CrossRef] [Green Version]
- Hermsdorff, H.H.M.; Zulet, M.Á.; Abete, I.; Martínez, J.A. Discriminated benefits of a Mediterranean dietary pattern within a hypocaloric diet program on plasma RBP4 concentrations and other inflammatory markers in obese subjects. Endocrine 2009, 36, 445–451. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (N = 115) | Intervention Group (N = 151) | p | ||
|---|---|---|---|---|
| Age, years | 42.5 ± 5.13 | 42.0 ± 5.26 | 0.483 | |
| Men, n (%) | 39 (33.9%) | 51 (33.5%) | 0.682 | |
| Baseline body weight, kg | 78.7 ± 17.5 | 80.1 ± 17.1 | 0.508 | |
| Baseline BMI, kg/m2 | 28.5 ± 5.75 | 28.9 ± 5.20 | 0.502 | |
| Baseline waist, cm | 96.4 ± 13.3 | 98.1 ± 12.8 | 0.293 | |
| Baseline total cholesterol, mg/dL | 202 ± 34.6 | 198 ± 34.6 | 0.326 | |
| Baseline LDL cholesterol, mg/dL | 127 ± 29.7 | 124 ± 29.4 | 0.365 | |
| Baseline triglycerides, mg/dL | 88.0 (31.0–118) | 80.0 (63.0–119) | 0.499 | |
| Baseline HDL cholesterol, mg/dL | 54.6 ± 12.7 | 53.7 ± 11.1 | 0.550 | |
| Baseline apolipoprotein A, mg/dL | 169 ± 32.5 | 167 ± 24.6 | 0.642 | |
| Baseline apolipoprotein B, mg/dL | 96.9 ± 23.9 | 95.9 ± 25.9 | 0.583 | |
| Baseline glucose, mg/dL | 92.4 ± 18.1 | 91.9 ± 15.4 | 0.621 | |
| Baseline insulin, UI | 6.04 ± 3.68 | 7.21 ± 4.81 | 0.027 | |
| Baseline HbA1c, % | 5.53 ± 0.75 | 5.51 ± 0.44 | 0.569 | |
| Baseline HOMA-IR | 1.35 ± 0.85 | 1.68 ± 1.30 | 0.045 | |
| Baseline GGT, U/L | 27.3± 20.5 | 27.1 ± 26.1 | 0.722 | |
| Baseline GOT, U/L | 20.8± 7.63 | 21.3 ± 6.60 | 0.211 | |
| Baseline GPT, U/L | 22.0 ± 14.9 | 20.3 ± 11.5 | 0.737 | |
| Baseline DM, n (%) | Prediabetes 1 | 10 (8.69%) | 12 (7.95%) | 0.776 |
| Diabetes 2 | 4 (3.48%) | 8 (5.26%) | ||
| Baseline score FINDRISK | 12.0 (10.0–13.0) | 11.0 (9.50–13.0) | 0.224 | |
| Baseline BCAA, nmol/nL | 406 ± 105 | 411 ± 113 | 0.745 | |
| Baseline RBP4, ng/ml | 7.09 ± 5.18 | 7.57 ± 5.12 | 0.327 | |
| Physical activity, steps/day | 6071 ± 3387 | 7082 ± 2756 | 0.364 | |
| Diabetic Subjects 1 (N = 12) | Prediabetic Subjects 2 (N = 22) | Normoglycemic Subjects (N = 232) | p | |
|---|---|---|---|---|
| Age, years | 43.5 ± 3.02 | 43.8 ± 5.23 | 42.0 ± 5.27 | 0.237 |
| Men, n (%) | 7 (58.3%) | 13 (59.1%) | 70 (30.2%) | 0.004 |
| Baseline body weight, kg | 89.9 ± 20.8 | 83.6 ± 15.2 | 78.6 ± 17.1 | 0.043 |
| Baseline BMI, kg/m2 | 32.1 ± 7.02 | 30.0 ± 4.37 | 28.5 ± 5.39 | 0.045 |
| Baseline waist, cm | 106 ± 19.4 | 100 ± 8.62 | 96.8 ± 12.9 | 0.062 |
| Baseline total cholesterol, mg/dL | 196 ± 41.3 | 210 ± 35.5 | 199 ± 34.1 | 0.357 |
| Baseline LDL cholesterol, mg/dL | 113 ± 32.6 | 133 ± 28.8 | 125 ± 29.4 | 0.183 |
| Baseline triglycerides, mg/dL | 126 (109–187) | 87.5 (70.5–169) | 81.0 (62.0–111) | 0.020 |
| Baseline HDL cholesterol, mg/dL | 49.4 ± 10.9 | 53.5 ± 9.62 | 54.4 ± 12.0 | 0.356 |
| Baseline glucose, mg/dL | 146 ± 43.1 | 106 ± 5.19 | 88.1 ± 6.44 | <0.001 |
| Baseline insulin, UI | 10.1 ± 7.09 | 7.49 ± 3.90 | 6.52 ± 4.29 | 0.104 |
| Baseline HbA1c, % | 7.24 ± 1.76 | 5.70 ±0.24 | 5.41 ± 0.29 | <0.001 |
| Baseline HOMA-IR | 3.15 ± 2.48 | 2.00 ± 1.16 | 1.44 ± 1.02 | 0.001 |
| Baseline BCAA, nmol/nL | 486 ± 114 | 435 ± 69.3 | 403 ± 111 | 0.018 |
| Baseline RBP4, ng/ml | 7.92 ± 3.55 | 8.24 ± 3.99 | 7.25 ± 5.31 | 0.192 |
| Physical activity, steps/day | 4291 ± 1293 | 6990 ± 3114 | 6930 ± 2947 | 0.466 |
| Control Group (N = 115) | Intervention Group (N = 151) | Overall p | |||||
|---|---|---|---|---|---|---|---|
| 2016 (N = 115) | 2017 (N = 115) | 2018 (N = 115) | 2016 (N = 151) | 2017 (N = 151) | 2018 (N = 151) | ||
| Men, n (%) | 39 (33.9%) | 39 (33.9%) | 39 (33.9%) | 51 (33.5%) | 51 (33.5%) | 51 (33.5%) | 0.682 |
| Body weight, kg | 78.7 ± 17.5 | 77.5 ± 16.0 * | 77.9 ± 16.4 | 80.1 ± 17.1 | 79.2 ± 16.7 * | 79.5 ± 16.8 | 0.638 |
| BMI, kg/m2 | 28.5 ± 5.75 | 28.3 ± 5.71 | 28.4 ± 5.77 | 28.9 ± 5.20 | 28.3 ± 5.23 * | 28.5 ± 5.21 | 0.703 |
| Total cholesterol, mg/dL | 202 ± 34.6 | 198 ± 35.1 | 196 ± 37.3 | 198 ± 34.6 | 196 ± 34.2 | 199 ± 34.1 | 0.068 |
| LDL cholesterol, mg/dL | 127 ± 29.7 | 122 ± 30.8 | 124 ± 34.5 | 124 ± 29.4 | 120 ± 27.8 | 124 ± 28.2 | 0.344 |
| Triglycerides, mg/dL | 88.0 (31.0–118) | 78.0 (61.0–111) * | 81.0 (57.5–119) ** | 80.0 (63.0–119) | 79.0 (60.5–116) | 84.0 (63.0–113) | 0.542 |
| HDL cholesterol, mg/dL | 54.6 ± 12.7 | 56.4 ± 13.0* | 54.6 ± 11.4 | 53.7 ± 11.1 | 56.4 ± 11.5* | 55.1 ± 11.8 ** | 0.089 |
| Apolipoprotein A, mg/dL | 169 ± 32.5 | 167 ± 28.6 | 144 ± 21.2 ** | 167 ± 24.6 | 172 ± 25.8* | 145 ± 20.0 ** | 0.334 |
| Apolipoprotein B, mg/dL | 96.9 ± 23.9 | 95.8 ± 21.9 | 88.1 ± 24.0 ** | 95.9 ± 25.9 | 94.9 ± 24.8 | 88.5 ± 21.1 ** | 0.264 |
| Glucose, mg/dL | 92.4 ± 18.1 | 95.6 ± 33.8 * | 92.6 ± 18.0 | 91.9 ± 15.4 | 93.0 ± 15.1 | 90.6 ± 11.7 | 0.417 |
| HbA1c, % | 5.53 ± 0.75 | 5.46 ± 0.81 * | 5.36 ± 0.33 ** | 5.51 ± 0.44 | 5.40 ± 0.53* | 5.36 ± 0.36 ** | 0.011 |
| GGT, U/L | 27.3± 20.5 | 27.0 ± 21.1 | 28.1 ± 26.4 | 27.1 ± 26.1 | 27.5 ± 25.0 | 26.3 ± 21.7 | 0.271 |
| GOT, U/L | 20.8± 7.63 | 21.8 ± 8.81 | 21.6 ± 8.81 | 21.3 ± 6.60 | 22.7 ± 9.45 | 21.4 ± 4.94 | 0.489 |
| GPT, U/L | 22.0 ± 14.9 | 22.4 ± 17.5 | 22.4 ± 17.5 | 20.3 ± 11.5 | 22.3 ± 15.2 | 22.3 ± 15.2 | 0.332 |
| BCAA, nmol/nL | 406 ± 105 | 400 ± 108 | 402 ± 103 | 411 ± 113 | 395 ± 86.8* | 363 ± 80.5 ** | <0.001 |
| RBP4, ng/mL | 7.09 ± 5.18 | 7.09 ±5.27 | 6.87 ± 5.09 | 7.57 ± 5.12 | 7.42 ± 4.83 | 7.76 ± 5.31 | 0.523 |
| Physical activity, steps/day | 4637 ± 2885 | 5544 ± 3433 | 6127 ± 3808 | 5601 ± 1834 | 5851 ± 2349 | 7208 ± 2543 | 0.273 |
| BCAA Variation | p | p1 | RBP4 Variation | p | p1 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 (N = 67) | Q2 (N = 66) | Q3 (N = 65) | Q4 (N = 68) | Q1 (N = 66) | Q2 (N = 66) | Q3 (N = 66) | Q4 (N = 68) | |||||
| BCAA variation, % | −28.3 ± 9.03 | −10.8 ± 3.79 | −0.42 ± 3.16 | 18.8 ± 12.4 | <0.001 | <0.001 | −2.13 ± 20.4 | −4.17 ± 18.4 | −9.11 ± 18.2 | −5.35 ± 18.5 | 0.194 | 0.343 |
| RBP4 variation, % | 22.8 ± 80.7 | 8.98 ± 55.7 | 15.4 ± 75.4 | 13.2 ± 60.6 | 0.706 | 0.440 | −41.5 ± 14.6 | −11.0 ± 6.62 | 16.7 ± 9.33 | 96.2 ± 90.0 | <0.001 | <0.001 |
| BMI variation, % | −0.79 ± 7.43 | −1.73 ± 8.37 | 0.34 ± 6.33 | 0.58 ± 5.33 | 0.201 | 0.224 | −0.60 ± 6.54 | −0.50 ± 6.11 | −0.36 ± 7.56 | −0.16 ± 7.68 | 0.987 | 0.731 |
| Body weight variation, % | −0.67 ± 7.58 | −1.37 ± 8.29 | 0.56 ± 5.12 | 0.63 ± 5.74 | 0.260 | 0.263 | −0.27 ± 6.68 | −0.33 ± 6.15 | −0.13 ± 7.71 | −0.11 ± 6.82 | 0.997 | 0.894 |
| Glucose variation, % | 0.25 ± 9.46 | −1.43 ± 11.2 | 0.20 ± 9.15 | 0.71 ± 9.86 | 0.624 | 0.785 | −0.63 ± 8.26 | 0.70 ± 9.98 | 1.11 ± 10.2 | −1.38 ± 11.1 | 0.437 | 0.654 |
| Hb1Ac variation, % | −1.33 ± 5.62 | −2.74 ± 3.41 | −1.65 ± 3.84 | −1.84 ± 3.56 | 0.263 | 0.537 | −1.79 ± 3.78 | −1.68 ± 2.98 | −1.41 ± 5.77 | −2.63 ± 3.87 | 0.379 | 0.209 |
| Vegetables variation consumption (g/week), % | 55.2 ± 179 | 52.5 ± 182 | 35.7 ± 166 | 55.3 ± 176 | 0.919 | 0.995 | 45.4 ± 172 | 67.5 ± 227 | 37.7 ± 160 | 47.2 ± 127 | 0.825 | 0.951 |
| Legume variation consumption (g/week), % | 49.3 ± 114 | 24.1 ± 105 | 88.6 ± 218 | 52.4 ± 144 | 0.216 | 0.907 | 46.2 ± 125 | 39.6 ± 149 | 39.0 ± 97.4 | 91.4 ± 216 | 0.292 | 0.227 |
| Read meat variation consumption (g/week), % | 2.21 ± 72.6 | -20.0 ± 62.3 | 52.3 ± 149 | 4.76 ± 73.4 | 0.002 | 0.862 | 10.4 ± 110 | 10.4 ± 75.4 | 10.7 ± 94.4 | 14.6 ± 121 | 0.996 | 0.856 |
| Fish variation consumption (g/week), % | 14.5 ± 72.1 | -2.88 ± 65.5 | 25.7 ± 123 | 39.4 ± 96.0 | 0.133 | 0.145 | 18.1 ± 69.2 | 23.0 ± 117 | 19.8 ± 97.8 | 19.7 ± 90.0 | 0.995 | 0.919 |
| Physical activity variation (number steps/day), % | 48.5 ± 64.9 | 14.9 ± 43.3 | 50.7 ± 65.6 | −18.9 ± 45.5 | 0.537 | 0.001 | 58.7 ± 78.9 | 18.7 ± 28.9 | 7.44 ± 41.2 | 18.0 ± 59.7 | 0.696 | <0.001 |
| Control Group | p2 | Intervention Group | p2 | |||||
|---|---|---|---|---|---|---|---|---|
| Subjects who Have Lost more than 5% of Weight throughout the F4D Study (N = 19) | Subjects who Have Varied less than 5% of Weight throughout the F4D Study (N = 78) | Subjects who Have Gained more than 5% of Weight throughout the F4D Study (N = 17) | Subjects who Have Lost more than 5% of Weight throughout the F4D Study (N = 21) | Subjects who Have Varied less than 5% of Weight throughout the F4D Study (N = 103) | Subjects who Have Gained more than 5% of Weight throughout the F4D Study (N = 24) | |||
| BCAA variation, % | −1.48 ± 17.2 | −0.11 ± 19.9 | 5.58 ± 16.8 | 0.493 | −10.9 ± 28.6 | −9.55 ± 15.3 | −7.14 ± 17.3 | 0.768 |
| RBP4 variation, % | 16.8 ± 73.4 | 10.9 ± 54.0 | 9.27 ± 36.3 | 0.904 | 44.2 ± 129 | 13.1 ± 51.8 | 24.2 ± 104 | 0.232 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamiquiz-Moneo, I.; Bea, A.M.; Palacios-Pérez, C.; De Miguel-Etayo, P.; González-Gil, E.M.; López-Ariño, C.; Civeira, F.; Moreno, L.A.; Mateo-Gallego, R. Effect of Lifestyle Intervention in the Concentration of Adipoquines and Branched Chain Amino Acids in Subjects with High Risk of Developing Type 2 Diabetes: Feel4Diabetes Study. Cells 2020, 9, 693. https://0-doi-org.brum.beds.ac.uk/10.3390/cells9030693
Lamiquiz-Moneo I, Bea AM, Palacios-Pérez C, De Miguel-Etayo P, González-Gil EM, López-Ariño C, Civeira F, Moreno LA, Mateo-Gallego R. Effect of Lifestyle Intervention in the Concentration of Adipoquines and Branched Chain Amino Acids in Subjects with High Risk of Developing Type 2 Diabetes: Feel4Diabetes Study. Cells. 2020; 9(3):693. https://0-doi-org.brum.beds.ac.uk/10.3390/cells9030693
Chicago/Turabian StyleLamiquiz-Moneo, Itziar, Ana M. Bea, Cristian Palacios-Pérez, Pilar De Miguel-Etayo, Esther M. González-Gil, Chuan López-Ariño, Fernando Civeira, Luis A. Moreno, and Rocio Mateo-Gallego. 2020. "Effect of Lifestyle Intervention in the Concentration of Adipoquines and Branched Chain Amino Acids in Subjects with High Risk of Developing Type 2 Diabetes: Feel4Diabetes Study" Cells 9, no. 3: 693. https://0-doi-org.brum.beds.ac.uk/10.3390/cells9030693