Double Hyperautofluorescent Rings in Patients with USH2A-Retinopathy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
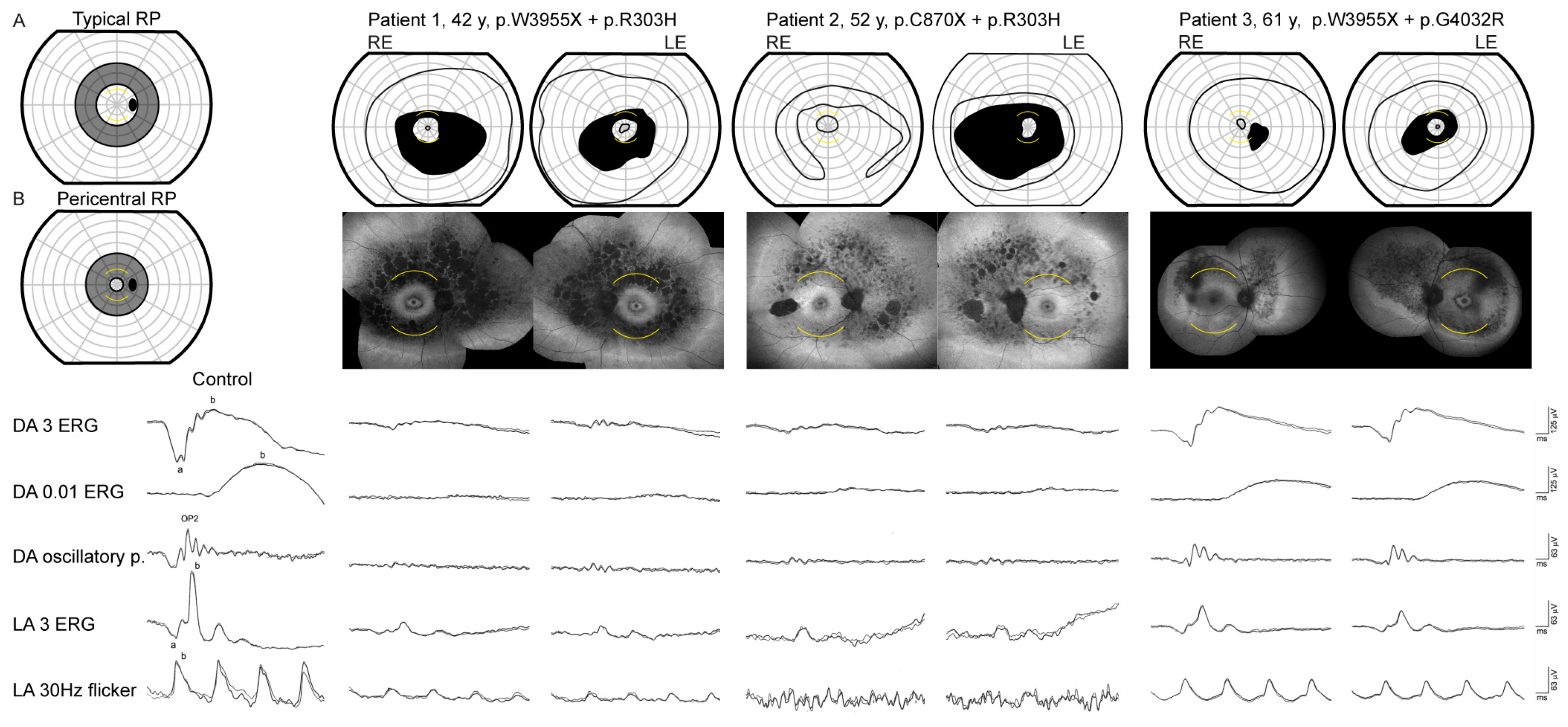
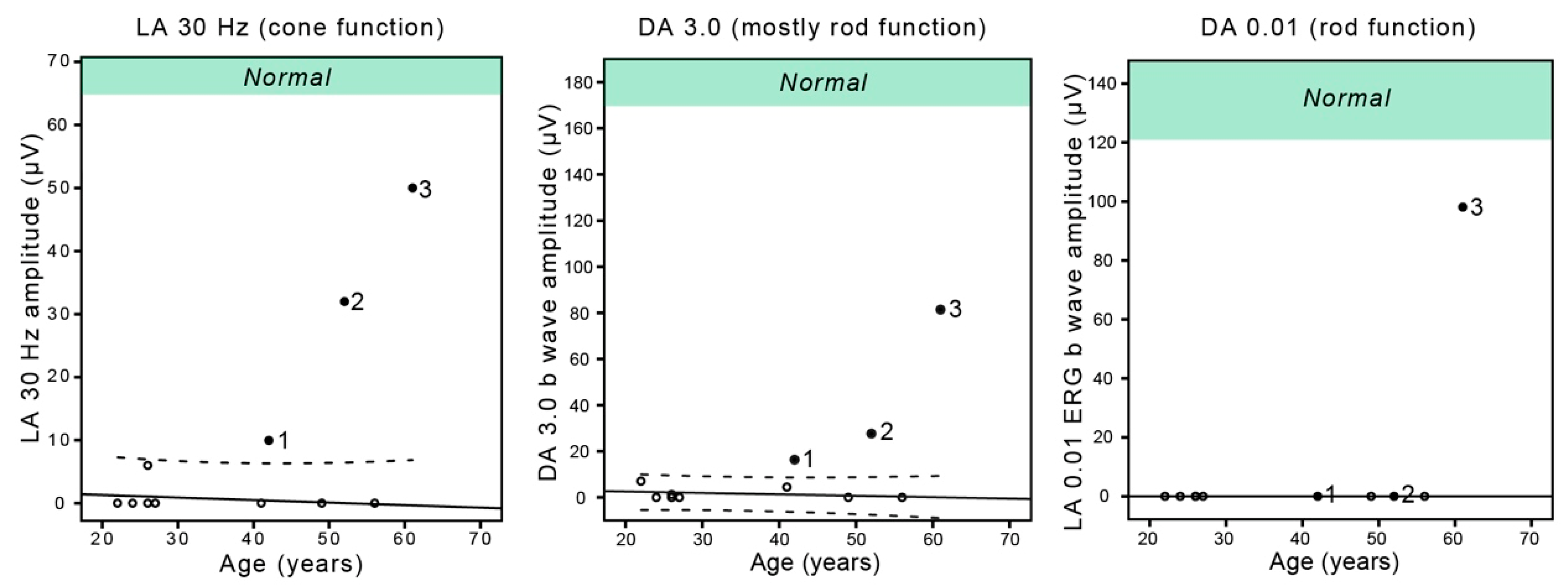
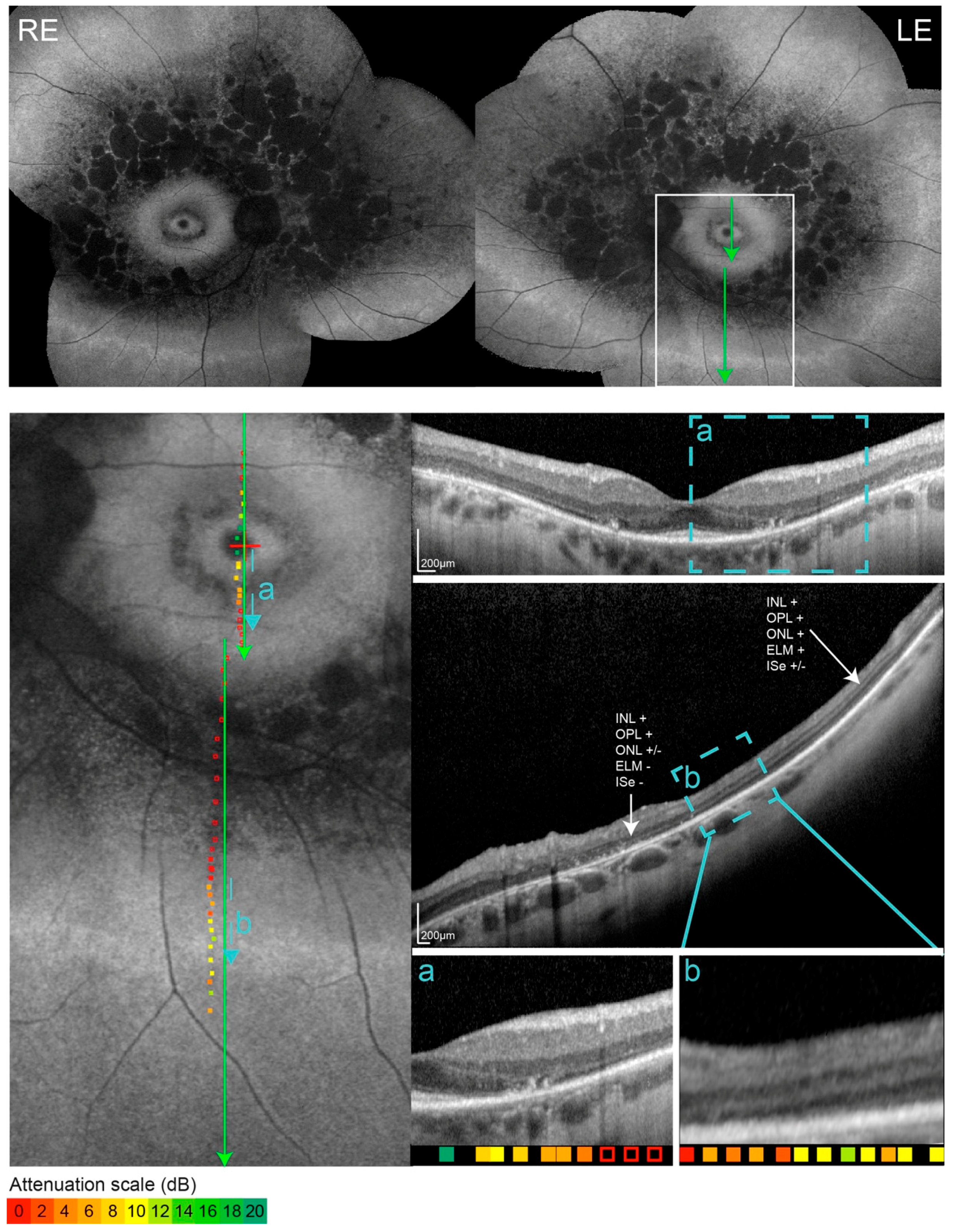
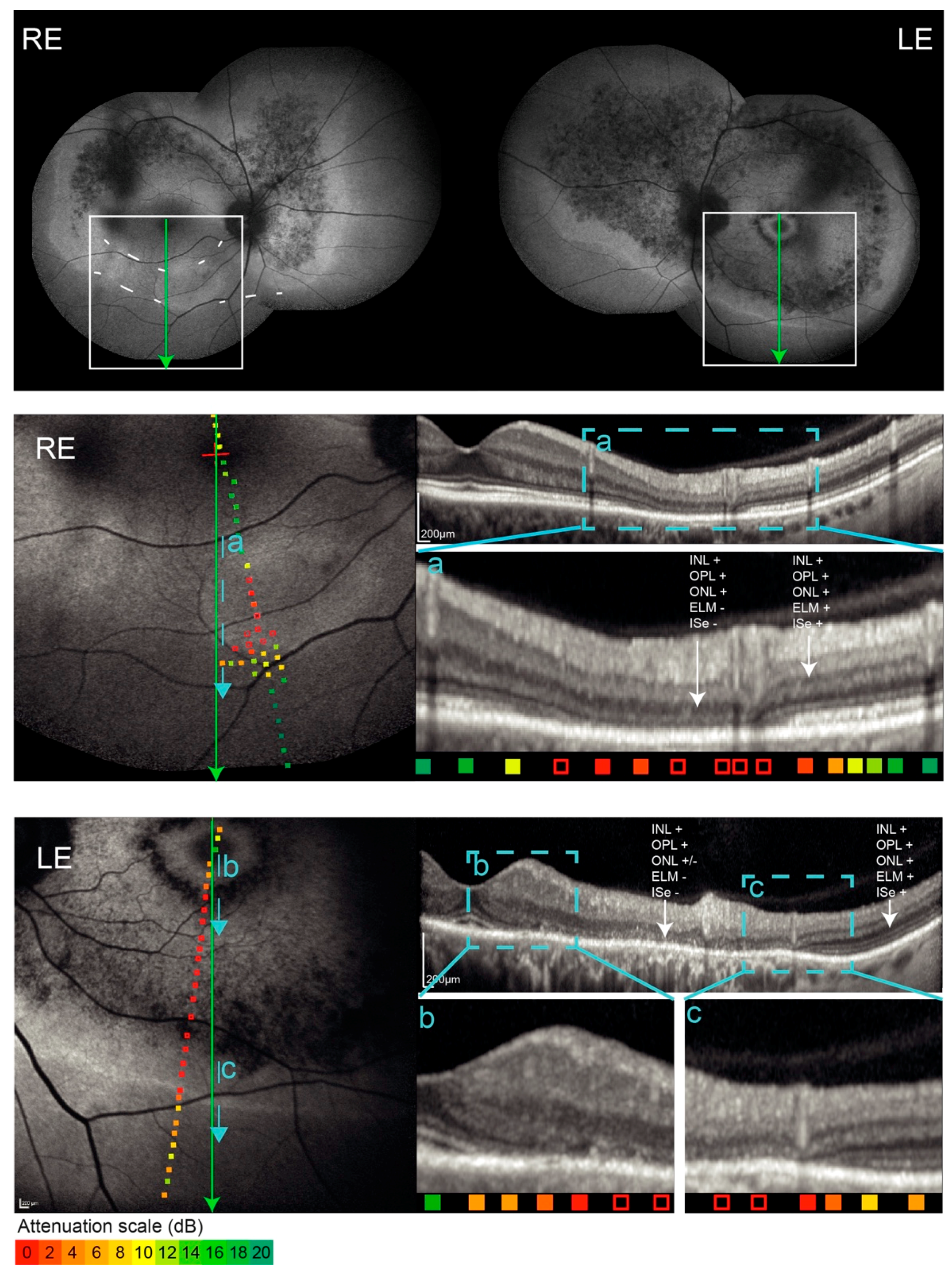
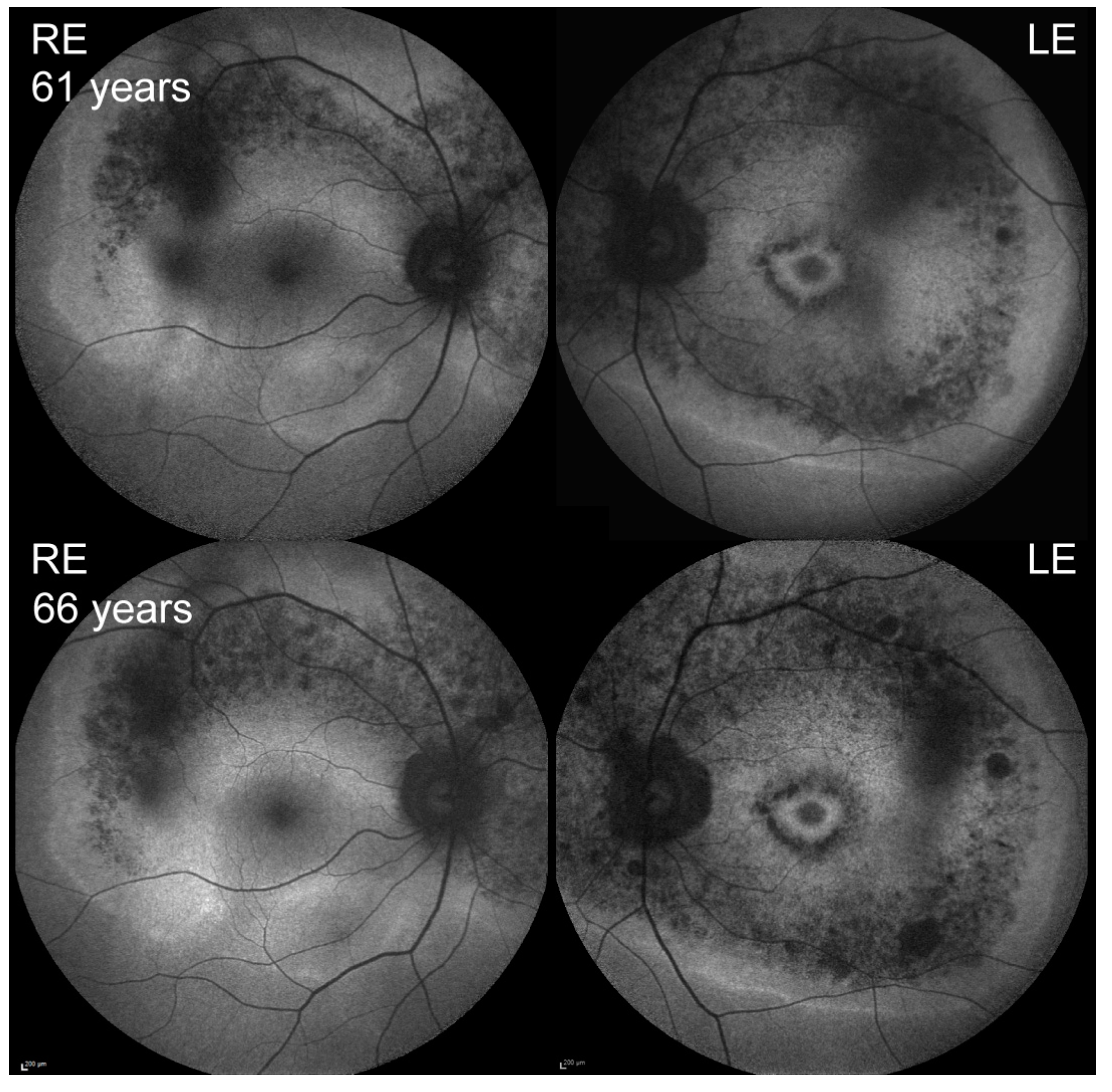
3.1. Clinical Findings in Patients with Double Hyperautofluorecent Rings
3.2. Comparison with the Patients with Single Hyperautofluorescent Rings
3.3. Genetic Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Verbakel, S.K.; van Huet, R.A.; Boon, C.J.; den Hollander, A.I.; Collin, R.W.; Klaver, C.C.; Hoyng, C.B.; Roepman, R.; Klevering, B.J. Non-syndromic retinitis pigmentosa. Progress Retin. Eye Res. 2018, 66, 57–186. [Google Scholar] [CrossRef] [PubMed]
- Malm, E.; Ponjavic, V.; Möller, C.; Kimberling, W.J.; Stone, E.S.; Andréasson, S. Alteration of rod and cone function in children with Usher syndrome. Eur. J. Ophthalmol. 2011, 21, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, M.A.; Rosner, B.; Weigel-DiFranco, C.; McGee, T.L.; Dryja, T.P.; Berson, E.L. Disease course in patients with autosomal recessive retinitis pigmentosa due to the USH2A gene. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5532–5539. [Google Scholar] [CrossRef] [PubMed]
- Hartong, D.T.; Berson, E.L.; Dryja, T.P. Retinitis pigmentosa. Lancet 2006, 68, 1795–1809. [Google Scholar] [CrossRef]
- Mendieta, L.; Berezovsky, A.; Salomão, S.R.; Sacai, P.Y.; Pereira, J.M.; Fantini, S.C. Visual acuity and full-field electroretinography in patients with Usher’s syndrome. Arq. Bras. Oftalmol. 2005, 68, 171–176. [Google Scholar] [CrossRef]
- Fakin, A.; Jarc-Vidmar, M.; Glavač, D.; Bonnet, C.; Petit, C.; Hawlina, M. Fundus autofluorescence and optical coherence tomography in relation to visual function in Usher syndrome type 1 and 2. Vis. Res. 2012, 75, 60–70. [Google Scholar] [CrossRef]
- McCulloch, D.L.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; Holder, G.E.; Tzekov, R.; Bach, M. ISCEV Standard for full-field clinical electroretinography (2015 update). Doc. Ophthalmol. 2015, 130, 1–12. [Google Scholar] [CrossRef]
- Bonnet, C.; Riahi, Z.; Chantot-Bastaraud, S.; Smagghe, L.; Letexier, M.; Marcaillou, C.; Lefèvre, G.M.; Hardelin, J.P.; El-Amraoui, A.; Singh-Estivalet, A.; et al. An innovative strategy for the molecular diagnosis of Usher syndrome identifies causal biallelic mutations in 93% of European patients. Eur. J. Hum. Genet. 2016, 24, 1730–1738. [Google Scholar] [CrossRef]
- Sandberg, M.A.; Gaudio, A.R.; Berson, E.L. Disease course of patients with pericentral retinitis pigmentosa. Am. J. Ophthalmol. 2005, 140, 100–106. [Google Scholar] [CrossRef]
- Lima, L.H.; Cella, W.; Greenstein, V.C.; Wang, N.K.; Busuioc, M.; Smith, R.T.; Yannuzzi, L.A.; Tsang, S.H. Structural assessment of hyperautofluorescent ring in patients with retinitis pigmentosa. Retina 2009, 29, 1025–1031. [Google Scholar] [CrossRef]
- Delori, F.C.; Delori, F.C.; Dorey, C.K.; Staurenghi, G.; Arend, O.; Goger, D.G.; Weiter, J.J. In vivo fluorescence of the ocular fundus exhibits retinal pigment epithelium lipofuscin characteristics. Investig. Ophthalmol. Vis. Sci. 1995, 36, 718–729. [Google Scholar]
- Sparrow, J.R.; Yoon, K.D.; Wu, Y.; Yamamoto, K. Interpretations of fundus autofluorescence from studies of the bisretinoids of the retina. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4351–4357. [Google Scholar] [CrossRef] [PubMed]
- Cottet, S.; Schorderet, D.F. Mechanisms of apoptosis in retinitis pigmentosa. Curr. Mol. Med. 2009, 9, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Maeda, A.; Maeda, T.; Golczak, M.; Palczewski, K. Retinopathy in mice induced by disrupted all-trans-retinal clearance. J. Biol. Chem. 2008, 283, 26684–26693. [Google Scholar] [CrossRef] [PubMed]
- Robson, A.G.; Michaelides, M.; Saihan, Z.; Bird, A.C.; Webster, A.R.; Moore, A.T.; Fitzke, F.W.; Holder, G.E. Functional characteristics of patients with retinal dystrophy that manifest abnormal parafoveal annuli of high density fundus autofluorescence; a review and update. Doc. Ophthalmol. 2008, 116, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Lenassi, E.; Vincent, A.; Li, Z.; Saihan, Z.; Coffey, A.J.; Steele-Stallard, H.B.; Moore, A.T.; Steel, K.P.; Luxon, L.M.; Héon, E.; et al. A detailed clinical and molecular survey of subjects with nonsyndromic USH2A retinopathy reveals an allelic hierarchy of disease-causing variants. Eur. J. Hum. Genet. 2015, 23, 1318–1327. [Google Scholar] [CrossRef]
- Murakami, T.; Akimoto, M.; Ooto, S.; Suzuki, T.; Ikeda, H.; Kawagoe, N.; Takahashi, M.; Yoshimura, N. Association between abnormal autofluorescence and photoreceptor disorganization in retinitis pigmentosa. Am. J. Ophthalmol. 2008, 145, 687–694. [Google Scholar] [CrossRef]
- Robson, A.G.; Egan, C.A.; Luong, V.A.; Bird, A.C.; Holder, G.E.; Fitzke, F.W. Comparison of fundus autofluorescence with photopic and scotopic fine-matrix mapping in patients with retinitis pigmentosa and normal visual acuity. Invest. Ophthalmol. Vis. Sci. 2004, 45, 4119–4125. [Google Scholar] [CrossRef]
- Robson, A.G.; El-Amir, A.; Bailey, C.; Egan, C.A.; Fitzke, F.W.; Webster, A.R.; Bird, A.C.; Holder, G.E. Pattern ERG correlates of abnormal fundus autofluorescence in patients with retinitis pigmentosa and normal visual acuity. Investig. Ophthalmol. Vis. Sci. 2003, 44, 3544–3550. [Google Scholar] [CrossRef]
- Popovic, P.; Jarc-Vidmar, M.; Hawlina, M. Abnormal fundus autofluorescence in relation to retinal function in patients with retinitis pigmentosa. Graefes Arch. Clin. Exp. Ophthalmol. 2005, 243, 1018–1027. [Google Scholar] [CrossRef]
- Escher, P.; Tran, H.V.; Vaclavik, V.; Borruat, F.X.; Schorderet, D.F.; Munier, F.L. Double concentric autofluorescence ring in NR2E3-p.G56R-linked autosomal dominant retinitis pigmentosa. Investig. Ophthalmol. Vis. Sci. 2012, 53, 4754–4764. [Google Scholar] [CrossRef] [PubMed]
- Coppieters, F.; Leroy, B.P.; Beysen, D.; Hellemans, J.; De Bosscher, K.; Haegeman, G.; Robberecht, K.; Wuyts, W.; Coucke, P.J.; De Baere, E. Recurrent mutation in the first zinc finger of the orphan nuclear receptor NR2E3 causes autosomal dominant retinitis pigmentosa. Am. J. Hum. Genet. 2007, 81, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Matsui, R.; Cideciyan, A.V.; Schwartz, S.B.; Sumaroka, A.; Roman, A.J.; Swider, M.; Huang, W.C.; Sheplock, R.; Jacobson, S.G. Molecular Heterogeneity Within the Clinical Diagnosis of Pericentral Retinal Degeneration. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6007–6018. [Google Scholar] [CrossRef] [PubMed]
- Comander, J.; Weigel-DiFranco, C.; Maher, M.; Place, E.; Wan, A.; Harper, S.; Sandberg, M.; Navarro-Gomez, D.; Pierce, E. The Genetic Basis of Pericentral Retinitis Pigmentosa-A Form of Mild Retinitis Pigmentosa. Genes 2017, 8, 256. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Fishman, G.A.; Brown, J., Jr. Patterns of visual field progression in patients with retinitis pigmentosa. Ophthalmology 1998, 105, 1069–1075. [Google Scholar] [CrossRef]
- Fishman, G.A.; Bozbeyoglu, S.; Massof, R.W.; Kimberling, W. Natural course of visual field loss in patients with Type 2 Usher syndrome. Retina 2007, 27, 601–608. [Google Scholar] [CrossRef]
- Garcia-Garcia, G.; Aparisi, M.J.; Jaijo, T.; Rodrigo, R.; Leon, A.M.; Avila-Fernandez, A.; Blanco-Kelly, F.; Bernal, S.; Navarro, R.; Diaz-Llopis, M.; et al. Mutational screening of the USH2A gene in Spanish USH patients reveals 23 novel pathogenic mutations. Orphanet J. Rare Dis. 2011, 6, 65. [Google Scholar] [CrossRef]
- Yan, D.; Ouyang, X.; Patterson, D.M.; Du, L.L.; Jacobson, S.G.; Liu, X.Z. Mutation analysis in the long isoform of USH2A in American patients with Usher Syndrome type II. J. Hum. Genet. 2009, 54, 732–738. [Google Scholar] [CrossRef]
- Cartegni, L.; Chew, S.L.; Krainer, A.R. Listening to silence and understanding nonsense: Exonic mutations that affect splicing. Nat. Rev. Genet. 2002, 3, 285–298. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
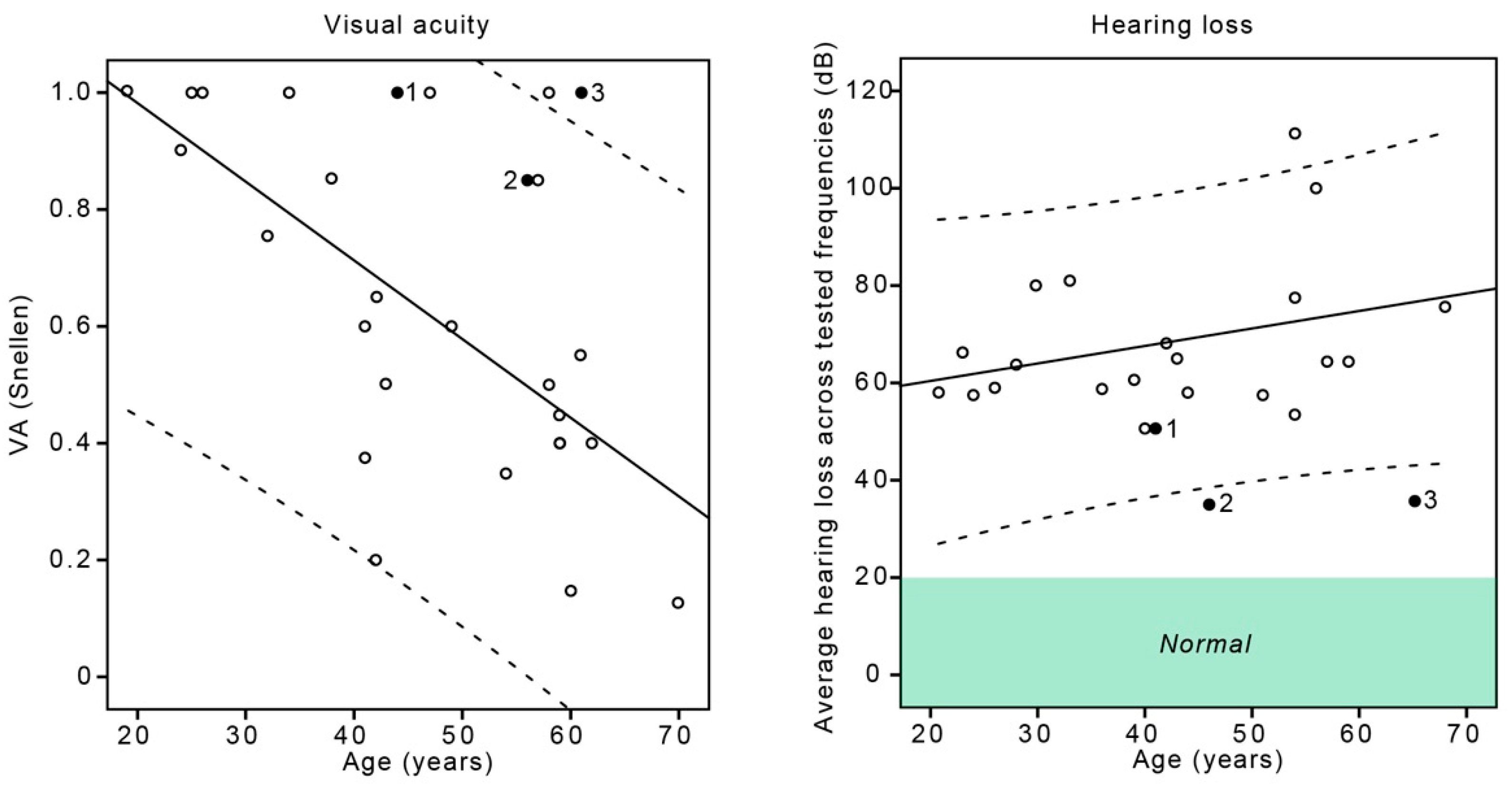
| ID | USH2A Alleles | Sex | Age (Years) | Onset (Years) | BCVA; R, L | ERG | Hearing Loss # (dB); R, L (Age) |
|---|---|---|---|---|---|---|---|
| 1 | p.Trp3955Ter, p.Arg303His | M | 42 | 18 | 1.0, 1.0 | rod-cone dystrophy | 56, 45 (41) |
| 2 | p.Cys870Ter, p.Arg303His | F | 52 | 22 | 0.8, 0.9 | rod-cone dystrophy | 34, 36 (46) |
| 3 | p.Trp3955Ter, p.Gly4032Arg | F | 61 | 58 | 1.0, 1.0 | cone-rod dystrophy | 31, 40 (65) |
| N | USH2A Alleles | Sex | Age (Years) | Onset (Years) | BCVA | ERG | Hearing Loss # (dB) |
|---|---|---|---|---|---|---|---|
| 24 | 75% (18/24) null + null; 25% (6/24) null + missense | 12 M, 12 F | median 45, range 19–70 | median 19, range 6–42 | median 0.6, range 0.1–1.0 | rod-cone dystrophy in 8/8 performed, at the median age of 27 y | Median 64 dB, range 51–111 dB) in 21 performed, at the median age of 42 y * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fakin, A.; Šuštar, M.; Brecelj, J.; Bonnet, C.; Petit, C.; Zupan, A.; Glavač, D.; Jarc-Vidmar, M.; Battelino, S.; Hawlina, M. Double Hyperautofluorescent Rings in Patients with USH2A-Retinopathy. Genes 2019, 10, 956. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10120956
Fakin A, Šuštar M, Brecelj J, Bonnet C, Petit C, Zupan A, Glavač D, Jarc-Vidmar M, Battelino S, Hawlina M. Double Hyperautofluorescent Rings in Patients with USH2A-Retinopathy. Genes. 2019; 10(12):956. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10120956
Chicago/Turabian StyleFakin, Ana, Maja Šuštar, Jelka Brecelj, Crystel Bonnet, Christine Petit, Andrej Zupan, Damjan Glavač, Martina Jarc-Vidmar, Saba Battelino, and Marko Hawlina. 2019. "Double Hyperautofluorescent Rings in Patients with USH2A-Retinopathy" Genes 10, no. 12: 956. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10120956