Meeting the Challenge of Eliminating Chronic Hepatitis B Infection


1
Victorian Infectious Diseases Reference Laboratory, Royal Melbourne Hospital at the Peter Doherty Institute for Infection and Immunity, Melbourne 3000, Australia
2
Department of Microbiology and Immunology, University of Melbourne at the Peter Doherty Institute for Infection and Immunity, Melbourne 3000, Australia
3
Directorate, Peter Doherty Institute for Infection and Immunity, Melbourne 3000, Australia
4
University of South Florida, Tampa, FL 33612, USA
5
Romark Laboratory, Tampa, FL 33607, USA
6
Global Virus Network, Baltimore, MD 21201-1009, USA
7
INSERM Unit 1052—Cancer Research Center of Lyon, 69000 Lyon, France
*
Author to whom correspondence should be addressed.
Genes 2019, 10(4), 260; https://0-doi-org.brum.beds.ac.uk/10.3390/genes10040260
Submission received: 14 December 2018
/
Revised: 29 January 2019
/
Accepted: 1 February 2019
/
Published: 1 April 2019
(This article belongs to the Special Issue Hepatitis B Virus Infection: An Update on Epidemiology, Diagnosis, Treatment and Prevention)
Abstract
:Over 257 million people live with chronic hepatitis B virus (HBV) infection and there is no known cure. The effective preventative vaccine has no impact on existing infection. Despite the existence of drugs which efficiently suppress viral replication, treatment is usually life-long and finite therapies that cure HBV infection are urgently required. However, even if such therapies were available today, it is unlikely they would reach all of those who need it most, due to chronic hepatitis B (CHB) being largely undiagnosed across the globe and to the dire need for health systems promoting access to therapy. Considerable challenges to developing and implementing an effective HBV cure remain. Nonetheless, important advances towards a cure are being made, both in the development of a multitude of new therapeutic agents currently undergoing clinical trials, and through the establishment of a new global initiative dedicated to an HBV cure, ICE-HBV, that is working together with existing organisations to fast-track an HBV cure available to all.
1. Background
Today, over 1.3 billion people show evidence of past hepatitis B virus (HBV) infection, with 257 million people having progressed to chronic hepatitis B (CHB), which directly contributes to the deaths of over 880,000 people annually [1]. This public health catastrophe is made worse by the absence of effective curative interventions [2,3]. There are currently only two approaches to therapy-direct acting antivirals (DAAs) and interferon. Current DAA (nucleos(t)ide analogues (NUCs)) therapies reduce viral replication, but have minimal impact on the nuclear viral reservoir of covalently closed circular DNA (cccDNA) present in the nucleus of infected hepatocytes as a histone-bound mini-chromosome, which contributes heavily to viral persistence [2,3,4]. Also, they show no effect on integrated viral sequences which contribute to continued hepatitis B surface antigen (HBsAg) expression as well as to HBV-related carcinogenicity. Thus, they do not promote a “functional cure,” which is currently defined as hepatitis B surface antigen loss (plus or minus the production of anti-HBs) [2,3,5]. In contrast, the current “gold-standard” for immune-mediated therapy, pegylated interferon alpha (IFN-α), may result in a functional cure (hepatitis B surface antigen (HBsAg) loss) [2,5], but only in a minor proportion of recipients, with treatment response highly variable across HBV genotypes [6,7].
The inability of current therapies to induce a functional cure means that patients are invariably committed to life-long therapy. With the presence of a highly effective prophylactic vaccine, if finite curative regimens were to be developed and effectively distributed to all persons living with CHB, CHB could rapidly be eliminated as a global public health challenge. This review discusses some of the obstacles associated with meeting this admirable goal as well as describing a new collaborative approach to fast-track an HBV cure, recently instigated by the international HBV research community.
2. A New Global Initiative Promoting Hepatitis B Cure
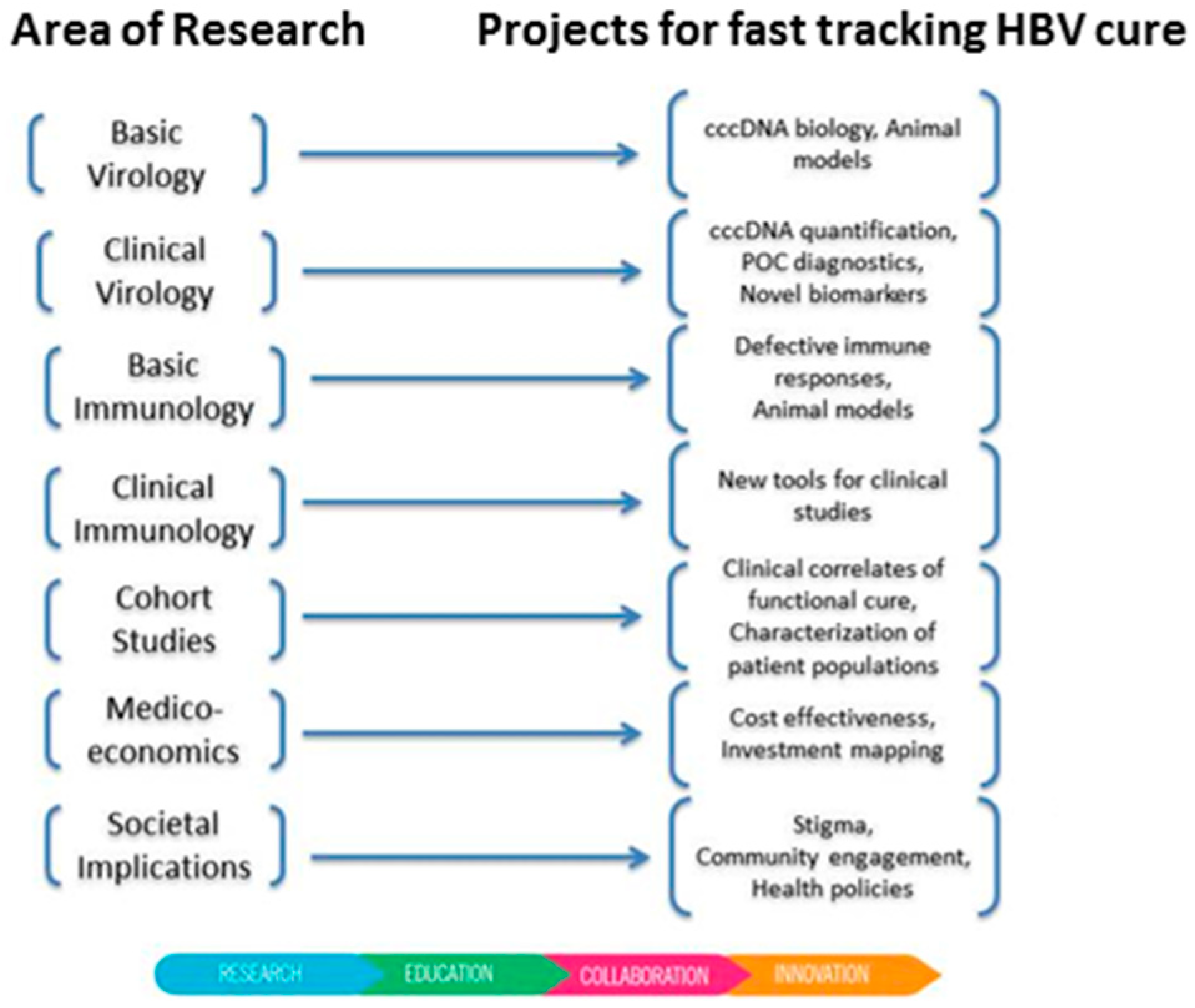
The International Coalition to Eliminate Hepatitis B (ICE-HBV) (https://ice-hbv.org/) was formed in 2016 following a call to promote global collaboration in HBV cure research [2]. ICE-HBV aims to fast-track the discovery of a safe, effective, affordable and scalable cure to benefit all people living with CHB, including children and people living with hepatitis C virus (HCV), hepatitis D virus (HDV) and HIV co-infection. This will be achieved by generating knowledge, fostering collaborations and performing research to accelerate scientific innovation in collaboration with key stakeholders around the globe. ICE-HBV works with stakeholders to ensure the timely translation of discoveries into positive health outcomes and quality of life for people living with hepatitis B. Following an in-depth gap analysis, researchers leading ICE-HBV have developed a comprehensive multidisciplinary scientific roadmap for HBV cure research as a position paper for publication in early 2019. On this basis, new international collaborations have been formed in the following fields: cccDNA quantification standards, mathematical modelling of HBV cure, health systems strengthening and health policy research for HBV elimination as well as community engagement and literacy. The Coalition is now recognized as a key player in hepatitis research by the World Health Organisation (WHO) [8] and others. Next steps include the development of public–private partnerships with industry and foundations to accelerate HBV cure research, answer key research questions and fill gaps through new research projects about animal models, serum biomarkers, point-of-care assays, HBV research global investments mapping and a research protocols online repository (Figure 1). Each of these projects is designed in collaboration with key stakeholders. ICE-HBV supports the community of people living with hepatitis, particularly in recent calls from the Hepatitis B Foundation to increase HBV cure research and funding in the USA [9]. These stakeholders also include the World Hepatitis Alliance and the World Health Organisation, who collaborate with ICE-HBV to ensure that ICE-HBV’s actions align with and complement their goals to eliminate chronic HBV as a public health challenge by 2030 through universal vaccine coverage including providing a birth-dose, “finding the missing millions” of people that are undiagnosed, enabling increased access to therapy and promoting the development of finite cure regimens.
3. Hepatitis B Virus Life Cycle
HBV virions enter hepatocytes via the sodium-taurocholate co-transporting polypeptide (NTCP) receptor [10], where HBV virions de-envelope and the HBV DNA genome is transported to the nucleus, where it is converted to the highly stable cccDNA episome [11,12,13]. This molecule interacts with host histones to form a minichromosome, which is the transcription template for the expression of viral mRNAs, including the major transcriptional pregenomic RNA (pgRNA) template. Following encapsidation within viral nucleocapsids, pgRNA is reverse transcribed to minus then plus sense DNA, forming a relaxed circular partially double-stranded DNA molecule (RC DNA) which is then enveloped to form virions that egress from the cell. Alternatively, nucleocapsids may also be transported to the nucleus whereby RC DNA may be converted to form additional cccDNA molecules. The absence of proofreading in the viral RNA-dependent DNA polymerase (reverse transcriptase) means that errors in reverse transcription are not corrected, leading to a large quasispecies pool of HBV variants, which may in turn emerge as the dominant virus depending on selection pressures. Examples include the emergence of drug-resistant variants during lamivudine therapy [14] and precore/basal core promoter variants that emerge during hepatitis B virus e antigen seroconversion [15]. pgRNA may also undergo splicing, resulting in numerous smaller-than-genome-length molecules that are reverse-transcribed in trans and packaged into virions [16,17]. Although thought not to be critical for HBV replication, some HBV “splice variants” are associated with increased pathogenesis, including liver cancer [16,18,19,20,21].
4. Barriers to Hepatitis B Virus Cure
Difficulties in targeting the HBV cccDNA reservoir means that much of the current emphasis from pharmaceutical companies and academia in identifying new targets and developing CHB curative regimens lies in developing agents which target other steps of the HBV replication cycle. These include siRNA molecules which target HBV mRNAs [22,23], capsid inhibitors [24,25,26] which disrupt capsid assembly or inhibit the packaging of the viral pregenomic RNA (pgRNA) intermediate, nucleic acid polymers (NAPS) that prevent the egress of viral subviral particles [27,28] and more potent reverse transcriptase/polymerase inhibitors [29,30]. Other direct acting antiviral approaches include entry inhibitors which prevent viral entry [31] via the NTCP [10] receptor, the development of RNAse H inhibitors [32]. Approaches directly targeting HBV cccDNA, such as CRISPR-CAS9 [33,34] and TALENS [35,36] are also being tested, however, challenges associated with potential off-target effects and delivery to the infected hepatocyte must be overcome if these latter approaches are to reach the clinic. Novel direct acting antiviral approaches currently undergoing clinical trial are shown in Table 1. One of the further challenges associated with developing approaches to target cccDNA to date has been the absence of standardised methods for cccDNA detection and quantification. We applaud recent global collaborative efforts to standardise cccDNA detection and quantification through the ICE-HBV cccDNA harmonization project (Figure 1). As it is becoming increasingly difficult to obtain liver samples for analysis from HBV patients, the development of serum biomarkers which accurately represent cccDNA activity will be increasingly required.
5. Clinical Advances towards Hepatitis B Virus Cure
It is likely that an eventual HBV curative regimen will require the combination of two or more of these approaches, either DAAs alone or in combination with approaches that stimulate innate and/or adaptive immune responses. For an up-to-date description of antivirals at different stages of clinical development, the reader is encouraged to regularly consult the Hepatitis B Foundation’s drug watch website [41]. A summary of current clinical trials, drawn from the Hepatitis B Foundation’s drug watch and the Clinical.trial.gov [42] websites, is presented in Table 1. These include RNAi approaches, HBV entry inhibitors, capsid inhibitors, HBsAg inhibitors and activators of innate immune responses.
In addition, Bristol Myers Squib recently concluded a Phase I/II trial on the checkpoint inhibitor Nivolumab in advanced hepatocellular carcinoma [45]. A number of these patients had chronic HBV infection. Transgene completed a Phase 1b trial on the safety and immunogenicity of their therapeutic vaccine TG1050 in nuc-suppressed CHB patients (NCT02428400; AASLD poster 426, San Francisco, 2018).
6. Further Challenges
Chronic hepatitis B is not a “one size fits all” disease, with striking differences in HBV natural history, disease progression and even treatment response across the globe [6,7,46,47,48]. For example, in Asia genotype C is usually associated with more progressive liver disease than genotype B, and in the western world, genotype D is usually associated with more progressive disease than genotype A. However, in Africa and India, genotype A (subtype A1) is associated with rapid progression to liver cancer in African male teenagers [49,50,51]. Indigenous Australians infected with the C4 subtype are six times more likely to have CHB than non-Indigenous Australians [52,53]. Differences in genotype also extend to treatment response, with genotype A patients responding best to IFN-α treatment and genotype D patients responding the least [6,7]. Recent in vitro studies have suggested that this may be more due to host differences rather than HBV genotype differences per se [54], with cell type rather than HBV genotype contributing most to IFN-α response. Differences have also been observed in DAA therapy, with a recent study showing that genotype A and D patients receiving the DAA tenofovir were significantly more likely to achieve a functional cure than genotype B and C patients [15,55]. Whether genotype-associated differences in treatment response are due to the virus, host, duration of infection, other factors or a combination thereof remains to be elucidated. However, it is essential that any curative regimen is pan-genotypic, to be effective in as many people living with CHB as possible.
7. Finding the Missing Millions
We endorse the “Find the Missing Millions” campaign recently initiated by The World Hepatitis Alliance (WHA) [56] to identify all persons living with chronic viral hepatitis, as well as the goals of the World Health Organisation to ensure that antiviral therapy reaches 50% of CHB patients worldwide by 2030. It is estimated that currently only 10% of the world’s population were diagnosed and 5% of people eligible for treatment were receiving it in 2016 [57]. Treatment rates are extraordinarily low even in western countries, reaching 8% in Australia in 2017 [58]. Of major importance to increasing diagnosis rates will be the development of point-of-care tests that enable the accurate detection of HBsAg and DNA in field applications at a limited cost. To date, two HBsAg POC test have received WHO precertification [59]. Pan-genotypic POC tests that function equally well in Africa, America, Asia, Alaska, Australia and Europe are urgently required. If a future cure is to be restricted to some stages of CHB natural history, a POC test identifying immune correlates of liver disease will also be required.
8. Conclusions
There has never been more interest amongst the HBV research community, public health organisations, pharmaceutical companies and the HBV-affected community in the development of an effective HBV cure. Collaborative approaches such as those fostered by ICE-HBV in partnership with the International HBV Meeting [60], WHO [61], WHA [43], The Coalition for the Eradication of Viral Hepatitis in Asia Pacific (CEVHAP) [44] and the broader HBV-affected community will be critical to achieving this goal as soon as possible.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Hepatitis B Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs204/en/ (accessed on 10 December 2018).
- Revill, P.; Testoni, B.; Locarnini, S.; Zoulim, F. Global strategies are required to cure and eliminate HBV infection. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Zeisel, M.B.; Lucifora, J.; Mason, W.S.; Sureau, C.; Beck, J.; Levrero, M.; Kann, M.; Knolle, P.A.; Benkirane, M.; Durantel, D.; et al. Towards an HBV cure: State-of-the-art and unresolved questions—Report of the ANRS workshop on HBV cure. Gut 2015, 64, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Zoulim, F.; Testoni, B.; Lebosse, F. Kinetics of intrahepatic covalently closed circular DNA and serum hepatitis B surface antigen during antiviral therapy for chronic hepatitis B: Lessons from experimental and clinical studies. Clin. Gastroenterol. Hepatol. 2013, 11, 1011–1013. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.; Zoulim, F.; Dusheiko, G.; Ghany, M.G. Hepatitis B cure: From discovery to regulatory approval. Hepatology 2017, 66, 1296–1313. [Google Scholar] [CrossRef] [PubMed]
- Kramvis, A. Genotypes and genetic variability of hepatitis B virus. Intervirology 2014, 57, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Revill, P.A.; Ahn, S.H. HBV genotypes: Relevance to natural history, pathogenesis and treatment of chronic hepatitis B. Antivir. Ther. 2011, 16, 1169–1186. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: Finding a Cure for Hepatitis B: Are We Close? Available online: https://protect-au.mimecast.com/s/HVSYCvl0E5unJwJWHQC44B?domain=who.int (accessed on 10 December 2018).
- Alter, H.; Block, T.M.; Brown, N.; Brownstein, A.; Brosgart, C.; Chang, K.M.; Chen, P.J.; Chisari, F.V.; Cohen, C.; El-Serag, H.; et al. A Research Agenda for Curing Chronic Hepatitis B Virus Infection. Hepatology 2017. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Zhong, G.; Xu, G.; He, W.; Jing, Z.; Gao, Z.; Huang, Y.; Qi, Y.; Peng, B.; Wang, H.; et al. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. eLife 2012, 1, e00049. [Google Scholar] [CrossRef]
- Nassal, M. HBV cccDNA: Viral persistence reservoir and key obstacle for a cure of chronic hepatitis B. Gut 2015, 64, 1972–1984. [Google Scholar] [CrossRef]
- Newbold, J.E.; Xin, H.; Tencza, M.; Sherman, G.; Dean, J.; Bowden, S.; Locarnini, S. The covalently closed duplex form of the hepadnavirus genome exists in situ as a heterogeneous population of viral minichromosomes. J. Virol. 1995, 69, 3350–3357. [Google Scholar]
- Bock, C.T.; Schwinn, S.; Locarnini, S.; Fyfe, J.; Manns, M.P.; Trautwein, C.; Zentgraf, H. Structural organization of the hepatitis B virus minichromosome. J. Mol. Biol. 2001, 307, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Zoulim, F.; Locarnini, S. Hepatitis B virus resistance to nucleos(t)ide analogues. Gastroenterology 2009, 137, 1593–1608. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, J.; Yuen, L.; Rosenberg, G.; Wong, D.; Littlejohn, M.; Jackson, K.; Gaggar, A.; Kitrinos, K.M.; Subramanian, G.M.; Marcellin, P.; et al. Deep sequencing shows that HBV basal core promoter and precore variants reduce the likelihood of HBsAg loss following tenofovir disoproxil fumarate therapy in HBeAg-positive chronic hepatitis B. Gut 2016. [Google Scholar] [CrossRef] [PubMed]
- Soussan, P.; Pol, J.; Garreau, F.; Schneider, V.; Le Pendeven, C.; Nalpas, B.; Lacombe, K.; Bonnard, P.; Pol, S.; Kremsdorf, D. Expression of defective hepatitis B virus particles derived from singly spliced RNA is related to liver disease. J. Infect. Dis. 2008, 198, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Soussan, P.; Garreau, F.; Zylberberg, H.; Ferray, C.; Brechot, C.; Kremsdorf, D. In vivo expression of a new hepatitis B virus protein encoded by a spliced RNA. J. Clin. Invest. 2000, 105, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Redelsperger, F.; Lekbaby, B.; Mandouri, Y.; Giang, E.; Duriez, M.; Desire, N.; Roque Afonso, A.M.; Brichler, S.; Dubreuil, P.; Dobrin, A.; et al. Production of hepatitis B defective particles is dependent on liver status. Virology 2012, 431, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Soussan, P.; Tuveri, R.; Nalpas, B.; Garreau, F.; Zavala, F.; Masson, A.; Pol, S.; Brechot, C.; Kremsdorf, D. The expression of hepatitis B spliced protein (HBSP) encoded by a spliced hepatitis B virus RNA is associated with viral replication and liver fibrosis. J. Hepatol. 2003, 38, 343–348. [Google Scholar] [CrossRef]
- Bayliss, J.; Lim, L.; Thompson, A.J.; Desmond, P.; Angus, P.; Locarnini, S.; Revill, P.A. Hepatitis B virus splicing is enhanced prior to development of hepatocellular carcinoma. J. Hepatol. 2013, 59, 1022–1028. [Google Scholar] [CrossRef]
- Pan, M.-H.; Hu, H.-H.; Mason, H.; Bayliss, J.; Littlejohn, M.; Lin, Y.-L.; Su, C.-Y.; Chiang, C.-T.; Chen, C.-J.; Locarnini, S.; et al. Hepatitis B splice variants are strongly associated with and are indeed predictive of hepatocellular carcinoma. J. Hepatol. 2018, 68, 474–475. [Google Scholar] [CrossRef]
- Wooddell, C.I.; Yuen, M.F.; Chan, H.L.; Gish, R.G.; Locarnini, S.A.; Chavez, D.; Ferrari, C.; Given, B.D.; Hamilton, J.; Kanner, S.B.; et al. RNAi-based treatment of chronically infected patients and chimpanzees reveals that integrated hepatitis B virus DNA is a source of HBsAg. Sci. Transl. Med. 2017, 9, eaan0241. [Google Scholar] [CrossRef]
- Thi, E.P.; Dhillon, A.P.; Ardzinski, A.; Bidirici-Ertekin, L.; Cobarrubias, K.D.; Cuconati, A.; Kondratowicz, A.S.; Kwak, K.; Li, A.H.L.; Miller, A.; et al. ARB-1740, a RNA Interference Therapeutic for Chronic Hepatitis B Infection. ACS Infect. Dis. 2018. [Google Scholar] [CrossRef] [PubMed]
- Klumpp, K.; Lam, A.M.; Lukacs, C.; Vogel, R.; Ren, S.; Espiritu, C.; Baydo, R.; Atkins, K.; Abendroth, J.; Liao, G.; et al. High-resolution crystal structure of a hepatitis B virus replication inhibitor bound to the viral core protein. Proc. Natl. Acad. Sci. USA 2015, 112, 15196–15201. [Google Scholar] [CrossRef] [PubMed]
- Klumpp, K.; Shimada, T.; Allweiss, L.; Volz, T.; Lutgehetmann, M.; Hartman, G.; Flores, O.A.; Lam, A.M.; Dandri, M. Efficacy of NVR 3-778, Alone and In Combination With Pegylated Interferon, vs. Entecavir In uPA/SCID Mice With Humanized Livers and HBV Infection. Gastroenterology 2018, 154, 652–662. [Google Scholar] [CrossRef]
- Lam, A.M.; Espiritu, C.; Vogel, R.; Ren, S.; Lau, V.; Kelly, M.; Kuduk, S.D.; Hartman, G.D.; Flores, O.A.; Klumpp, K. Preclinical Characterization of NVR 3-778, a First-in-Class Capsid Assembly Modulator against Hepatitis B Virus. Antimicrob. Agents Chemother. 2019, 63, e01734-18. [Google Scholar] [CrossRef] [PubMed]
- Bazinet, M.; Pantea, V.; Cebotarescu, V.; Cojuhari, L.; Jimbei, P.; Albrecht, J.; Schmid, P.; Le Gal, F.; Gordien, E.; Krawczyk, A.; et al. Safety and efficacy of REP 2139 and pegylated interferon alfa-2a for treatment-naive patients with chronic hepatitis B virus and hepatitis D virus co-infection (REP 301 and REP 301-LTF): A non-randomised, open-label, phase 2 trial. Lancet Gastroenterol. Hepatol. 2017, 2, 877–889. [Google Scholar] [CrossRef]
- Roehl, I.; Seiffert, S.; Brikh, C.; Quinet, J.; Jamard, C.; Dorfler, N.; Lockridge, J.A.; Cova, L.; Vaillant, A. Nucleic Acid Polymers with Accelerated Plasma and Tissue Clearance for Chronic Hepatitis B Therapy. Mol. Nucleic Acids 2017, 8, 1–12. [Google Scholar] [CrossRef]
- Agarwal, K.; Brunetto, M.; Seto, W.K.; Lim, Y.S.; Fung, S.; Marcellin, P.; Ahn, S.H.; Izumi, N.; Chuang, W.L.; Bae, H.; et al. 96weeks treatment of tenofovir alafenamide vs. tenofovir disoproxil fumarate for hepatitis B virus infection. J. Hepatol. 2018, 68, 672–681. [Google Scholar] [CrossRef]
- Cathcart, A.L.; Chan, H.L.; Bhardwaj, N.; Liu, Y.; Marcellin, P.; Pan, C.Q.; Shalimar; Buti, M.; Cox, S.; Parhy, B.; et al. No Resistance to Tenofovir Alafenamide Detected through 96 Weeks of Treatment in Patients with Chronic Hepatitis B Infection. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef]
- Petersen, J.; Dandri, M.; Mier, W.; Lutgehetmann, M.; Volz, T.; von Weizsacker, F.; Haberkorn, U.; Fischer, L.; Pollok, J.M.; Erbes, B.; et al. Prevention of hepatitis B virus infection in vivo by entry inhibitors derived from the large envelope protein. Nat. Biotechnol. 2008, 26, 335–341. [Google Scholar] [CrossRef]
- Long, K.R.; Lomonosova, E.; Li, Q.; Ponzar, N.L.; Villa, J.A.; Touchette, E.; Rapp, S.; Liley, R.M.; Murelli, R.P.; Grigoryan, A.; et al. Efficacy of hepatitis B virus ribonuclease H inhibitors, a new class of replication antagonists, in FRG human liver chimeric mice. Antivir. Res. 2018, 149, 41–47. [Google Scholar] [CrossRef]
- Schiwon, M.; Ehrke-Schulz, E.; Oswald, A.; Bergmann, T.; Michler, T.; Protzer, U.; Ehrhardt, A. One-Vector System for Multiplexed CRISPR/Cas9 against Hepatitis B Virus cccDNA Utilizing High-Capacity Adenoviral Vectors. Mol. Therapy. Nucleic Acids 2018, 12, 242–253. [Google Scholar] [CrossRef]
- Song, J.; Zhang, X.; Ge, Q.; Yuan, C.; Chu, L.; Liang, H.F.; Liao, Z.; Liu, Q.; Zhang, Z.; Zhang, B. CRISPR/Cas9-mediated knockout of HBsAg inhibits proliferation and tumorigenicity of HBV-positive hepatocellular carcinoma cells. J. Cell. Biochem. 2018, 119, 8419–8431. [Google Scholar] [CrossRef]
- Joung, J.K.; Sander, J.D. TALENs: A widely applicable technology for targeted genome editing. Nat. Reviews. Mol. Cell Biol. 2013, 14, 49–55. [Google Scholar] [CrossRef]
- Bloom, K.; Ely, A.; Mussolino, C.; Cathomen, T.; Arbuthnot, P. Inactivation of hepatitis B virus replication in cultured cells and in vivo with engineered transcription activator-like effector nucleases. Mol. Ther. 2013, 21, 1889–1897. [Google Scholar] [CrossRef]
- Wieland, S.F.; Chisari, F.V. Stealth and cunning: Hepatitis B and hepatitis C viruses. J. Virol. 2005, 79, 9369–9380. [Google Scholar] [CrossRef]
- Cheng, X.; Xia, Y.; Serti, E.; Block, P.D.; Chung, M.; Chayama, K.; Rehermann, B.; Liang, T.J. Hepatitis B virus evades innate immunity of hepatocytes but activates cytokine production by macrophages. Hepatology 2017, 66, 1779–1793. [Google Scholar] [CrossRef] [PubMed]
- Wieland, D.; Hofmann, M.; Thimme, R. Overcoming CD8+ T-Cell Exhaustion in Viral Hepatitis: Lessons from the Mouse Model and Clinical Perspectives. Dig. Dis. 2017, 35, 334–338. [Google Scholar] [CrossRef]
- Burton, A.R.; Pallett, L.J.; McCoy, L.E.; Suveizdyte, K.; Amin, O.E.; Swadling, L.; Alberts, E.; Davidson, B.R.; Kennedy, P.T.; Gill, U.S.; et al. Circulating and intrahepatic antiviral B cells are defective in hepatitis B. J. Clin. Invest. 2018, 128, 4588–4603. [Google Scholar] [CrossRef]
- Hepatitis B Foundation: Drug Watch. Available online: http://www.hepb.org/treatment-and-management/drug-watch (accessed on 22 January 2019).
- ClinicalTrials.gov: Home. Available online: https://clinicaltrials.gov (accessed on 22 January 2019).
- World Hepatitis Alliance. Available online: http://www.worldhepatitisalliance.org/ (accessed on 10 December 2018).
- CEVHAP. Available online: http://www.cevhap.org /index.php/en/ (accessed on 10 December 2018).
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H.R.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Kramvis, A.; Kew, M.; Francois, G. Hepatitis B virus genotypes. Vaccine 2005, 23, 2409–2423. [Google Scholar] [CrossRef]
- Kramvis, A.; Kew, M.C. Relationship of genotypes of hepatitis B virus to mutations, disease progression and response to antiviral therapy. J. Viral Hepat. 2005, 12, 456–464. [Google Scholar] [CrossRef]
- Sozzi, V.; Walsh, R.; Littlejohn, M.; Colledge, D.; Jackson, K.; Warner, N.; Yuen, L.; Locarnini, S.A.; Revill, P.A. In Vitro Studies Show that Sequence Variability Contributes to Marked Variation in Hepatitis B Virus Replication, Protein Expression, and Function Observed across Genotypes. J. Virol. 2016, 90, 10054–10064. [Google Scholar] [CrossRef]
- Kew, M.C.; Kramvis, A.; Yu, M.C.; Arakawa, K.; Hodkinson, J. Increased hepatocarcinogenic potential of hepatitis B virus genotype A in Bantu-speaking sub-saharan Africans. J. Med. Virol. 2005, 75, 513–521. [Google Scholar] [CrossRef]
- Kramvis, A.; Kew, M.C. Epidemiology of hepatitis B virus in Africa, its genotypes and clinical associations of genotypes. Hepatol. Res. 2007, 37, S9–S19. [Google Scholar] [CrossRef] [PubMed]
- Kramvis, A.; Kew, M.C. Molecular characterization of subgenotype A1 (subgroup Aa) of hepatitis B virus. Hepatol. Res. 2007, 37, S27–S32. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Littlejohn, M.; Locarnini, S.A.; Whiting, S.; Hajkowicz, K.; Cowie, B.C.; Bowden, D.S.; Tong, S.Y.; Davis, J.S. Molecular epidemiology of hepatitis B in the Indigenous people of northern Australia. J. Gastroenterol. Hepatol. 2013, 28, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Littlejohn, M.; Davies, J.; Yuen, L.; Edwards, R.; Sozzi, T.; Jackson, K.; Cowie, B.; Tong, S.; Davis, J.; Locarnini, S. Molecular virology of hepatitis B virus, sub-genotype C4 in northern Australian Indigenous populations. J. Med. Virol. 2014, 86, 695–706. [Google Scholar] [CrossRef]
- Shen, F.; Li, Y.; Wang, Y.; Sozzi, V.; Revill, P.A.; Liu, J.; Gao, L.; Yang, G.; Lu, M.; Sutter, K.; et al. Hepatitis B virus sensitivity to interferon-alpha in hepatocytes is more associated with cellular interferon response than with viral genotype. Hepatology 2018, 67, 1237–1252. [Google Scholar] [CrossRef]
- Marcellin, P.; Heathcote, E.J.; Buti, M.; Gane, E.; de Man, R.A.; Krastev, Z.; Germanidis, G.; Lee, S.S.; Flisiak, R.; Kaita, K.; et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N. Engl. J. Med. 2008, 359, 2442–2455. [Google Scholar] [CrossRef]
- The World Alliance Hepatitis. Available online: http://www.worldhepatitisalliance.org/find-missing-millions (accessed on 10 December 2018).
- Polaris Observatory, C. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: A modelling study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar]
- HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: Annual Surveillance Report 2018. Available online: https://kirby.unsw.edu.au/report/hiv-viral-hepatitis-and-sexually-transmissible-infections-australia-annual-surveillance (accessed on 10 December 2018).
- World Health Organization, Public Reports of WHO prequalified IVDs. Available online: https://www.who.int/diagnostics_laboratory/evaluations/pq-list/hiv-rdts/public_report/en/ (accessed on 10 December 2018).
- International HBV Meeting. Available online: www.hbvmeeting.org/ (accessed on 10 December 2018).
- World Health Organization. Available online: www.who.int (accessed on 10 December 2018).
Figure 1.
Current and future International Coalition to Eliminate Hepatitis B (ICE-HBV) projects to fast-track a hepatitis B virus (HBV) cure.
Figure 1.
Current and future International Coalition to Eliminate Hepatitis B (ICE-HBV) projects to fast-track a hepatitis B virus (HBV) cure.


{kind=link}
Table 1.
Current clinical trials of new hepatitis B virus (HBV) therapies (Phases I/II and II).
| Approach | Name/Type | Company | Status |
|---|---|---|---|
| Silencing HBV RNAs | RNAi gene silencer (1.0) | Arrowhead Pharma | NCT03365947 (R) |
| HBV Locked Nucleic Acid (LNA) RO7062931 | Roche | NCT03038113 (R) NCT03505190 (R) | |
| SiRNA VIR-2218 | Alnylam and Vir Biotech | NCT03672188 (R) | |
| Liquid nano-particle (LNP) RNAi (ARB-1462) | Arbutus Biopharma | Phase 2 (IMPACT study) | |
| Antisense Molecules | IONIS-HBVRx (GSK3228836) (GSK33389404) | IONIS/GSK | NCT02981602 (R) NCT03020745 (R) |
| Entry inhibitor | Myrcludex B | Myr-pharma | NCT02888106 Recruiting hepatitis delta virus HDV/HBV coinfected patients |
| Capsid Inhibitors | GLS4 | HEC Pharma | NCT03638076 (R) |
| JNJ 56136379 | Janssen Sciences | NCT03439488 (R) NCT03361956 (R) | |
| ABI-H0731 | Assembly Biosciences | NCT03714152 (R) | |
| RO7049389 | Roche | NCT 02952924 (R) NCT 03570658 (R) NCT 03717064 (A) | |
| AB-506 | Arbutus Biopharma | Phase 1a studies completed | |
| HBsAg Inhibitors | REP 2139/2165 | Replicor, Canada | NCT02565719 (A) NCT02876419 (A) |
| TLR7 Antagonist | JNJ-64794964 (AL-034) | Janssen Sciences | NCT03285620 (R) |
| RO7020531 | Roche | NCT02956850 (R) NCT03530917 (R) | |
| TLR8 Antagonist | GS-9688 | Gilead, USA | NCT03615066 (R) |
| Innate Immune Activators | Inarigavir RIG-I agonist (also an HBV replication inhibitor). | Springbank Pharmaceuticals | NCT02751996 (R) |
| Immune Therapy | HBsAg monoclonal antibody | Green Cross | NCT03519113 (R) |
| Therapeutic DNA Vaccine | JNJ-64300535 | Janssen Sciences | NCT03463369 (R) |
| Undisclosed | RO7239958 | Roche | NCT03762681 Not yet recruiting |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Revill, P.A.; Penicaud, C.; Brechot, C.; Zoulim, F. Meeting the Challenge of Eliminating Chronic Hepatitis B Infection. Genes 2019, 10, 260. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10040260
AMA Style
Revill PA, Penicaud C, Brechot C, Zoulim F. Meeting the Challenge of Eliminating Chronic Hepatitis B Infection. Genes. 2019; 10(4):260. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10040260
Chicago/Turabian StyleRevill, Peter A., Capucine Penicaud, Christian Brechot, and Fabien Zoulim. 2019. "Meeting the Challenge of Eliminating Chronic Hepatitis B Infection" Genes 10, no. 4: 260. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10040260
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.