
Influence of Renal Impairment and Genetic Subtypes on Warfarin Control in Japanese Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Settings
2.2. Evaluation of Demographics
2.3. Genetic Subtyping
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
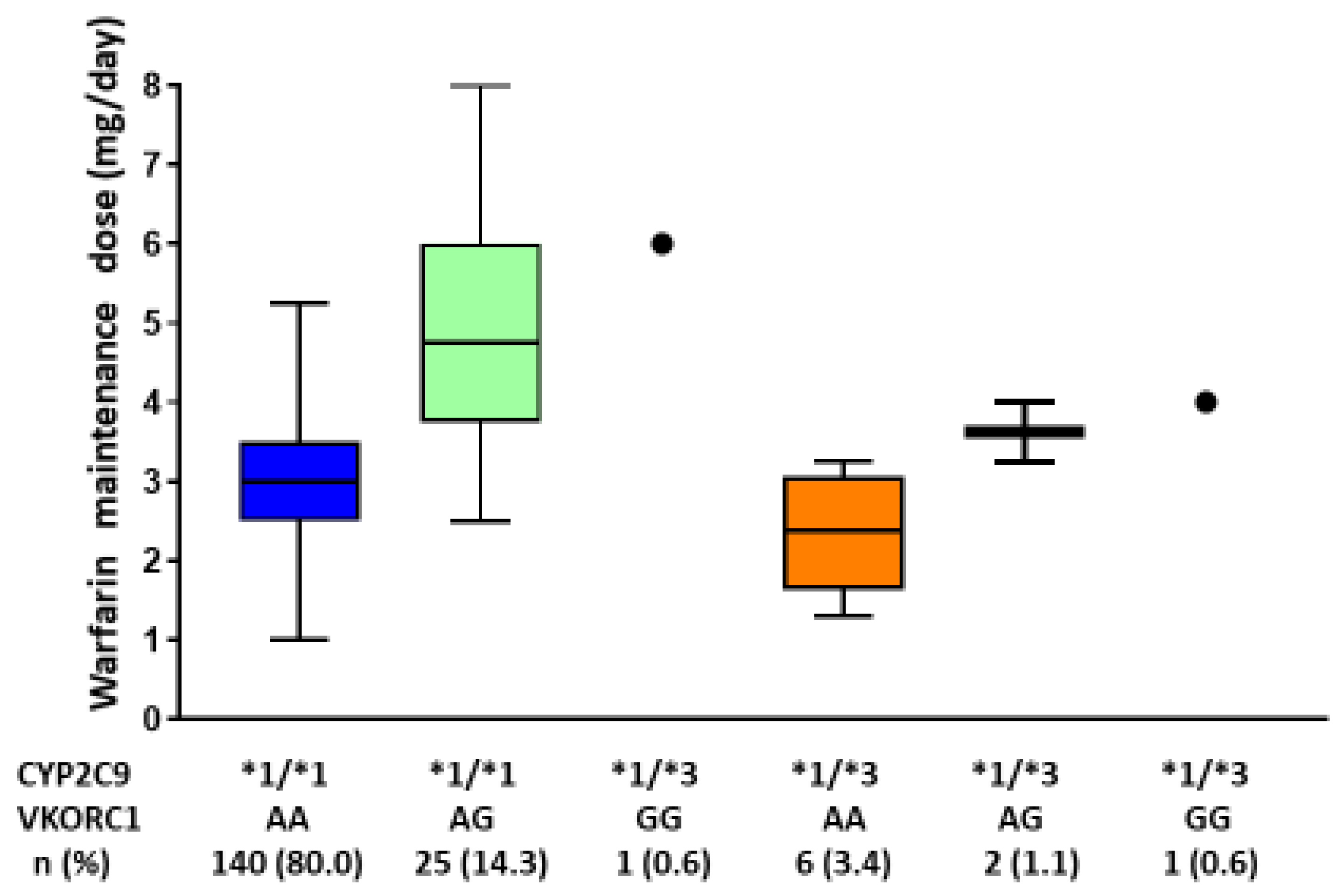
3.2. The Genotypes of CYP2C9 and VKORC1 and Their Associations with the Warfarin Maintenance Dose
3.3. Relationship between the Warfarin Maintenance Dose and the eGFR
3.4. Determining the Factors Associated with the Warfarin Maintenance Dose
3.5. Pharmacogenetics-Guided Warfarin Dosing Algorithm for Predicting the Therapeutic Dose
(/10 mL/min/1.73 m2) + 1.886 × VC2 † − 1.164 × VC3 ‡ + 0.601 × VC4 ¶ + 0.011 × VK
(/10 µg/day) − 0.021 × AST (IU/L) + 0.186 × drinking
- VC2 †: CYP2C9 *1/*1, VKORC1 (-1639G>A) GA or GG
- VC3 ‡: CYP2C9 *1/*3, VKORC1 (-1639G>A) AA
- VC4 ¶: CYP2C9 *1/*3, VKORC1 (-1639G>A) GA or GG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klein, T.E.; Altman, R.B.; Eriksson, N.; Gage, B.F.; Kimmel, S.E.; Lee, M.-T.M.; Limdi, N.A.; Page, D.; Roden, D.M.; Wagner, M.J.; et al. Estimation of the warfarin dose with clinical and pharmacogenetic data. N. Engl. J. Med. 2009, 360, 753–764. [Google Scholar] [CrossRef] [PubMed]
- Cavallari, L.H.; Limdi, N.A. Warfarin pharmacogenomics. Curr. Opin. Mol. Ther. 2009, 11, 243–251. [Google Scholar] [PubMed]
- Oldenburg, J.; Bevans, C.G.; Fregin, A.; Geisen, C.; Muller-Reible, C.; Watzka, M. Current pharmacogenetic developments in oral anticoagulation therapy: The influence of variant VKORC1 and CYP2C9 alleles. Thromb. Haemost. 2007, 98, 570–578. [Google Scholar]
- Wittkowsky, A.K.; Devine, E.B. Frequency and causes of overanticoagulation and underanticoagulation in patients treated with warfarin. Pharmacotherapy 2004, 24, 1311–1316. [Google Scholar] [CrossRef] [PubMed]
- Visser, L.E.; van Schaik, R.H.; van Vliet, M.; Trienekens, P.H.; De Smet, P.A.; Vulto, A.G.; Hofman, A.; van Duijn, C.M.; Stricker, B.H. The risk of bleeding complications in patients with cytochrome P450 CYP2C9*2 or CYP2C9*3 alleles on acenocoumarol or phenprocoumon. Thromb. Haemost. 2004, 92, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Gage, B.F.; Lesko, L.J. Pharmacogenetics of warfarin: Regulatory, scientific, and clinical issues. J. Thromb. Thrombolysis 2008, 25, 45–51. [Google Scholar] [CrossRef]
- Caldwell, M.D.; Awad, T.; Johnson, J.A.; Gage, B.F.; Falkowski, M.; Gardina, P.; Hubbard, J.; Turpaz, Y.; Langaee, T.Y.; Eby, C.; et al. CYP4F2 genetic variant alters required warfarin dose. Blood 2008, 111, 4106–4112. [Google Scholar] [CrossRef] [Green Version]
- Rieder, M.J.; Reiner, A.P.; Rettie, A.E. Gamma-glutamyl carboxylase (GGCX) tagSNPs have limited utility for predicting warfarin maintenance dose. J. Thromb. Haemost. 2007, 5, 2227–2234. [Google Scholar] [CrossRef]
- Dhabali, A.A.; Awang, R.; Zyoud, S.H. Clinically important drug-drug interactions in primary care. J. Clin. Pharm. Ther. 2012, 37, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Asiimwe, I.G.; Zhang, E.J.; Osanlou, R.; Jorgensen, A.L.; Pirmohamed, M. Warfarin dosing algorithms: A systematic review. Br. J. Clin. Pharmacol. 2021, 87, 1717–1729. [Google Scholar] [CrossRef] [PubMed]
- Limdi, N.A.; Wadelius, M.; Cavallari, L.; Eriksson, N.; Crawford, D.C.; Lee, M.T.; Chen, C.H.; Motsinger-Reif, A.; Sagreiya, H.; Liu, N.; et al. Warfarin pharmacogenetics: A single VKORC1 polymorphism is predictive of dose across 3 racial groups. Blood 2010, 115, 3827–3834. [Google Scholar] [CrossRef]
- Yin, T.; Miyata, T. Warfarin dose and the pharmacogenomics of CYP2C9 and VKORC1-rationale and perspectives. Thromb. Res. 2007, 120, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Miao, L.; Yang, J.; Huang, C.; Shen, Z. Contribution of age, body weight, and CYP2C9 and VKORC1 genotype to the anticoagulant response to warfarin: Proposal for a new dosing regimen in Chinese patients. Eur. J. Clin. Pharmacol. 2007, 63, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Kimura, R.; Miyashita, K.; Kokubo, Y.; Akaiwa, Y.; Otsubo, R.; Nagatsuka, K.; Otsuki, T.; Okayama, A.; Minematsu, K.; Naritomi, H.; et al. Genotypes of vitamin K epoxide reductase, gamma-glutamyl carboxylase, and cytochrome P450 2C9 as determinants of daily warfarin dose in Japanese patients. Thromb. Res. 2007, 120, 181–186. [Google Scholar] [CrossRef]
- Dani, M.; Boisvert, C.; Michaud, J.; Naud, J.; Lefrancois, S.; Leblond, F.A.; Pichette, V. Down-regulation of liver drug-metabolizing enzymes in a murine model of chronic renal failure. Drug Metab. Dispos. 2010, 38, 357–360. [Google Scholar] [CrossRef] [Green Version]
- Limdi, N.A.; Beasley, T.M.; Baird, M.F.; Goldstein, J.A.; McGwin, G.; Arnett, D.K.; Acton, R.T.; Allon, M. Kidney function influences warfarin responsiveness and hemorrhagic complications. J. Am. Soc. Nephrol. 2009, 20, 912–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, X.; Kuang, Y.; Yang, G.; Xie, J.; Miao, D.; Guo, C.; Huang, Z. Influence of renal insufficiency on anticoagulant effects and safety of warfarin in Chinese patients: Analysis from a randomized controlled trial. Naunyn. Schmiedebergs. Arch. Pharmacol. 2021, 394, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Canga, Y.; Guvenc, T.S.; Calik, A.N.; Karatas, M.B.; Akdeniz, E.; Yuksel, G.; Emre, A. Renal function in patients with mechanical prosthetic valves: Long-term effects of anticoagulation and over-anticoagulation with warfarin. Wien. Klin. Wochenschr. 2018, 130, 436–445. [Google Scholar] [CrossRef]
- Shaw, P.B.; Donovan, J.L.; Tran, M.T.; Lemon, S.C.; Burgwinkle, P.; Gore, J. Accuracy assessment of pharmacogenetically predictive warfarin dosing algorithms in patients of an academic medical center anticoagulation clinic. J. Thromb. Thrombolysis 2010, 30, 220–225. [Google Scholar] [CrossRef]
- Du Bois, D.; Du Bois, E.F. A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition 1989, 5, 303–311, discussion 312–303. [Google Scholar]
- Ishihara, J.; Inoue, M.; Kobayashi, M.; Tanaka, S.; Yamamoto, S.; Iso, H.; Tsugane, S.; Group, J.F.V.S. Impact of the revision of a nutrient database on the validity of a self-administered food frequency questionnaire (FFQ). J. Epidemiol. 2006, 16, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Nasu, K.; Kubota, T.; Ishizaki, T. Genetic analysis of CYP2C9 polymorphism in a Japanese population. Pharmacogenetics 1997, 7, 405–409. [Google Scholar] [CrossRef]
- Harada, T.; Ariyoshi, N.; Shimura, H.; Sato, Y.; Yokoyama, I.; Takahashi, K.; Yamagata, S.; Imamaki, M.; Kobayashi, Y.; Ishii, I.; et al. Application of Akaike information criterion to evaluate warfarin dosing algorithm. Thromb. Res. 2010, 126, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T. Optimal intensity of warfarin therapy for secondary prevention of stroke in patients with nonvalvular atrial fibrillation: A multicenter, prospective, randomized trial. Japanese Nonvalvular Atrial Fibrillation-Embolism Secondary Prevention Cooperative Study Group. Stroke 2000, 31, 817–821. [Google Scholar] [CrossRef] [Green Version]
- Wakita, M.; Yasaka, M.; Minematsu, K.; Yamaguchi, T. Effects of anticoagulation on infarct size and clinical outcome in acute cardioembolic stroke. Angiology 2002, 53, 551–556. [Google Scholar] [CrossRef]
- Froom, P.; Miron, E.; Barak, M. Oral anticoagulants in the elderly. Br. J. Haematol. 2003, 120, 526–528. [Google Scholar] [CrossRef]
- Gage, B.F.; Eby, C.; Johnson, J.A.; Deych, E.; Rieder, M.J.; Ridker, P.M.; Milligan, P.E.; Grice, G.; Lenzini, P.; Rettie, A.E.; et al. Use of pharmacogenetic and clinical factors to predict the therapeutic dose of warfarin. Clin. Pharmacol. Ther. 2008, 84, 326–331. [Google Scholar] [CrossRef]
- Limdi, N.A.; Limdi, M.A.; Cavallari, L.; Anderson, A.M.; Crowley, M.R.; Baird, M.F.; Allon, M.; Beasley, T.M. Warfarin dosing in patients with impaired kidney function. Am. J. Kidney Dis. 2010, 56, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Naud, J.; Michaud, J.; Leblond, F.A.; Lefrancois, S.; Bonnardeaux, A.; Pichette, V. Effects of chronic renal failure on liver drug transporters. Drug Metab. Dispos. 2008, 36, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Dreisbach, A.W.; Japa, S.; Gebrekal, A.B.; Mowry, S.E.; Lertora, J.J.; Kamath, B.L.; Rettie, A.E. Cytochrome P4502C9 activity in end-stage renal disease. Clin. Pharmacol. Ther. 2003, 73, 475–477. [Google Scholar] [CrossRef]
- Momper, J.D.; Venkataramanan, R.; Nolin, T.D. Nonrenal drug clearance in CKD: Searching for the path less traveled. Adv. Chronic Kidney Dis. 2010, 17, 384–391. [Google Scholar] [CrossRef]
- Michaud, J.; Naud, J.; Chouinard, J.; Desy, F.; Leblond, F.A.; Desbiens, K.; Bonnardeaux, A.; Pichette, V. Role of parathyroid hormone in the downregulation of liver cytochrome P450 in chronic renal failure. J. Am. Soc. Nephrol. 2006, 17, 3041–3048. [Google Scholar] [CrossRef]
- Leung, N.; Eirin, A.; Irazabal, M.V.; Maddox, D.E.; Gunderson, H.D.; Fervenza, F.C.; Garovic, V.D. Acute kidney injury in patients with inactive cytochrome P450 polymorphisms. Ren. Fail. 2009, 31, 749–752. [Google Scholar] [CrossRef]
- Genovesi, S.; Santoro, A. Warfarin and stroke outcomes in hemodialysis patients with atrial fibrillation. J. Am. Soc. Nephrol. 2009, 20, 2090–2092. [Google Scholar] [CrossRef] [Green Version]
- Holden, R.M.; Clase, C.M. Use of warfarin in people with low glomerular filtration rate or on dialysis. Semin. Dial. 2009, 22, 503–511. [Google Scholar] [CrossRef]
- Shearer, M.J.; Newman, P. Metabolism and cell biology of vitamin K. Thromb. Haemost. 2008, 100, 530–547. [Google Scholar] [PubMed]
- Rockson, S.G.; Albers, G.W. Comparing the guidelines: Anticoagulation therapy to optimize stroke prevention in patients with atrial fibrillation. J. Am. Coll. Cardiol. 2004, 43, 929–935. [Google Scholar] [CrossRef]
- Cavallari, L.H.; Aston, J.L.; Momary, K.M.; Shapiro, N.L.; Patel, S.R.; Nutescu, E.A. Predictors of unstable anticoagulation in African Americans. J. Thromb. Thrombolysis 2009, 27, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Cha, P.C.; Mushiroda, T.; Takahashi, A.; Kubo, M.; Minami, S.; Kamatani, N.; Nakamura, Y. Genome-wide association study identifies genetic determinants of warfarin responsiveness for Japanese. Hum. Mol. Genet. 2010, 19, 4735–4744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarvela, K.; Maaranen, P.; Harmoinen, A.; Huhtala, H.; Sisto, T. Cystatin C in diabetics as a marker of mild renal insufficiency after CABG. Ann. Thorac. Cardiovasc. Surg. 2011, 17, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | N = 176 |
|---|---|
| Age (years, mean ± SD) | 72.1 ± 8.1 |
| Male (n, %) | 126 (71.6%) |
| Body height (cm, mean ± SD) | 162.4 ± 8.2 |
| Body weight (kg, mean ± SD) | 61.2 ± 10.5 |
| BSA (m2, mean ± SD) | 1.65 ± 0.17 |
| Current smokers (n, %) | 8 (4.5%) |
| Current alcohol consumption (n, %) | 86 (48.9%) |
| History of embolic event (n, %) | 17 (9.7%) |
| Concomitant medication | |
| Aspirin use (n, %) | 30 (17.0%) |
| Another antiplatelet drugs use (n, %) | 5 (2.8%) |
| Statin use (n, %) | 62 (35.2%) |
| PT-INR (mean ± SD) | 2.0 ± 0.4 |
| WBC (count/L, mean ± SD) | 5.9 ± 1.6 × 109 |
| Hemoglobin (g/dL, mean ± SD) | 13.7 ± 1.5 |
| AST (IU/L, mean ± SD) | 26.3 ± 8.2 |
| ALT (IU/L, mean ± SD) | 20.7 ± 11.5 |
| BUN (mg/dL, mean ± SD) | 17.1 ± 5.1 |
| Creatinine (mg/dL, mean ± SD) | 0.9 ± 0.3 |
| eGFR (mL/min/1.73 m2, mean ± SD) | 65.04 ± 16.98 |
| VKORC1 Genotype (-1639G>A) | |||
|---|---|---|---|
| CYP2C9 Genotype | AA | GA | GG |
| *1/*1 | 140 (80.0%) | 25 (14.3%) † | 1 (0.6%) † |
| *1/*3 | 6 (3.4%) ‡ | 2 (1.1%) ¶ | 1 (0.6%) ¶ |
| *3/*3 | 0 | 0 | 0 |
| Variables | β Value | Standard Error | p Value |
|---|---|---|---|
| Sex | −0.196 | 0.208 | 0.348 |
| Age | −0.043 | 0.011 | 0.0001 ** |
| Height | 0.041 | 0.011 | 0.0004 ** |
| Weight | 0.022 | 0.009 | 0.016 * |
| BSA | 0.00017 | 0.00005 | 0.0023 ** |
| BUN | −0.041 | 0.018 | 0.022 * |
| Creatinine | −0.806 | 0.324 | 0.014 * |
| AST | −0.02 | 0.012 | 0.087 |
| WBC | −0.0001 | 0.00006 | 0.076 |
| Vitamin K intake | 0.018 | 0.012 | 0.134 |
| Smoking | 0.252 | 0.439 | 0.567 |
| Alcohol intake | 0.209 | 0.188 | 0.268 |
| Aspirin use | −0.138 | 0.247 | 0.578 |
| Statin use | 0.133 | 0.197 | 0.501 |
| eGFR | 0.02 | 0.005 | 0.0003 ** |
| Genotypes | |||
| VC2 † | 1.896 | 0.213 | <0.0001 ** |
| VC3 ‡ | −0.984 | 0.499 | 0.050 |
| VC4 ¶ | 0.34 | 0.707 | 0.632 |
| Variables | β Value | Standard Error | p Value |
|---|---|---|---|
| age (/10 years) | −0.217 | 0.103 | 0.037 |
| BSA (/100 m2) | 0.015 | 0.005 | 0.002 |
| eGFR (/10 mL/min/1.73 m2) | 0.201 | 0.047 | <0.001 |
| Genotypes | |||
| VC2 † | 1.886 | 0.189 | <0.001 |
| VC3 ‡ | −1.164 | 0.406 | 0.005 |
| VC4 ¶ | 0.601 | 0.633 | 0.344 |
| Vitamin K intake (µg/day) | 0.011 | 0.009 | 0.225 |
| AST (IU/L) | −0.021 | 0.009 | 0.029 |
| Alcohol intake | 0.186 | 0.148 | 0.210 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, T.; Ihara, M.; Fukuma, K.; Yamamoto, H.; Washida, K.; Kimura, S.; Kada, A.; Miyata, S.; Miyata, T.; Nagatsuka, K. Influence of Renal Impairment and Genetic Subtypes on Warfarin Control in Japanese Patients. Genes 2021, 12, 1537. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12101537
Tanaka T, Ihara M, Fukuma K, Yamamoto H, Washida K, Kimura S, Kada A, Miyata S, Miyata T, Nagatsuka K. Influence of Renal Impairment and Genetic Subtypes on Warfarin Control in Japanese Patients. Genes. 2021; 12(10):1537. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12101537
Chicago/Turabian StyleTanaka, Tomotaka, Masafumi Ihara, Kazuki Fukuma, Haruko Yamamoto, Kazuo Washida, Shunsuke Kimura, Akiko Kada, Shigeki Miyata, Toshiyuki Miyata, and Kazuyuki Nagatsuka. 2021. "Influence of Renal Impairment and Genetic Subtypes on Warfarin Control in Japanese Patients" Genes 12, no. 10: 1537. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12101537