
Lower Fractions of TCF4 Transcripts Spanning over the CTG18.1 Trinucleotide Repeat in Human Corneal Endothelium


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. FECD Patients and Controls Characteristics
3.2. TCF4 Genotyping
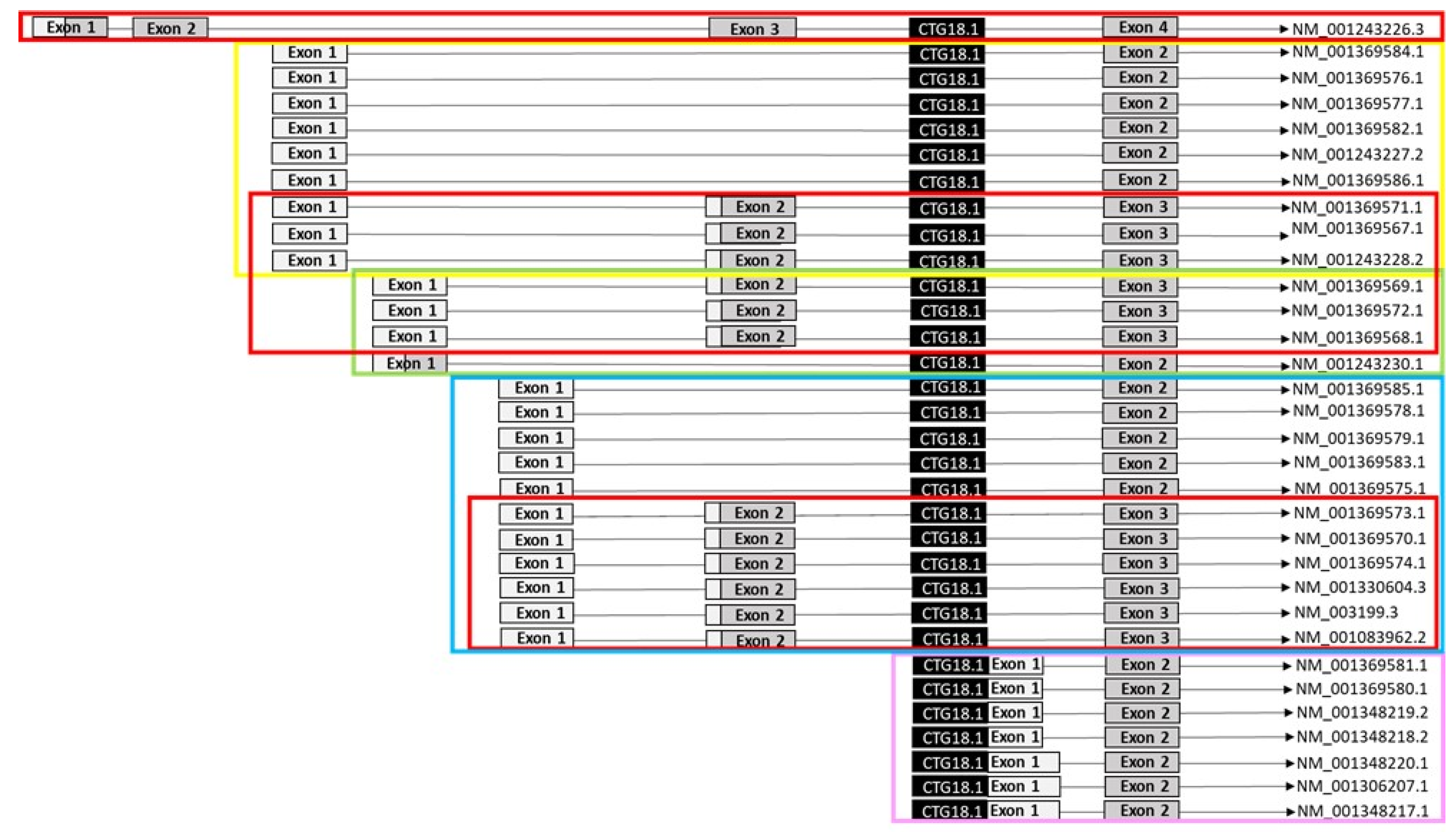
3.3. TCF4 mRNA Expression by Digital Droplet PCR (ddPCR)
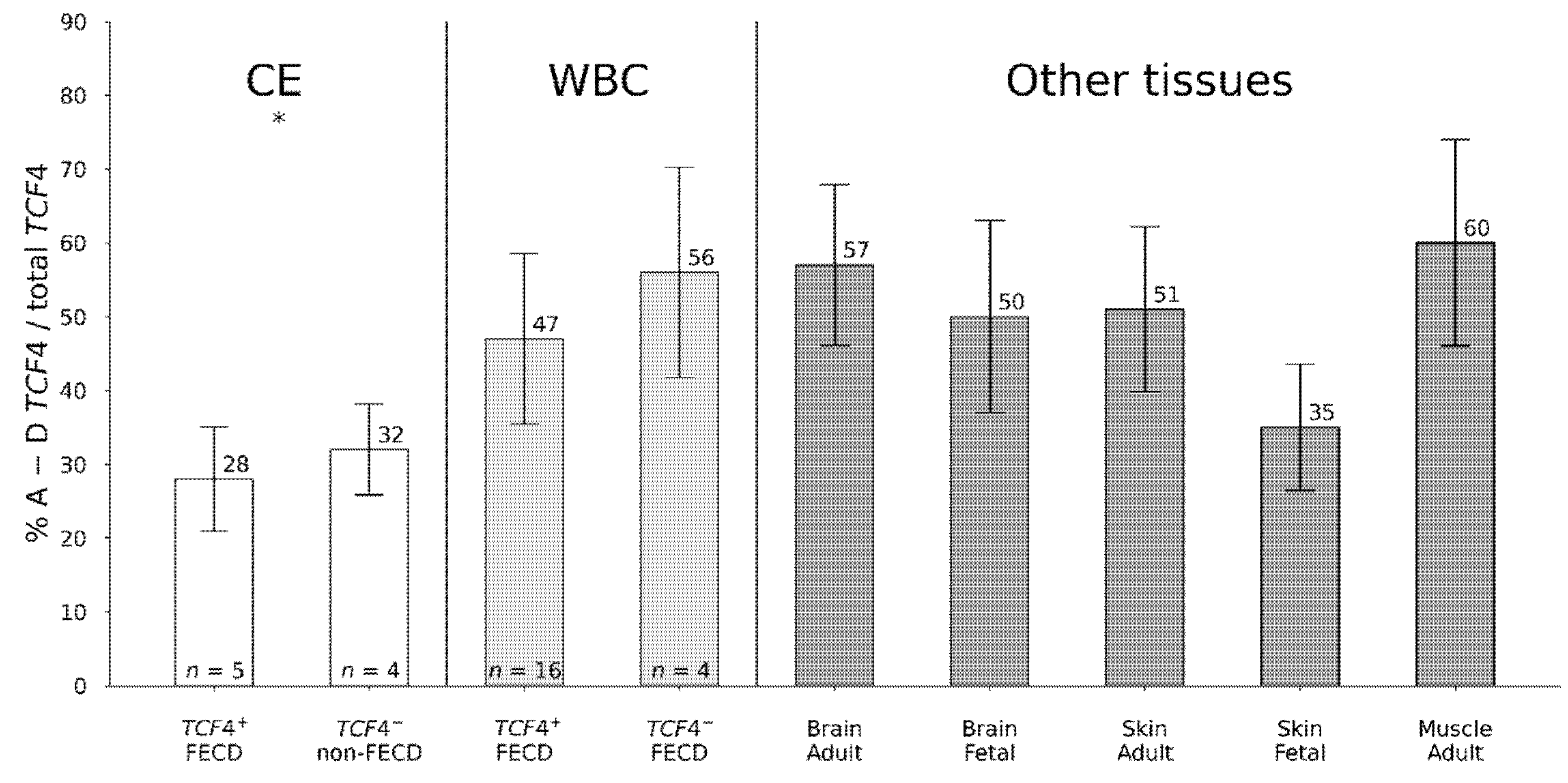
3.4. Differential TCF4 mRNA Expression in Corneal Endothelium
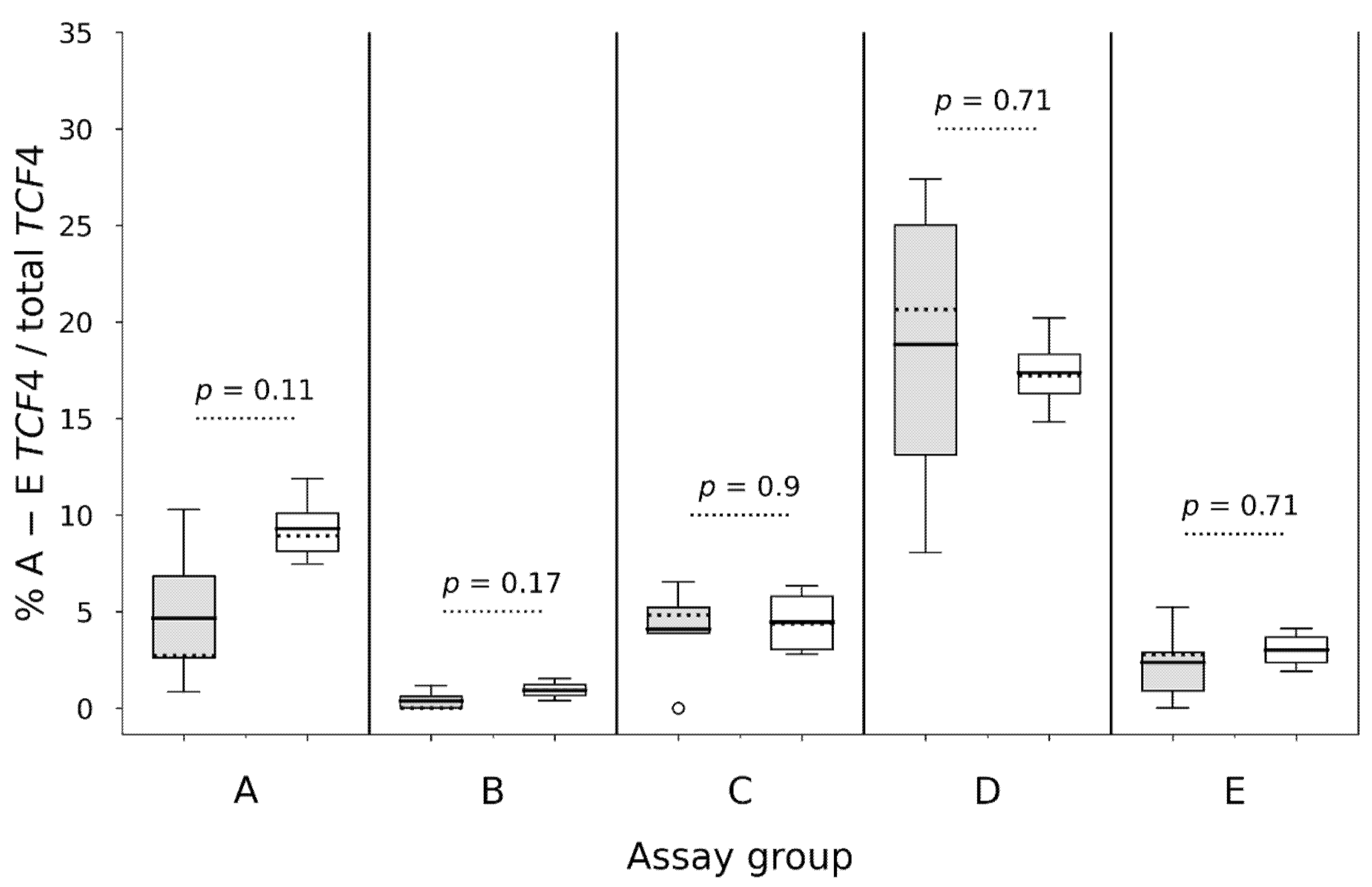
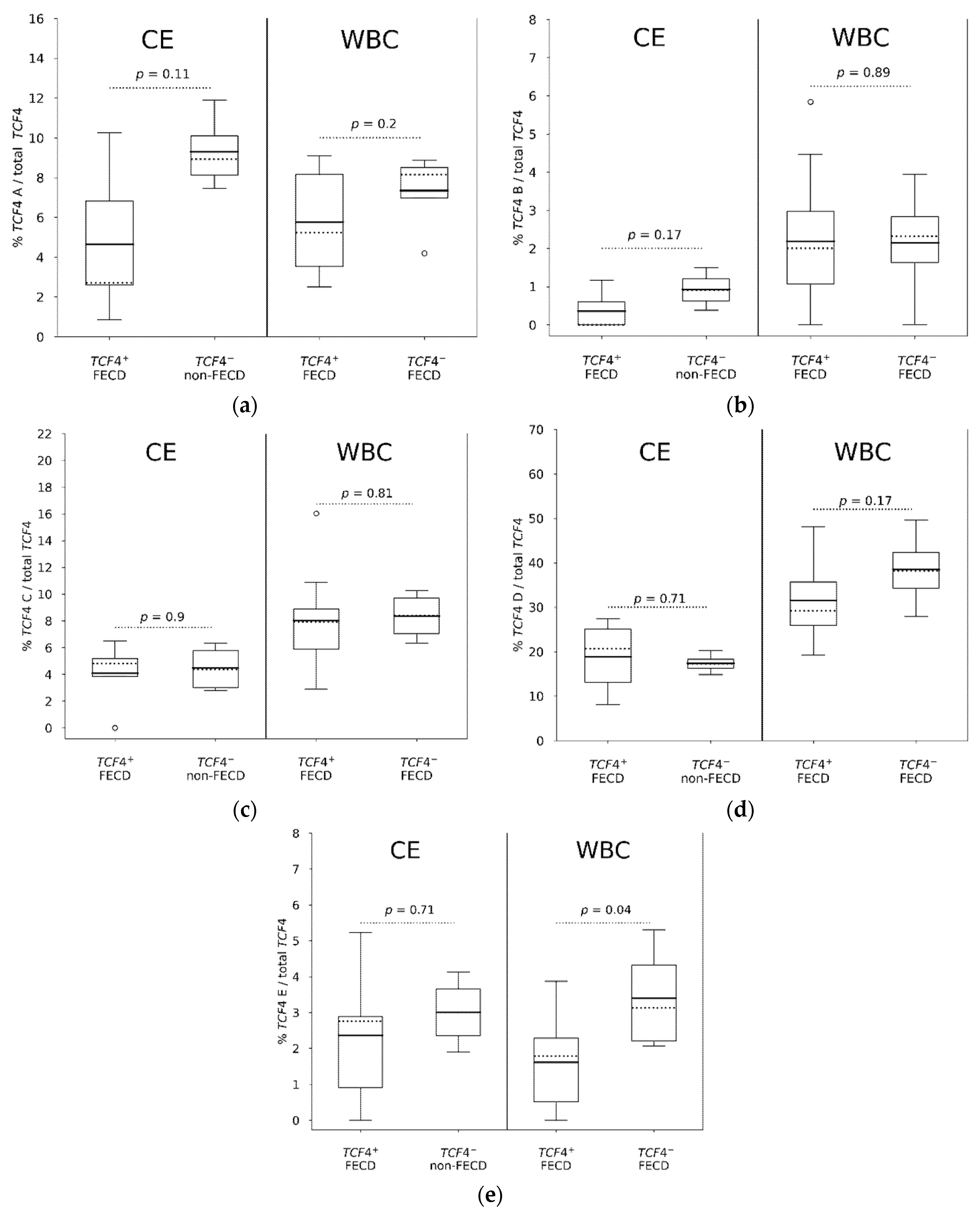
3.5. Comparison of TCF4 mRNA Expression in Individual Assays (A to E) in WBC and CE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mok, J.W.; Kim, H.S.; Joo, C.K. Q455V mutation in COL8A2 is associated with Fuchs’ corneal dystrophy in Korean patients. Eye 2009, 23, 895–903. [Google Scholar] [CrossRef] [Green Version]
- Gottsch, J.D.; Sundin, O.H.; Liu, S.H.; Jun, A.S.; Broman, K.W.; Stark, W.J.; Vito, E.C.; Narang, A.K.; Thompson, J.M.; Magovern, M. Inheritance of a novel COL8A2 mutation defines a distinct early-onset subtype of fuchs corneal dystrophy. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1934–1939. [Google Scholar] [CrossRef] [Green Version]
- Biswas, S.; Munier, F.L.; Yardley, J.; Hart-Holden, N.; Perveen, R.; Cousin, P.; Sutphin, J.E.; Noble, B.; Batterbury, M.; Kielty, C.; et al. Missense mutations in COL8A2, the gene encoding the alpha2 chain of type VIII collagen, cause two forms of corneal endothelial dystrophy. Hum. Mol. Genet. 2001, 10, 2415–2423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baratz, K.H.; Tosakulwong, N.; Ryu, E.; Brown, W.L.; Branham, K.; Chen, W.; Tran, K.D.; Schmid-Kubista, K.E.; Heckenlively, J.R.; Swaroop, A.; et al. E2-2 protein and Fuchs’s corneal dystrophy. N. Engl. J. Med. 2010, 363, 1016–1024. [Google Scholar] [CrossRef] [Green Version]
- Breschel, T.S.; McInnis, M.G.; Margolis, R.L.; Sirugo, G.; Corneliussen, B.; Simpson, S.G.; McMahon, F.J.; MacKinnon, D.F.; Xu, J.F.; Pleasant, N.; et al. A novel, heritable, expanding CTG repeat in an intron of the SEF2-1 gene on chromosome 18q21.1. Hum. Mol. Genet. 1997, 6, 1855–1863. [Google Scholar] [CrossRef] [Green Version]
- Wieben, E.D.; Aleff, R.A.; Tosakulwong, N.; Butz, M.L.; Highsmith, W.E.; Edwards, A.O.; Baratz, K.H. A common trinucleotide repeat expansion within the transcription factor 4 (TCF4, E2-2) gene predicts Fuchs corneal dystrophy. PLoS ONE 2012, 7, e49083. [Google Scholar] [CrossRef] [PubMed]
- Foja, S.; Luther, M.; Hoffmann, K.; Rupprecht, A.; Gruenauer-Kloevekorn, C. CTG18.1 repeat expansion may reduce TCF4 gene expression in corneal endothelial cells of German patients with Fuchs’ dystrophy. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1621–1631. [Google Scholar] [CrossRef]
- Rao, B.S.; Tharigopala, A.; Rachapalli, S.R.; Rajagopal, R.; Soumittra, N. Association of polymorphisms in the intron of TCF4 gene to late-onset Fuchs endothelial corneal dystrophy: An Indian cohort study. Indian J. Ophthalmol. 2017, 65, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Nanda, G.G.; Padhy, B.; Samal, S.; Das, S.; Alone, D.P. Genetic association of TCF4 intronic polymorphisms, CTG18.1 and rs17089887, with Fuchs’ endothelial corneal dystrophy in an Indian population. Investig. Ophthalmol. Vis. Sci. 2014, 55, 7674–7680. [Google Scholar] [CrossRef] [Green Version]
- Okumura, N.; Hayashi, R.; Nakano, M.; Yoshii, K.; Tashiro, K.; Sato, T.; Blake, D.J.; Aleff, R.; Butz, M.; Highsmith, E.W.; et al. Effect of trinucleotide repeat expansion on the expression of TCF4 mRNA in Fuchs’ endothelial corneal dystrophy. Investig. Ophthalmol. Vis. Sci. 2019, 60, 779–786. [Google Scholar] [CrossRef] [Green Version]
- Viberg, A.; Westin, I.M.; Golovleva, I.; Bystrom, B. TCF4 trinucleotide repeat expansion in Swedish cases with Fuchs’ endothelial corneal dystrophy. Acta Ophthalmol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Xing, C.; Gong, X.; Hussain, I.; Khor, C.C.; Tan, D.T.; Aung, T.; Mehta, J.S.; Vithana, E.N.; Mootha, V.V. Transethnic replication of association of CTG18.1 repeat expansion of TCF4 gene with Fuchs’ corneal dystrophy in Chinese implies common causal variant. Investig. Ophthalmol. Vis. Sci. 2014, 55, 7073–7078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuot, A.; Hewitt, A.W.; Snibson, G.R.; Souzeau, E.; Mills, R.; Craig, J.E.; Burdon, K.P.; Sharma, S. TGC repeat expansion in the TCF4 gene increases the risk of Fuchs’ endothelial corneal dystrophy in Australian cases. PLoS ONE 2017, 12, e0183719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okumura, N.; Puangsricharern, V.; Jindasak, R.; Koizumi, N.; Komori, Y.; Ryousuke, H.; Nakahara, M.; Nakano, M.; Adachi, H.; Tashiro, K.; et al. Trinucleotide repeat expansion in the transcription factor 4 (TCF4) gene in Thai patients with Fuchs endothelial corneal dystrophy. Eye 2020, 34, 880–885. [Google Scholar] [CrossRef]
- Skorodumova, L.O.; Belodedova, A.V.; Antonova, O.P.; Sharova, E.I.; Akopian, T.A.; Selezneva, O.V.; Kostryukova, E.S.; Malyugin, B.E. CTG18.1 expansion is the best classifier of late-onset Fuchs’ corneal dystrophy among 10 biomarkers in a cohort from the European part of Russia. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4748–4754. [Google Scholar] [CrossRef] [PubMed]
- Mootha, V.V.; Hussain, I.; Cunnusamy, K.; Graham, E.; Gong, X.; Neelam, S.; Xing, C.; Kittler, R.; Petroll, W.M. TCF4 triplet repeat expansion and nuclear RNA foci in Fuchs’ endothelial corneal dystrophy. Investig. Ophthalmol. Vis. Sci. 2015, 56, 2003–2011. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Rong, Z.; Gong, X.; Zhou, Z.; Sharma, V.K.; Xing, C.; Watts, J.K.; Corey, D.R.; Mootha, V.V. Oligonucleotides targeting TCF4 triplet repeat expansion inhibit RNA foci and mis-splicing in Fuchs’ dystrophy. Hum. Mol. Genet. 2018, 27, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Zarouchlioti, C.; Sanchez-Pintado, B.; Tear, N.J.H.; Klein, P.; Liskova, P.; Dulla, K.; Semo, M.; Vugler, A.A.; Muthusamy, K.; Dudakova, L.; et al. Antisense therapy for a common corneal dystrophy ameliorates TCF4 repeat expansion-mediated toxicity. Am. J. Hum. Genet. 2018, 102, 528–539. [Google Scholar] [CrossRef] [Green Version]
- Massari, M.E.; Murre, C. Helix-loop-helix proteins: Regulators of transcription in eucaryotic organisms. Mol. Cell. Biol. 2000, 20, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, J.R.; Szeto, R.A.; Carvalho, V.M.A.; Muotri, A.R.; Papes, F. Transcription factor 4 and its association with psychiatric disorders. Transl. Psychiatry 2021, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Oldak, M.; Ruszkowska, E.; Udziela, M.; Ozieblo, D.; Binczyk, E.; Sciezynska, A.; Ploski, R.; Szaflik, J.P. Fuchs endothelial corneal dystrophy: Strong association with rs613872 not paralleled by changes in corneal endothelial TCF4 mRNA level. Biomed. Res. Int. 2015, 2015, 640234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sirp, A.; Leite, K.; Tuvikene, J.; Nurm, K.; Sepp, M.; Timmusk, T. The Fuchs corneal dystrophy-associated CTG repeat expansion in the TCF4 gene affects transcription from its alternative promoters. Sci. Rep. 2020, 10, 18424. [Google Scholar] [CrossRef]
- Miller, S.A.; Dykes, D.D.; Polesky, H.F. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988, 16, 1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madzak, A.; Hjortdal, J. Outcome of human donor corneas stored for more than 4 weeks. Cornea 2018, 37, 1232–1236. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Custom TaqMan® Assay | Primer and Probe (5′ ⟶ 3′) |
|---|---|
| A | F 1: GTCTCTCTTTTTAAAGTCTCTTTCCTTGGAA R 2: TTGAGCCAGTAAAATGTCCA Probe: TGTGGCCATTTAAGATGTT |
| B | F: GGGATGTAAACTCGAATAAATTTCAAAGTG R: TTGAGCCAGTAAAATGTCCA Probe: AGGCTTCAGATTGTAACTGAC |
| C | F: TGAACGCCGCCTCGG R: TTGAGCCAGTAAAATGTCCAC Probe: TGCACGGAGAGCCC |
| E | F: CCATTCGTTCCTTTGCTTTTTGCA R: CCCCAGGACCCTGAGCTA Probe: TTGAGCCAGTAAAATGTC |
| Tissue | Group | Sex | Age (Years) | TCF4 Allele 1 | TCF4 Allele 2 | TCF4 Genotype | |
|---|---|---|---|---|---|---|---|
| KFUH9 | CE 1 | control | female | 78 | 12 | 25 | TCF4− |
| KFUH12 | CE | control | female | 25 | 12 | 18 | TCF4− |
| KFUH13 | CE | control | female | 56 | 12 | 18 | TCF4− |
| KFUH15 | CE | control | male | 76 | 12 | 18 | TCF4− |
| FUH18 | CE | FECD | male | 76 | 76 | 87 | TCF4+ |
| FUH19 | CE | FECD | male | 85 | 22 | 75 | TCF4+ |
| FUH20 | CE | FECD | male | 85 | 12 | 93 | TCF4+ |
| FUH21 | CE | FECD | male | 71 | 12 | 71 | TCF4+ |
| FUH22 | CE | FECD | female | 63 | 12 | 105 | TCF4+ |
| FUB1 | WBC 2 | FECD | female | 62 | 12 | 95 | TCF4+ |
| FUB2 | WBC | FECD | female | 81 | 15 | 93 | TCF4+ |
| FUB3 | WBC | FECD | female | 69 | 81 | >81 | TCF4+ |
| FUB4 | WBC | FECD | male | 59 | 17 | >125 | TCF4+ |
| FUB5 | WBC | FECD | female | 76 | 37 | 97 | TCF4+ |
| FUB7 | WBC | FECD | female | 84 | 20 | 52 | TCF4+ |
| FUB8 | WBC | FECD | male | 75 | 12 | 95 | TCF4+ |
| FUB9 | WBC | FECD | female | 73 | 19 | 85 | TCF4+ |
| FUB10 | WBC | FECD | male | 62 | 27 | 78 | TCF4+ |
| FUB11 | WBC | FECD | female | 72 | 27 | 91 | TCF4+ |
| FUB12 | WBC | FECD | female | 84 | 12 | 67 | TCF4+ |
| FUB13 | WBC | FECD | female | 84 | 18 | 96 | TCF4+ |
| FUB14 | WBC | FECD | female | 76 | 19 | 83 | TCF4+ |
| FUB15 | WBC | FECD | male | 79 | 17 | 103 | TCF4+ |
| FUB16 | WBC | FECD | female | 59 | 19 | 98 | TCF4+ |
| FUB17 | WBC | FECD | female | 65 | 29 | 101 | TCF4+ |
| 7753 | WBC | FECD | male | 70 | 13 | 13 | TCF4− |
| 8360 | WBC | FECD | female | 75 | 15 | 19 | TCF4− |
| 1494 | WBC | FECD | female | 78 | 12 | 15 | TCF4− |
| 9309 | WBC | FECD | male | 74 | 13 | 13 | TCF4− |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Westin, I.M.; Viberg, A.; Byström, B.; Golovleva, I. Lower Fractions of TCF4 Transcripts Spanning over the CTG18.1 Trinucleotide Repeat in Human Corneal Endothelium. Genes 2021, 12, 2006. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12122006
Westin IM, Viberg A, Byström B, Golovleva I. Lower Fractions of TCF4 Transcripts Spanning over the CTG18.1 Trinucleotide Repeat in Human Corneal Endothelium. Genes. 2021; 12(12):2006. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12122006
Chicago/Turabian StyleWestin, Ida Maria, Andreas Viberg, Berit Byström, and Irina Golovleva. 2021. "Lower Fractions of TCF4 Transcripts Spanning over the CTG18.1 Trinucleotide Repeat in Human Corneal Endothelium" Genes 12, no. 12: 2006. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12122006