
Sensory Reactivity Phenotype in Phelan–McDermid Syndrome Is Distinct from Idiopathic ASD


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethics Declaration
2.3. Sensory Evaluation
2.4. Analysis
3. Results
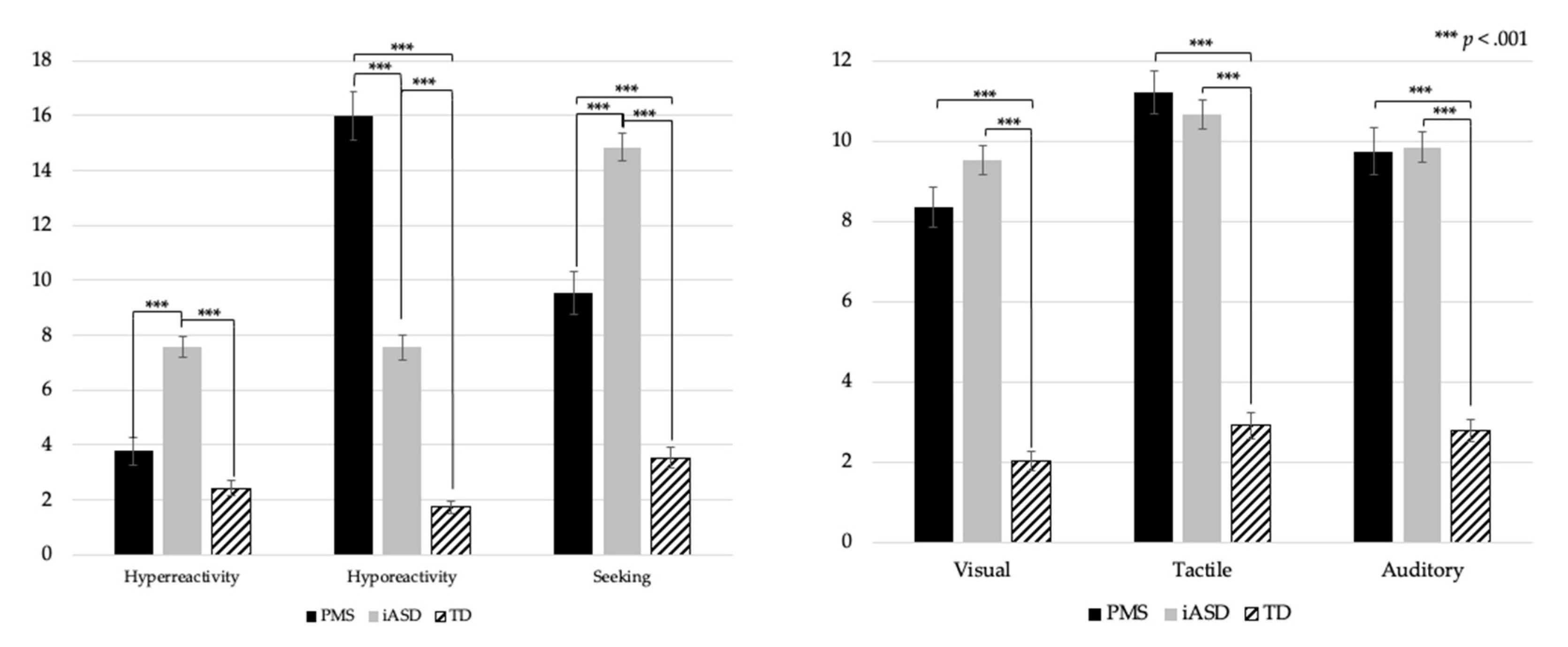
3.1. Group Comparisons on SAND Domain, Modality and Subscale Scores
3.2. SAND Score Comparisons for Participants with Intellectual Disability
3.3. Stability of SAND Scores
3.4. Genotype–Phenotype Associations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Baio, J.; Wiggins, L.; Christensen, D.L.; Maenner, M.J.; Daniels, J.; Warren, Z.; Kurzius-Spencer, M.; Zahorodny, W.; Robinson, C.; Rosenberg, C.R.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. MMWR Surveill. Summ. 2018, 67, 1–23. [Google Scholar] [CrossRef]
- Miles, J.H. Autism spectrum disorders—A genetics review. Genet. Med. 2011, 13, 278–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, G.B.; Mendelsohn, N.J. Clinical genetics evaluation in identifying the etiology of autism spectrum disorders: 2013 guideline revisions. Genet. Med. 2013, 15, 399–407. [Google Scholar] [CrossRef] [Green Version]
- Genovese, A.; Butler, M.G. Clinical Assessment, Genetics, and Treatment Approaches in Autism Spectrum Disorder (ASD). Int. J. Mol. Sci. 2020, 21, 4726. [Google Scholar] [CrossRef]
- Betancur, C.; Buxbaum, J.D. SHANK3 haploinsufficiency: A common but underdiagnosed highly penetrant monogenic cause of autism spectrum disorders. Mol. Autism 2013, 4, 17. [Google Scholar] [CrossRef] [Green Version]
- Leblond, C.S.; Nava, C.; Polge, A.; Gauthier, J.; Huguet, G.; Lumbroso, S.; Giuliano, F.; Stordeur, C.; Depienne, C.; Mouzat, K.; et al. Meta-analysis of SHANK Mutations in Autism Spectrum Disorders: A Gradient of Severity in Cognitive Impairments. PLoS Genet. 2014, 10, e1004580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozdagi, O.; Sakurai, T.; Papapetrou, D.; Wang, X.; Dickstein, D.L.; Takahashi, N.; Kajiwara, Y.; Yang, M.; Katz, A.; Scattoni, M.; et al. Haploinsufficiency of the autism-associated Shank3 gene leads to deficits in synaptic function, social interaction, and social communication. Mol. Autism 2010, 1, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; Bozdagi, O.; Scattoni, M.L.; Wöhr, M.; Roullet, F.I.; Katz, A.M.; Abrams, D.N.; Kalikhman, D.; Simon, H.; Woldeyohannes, L.; et al. Reduced Excitatory Neurotransmission and Mild Autism-Relevant Phenotypes in Adolescent Shank3 Null Mutant Mice. J. Neurosci. 2012, 32, 6525–6541. [Google Scholar] [CrossRef]
- Kolevzon, A.; Angarita, B.; Bush, L.; Wang, A.T.; Frank, Y.; Yang, A.; Rapaport, R.; Saland, J.; Srivastava, S.; Farrell, C.; et al. Phelan-McDermid syndrome: A review of the literature and practice parameters for medical assessment and monitoring. J. Neurodev. Disord. 2014, 6, 39. [Google Scholar] [CrossRef]
- Soorya, L.; Kolevzon, A.; Zweifach, J.; Lim, T.; Dobry, Y.; Schwartz, L.; Frank, Y.; Wang, A.T.; Cai, G.; Parkhomenko, E.; et al. Prospective investigation of autism and genotype-phenotype correlations in 22q13 deletion syndrome and SHANK3 deficiency. Mol. Autism 2013, 4, 18. [Google Scholar] [CrossRef] [Green Version]
- Tomchek, S.D.; Dunn, W. Sensory Processing in Children With and Without Autism: A Comparative Study Using the Short Sensory Profile. Am. J. Occup. Ther. 2007, 61, 190–200. [Google Scholar] [CrossRef] [Green Version]
- Tavassoli, T.; Miller, L.J.; Schoen, S.; Nielsen, D.M.; Baron-Cohen, S. Sensory over-responsivity in adults with autism spectrum conditions. Autism 2014, 18, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, T.; Bellesheim, K.; Siper, P.M.; Wang, A.T.; Halpern, D.; Gorenstein, M.; Grodberg, D.; Kolevzon, A.; Buxbaum, J. Measuring Sensory Reactivity in Autism Spectrum Disorder: Application and Simplification of a Clinician-Administered Sensory Observation Scale. J. Autism Dev. Disord. 2015, 46, 287–293. [Google Scholar] [CrossRef]
- Green, S.A.; Hernandez, L.; Tottenham, N.; Krasileva, K.; Bookheimer, S.Y.; Dapretto, M. Neurobiology of Sensory Overresponsivity in Youth With Autism Spectrum Disorders. JAMA Psychiatry 2015, 72, 778–786. [Google Scholar] [CrossRef] [Green Version]
- Mieses, A.M.; Tavassoli, T.; Li, E.; Soorya, L.; Lurie, S.; Wang, A.T.; Siper, P.; Kolevzon, A. Brief Report: Sensory Reactivity in Children with Phelan-McDermid Syndrome. J. Autism Dev. Disord. 2016, 46, 2508–2513. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, T.; Auyeung, B.; Murphy, L.C.; Baron-Cohen, S.; Chakrabarti, B. Variation in the autism candidate gene GABRB3 modulates tactile sensitivity in typically developing children. Mol. Autism 2012, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- DeLorey, T.M.; Sahbaie, P.; Hashemi, E.; Li, W.-W.; Salehi, A.; Clark, D.J. Somatosensory and sensorimotor consequences associated with the heterozygous disruption of the autism candidate gene, Gabrb3. Behav. Brain Res. 2011, 216, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Siper, P.M.; Tavassoli, T. Sensory Assessment for Neurodevelopmental Disorders; Stoelting Co.: Wood Dale, IL, USA, 2021. [Google Scholar]
- Siper, P.M.; Kolevzon, A.; Wang, A.T.; Buxbaum, J.D.; Tavassoli, T. A clinician-administered observation and corresponding caregiver interview capturing DSM-5 sensory reactivity symptoms in children with ASD. Autism Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Siper, P.; Layton, C.; Levy, T.; Lurie, S.; Benrey, N.; Zweifach, J.; Rowe, M.; Tang, L.; Guillory, S.; Halpern, D.; et al. Sensory Reactivity Symptoms Are a Core Feature of ADNP Syndrome Irrespective of Autism Diagnosis. Genes 2021, 12, 351. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; DiLavore, P.S.; Risi, S.; Gotham, K.D.B. Autism Diagnostic Observation Schedule, 2nd ed.; ADOS-2 Mannual Part I: Modules 1–4; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Western Psychological Services. Responsiveness Scale, 2nd ed.; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Mullen, M. Mullen Scales of Early Learning; American Guidance Services: Circle Pines, MN, USA, 1995. [Google Scholar]
- Roid, G.H. Stanford Binet Intelligence Scales, 5th ed.; Riverside Publishing: Itasca, IL, USA, 2003. [Google Scholar]
- Elliott, C. Differential Ability Scales, 2nd ed.; Harcourt Assessment: San Antonio, TX, USA, 2007. [Google Scholar]
- Han, Q.; Kim, Y.H.; Wang, X.; Liu, D.; Zhang, Z.-J.; Bey, A.L.; Lay, M.; Chang, W.; Berta, T.; Zhang, Y.; et al. SHANK3 Deficiency Impairs Heat Hyperalgesia and TRPV1 Signaling in Primary Sensory Neurons. Neuron 2016, 92, 1279–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Droogmans, G.; Swillen, A.; Van Buggenhout, G. Deep Phenotyping of Development, Communication and Behaviour in Phelan-McDermid Syndrome. Mol. Syndr. 2019, 10, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Rais, M.; Binder, D.K.; Razak, K.A.; Ethell, I.M. Sensory Processing Phenotypes in Fragile X Syndrome. ASN Neuro 2018, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| M(SD) | Male/Female | Age (years) | ASD Dx | ADOS-2 Comparison Score | Full Scale IQ/DQ | Nonverbal IQ/DQ | Verbal IQ/DQ | VABS Adaptive Behavior Composite |
|---|---|---|---|---|---|---|---|---|
| PMS | 26/26 | 6.65 (2.90) | 42/52 | 6.63 (2.23) | 30.20 (16.88) | 35.74 (19.66) | 27.52 (19.53) | 55.14 (12.61) |
| iASD | 114/18 | 6.11 (2.55) | 132/132 | 7.31 (1.60) | 72.80 (29.99) | 79.27 (30.17) | 69.76 (30.66) | 70.70 (15.39) |
| TD | 24/30 | 5.39 (2.55) | 0/54 | N/A | 117.21 (16.06) | 115.18 (17.70) | 114.88 (12.84) | N/A |
| SAND Subscale | Group | Mean | SD | F | p |
|---|---|---|---|---|---|
| Hyperreactivity Total | TD | 2.43 | 1.90 | 45.86 | <0.001 |
| iASD | 7.64 | 4.51 | |||
| PMS | 3.54 | 3.19 | |||
| Visual | TD | 0.24 | 0.64 | 10.75 | <0.001 |
| iASD | 1.39 | 1.92 | |||
| PMS | 0.77 | 1.32 | |||
| Tactile | TD | 1.06 | 1.34 | 16.70 | <0.001 |
| iASD | 2.74 | 2.17 | |||
| PMS | 1.60 | 1.87 | |||
| Auditory | TD | 1.13 | 1.36 | 40.37 | <0.001 |
| iASD | 3.51 | 2.29 | |||
| PMS | 1.17 | 1.81 | |||
| Hyporeactivity Total | TD | 1.74 | 1.65 | 114.89 | <0.001 |
| iASD | 7.55 | 5.23 | |||
| PMS | 16.19 | 6.32 | |||
| Visual | TD | 0.74 | 1.05 | 74.45 | <0.001 |
| iASD | 3.05 | 2.28 | |||
| PMS | 5.63 | 2.28 | |||
| Tactile | TD | 0.41 | 0.81 | 71.67 | <0.001 |
| iASD | 2.45 | 2.12 | |||
| PMS | 4.94 | 2.31 | |||
| Auditory | TD | 0.59 | 0.92 | 68.50 | <0.001 |
| iASD | 2.05 | 2.45 | |||
| PMS | 5.62 | 2.85 | |||
| Seeking Total | TD | 3.54 | 2.88 | 89.07 | <0.001 |
| iASD | 14.80 | 5.83 | |||
| PMS | 9.56 | 5.81 | |||
| Visual | TD | 1.04 | 1.39 | 85.91 | <0.001 |
| iASD | 5.04 | 2.39 | |||
| PMS | 1.90 | 2.00 | |||
| Tactile | TD | 1.44 | 1.69 | 47.79 | <0.001 |
| iASD | 5.44 | 2.75 | |||
| PMS | 4.67 | 2.72 | |||
| Auditory | TD | 1.06 | 1.38 | 31.75 | <0.001 |
| iASD | 4.32 | 2.85 | |||
| PMS | 2.98 | 2.68 |
| Total | Hyperreactivity | Hyporeactivity | Seeking | Visual | Tactile | Auditory | |
|---|---|---|---|---|---|---|---|
| PMS | 92.31% | 11.54% | 92.31% | 65.38% | 57.69% | 80.77% | 69.23% |
| iASD | 93.18% | 44.70% | 43.18% | 87.88% | 65.15% | 80.30% | 71.97% |
| Dx | ICC | 95% CI Range | Sig | |
|---|---|---|---|---|
| SAND | ||||
| Total | PMS | 0.879 | 0.674–0.956 | <0.001 |
| iASD | 0.834 | 0.653–0.920 | <0.001 | |
| Hyperreactivity | PMS | 0.736 | 0.296–0.903 | 0.003 |
| iASD | 0.665 | 0.297–0.839 | 0.002 | |
| Hyporeactivity | PMS | 0.775 | 0.368–0.919 | 0.003 |
| iASD | 0.766 | 0.512–0.887 | <0.001 | |
| Seeking | PMS | 0.821 | 0.495–0.936 | <0.001 |
| iASD | 0.91 | 0.813–0.957 | <0.001 | |
| Visual | PMS | 0.857 | 0.617–0.948 | <0.001 |
| iASD | 0.617 | 0.196–0.817 | 0.006 | |
| Auditory | PMS | 0.927 | 0.804–0.973 | <0.001 |
| iASD | 0.766 | 0.513–0.888 | <0.001 | |
| Tactile | PMS | 0.615 | −0.109–0.863 | 0.038 |
| iASD | 0.837 | 0.666–0.921 | <0.001 |
| Scores | Proportion Surpassed Clinical Threshold | |||||
|---|---|---|---|---|---|---|
| Domain/Subscale | Class I | Class II | p | Class I | Class II | p |
| Hyperreactivity | 3.83 (3.6) | 3.14 (2.5) | 0.679 | 16.67% | 4.55% | 0.176 |
| Hyporeactivity | 14.73 (6.2) | 18.18 (6.0) | 0.086 | 86.67% | 100.00% | 0.075 |
| Seeking | 10.07 (5.4) | 8.86 (6.4) | 0.504 | 70.00% | 59.09% | 0.414 |
| Visual | 7.83 (4.2) | 8.95 (2.8) | 0.199 | 46.67% | 72.73% | 0.06 |
| Auditory | 10.93 (3.7) | 11.59 (4.3) | 0.418 | 80.00% | 81.82% | 0.869 |
| Tactile | 9.87 (4.9) | 9.64 (3.3) | 0.918 | 66.67% | 72.73% | 0.64 |
| Visual Hyperreactivity | 0.80 (1.3) | 0.73 (1.4) | 0.798 | 0.00% | 4.55% | 0.238 |
| Visual Hyporeactivity | 5.10 (2.4) | 6.36 (1.9) | 0.073 | 66.67% | 77.27% | 0.404 |
| Visual Seeking | 1.93 (2.1) | 1.86 (1.9) | 0.977 | 16.67% | 9.09% | 0.429 |
| Tactile Hyperreactivity | 1.27 (1.6) | 2.05 (2.1) | 0.178 | 3.33% | 4.55% | 0.822 |
| Tactile Hyporeactivity | 4.83 (1.9) | 5.09 (2.8) | 0.562 | 66.67% | 59.09% | 0.575 |
| Tactile Seeking | 4.83 (2.3) | 4.45 (3.3) | 0.702 | 60.00% | 45.45% | 0.299 |
| Auditory Hyperreactivity | 1.77 (2.1) | 0.36 (0.8) | 0.011 * | 16.67% | 0.00% | 0.044 * |
| Auditory Hyporeactivity | 4.80 (3.0) | 6.73 (2.3) | 0.02 * | 53.33% | 81.82% | 0.033 * |
| Auditory Seeking | 3.30 (2.6) | 2.55 (2.8) | 0.26 | 26.67% | 27.27% | 0.961 |
| Total | 28.63 (11.1) | 30.18 (7.5) | 0.364 | 90.00% | 100.00% | 0.075 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavassoli, T.; Layton, C.; Levy, T.; Rowe, M.; George-Jones, J.; Zweifach, J.; Lurie, S.; Buxbaum, J.D.; Kolevzon, A.; Siper, P.M. Sensory Reactivity Phenotype in Phelan–McDermid Syndrome Is Distinct from Idiopathic ASD. Genes 2021, 12, 977. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12070977
Tavassoli T, Layton C, Levy T, Rowe M, George-Jones J, Zweifach J, Lurie S, Buxbaum JD, Kolevzon A, Siper PM. Sensory Reactivity Phenotype in Phelan–McDermid Syndrome Is Distinct from Idiopathic ASD. Genes. 2021; 12(7):977. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12070977
Chicago/Turabian StyleTavassoli, Teresa, Christina Layton, Tess Levy, Mikaela Rowe, Julia George-Jones, Jessica Zweifach, Stacey Lurie, Joseph D. Buxbaum, Alexander Kolevzon, and Paige M. Siper. 2021. "Sensory Reactivity Phenotype in Phelan–McDermid Syndrome Is Distinct from Idiopathic ASD" Genes 12, no. 7: 977. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12070977