
Evaluating TNF-α and Interleukin-2 (IL-2) Levels in African American Primary Open-Angle Glaucoma Patients

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Criteria
2.2. Genotyping
2.3. Sample Collection
2.4. ELISA to Assay IL-2 and TNF-α
TNF-α and IL-2 Concentration Normalization
2.5. Statistical Analysis
3. Results
3.1. Genotyping Analysis
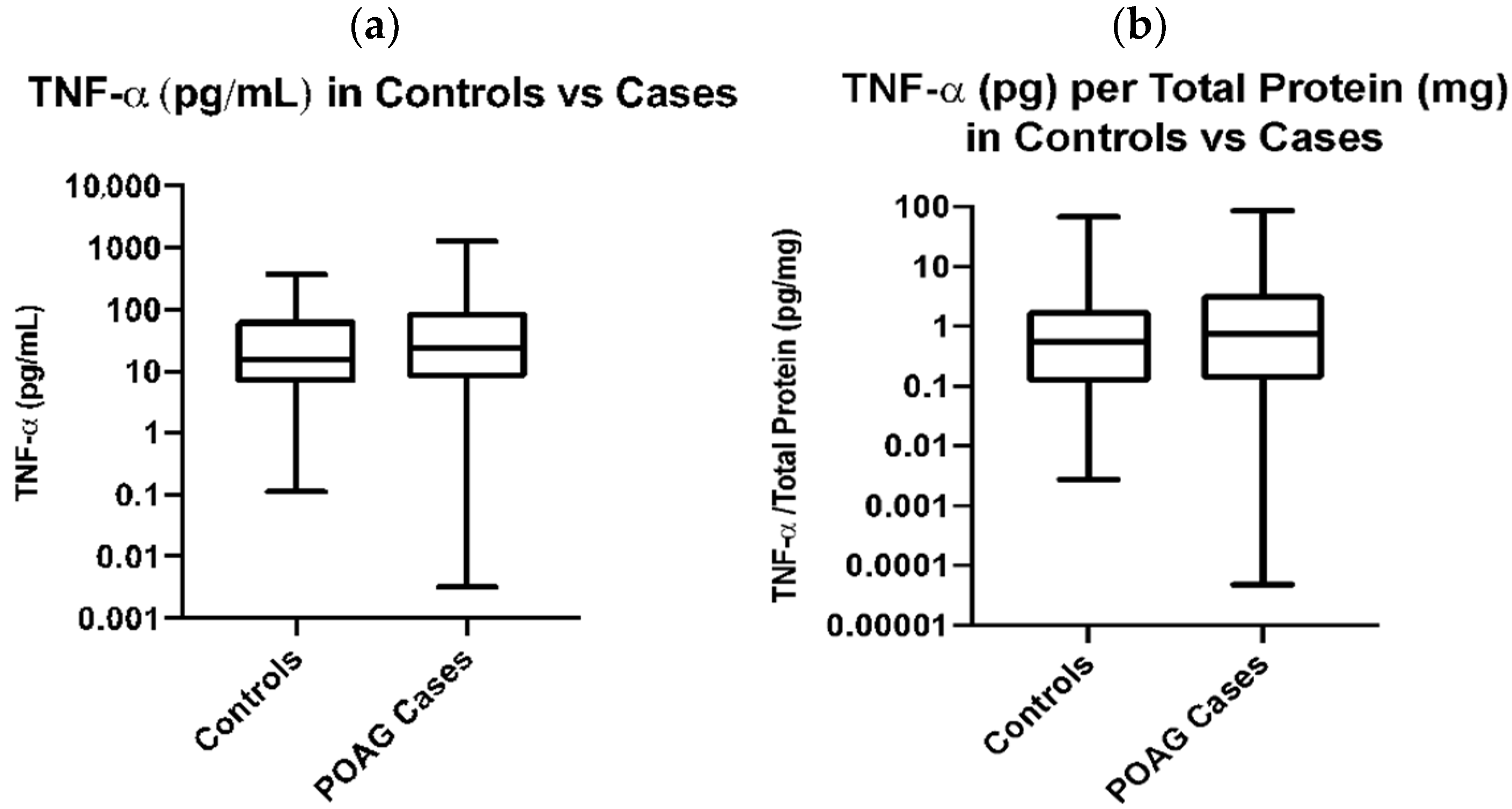
3.2. Association of Plasma TNF-α and IL2 with POAG
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwon, Y.H.; Fingert, J.H.; Kuehn, M.H.; Alward, W.L. Primary open-angle glaucoma. N. Engl. J. Med. 2009, 360, 1113–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinreb, R.N.; Khaw, P.T. Primary open-angle glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef]
- Caprioli, J. Intraocular pressure fluctuation: An independent risk factor for glaucoma? Arch. Ophthalmol. 2007, 125, 1124–1125. [Google Scholar] [CrossRef]
- Friedman, D.S.; Wolfs, R.C.; O’Colmain, B.J.; Klein, B.E.; Taylor, H.R.; West, S.; Leske, M.C.; Mitchell, P.; Congdon, N.; Kempen, J.; et al. Prevalence of open-angle glaucoma among adults in the United States. Arch. Ophthalmol. 2004, 122, 532–538. [Google Scholar] [CrossRef] [Green Version]
- Abu-Amero, K.; Kondkar, A.A.; Chalam, K.V. An Updated Review on the Genetics of Primary Open Angle Glaucoma. Int. J. Mol. Sci. 2015, 16, 28886–28911. [Google Scholar] [CrossRef] [Green Version]
- Flammer, J. The vascular concept of glaucoma. Surv. Ophthalmol. 1994, 38, S3–S6. [Google Scholar] [CrossRef]
- Marcic, T.S.; Belyea, D.A.; Katz, B. Neuroprotection in glaucoma: A model for neuroprotection in optic neuropathies. Curr. Opin. Ophthalmol. 2003, 14, 353–356. [Google Scholar] [CrossRef]
- Tezel, G.; Wax, M.B. The immune system and glaucoma. Curr. Opin. Ophthalmol. 2004, 15, 80–84. [Google Scholar] [CrossRef]
- Sommer, A.; Tielsch, J.M.; Katz, J.; Quigley, H.A.; Gottsch, J.D.; Javitt, J.; Singh, K. Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans. The Baltimore Eye Survey. Arch. Ophthalmol. 1991, 109, 1090–1095. [Google Scholar] [CrossRef]
- de Lemos, J.A.; Lloyd-Jones, D.M. Multiple biomarker panels for cardiovascular risk assessment. N. Engl. J. Med. 2008, 358, 2172–2174. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, A.H.; McGuire, J.; Hansson, O.; Zetterberg, H.; Podust, V.N.; Davies, H.A.; Waldemar, G.; Minthon, L.; Blennow, K. Novel panel of cerebrospinal fluid biomarkers for the prediction of progression to Alzheimer dementia in patients with mild cognitive impairment. Arch. Neurol. 2007, 64, 366–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, H.J.; Flammer, J.; Graf, T.; Stumpfig, D. Systemic blood pressure in glaucoma patients. Graefes. Arch. Clin. Exp. Ophthalmol. 1993, 231, 677–680. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, J.; Murphy, C.; Juster, R. Trabecular meshwork cellularity in primary open-angle glaucoma and nonglaucomatous normals. Ophthalmology 1984, 91, 564–579. [Google Scholar] [CrossRef]
- Izzotti, A.; Sacca, S.C.; Cartiglia, C.; De Flora, S. Oxidative deoxyribonucleic acid damage in the eyes of glaucoma patients. Am. J. Med. 2003, 114, 638–646. [Google Scholar] [CrossRef]
- Nagasubramanian, S.; Rahi, A.H.; Gloster, J. Immunological investigations in chronic simple glaucoma. Trans. Ophthalmol. Soc. UK 1978, 98, 22–27. [Google Scholar]
- Munoz-Fernandez, M.A.; Fresno, M. The role of tumour necrosis factor, interleukin 6, interferon-γ and inducible nitric oxide synthase in the development and pathology of the nervous system. Prog. Neurobiol. 1998, 56, 307–340. [Google Scholar] [CrossRef]
- Shi, J.; Lv, J.; Wu, H. Th1/Th2 cytokines and its clinical significance in obstructive sleep apnea hypopnea syndrome children without allergic rhinitis and asthma. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2012, 26, 1073–1076. [Google Scholar]
- Abrahamsson, T.R.; Sandberg Abelius, M.; Forsberg, A.; Bjorksten, B.; Jenmalm, M.C. A Th1/Th2-associated chemokine imbalance during infancy in children developing eczema, wheeze and sensitization. Clin. Exp. Allergy 2011, 41, 1729–1739. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.; Qi, Y.; Xu, Y.S.; Liu, J.; Liao, D.; Zhang, S.S.; Zhang, C. Serum cytokine alteration is associated with optic neuropathy in human primary open angle glaucoma. J. Glaucoma 2010, 19, 324–330. [Google Scholar] [CrossRef]
- Sanchez, R.N.; Chan, C.K.; Garg, S.; Kwong, J.M.; Wong, M.J.; Sadun, A.A.; Lam, T.T. Interleukin-6 in retinal ischemia reperfusion injury in rats. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4006–4011. [Google Scholar] [CrossRef] [Green Version]
- Koeberle, P.D.; Gauldie, J.; Ball, A.K. Effects of adenoviral-mediated gene transfer of interleukin-10, interleukin-4, and transforming growth factor-β on the survival of axotomized retinal ganglion cells. Neuroscience 2004, 125, 903–920. [Google Scholar] [CrossRef]
- Takai, Y.; Tanito, M.; Ohira, A. Multiplex cytokine analysis of aqueous humor in eyes with primary open-angle glaucoma, exfoliation glaucoma, and cataract. Investig. Ophthalmol. Vis. Sci. 2012, 53, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Tong, Y.; Zhou, Y.L.; Zheng, Y.; Biswal, M.; Zhao, P.Q.; Wang, Z.Y. Analyzing cytokines as biomarkers to evaluate severity of glaucoma. Int. J. Ophthalmol. 2017, 10, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.R.; Miao, H.; Tao, Y.; Li, X.X.; Wong, I.Y. Expression of cytokines on the iris of patients with neovascular glaucoma. Acta Ophthalmol. 2015, 93, e100–e104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, C.; Forster, V.; Balse, E.; Sahel, J.A.; Picaud, S.; Tessier, L.H. Retinal-cell-conditioned medium prevents TNF-α-induced apoptosis of purified ganglion cells. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2983–2991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tezel, G.; Yang, X.; Yang, J.; Wax, M.B. Role of tumor necrosis factor receptor-1 in the death of retinal ganglion cells following optic nerve crush injury in mice. Brain Res. 2004, 996, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Sawada, H.; Fukuchi, T.; Tanaka, T.; Abe, H. Tumor necrosis factor-α concentrations in the aqueous humor of patients with glaucoma. Investig. Ophthalmol. Vis. Sci. 2010, 51, 903–906. [Google Scholar] [CrossRef]
- Balaiya, S.; Edwards, J.; Tillis, T.; Khetpal, V.; Chalam, K.V. Tumor necrosis factor-α (TNF-α) levels in aqueous humor of primary open angle glaucoma. Clin. Ophthalmol. 2011, 5, 553–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondkar, A.A.; Sultan, T.; Almobarak, F.A.; Kalantan, H.; Al-Obeidan, S.A.; Abu-Amero, K.K. Association of increased levels of plasma tumor necrosis factor α with primary open-angle glaucoma. Clin. Ophthalmol. 2018, 12, 701–706. [Google Scholar] [CrossRef] [Green Version]
- Ertel, W.; Keel, M.; Bonaccio, M.; Steckholzer, U.; Gallati, H.; Kenney, J.S.; Trentz, O. Release of anti-inflammatory mediators after mechanical trauma correlates with severity of injury and clinical outcome. J. Trauma 1995, 39, 879–885; discussion 885–887. [Google Scholar] [CrossRef] [PubMed]
- Gudiseva, H.V.; Verma, S.S.; Chavali, V.R.M.; Salowe, R.J.; Lucas, A.; Collins, D.W.; Rathi, S.; He, J.; Lee, R.; Merriam, S.; et al. Genome wide-association study identifies novel loci in the Primary Open-Angle African American Glaucoma Genetics (POAAGG) study. bioRxiv 2020. [Google Scholar] [CrossRef]
- Charlson, E.S.; Sankar, P.S.; Miller-Ellis, E.; Regina, M.; Fertig, R.; Salinas, J.; Pistilli, M.; Salowe, R.J.; Rhodes, A.L.; Merritt, W.T., 3rd; et al. The Primary Open-Angle African American Glaucoma Genetics Study: Baseline Demographics. Ophthalmology 2015, 122, 711–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeger, S.L.; Liang, K.Y.; Albert, P.S. Models for longitudinal data: A generalized estimating equation approach. Biometrics 1988, 44, 1049–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, J.; Vania, M.; Cheung, C.M.; Ang, M.; Chee, S.P.; Yang, H.; Li, J.; Wong, T.T. Expression profile of inflammatory cytokines in aqueous from glaucomatous eyes. Mol. Vis. 2012, 18, 431–438. [Google Scholar]
- Borkenstein, A.; Faschinger, C.; Maier, R.; Weger, M.; Theisl, A.; Demel, U.; Graninger, W.; Irene, H.; Mossbock, G. Measurement of tumor necrosis factor-α, interleukin-6, Fas ligand, interleukin-1alpha, and interleukin-1beta in the aqueous humor of patients with open angle glaucoma using multiplex bead analysis. Mol. Vis. 2013, 19, 2306–2311. [Google Scholar]
- Knepper, P.A.; Mayanil, C.S.; Goossens, W.; Wertz, R.D.; Holgren, C.; Ritch, R.; Allingham, R.R. Aqueous humor in primary open-angle glaucoma contains an increased level of CD44S. Investig. Ophthalmol. Vis. Sci. 2002, 43, 133–139. [Google Scholar]
- Ray, S.; Britschgi, M.; Herbert, C.; Takeda-Uchimura, Y.; Boxer, A.; Blennow, K.; Friedman, L.F.; Galasko, D.R.; Jutel, M.; Karydas, A.; et al. Classification and prediction of clinical Alzheimer’s diagnosis based on plasma signaling proteins. Nat. Med. 2007, 13, 1359–1362. [Google Scholar] [CrossRef]
- Yang, J.; Patil, R.V.; Yu, H.; Gordon, M.; Wax, M.B. T cell subsets and sIL-2R/IL-2 levels in patients with glaucoma. Am. J. Ophthalmol. 2001, 131, 421–426. [Google Scholar] [CrossRef]
- Tomarev, S.I.; Wistow, G.; Raymond, V.; Dubois, S.; Malyukova, I. Gene expression profile of the human trabecular meshwork: NEIBank sequence tag analysis. Investig. Ophthalmol. Vis. Sci. 2003, 44, 2588–2596. [Google Scholar] [CrossRef] [Green Version]
- Knepper, P.A.; Samples, J.R.; Yue, B.Y. Biomarkers of primary open-angle glaucoma. Expert Rev. Ophthalmol. 2010, 5, 731–742. [Google Scholar] [CrossRef] [PubMed]
- Tezel, G. TNF-α signaling in glaucomatous neurodegeneration. Prog. Brain Res. 2008, 173, 409–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tezel, G.; Li, L.Y.; Patil, R.V.; Wax, M.B. TNF-α and TNF-α receptor-1 in the retina of normal and glaucomatous eyes. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1787–1794. [Google Scholar]
- Bruunsgaard, H.; Pedersen, B.K. Age-related inflammatory cytokines and disease. Immunol. Allergy Clin. N. Am. 2003, 23, 15–39. [Google Scholar] [CrossRef]
- Ahoor, M.H.; Ghorbanihaghjo, A.; Sorkhabi, R.; Kiavar, A. Klotho and Endothelin-1 in Pseudoexfoliation Syndrome and Glaucoma. J. Glaucoma 2016, 25, 919–922. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Normal (n = 72) | POAG Cases (n = 118) | p-Value |
|---|---|---|---|
| Age, mean (SD) (years) | 61.82 ± 11.49 | 71.29 ± 12.29 | <0.0001 |
| Gender (Female) | 52 (72%) | 72 (61%) | 0.12 |
| Gender (Male) | 20 (28%) | 46 (39%) | 0.31 |
| TNF-α, mean ± SD (pg/mL) | 60.6 ± 10.84 | 86.96 ± 15.42 | 0.68 |
| TNF-α (pg/mL) per total protein (mg/mL), mean ± SD | 2.47 ± 8.08 | 4.56 ± 10.89 | 0.29 |
| BMI | 32.3 ± 7.51 | 29.42 ± 6.12 | <0.003 |
| Variable | POAG Cases (n = 232) | Normal (n = 135) | p-Value |
|---|---|---|---|
| Age, mean (SD) (years) | 69.91 ± 12.42 | 63.11 ± 11.52 | <0.001 |
| Gender (Female) | 144 (62%) | 96 (71%) | 0.08 |
| Gender (Males) | 88 (38%) | 39 (29%) | 0.08 |
| IL-2, mean ± SD (pg/mL) | 26.12 ± 40.39 | 32.42 ± 61.28 | 0.45 |
| IL-2 in males (pg/mL) | 31.21 ± 45.51 | 34.92 ± 63.8 | 0.71 |
| IL-2 in females (pg/mL) | 23.01 ± 36.73 | 31.41 ± 60.53 | 0.96 |
| Variable | Males | Females | p-Value |
|---|---|---|---|
| IL-2 in Cases (n) (pg/mL) | 31.21 ± 45.51 (88) | 23.01 ± 36.73 (144) | 0.026 |
| IL-2 in Controls (n) (pg/mL) | 34.92 ± 63.81 (39) | 31.41 ± 60.53 (96) | 0.78 |
| IL-2 in Cases + Controls (n) (pg/mL) | 32.35 ± 51.58 (127) | 26.37 ± 47.76 (240) | 0.054 |
| Cases: IL-2 vs. Endophenotype | n | Spearman Rho | p-Value |
|---|---|---|---|
| Mean Intraocular Pressure | 423 | −0.14 | 0.03 |
| Latest Central Corneal Thickness | 375 | 0.00 | 0.98 |
| Baseline Cup-to-Disc Ratio | 382 | 0.04 | 0.55 |
| Baseline Retinal Nerve Fiber Layer Mean Thickness | 312 | −0.02 | 0.80 |
| Baseline Pattern Standard Deviation | 337 | −0.07 | 0.29 |
| Baseline Mean Deviation | 337 | 0.06 | 0.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alapati, T.; Sagal, K.M.; Gudiseva, H.V.; Pistilli, M.; Pyfer, M.; Chavali, V.R.M.; O’Brien, J.M. Evaluating TNF-α and Interleukin-2 (IL-2) Levels in African American Primary Open-Angle Glaucoma Patients. Genes 2022, 13, 54. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13010054
Alapati T, Sagal KM, Gudiseva HV, Pistilli M, Pyfer M, Chavali VRM, O’Brien JM. Evaluating TNF-α and Interleukin-2 (IL-2) Levels in African American Primary Open-Angle Glaucoma Patients. Genes. 2022; 13(1):54. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13010054
Chicago/Turabian StyleAlapati, Teja, Kyra M. Sagal, Harini V. Gudiseva, Maxwell Pistilli, Mark Pyfer, Venkata Ramana Murthy Chavali, and Joan M. O’Brien. 2022. "Evaluating TNF-α and Interleukin-2 (IL-2) Levels in African American Primary Open-Angle Glaucoma Patients" Genes 13, no. 1: 54. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13010054