
Assessing Health Impacts of Winter Smog in Lahore for Exposed Occupational Groups



1
Environmental Health and Wildlife Laboratory, Institute of Zoology, University of the Punjab, Lahore 54000, Pakistan
2
The International Centre for Integrated Mountain Development, Kathmandu 44700, Nepal
*
Authors to whom correspondence should be addressed.
Atmosphere 2021, 12(11), 1532; https://0-doi-org.brum.beds.ac.uk/10.3390/atmos12111532
Submission received: 7 October 2021
/
Revised: 5 November 2021
/
Accepted: 18 November 2021
/
Published: 20 November 2021
(This article belongs to the Special Issue Urban Air Pollution Exposure and Related Diseases)
Abstract
:The goal of this research was to investigate the health effects of winter pollution on various occupations in Lahore and its neighboring peri-urban areas. A questionnaire survey, key informants, and focused group discussions were employed to collect data, which included demographic, socioeconomic, and health-related information. Descriptive statistics and the multivariate logistic regression model (MLRM) were used to examine the effects of pollution on exposed occupational groups who experienced symptoms such as coughing, shortness of breath, and eye discomfort. According to data from interviews, MLRM revealed that individuals working in various occupations with outdoor and indoor environments are equally affected by winter smog, but being middle-aged (odds ratio OR = 5.73), having a history of a respiratory ailment (OR = 4.06), and location (OR = 2.26) all play important roles in determining health. However, less educated people, elders, and people who already live in polluted areas are more likely to develop respiratory health symptoms. During the smog incident, it was determined that diverse health and socioeconomic factors exacerbate an individual’s negative health impact more than others.
1. Introduction
Air pollution is associated with adverse health conditions, including cardiovascular diseases, diabetes, neurodegenerative disorders, reduced life expectancy, and the development of several types of cancers [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15].
Air pollution primarily has adverse effects on human health by causing and/or exacerbating respiratory, cardiovascular, and ocular problems, as well as affecting allergic responses (e.g., [16]). It also indirectly affects mortality in the region though visibility degradation and associated travel issues through the formation of fog and smog [17,18]. When water droplets are suspended in the air at ground level, fog forms. This is usually connected with low-level cooling of the air and the development of condensate, which can remain under stable conditions (e.g., low wind speeds and atmospheric inversions). In the presence of particle matter (both primary and secondary particulates), these water droplets can increase the potential for fog formation by boosting condensation nuclei and interacting chemically with fog droplets [19]. The smog results from the interaction of pollutants from, e.g., burning, recirculated dust, and industrial activity under humid conditions [20]. Gaseous pollutants such as sulfur dioxide (SO2), nitrogen oxides (NOx, the sum of nitrogen oxide (NO) and nitrogen dioxide (NO2)), and ozone (O3) are among the main constituents of winter smog [21]. The increase in cardiopulmonary diseases and respiratory diseases has generally been attributed to these gaseous components of winter smog and particulate matter [22,23,24].
Different components of air pollution affect human health in various ways; for example, NO2 has been shown to cause lung irritation by increasing inflammation of airways and may decrease immunity against respiratory infections [25]. Fine particulate matter (PM2.5) can potentially cause respiratory problems; due to its higher penetration into the alveoli, it can affect the deepest parts of the lungs [26,27].
The mechanisms through which PM2.5 harms respiratory health is of interest to researchers, with various theories being proposed. However, the most widely accepted theory is that it induces an inflammatory response, thus weakening the body’s immune system [1,28]. Ozone (O3), the major component of urban smog, is a highly reactive compound that causes tissue damage, also in addition to sensitizing the respiratory system to other irritants resulting in reduced lung function [29]. Singh et al. [30] and Khanum et al. [31] reported adverse health effects and disruption to normal life due to higher smog incidences during the winter season in India and Pakistan. It has also been reported that exposure to smog in early life may cause severe asthma, while mortality rates for the elderly have also been found to be higher during the winter months [32,33].
In addition to health effects, the higher frequency of winter smog events severely affects the everyday life of millions of people in the form of traffic delays, poor visibility, and disturbed daily routines [34,35]. Countries across Asia have experienced rapid industrial and economic growth, population increases, and urbanization [36,37]. Increased air pollution in the regionally expanded urban area and its density have resulted in the exposure of large urban populations to poor air quality [38]. Pakistan has one of the most rapidly increasing urban populations in the region. It is estimated that a total of 4,705,933 DALYs (number of disability-adjusted life years) are lost in Pakistan with 121,301 individuals dying annually from ambient air pollution-related illnesses [38].
The State of Global Air report (2020) included Asian countries (India, Nepal, Bangladesh, and Pakistan) among the top 10 countries with the highest PM2.5 levels, which were also described as nations with the highest recorded mortality rates. In 2015, 135,000 premature deaths (highest among the 10 most populous countries) owing to poor air quality were reported in Pakistan [39], which rose to 236,000 in 2019 according to The State of Global Air report (2020). The incidence of respiratory health problems increases in the winter season (November–December) in Pakistan [40,41]. Bulbul et al. [42] associated winter season foggy conditions with multiple health risks including respiratory disease, cardiovascular disease, and allergic reaction.
Lahore, the second-largest city of Pakistan, is growing at a rate of 4% per annum and is the most polluted Pakistani city [43,44]. In past studies, a successive increase of 61% in atmospheric aerosol optical depth (AOD) was recorded for winter periods. Similarly, other studies have also highlighted the problem of increasing air pollution in Lahore [35]. Alongside these, studies reported a sharp increase in cases of pulmonary, coronary, and cardiovascular diseases over the same time period (November–December) in Lahore, which was linked to urban air pollution [45,46].
Although there is a growing body of literature on air pollution’s impact on human health in the region, there is still a scarcity of literature regarding the impact of winter smog on the most vulnerable occupational groups in urban centers. We hypothesized that not everybody is exposed to air pollution equally as they go about their daily life. Exposure levels associated with area type and occupation play an important role in disease intensity and frequency among the population [47]. There are a broad range of studies that discussed the monetary disease burden using either data acquired from hospitals (e.g., [27,48,49,50,51]) or the direct relationship of air pollutants with health by estimating lung capacity [28,29,35,40,52].
The impact of air pollution on occupational health and livelihood loss is receiving attention, and data continue to demonstrate the significance of additional research in this field [43,52]. Lahore is a diverse area containing a range of types of urban and industrial land use. It provides livelihood opportunities for millions of people belonging to different occupations and social classes. However, there have been no studies on the role of occupational exposure linked to winter smog in Lahore, and there are very few studies quantifying the impact of winter smog on health [31,53,54,55]. The objective of this study was to assess the effect of winter smog on various occupational groups that are most exposed to poor air quality in their workplace and have the lowest coping capacity. Furthermore, the importance of location was investigated by comparing the situation in the urban core (Lahore municipality) and more peripheral areas.
2. Materials and Methods
2.1. Study Area
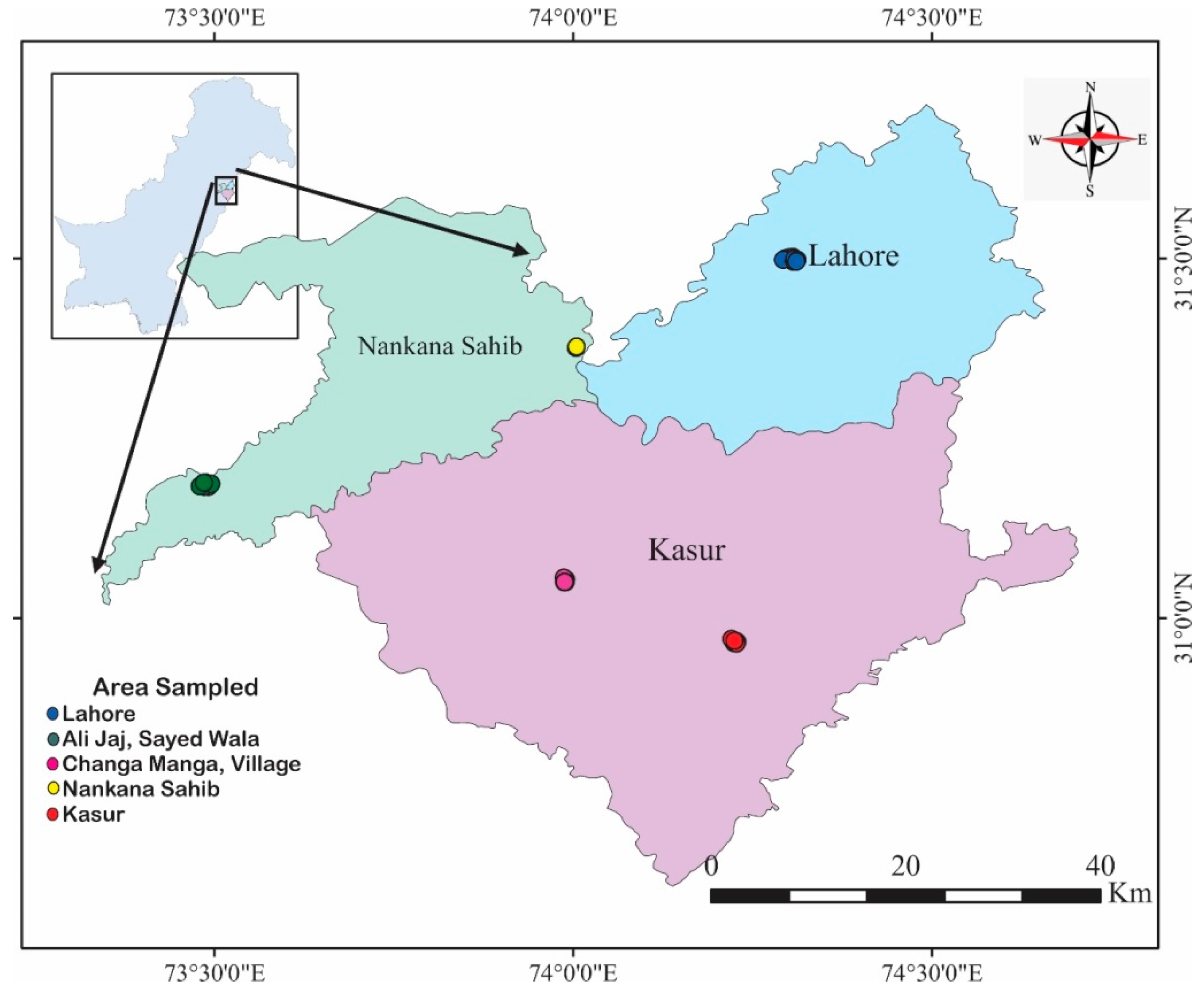
Because of a high incidence of winter smog and air pollution [56], Lahore city (capital of the Punjab province, Pakistan) and its adjoining areas were selected as the study domain (Figure 1). Lahore (31.5204° N, 74.3587° E) is a mega city with a population of 11.13 million, which has doubled in the last 15 years (growth rate of 3.58% to the year 2017). Major industrial activity in Lahore includes the chemical, automobile, manufacturing, and pharmaceutical sectors. The city is located in a subtropical arid setting with high industrial and vehicular load [57], leading to an increase in air pollution [56,57,58] and subsequent health issues [59]. The adjoining areas of Lahore municipality were included in order to compare the relative importance of location, i.e., between the urban core and the periphery. The study included the peripheral cities of Nankana, Kasur, Changa Manga, and Sayed Walla (Figure 1). In both areas, fog is a common meteorological phenomenon occurring in the winter (November–January), which results in smog when the various sources of pollution interact with the fog.
2.2. Data Collection
The main data for this study were collected through semi-structured interviews of individuals working in selected occupations (farmers, shopkeepers, office workers, drivers, household workers, and laborers). A total of 341 individuals were randomly selected and interviewed from different occupations and locations (Table 1). To facilitate the interviews, a semi-structured questionnaire was prepared, which was tested before the main survey and finalized. The questionnaire was translated into local languages (Urdu and Punjabi) for ease of understanding before the survey. The survey was conducted in November–December 2018. In addition to the individual interviews, information was collected through focus group discussions (FGD), key informant interviews (KII), and direct field observations. In each study site, at least one FGD and one KI interview were conducted. In the FGDs, efforts were made to ensure participation of individuals from different occupational groups.
For key informant interviews, mainly town representatives (known locally as Numbardar) and health practitioners (medical doctors) were identified for in-depth interviews in order to understand local context, as well as cross-validate survey data. Efforts were made to include at least one people’s representative in each study sites. In total, 35 medical doctors were interviewed using a prepared checklist with open-ended questions related to health, hospital admissions, and emergency cases during these periods. They were further questioned about perceived vulnerable locations and populations belonging to various occupations that are considered most likely to be affected by episodes of poor air quality (Table 1). The secondary data consisted of various scientific reports, maps, journal articles, and newspaper reports.
2.3. Data Analysis
The major objective of the study was to identify determinants of pulmonary disease and symptoms, particularly the role of ambient air pollution. For this, a multivariate logistic regression approach was chosen as the appropriate regression model following Ali et al. [60] and Sheikh and Akter [53]. Occupations with high exposure to ambient air pollution were used as a variable of interest. In addition to exposure to air pollution, other factors such as age, sex, socioeconomic status, and pre-existing conditions can influence the onset and severity of the adverse health impacts. Several control variables were also considered for this study (Table 2). The study mainly relied on descriptive statistics to analyze the survey data. To estimate the prevalence of disease, Equation (1) was used.
where P is the prevalence of a particular disease (%), Nd is the number of individuals suffering from a particular disease at the time of the survey, and NT is the total number of individuals studied.

{kind=link}
Table 2.
Variables associated with determinants of health symptoms.
| Variables 1 | Categories | Percentage |
|---|---|---|
| Gender | Male | 78 |
| Female | 22 | |
| Occupation group | Farmer | 19 |
| Household | 16 | |
| Labor | 18 | |
| Shopkeeper | 18 | |
| Driver | 14 | |
| Office employee | 15 | |
| Age (years) | 16–20 | 5 |
| 21–44 | 74 | |
| 45–64 | 17 | |
| >65 | 4 | |
| Literacy level | Illiterate | 30 |
| Primary | 20 | |
| High school | 24 | |
| Higher | 26 | |
| Smoking habit | Yes = 1 | 41 |
| No = 0 | 59 | |
| History of respiratory diseases | Yes = 1 | 22 |
| No | 78 | |
| Location | If location is Lahore = 1 | 17 |
| Otherwise = 0 | 83 | |
| Coping measures | Yes = 1 | 37 |
| No = 0 | 63 |
1 Total number of observations = 341; categories under the complex variables of gender, occupation group, age, and literacy level were operationalized as dummy variables (1, 0), and one of the categories under each complex variable was taken as the referent category. Table 3 presents the referent categories.
Table 3.
Prevalence of diseases among different occupations.
| Diseases | Farmer (n 1) | Unpaid Household Worker (n) | Labor (n) | Shopkeeper (n) | Office Goers (n) | Driver (n) | Total (n) | Prevalence (%) |
|---|---|---|---|---|---|---|---|---|
| Respiratory | 16 | 9 | 21 | 11 | 8 | 13 | 78 | 22.9 |
| Allergy | 4 | 12 | 8 | 9 | 7 | 8 | 48 | 14.1 |
| Cardiac | 3 | 3 | 1 | 1 | 1 | 2 | 11 | 3.2 |
| Neural disorders | 0 | 1 | 1 | 0 | 1 | 1 | 4 | 1.1 |
| Other non-respiratory diseases | 4 | 4 | 2 | 4 | 4 | 2 | 20 | 5.8 |
| Total | 27 | 29 | 33 | 25 | 21 | 26 | 116 |
1 Frequency of cases.
Logistic regression was used to investigate statistical association of risk factors with the occurrence of symptoms as a function of odds ratios (ORs) and 95% confidence intervals (CI). The significance of association of prevalence with these risk factors and differences between groups were tested at the 95% significance interval (p = 0.05).
The analysis was proceeded by studying the prevalence of each of the symptoms during winter fog events. The most prevalent symptoms among the surveyed individuals were selected. The next step consisted of analyzing predictors of health symptoms among various exposure groups. Logistic regression analysis (multivariate) was used to predict occurrence of symptoms in these groups. If we define as the probability of the symptom being present (i.e., 1), the multiple logistic regression can be presented as shown in Equation (2).
where X1, X2 … Xp represent the predictor variables in the equation, β0 is the intercept, and β1, β2, … βp are coefficients of the respective variables. Five outcome variables (symptoms), cough, phlegm, wheezing, breathlessness, and eye irritation, were taken into
consideration after adjudging that their prevalence was relatively higher than other symptoms. Several predictors were tested as independent variables to test the significance of odds of the incidence of the symptoms.
3. Results
3.1. Descriptive Results
The descriptive analysis of surveyed individuals is summarized in Table 2. The respondents were predominantly male (78%), reflecting the local cultural context where mostly men work outside the home and women take care of household work. Most women respondents were unpaid household workers, and some were involved in farming, factory labor, or office work. Almost half of the respondents were either illiterate or had only a primary level of education, and a majority of the respondents were in the age group of 20–45 years.
Overall, about 47% of the respondents reported having some form of pre-existing health condition. Respiratory diseases (23%) were the most reported pre-existing health issue, followed by allergies (14%). There was some difference in the type of pre-existing health issues reported by respondents involved in outdoor and indoor occupations. Whereas respondents exposed to outdoor ambient air pollution such as taxi drivers, laborers, and farmers reported respiratory diseases, the indoor occupation group (office workers and household workers) reported both allergy and respiratory disease in equal frequency. Additionally, respondents claimed that symptoms intensified in November and December when compared to other months.
3.2. Perception of Occupational Impacts of Winter Smog
The majority of the respondents (91%), irrespective of the occupation, reported that smog negatively affects their health. Laborers (60%), shopkeepers (57%), and farmers (57%) reported that, during the smog period, their livelihood was affected in terms of work efficiency, work availability, and mobility challenges.
During the winter smog period, 41% (n = 139) respondents stated that smog affects their daily routine and work, including their family life and their children missing school after being sick or due to the smog alerts issued by local authorities. Among these individuals, drivers (46%) and farmers (27%) were reported to be the most vulnerable to environmental factors. Laborers who work on daily wages and who work in construction or road work complained about smog affecting their job availability, as well as their work efficiency. Despite their vulnerability, only 38% of the total respondents were taking any coping measures; among them, the office goers were in the majority (71%) practicing one or more preventive measures. This was mainly due to the awareness, resources, and nature of the job, which were lacking in other occupations.
In addition to the individual survey, further information was gathered through FGD and KII, which helped to validate the findings of the individual survey. Although all the occupational groups were affected by winter smog, the degree and the way they were affected varied among the occupational groups. Drivers were reported to be highly susceptible to considerable loss of income as fog causes low visibility. On the other hand, the public tended to remain indoors during days of low visibility and high smog, thus impacting their earnings. The farmers reported that low sunlight during the smog days causes reduced crop productivity. Most of the farmers reported suffering from respiratory diseases and eye irritation during the smog period, with the symptoms getting worse in the morning and evening hours. Office employees were considered to be less socioeconomically affected by winter smog as they were not dependent on daily wages. Almost all respondents, irrespective of their occupation, were found to be concerned about their children’s health during the smog period. This fear was justified by the key informants (doctors) who declared children and elders as the most susceptible age groups. The common diseases and symptoms experienced during the smog period were perceived to be eye irritation, breathlessness, respiratory diseases, and skin allergies. The majority of respondents did not know that the diseases and symptoms they reported were due to winter smog; instead, they attributed the diseases to cold weather, whereas some even associated it with the wrath of God upon the people.
A total of 43 interviews were conducted with key informants: 35 medical practitioners and eight people’s representatives from the study sites. The results of KI interviews validated the individual survey findings. The medical professionals reported receiving patients with respiratory tract infections, allergies, ENT disorders, and eye irritations on smog days mostly from November to January. They considered the increase in dust particles, higher vehicular load, agricultural burning, and higher rates of industrialization as the reasons for increased incidence of winter smog. They stated that the most susceptible groups were children and elderly people from poor families, but the symptoms were not limited to certain groups.
3.3. Logistic Regression Results
Four separate logistic regression models were run: for four symptoms considered simultaneously (cough, phlegm, and wheezing) and for individual symptoms of coughing, breathlessness, and eye irritation. Results of the multi-symptom model revealed that gender, occupational groups, smoking habit, and coping measures did not have a statistically significant relationship with symptoms (Table 4). Among age groups, the middle-aged group (45–64 years) showed a statistically significant relationship with symptoms (p = 0.01). A history of respiratory diseases and the location of respondents showed a very strong statistical relationship with symptoms. Statistically significant (p < 0.05) variables can be considered as key identified factors that influence the probability of having symptoms. Values of odds ratios of the statistically significant variables revealed that the middle-aged group had almost a six times higher likelihood of facing multiple symptoms than adolescents (<20 years). Among literacy levels, the respondents with a primary level had almost an 80% higher probability of having multiple symptoms than illiterates. A history of respiratory disease increased the chances of facing multiple symptoms fourfold. It was found that staying in the urban area (Lahore metropolitan area) increased the odds of facing symptoms 2.26-fold (Table 4).
Results of the cough symptom model showed that the middle-aged group, primary level of literacy, history of respiratory diseases, and location had a statistically significant positive relationship with cough (p = 0.01, 0.0, and 0.01, respectively). Values of odds ratios for these statistically significant variables revealed that the middle-aged group had almost a six times higher likelihood of having cough compared to adolescents. The respondents with a primary literacy level had 80% higher chances of having cough compared to illiterates. Moreover, a history of respiratory diseases resulted in almost four times higher likelihood of having a cough. Living in urban areas (Lahore) was also likely to double the chances of having cough (Table 4).
Results of the model for the breathlessness symptom revealed the statistically significant relationship of only two variables with the symptom of breathlessness: old age group and history of respiratory diseases. Values of OR showed that the old age group had around six times higher likelihood of facing the symptom of breathlessness compared to adolescents. Similarly, a history of respiratory diseases was likely to increase the chances of facing breathlessness more than sixfold (Table 4). Regression analysis of the eye irritation symptom revealed that the categories of shopkeepers, adults, and the middle-aged group had a statistically significant positive relationship with the symptom of eye irritation. However, living in the urban areas (Lahore) had statistically significant but negative relationship with eye irritation. Values of odds ratios showed that adults and middle-aged groups had almost three times higher chances of having eye irritation compared to adolescents. Shopkeepers were two times more likely to face the symptom of eye irritation than the office employees. Interestingly, living in urban areas was likely to reduce the chances of having the symptom eye irritation by 68% compared to rural and peri-urban areas (Table 4).
4. Discussion
Our results show that increased episodes of winter smog adversely affected the health and livelihood of inhabitants of this study area and potentially other similar urban areas. A higher incidence of smog, especially in November/December, forced residents to restrict their occupational activities due to its adverse health impacts and restricted mobility due to poor visibility. Most of the prevalent health symptoms reported were related to respiratory ailments such as cough, phlegm, wheezing, and shortness of breath. Similar results were reported by Ali et al. [60] in their study in Rawalpindi, Pakistan.
No significant differences were observed in the occurrence of various health symptoms by occupational groups. This contradicts our hypothesis that people working outdoors with prolonged exposure to ambient air pollution are impacted differently than those working indoors. Such an observation indicates that, irrespective of indoor or outdoor activity, ambient air pollution during the most polluted time of the year affects everyone almost equally. Only in the case of eye irritation did shopkeepers report a higher (almost double) occurrence of this symptom compared to office workers. Although the logistic analysis highlighted that indoor and outdoor occupations were equally susceptible to air pollution, the self-reported health symptoms showed a variation among different occupational groups. For example, the outdoor workers were found to be most affected by respiratory problems, whereas household workers and other indoor workers were more prone to allergies (Table 3). Furthermore, the study revealed that indoor workers such as office workers and household workers were most likely to wear a mask when they went outdoors as compared to the other occupational groups potentially more exposed to ambient air pollution.
The logistic regression identified variables that had a significant influence on the occurrence of multiple symptoms (cough, breathlessness, and eye irritation). Age was an important variable influencing the occurrence of symptoms in individuals. The middle-aged group was almost six times more likely to exhibit multiple symptoms or cough and three times more likely to exhibit eye irritation than adolescents. The old age group was six times more likely to exhibit breathlessness and three times more likely to exhibit eye irritation compared to the adolescent group. A study by Ali et al. [60] and multiple other studies also reported that the population groups which are exposed to the air pollution for longer periods of time suffer from health symptoms such as cough and eye irritation and reduced lung capacity in later stages of life [27,28,49,61].
Across all literacy levels, respondents with less education had an almost 80% greater likelihood of having multiple symptoms, including cough, than respondents with a higher literacy level. This study shows the importance of education and awareness about air pollution and its impact. This was also reflected in the KII and FGD discussions. During the discussion, it was reported that people with education (up to graduation level) were found to be less prone to air pollution due mainly to the fact that they were more aware regarding winter smog from print and social media and could take necessary precautions. Neidell [62] reported that the net effect of air pollution is greater on individuals from low-socioeconomic and -literacy backgrounds. Riaz and Hamid [54] report that the poor are likely to have lower educations levels and be more susceptible to air pollution due to a lack of awareness, malnutrition, and an unhealthy environment. A higher ratio of monetary disease burden was identified on the lower socioeconomic class, whereby higher mortality and morbidity rates were described by Patanker and Trivedi [49,63]. This study is in line with the perception that less educated people belonging to a lower socioeconomic class are impacted most by air pollution mainly due to high exposure to ambient air pollution during fog periods and development of health symptoms due to dense fog, leading to the loss of livelihood and daily wages [19,53].
A history of respiratory diseases was another important variable contributing to the exhibition of the symptoms in the sample. The existence of respiratory disease history increased the chances of facing multiple symptoms and cough symptoms fourfold and of facing breathlessness sixfold. We found that 22.9% of the population had pre-existing respiratory problems and, among these, most of the population (70%) showed acute respiratory health symptoms during the winter fog episodes (Table 4). This is a logical finding, as people with respiratory disease history have already compromised lung capacity, which is further aggravated by the intense air pollution [64,65,66]. These findings are also endorsed by other studies such as Silva et al. [67], Asl et al. [68], and Rovira et al. [69].
The adverse impact of air pollution is influenced by the location of the residence. Generally, respondents living in urban areas of Lahore (Lahore metropolitan areas) were more likely to exhibit respiratory disease symptoms as compared to the peri-urban areas. Urban respondents were twice as likely to report multiple symptoms and cough symptoms than those living in peri-urban areas. This could be explained by the difference in the pollution concentration between the Lahore metropolitan area and its peripheral areas [41,70]. Lahore reports the highest concentrations of PM2.5 as compared to other neighboring cities. The average concentrations of PM2.5 were 292 and 330 µg/m3 in October and November 2019, respectively [44]. These elevated concentrations of PM2.5 during smog episodes are mainly due to the increased industrial and vehicular emissions, agricultural burning practices, and meteorological conditions around the city and across the border, as indicated by KI [71]. In smog formation, meteorology plays a significant role as the planetary boundary layer is lowered during the wintertime, due to which pollutants are not dispersed compared to the summer season, leading to an increased aerosol load, especially elevating the concentrations of fine particulate matter (PM2.5) [72].
Nevertheless, adjoining cities showed a one-third concentration of PM2.5 as compared to Lahore. Such a higher ratio of air pollution in Lahore may be associated with higher vehicular and industrial load in Lahore than the other cities, as Lahore sustains a population that is much higher than its neighboring large cities (e.g., Islamabad and Faisalabad). However, in contrast, peri-urban respondents reported higher incidences (68% more) of eye irritation as compared to urban respondents. This is counterintuitive, as air pollution is expected to increase eye irritation. One explanation for this could be the difference in activities and the type of pollution. In rural and peri-urban areas, agriculture is a major source of livelihood. Thus, smoke is a major source of air pollution. The winter season coincides with the practice of large-scale crop residue open burning [4,73], resulting in a smoky environment and higher levels of suspended soot particles in the air. This explains the higher reports of eye irritation in peri-urban areas. An additional reason could be associated with the low literacy rate in these peri-urban areas, which result in local populations groups not taking adequate measures to reduce the effects of agricultural burning and other related activities [74].
Lastly, it is believed that avoidance behaviors or coping mechanisms such as staying at home, using masks (especially masks with appropriate filters), and installing indoor air purifiers all play a vital role in reducing exposure and, therefore, the adverse effects of air pollution [62]. Wearing masks, occasionally minimizing outdoor working hours, or avoiding travel in intense smog episodes were avoidance behaviors reported by the respondent in the study. These coping measures might not be sufficiently effective mainly due to the higher intensity of smog. In addition, people reported behavioral constraints in wearing masks. Taking holidays during extreme smog events might not be feasible for the highly vulnerable occupations described here. Thus, for the poorest and most exposed population, avoiding air pollution exposure even during peak pollution events is a challenge, making them extremely vulnerable to the impacts of poor air quality.
5. Conclusions
According to interviews with individuals working in a variety of occupations with both outdoor and indoor work environments, this study concludes that, while winter smog affects all selected occupations equally, age, pre-existing health conditions, and location all have a significant impact on health outcomes in this purview. It was found that certain health and socioeconomic situations exacerbate the adverse health impact of individuals more than others. The existence of respiratory disease history increased the chances of facing multiple respiratory health symptoms in individuals. Similarly, middle-aged people and people with low literacy were more susceptible to respiratory health symptoms. While all the occupation groups, regardless of the nature of their job, were affected by ambient air pollution during winter smog, very few of them reported taking coping measures, and those measures were also not effective to protect them against the respiratory hazards posed by smog. This finding shows that the occupational groups most exposed to outdoor ambient air pollution were facing multiple vulnerabilities. Not only was their work in the informal sector highly vulnerable due to a lack of income/economic security, but it also further compelled them to work even during intense smog episodes, thus adversely affecting their health. The study has some important implications for the policymakers such as (i) the importance of regular monitoring of pollution levels, particularly during the winter period and providing necessary advisories, (ii) organizing awareness campaigns about the adverse health impact of air pollution, particularly targeting vulnerable occupation groups, (iii) finding and disseminating mitigation measures (to reduce air pollution) and promoting coping measures (for an individual’s protection from air pollution), and (iv) including vulnerable occupational groups and their challenges in the decision-making process.
Author Contributions
Conceptualization, F.J., Z.A. and A.M.; methodology, F.J. and Z.A.; data curation, F.J., A.M. and Z.A.; writing—review and editing, F.J., Z.A. and A.M.; supervision, A.M. and Z.A. All authors have read and agreed to the published version of the manuscript.
Funding
The International Center for Integrated Mountain Development ICIMOD is thanked for graciously awarding the Ph.D. fellowship and rendering financial support and mentorship to conduct this research.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the zoology department University of the Punjab, Lahore, Pakistan ethical clearance certificate reference number D-1130-02, dated 19 September 2019.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data can be made available upon request.
Acknowledgments
We would like to thank Sugat Bajracharya for his valuable time and analytical skills and Abid Hussain, Haider Abbas Khawaja, and Iqbal Mead for their valuable suggestions. The financial support for this paper was provided by ICIMOD and ICIMOD gratefully acknowledges the support of its core donors: the Governments of Afghanistan, Australia, Austria, Bangladesh, Bhutan, China, India, Myanmar, Nepal, Norway, Pakistan, Sweden, and Switzerland. The views and interpretations in this publication are those of the authors and are not necessarily attributable to ICIMOD.
Conflicts of Interest
The authors have declared no conflict of interest.
References
- Sui, X.; Zhang, J.; Zhang, Q.I.; Sun, S.; Lei, R.; Zhang, C.; Cheng, H.; Ding, L.; Ding, R.; Xiao, C.; et al. The short-term effect of PM2.5/O3 on daily mortality from 2013 to 2018 in Fefei, China. Environ. Geochem. Health 2021, 43, 153–169. [Google Scholar] [CrossRef] [PubMed]
- Gauderman, W.J. Sample size requirements for matched case-control studies of gene–environment interaction. Stat. Med. 2002, 21, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., 3rd; Hansen, M.L.; Long, R.W.; Nielsen, K.R.; Eatough, N.L.; Wilson, W.E.; Eatough, D.J. Ambient particulate air pollution, heart rate variability, and blood markers of inflammation in a panel of elderly subjects. Environ. Health Pers. 2004, 112, 339–345. [Google Scholar] [CrossRef]
- Liu, T.; Mickley, L.J.; Gautam, R.; Singh, M.K.; De Fries, R.S.; Marlier, M.E. Detection of delay in post-monsoon agricultural burning across Punjab, India: Potential drivers and consequences for air quality. Environ. Res. Let. 2021, 16, 014014. [Google Scholar] [CrossRef]
- Kampa, M.; Castanas, E. Human Health effects of Air Pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef]
- Arbex, M.A.; Santos, U.D.P.; Martins, L.C.; Saldiva, P.H.N.; Pereira, L.A.A.; Braga, A.L.F. Air pollution and the respiratory system. J. Bras. Pneumol. 2012, 38, 643–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khwaja, H.A.; Fatmi, Z.; Malashock, D.; Aminov, Z.; Kazi, A.; Siddique, A.; Qureshi, J.; Carpenter, D.O. Effect of air pollution on daily morbidity in Karachi, Pakistan. J. Local Glob. Health Sci. 2012, 2012, 3. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Ebenstein, A.; Greenstone, M.; Li, H. Evidence on the impact of sustained exposure to air pollution on life expectancy from China’s Huai River policy. Proc. Natl. Acad. Sci. USA 2013, 110, 12936–12941. [Google Scholar] [CrossRef]
- Janssen, B.G.; Godderis, L.; Pieters, N.; Poels, K.; Kiciński, M.; Cuypers, A.; Fierens, F.; Penders, J.; Plusquin, M.; Gyselaers, W.; et al. Placental DNA hypomethylation in association with particulate air pollution in early life. Part. Fibre Toxicol. 2013, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Jung, C.R.; Lin, Y.T.; Hwang, B.F. Air pollution and newly diagnostic autism spectrum disorders: A population-based cohort study in Taiwan. PLoS ONE 2013, 8, e75510. [Google Scholar]
- Kloog, I.; Ridgway, B.; Koutrakis, P.; Coull, B.A.; Schwartz, J.D. Long-and short-term exposure to PM2.5 and mortality: Using novel exposure models. Epidemiology 2013, 24, 555. [Google Scholar] [CrossRef]
- Tsai, S.S.; Chang, C.C.; Yang, C.Y. Fine particulate air pollution and hospital admissions for chronic obstructive pulmonary disease: A case-crossover study in Taipei. Int. J. Environ. Res. Public Health 2013, 10, 6015–6026. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Myung, W.; Won, H.H.; Shim, S.; Jeon, H.J.; Choi, J.; Carroll, B.J.; Kim, D.K. Association between air pollution and suicide in South Korea: A nationwide study. PLoS ONE 2015, 10, e0117929. [Google Scholar] [CrossRef] [PubMed]
- Kioumourtzoglou, M.A.; Schwartz, J.D.; Weisskopf, M.G.; Melly, S.J.; Wang, Y.; Dominici, F.; Zanobetti, A. Long-term PM2.5 exposure and neurological hospital admissions in the northeastern United States. Environ. Health Perspect. 2016, 124, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Shi, X.; Brasseur, G.P. The response in air quality to the reduction of Chinese economic activities during the COVID-19 outbreak. Geophys. Res. Lett. 2020, 47, e2020GL088070. [Google Scholar] [CrossRef]
- Tsai, S.; Cheng, M.; Chiu, H.; Wu, T.; Yang, C. Air Pollution and hospital admissions for asthma in a tropical city: Kaohsiung, Taiwan. Inhal. Toxicol. 2006, 18, 549–554. [Google Scholar] [CrossRef]
- Gurjar, B.R.; Ravindra, K.; Nagpure, A.S. Air pollution trends over Indian megacities and their local-to-global implication. Atmos. Environ. 2016, 142, 475–495. [Google Scholar] [CrossRef]
- Vega, E.; Eidels, S.; Ruiz, H.; Lopez-Veneroni, D.; Sosa, G.; Gonzalez, E.; Gasca, J.; Mora, V.; Reye, E.; Sanchez-Reyna, G.; et al. Particulate air pollution in Mexico City: A detailed view. Aerosol Air Qual. Res. 2010, 10, 193–211. [Google Scholar] [CrossRef] [Green Version]
- Ali, K.; Acharja, P.; Trivedi, D.K.; Kulkarni, R.; Pithani, P.; Safai, P.D.; Chate, D.M.; Ghude, S.; Jenamani, R.K.; Rajeevan, M. Charecterization and source identification of PM2.5 and its chemical and carbonaceous constituents during winter fog experiment 2015-16 at Indira Gandhi International Airport, Delhi. Sci. Total Environ. 2019, 662, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Tao, M.; Chen, L.; Xiong, X.; Zhang, M.; Ma, P.; Tao, J.; Wang, Z. Formation process of the widespread extreme haze pollution over northern China in January 2013: Implications for regional air quality and climate. Atmos. Environ. 2014, 98, 417–425. [Google Scholar] [CrossRef]
- Perez-Diaz, J.L.; Ivanov, O.; Peshev, Z.; Alvarez-Valenzuela, M.A.; Valiente-Blanco, I.; Evgenieva, T.; Dreischuh, T.; Gueorguiev, O.; Todorov, P.V.; Vaseashta, A. Fogs: Physical basis, characteristic properties, and impacts on the environment and human health. Water 2017, 9, 807. [Google Scholar] [CrossRef] [Green Version]
- WHO. Health Effects of Particulate Matter: Policy Implications for Countries in Eastern Europe Caucasus and Central Asia; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Zeng, Y.; Cao, Y.; Qiao, X.; Seyler, B.C.; Tang, Y. Air pollution reduction in China: Recent success but great challenge for the future. Sci. Total Environ. 2019, 663, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Badyda, A.J.; Grellier, J.; Dąbrowiecki, P. Ambient PM2.5 exposure and mortality due to lung cancer and cardiopulmonary diseases in Polish cities. In Respiratory Treatment and Prevention. Advances in Experimental Medicine and Biology; Pokorski, M., Ed.; Springer: Cham, Switzerland, 2016; Volume 944, pp. 9–17. [Google Scholar]
- US EPA. Integrated Risk Information System, Methylmercury Oral Reference Dose; Environmental Protection Agency: Washington, DC, USA, 2003. Available online: http://www.epa.gov/iris/subst/0073.html (accessed on 21 August 2021).
- Daniels, M.J.; Dominici, F.; Samet, J.M.; Zeger, S.L. Estimating particulate matter-mortality dose-response curves and threshold levels: An analysis of daily time series for the 20 largest US cities. Am. J. Epidemiol. 2000, 152, 397–406. [Google Scholar] [CrossRef] [Green Version]
- Kelly, F.J.; Fussell, J.C. Air Pollution and public health: Emerging hazards and improved understanding of risk. Environ. Geochem. Health 2015, 37, 631–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, S.; Chirkov, V.; Dentener, F.; Dingenen, R.V.; Pachauri, S.; Purohit, P.; Amann, M.; Heyes, C.; Kinney, P.; Kolp, P.; et al. Estimation of the Global Health Impacts of Air Pollution; IASA: Laxenburg, Austria, 2011. [Google Scholar]
- Lelieveld, J.; Evans, J.S.; Giannadaki, D.; Pozzer, A. The contribution of outdoor air pollution sources to permanent mortality on global scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef]
- Singh, D.P.; Gadi, R.; Mandal, T.K.; Dixit, C.K.; Singh, K.; Saud, T.; Singh, N.; Gupta, P.K. Study of temporal variation in ambient air quality during Diwali festival in India. Environ. Mon. Assess. 2010, 169, 1–13. [Google Scholar] [CrossRef]
- Khanum, F.; Chaudhry, M.N.; Kumar, P. Characterization of five-year observation data of fine particulate matter in the metropolitan area of Lahore. Air Qual. Atmos. Health 2017, 10, 725–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackney, J.D.; Linn, W.S.; Avol, E.L. Acid Fog: Effects on respiratory function and symptoms in healthy and asthmatic volunteers. Environ. Health Pres. 1989, 79, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, P.; Zivin, J.G.; Mulins, J.T.; Neideli, M. Early-life exposure to the great smog of 1952 and the development of asthma. Am. J. Respir. Crit. Care Med. 2016, 194, 1475–1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenamani, R.K. Alarming rise in fog and pollution causing a fall in maximum temperature over Delhi. Cur. Sci. 2007, 93, 314–322. [Google Scholar]
- Shrestha, S.; Moore, G.A.; Peel, M.C. Trends in winter fog in Terai region of Nepal. Agric. For. Meteorol. 2018, 259, 118–130. [Google Scholar] [CrossRef]
- Hopke, P.K.; Cohen, D.D.; Begum, B.A.; Biswas, S.K.; Ni, B.; Pandit, G.G.; Santoso, M.; Chung, Y.; Davy, P.; Markwitz, A.; et al. Urban air quality in Asian region. Sci. Total Environ. 2008, 404, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Jin, X.; Zucker, N.; Kennedy, R.; Urpelainen, J. Transboundary air pollution from coal-fired power generation. J. Environ. Manag. 2020, 270, 110862. [Google Scholar] [CrossRef] [PubMed]
- WHO. Air Quality Guidelines Global Update 2005 Geneva; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Hameed, S.; Mirza, M.I.; Ghauri, B.M.; Siddiqui, Z.R.; Javed, R.; Khan, A.R.; Rattigan, O.V.; Qureshi, S.; Husain, L. On the widespread winter fog in Northeastern Pakistan and India. Geophy. Res. Lett. 2000, 27, 1891–1894. [Google Scholar] [CrossRef]
- Ahmad, N.; Hussain, K.; Ahmad, N.; Khaleeq-ur-Rahman, M.; Hussnainn, A. A study of concentration of Lahore (Pakistan) suspended particulates and their trace elemental loadings. World Appl. Sci. J. 2014, 32, 1952–1961. [Google Scholar]
- Bulbul, G.; Shahid, I.; Chishte, F.; Shahid, M.Z.; Hundal, R.A.; Zahra, F.; Shahzad, M.I. PM10 Sampling and AOD Trends during 2016 winter fog season in the Islamabad region. Aerosol Air Qual. Res. 2018, 18, 188–199. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.; Athar, M. Impact of transport and industrial emissions on the ambient air quality of Lahore city, Pakistan. Environ. Monit. Assess. 2010, 171, 353–363. [Google Scholar] [CrossRef]
- Parveen, R.; Ahmad, A. Public Behavior in reducing urban air pollution: An application of the theory of planed behavior in Lahore. Environ. Sci. Pol. Res. 2020, 27, 17815–17830. [Google Scholar] [CrossRef]
- Aziz, A.; Bajwa, I.U. Minimizing human health effects of urban air pollution through quantification and control of motor vehicular carbon monoxide (CO) in Lahore. Environ. Monit. Assess. 2007, 135, 459–464. [Google Scholar] [CrossRef]
- Colbeck, I.; Nasir, Z.A.; Ali, Z. The state of ambient air quality in Pakistan—A review. Environ. Sci. Pollut. Res. 2010, 17, 49–63. [Google Scholar] [CrossRef] [Green Version]
- Prabhu, V.; Shridhar, V.; Choudhary, A. Investigation of the source, morphology, and trace elements associated with atmospheric PM10 and human health risks due to inhalation of carcinogenic elements at Dehradun, an Indo-Himalayan City. SN Appl. Sci. 2019, 1, 429. [Google Scholar] [CrossRef] [Green Version]
- Greven, S.; Dominici, F.; Zeger, S. An approach to the estimation of chronic air pollution effects using spatio-temporal information. J. Am. Stat. Assoc. 2011, 106, 396–406. [Google Scholar] [CrossRef] [Green Version]
- Patankar, A.M.; Trivedi, P.L. Monetary burden of health impacts of air pollution in Mumbai, India: Implication for public health policy. Public Health 2011, 125, 157–164. [Google Scholar] [CrossRef]
- Romero-Lankao, P.; Qin, H.; Borbor-Cordova, M. Exploration of health risks related to air pollution and temperature in three Latin American cities. Soc. Sci. Med. 2013, 83, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Rehman, S.; Iqbal, R. Smog. Pak. J. Med. Res. 2016, 55, 98. [Google Scholar]
- Colbeck, I.; Nasir, Z.A.; Ahmad, S.; Ali, Z. Exposure to PM10, PM2.5, PM1 and carbon monoxide on roads in Lahore Pakistan. Aerosol Air Qual. Res. 2011, 11, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Sheikh, M.R.; Akter, T. An assessment of climatic change impacts on livelihood patterns: A case study at Bakergonj Upazila, Barisal. J. Health Environ. Res. 2017, 3, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Riaz, R.; Hamid, K. Existing smog in Lahore, Pakistan: An alarming health concern. Cureus 2018, 10, e2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czechowski, P.O.; Dąbrowiecki, P.; Oniszczuk-Jastrząbek, A.; Bielawska, B.; Czermański, E.; Owczarek, T.; Rogula-Kopiec, P.; Badyda, A. A preliminary attempt at the identification and financial estimation of negative health effects of urban and industrial air pollution based on the agglomeration of Gdańsk. Sustainability 2019, 12, 42. [Google Scholar] [CrossRef] [Green Version]
- Khokhar, M.F.; Mehdi, H.; Abbas, Z.; Javed, Z. Temporal assessment of NO2 pollution levels in urban centers of Pakistan by employing ground-based and satellite observations. Aerosol Air Qual. Res. 2016, 16, 1854–1867. [Google Scholar] [CrossRef]
- Stone, E.; Schauer, J.; Quraishi, T.A.; Mahmood, A. Chemical characterization and source apportionment of fine and coarse particulate matter in Lahore, Pakistan. Atmos. Environ. 2010, 44, 1062–1070. [Google Scholar] [CrossRef]
- Khan, M.M.; Zaman, K.; Irfan, D.; Awan, U.; Ali, G.; Kyophilavong, P.; Shahbaz, M.; Naseem, I. Triangular relationship among energy consumption, air pollution and water resources in Pakistan. J. Clean. Prod. 2016, 112, 1375–1385. [Google Scholar] [CrossRef]
- Nasir, Z.A.; Murtaza, F.; Colbeck, I. Role of poverty in fuel choice and exposure to indoor air pollution in Pakistan. J. Integ. Environ. Sci. 2015, 12, 107–117. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.U.; Rashid, A.; Yousaf, B.; Kamal, A. Health outcomes of road-traffic pollution among exposed roadside-workers in the Rawalpindi city Pakistan. Hum. Ecol. Risk Assess. 2017, 23, 1330–1339. [Google Scholar] [CrossRef]
- Durand, M.; Grattan, J. Extensive respiratory health effects of volcanogenic dry fog in 1783 inferred from European documentary sources. Environ. Geochem. Health 1999, 21, 371–376. [Google Scholar] [CrossRef]
- Neidell, M.J. Air pollution, health, and socio-economic status: The effect of outdoor air quality on childhood asthma. J. Health Econ. 2004, 23, 1209–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilal, M.; Mhawish, A.; Nichol, J.E.; Qiu, Z.; Nazeer, M.; Ali, M.A.; de Leeuw, G.; Levy, R.C.; Wang, Y.; Chen, Y.; et al. Air pollution scenario over Pakistan: Characterization and ranking of extremely polluted cities using long-term concentrations of aerosol and trace gases. Remote Sens. Environ. 2021, 264, 112617. [Google Scholar] [CrossRef]
- Miri, M.; Derakhshan, Z.; Allahabadi, A.; Ahmadi, E.; Conti, G.O.; Ferrante, M.; Aval, H.E. Mortality and morbidity due to exposure to outdoor air pollution in Mashhad metropolis, Iran. The AirQ model approach. Environ. Res. 2016, 151, 451–457. [Google Scholar] [CrossRef]
- Badyda, A.J.; Dabrowiecki, P.; Czechowski, P.O.; Majewski, G. Risk of bronchi obstruction among non-smokers-Review of environmental factors affecting bronchoconstriction. Res. Physiol. Neurobiol. 2015, 209, 39–46. [Google Scholar] [CrossRef]
- Maji, S.; Ahmed, S.; Siddiqui, W.A.; Ghosh, S. Short term effects of criteria air pollutants in daily mortality in Delhi, India. Atmos. Environ. 2017, 150, 210–219. [Google Scholar] [CrossRef]
- Silva, R.A.; Adelman, Z.; Fry, M.M.; West, J.J. The impact of individual anthropogenic emissions sectors on the global burden of human mortality due to ambient air pollution. Environ. Health Pres. 2016, 124, 1776–1784. [Google Scholar] [CrossRef] [Green Version]
- Asl, F.B.; Leili, M.; Vaziri, Y.; Arian, S.S.; Cristaldi, A.; Conti, G.O.; Ferrante, M. Health impacts quantification of ambient air pollutants using AirQ model approach in Hamadan, Iran. Environ. Res. 2018, 161, 114–121. [Google Scholar]
- Rovira, J.; Domingo, J.L.; Schuhmacher, M. Air Quality, health impacts and burden of disease due to air pollution (PM10, PM2.5, NO2 and O3): Application of AirQ+ model to the Camp de Tarragona County (Catalonia, Spain). Sci. Total Environ. 2020, 703, 135538. [Google Scholar] [CrossRef]
- Anjum, M.S.; Ali, S.M.; Subhani, M.A.; Anwar, M.N.; Nizami, A.S.; Ashraf, U.; Khokhar, M.F. An emerged challenge of air pollution and ever-increasing particulate matter in Pakistan; A critical review. J. Hazard. Mater. 2021, 402, 123943. [Google Scholar] [CrossRef] [PubMed]
- Badarinath, K.V.S.; Chand, T.K.; Prasad, V.K. Agriculture crop residue burning in the Indo-Gangetic Plains—A study using IRS-P6 AWiFS satellite data. Curr. Sci. 2006, 91, 1085–1089. [Google Scholar]
- Miao, Y.; Che, H.; Zhang, X.; Liu, S. Relationship between summertime concurring PM2.5 and O3 pollution and boundary layer height differs between Beijing and Shanghai, China. Environ. Pollut. 2021, 268, 115775. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, A.; Singh, R.P. Decline in PM2.5 concentrations over major cities around the world associated with COVID-19. Environ. Res. 2020, 187, 109634. [Google Scholar] [CrossRef]
- Halder, R. Stubble burning in Punjab and Haryana back to foul up Delhi air. Times of India, 16 May 2019. [Google Scholar]
Figure 1.
Map of Lahore and its adjoining areas with five sampling locations.

Table 1.
Summary of sample size and data collection tools.
| Indicators/Tools | Study Sites | ||||
|---|---|---|---|---|---|
| Nankana Sahib | Changa Manga | Kasur | Lahore | Sayed Wala | |
| Sample distribution across gender | |||||
| Total sample | 64 | 75 | 72 | 60 | 70 |
| Male | 55 | 62 | 58 | 49 | 45 |
| Female | 9 | 13 | 14 | 11 | 25 |
| Sample distribution across different professions | |||||
| Farmers | 14 | 10 | 20 | 10 | 9 |
| Household workers | 10 | 13 | 9 | 10 | 12 |
| Laborers | 12 | 13 | 16 | 10 | 10 |
| Shopkeepers | 12 | 19 | 11 | 10 | 9 |
| Office employees | 6 | 10 | 6 | 10 | 20 |
| Drivers | 10 | 10 | 10 | 10 | 10 |
| Focus group discussions (FGD) | |||||
| Number of FGDs | 2 | 1 | 2 | 1 | 1 |
| Number of participants | 35 | 30 | 25 | 6 | 16 |
| Key informants | 1 (people’s representative) | 2 (people’s representative and government official) | 1 (people’s representative) | 2 (people’s representative and doctor) | 2 (people’s representative and doctor) |
| Field observations (nonparticipants) | In all sites, observations were made to note field activities, nearest pollution sources, and safety measures. | ||||
Table 4.
Predictors of health symptoms among exposed groups.
| Variables | Multiple Symptoms * | Cough | Breathlessness | Eye Irritation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B ** | p-Value | Odds Ratio | B | p-Value | Odds Ratio | B | p-Value | Odds Ratio | B | p-Value | Odds Ratio | ||
| Constant | −1.40 | 0.103 | 0.24 | −1.34 | 0.110 | 0.26 | −3.1 | 0.004 | 0.04 | −0.63 | 0.410 | 0.53 | |
| Gender (reference: female) | Male | 0.13 | 0.760 | 1.14 | 0.13 | 0.780 | 1.14 | 0.43 | 0.430 | 1.54 | −0.24 | 0.590 | 0.78 |
| Occupation groups (reference: office employee) | Farmer | −0.46 | 0.380 | 0.62 | −0.50 | 0.350 | 0.60 | 0.14 | 0.810 | 1.16 | 0.68 | 0.180 | 1.98 |
| Household | 0.29 | 0.570 | 1.34 | 0.27 | 0.610 | 1.30 | 1.00 | 0.105 | 2.74 | 0.22 | 0.660 | 1.24 | |
| Labor | −0.31 | 0.560 | 0.72 | −0.33 | 0.540 | 0.71 | −0.04 | 0.940 | 0.95 | 0.84 | 0.110 | 2.32 | |
| Shopkeeper | −0.06 | 0.880 | 0.93 | −0.17 | 0.720 | 0.84 | 0.44 | 0.430 | 1.55 | 0.79 | 0.094 | 2.20 | |
| Driver | −0.38 | 0.480 | 0.68 | −0.40 | 0.450 | 0.66 | −0.64 | 0.340 | 0.52 | 0.86 | 0.107 | 2.37 | |
| Age (years) (reference: adolescents aged 16–20 years) | 21–44 | 0.52 | 0.400 | 1.69 | 0.52 | 0.410 | 1.67 | 0.66 | 0.420 | 1.93 | 0.99 | 0.079 | 2.70 |
| 45–64 | 1.74 | 0.010 | 5.73 | 1.75 | 0.010 | 5.77 | 0.85 | 0.330 | 2.34 | 1.04 | 0.097 | 2.85 | |
| 65 and above | 1.02 | 0.220 | 2.79 | 1.03 | 0.220 | 2.80 | 1.79 | 0.080 | 5.99 | 0.42 | 0.590 | 1.50 | |
| Literacy level (reference: illiterate) | Primary | 0.58 | 0.099 | 1.79 | 0.58 | 0.090 | 1.79 | −0.15 | 0.700 | 0.85 | 0.52 | 0.140 | 1.69 |
| High School | −0.18 | 0.580 | 0.83 | −0.18 | 0.580 | 0.83 | 0.26 | 0.470 | 1.30 | 0.2 | 0.530 | 1.22 | |
| Higher | 0.06 | 0.870 | 1.06 | 0.008 | 0.980 | 1.00 | −0.23 | 0.610 | 0.79 | 0.14 | 0.710 | 1.15 | |
| Smoking habit | −0.12 | 0.670 | 0.88 | −0.087 | 0.760 | 0.91 | 0.28 | 0.390 | 1.32 | −0.4 | 0.150 | 0.66 | |
| History of respiratory diseases (yes = 1; no = 0) | 1.40 | 0.000 | 4.06 | 1.31 | 0.000 | 3.70 | 1.82 | 0.000 | 6.20 | −0.24 | 0.390 | 0.78 | |
| Location (Lahore = 1; otherwise = 0) | 0.81 | 0.010 | 2.26 | 0.75 | 0.020 | 2.12 | 0.32 | 0.370 | 1.37 | −1.11 | 0.000 | 0.32 | |
| Coping measures (yes = 1; no = 0) | 0.08 | 0.730 | 1.09 | 0.12 | 0.650 | 1.12 | 0.42 | 0.160 | 1.52 | 0.18 | 0.640 | 1.20 | |
* Multiple symptoms included cough, phlegm, and Wheezing; ** B = beta coefficient.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Jabeen, F.; Ali, Z.; Maharjan, A. Assessing Health Impacts of Winter Smog in Lahore for Exposed Occupational Groups. Atmosphere 2021, 12, 1532. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos12111532
AMA Style
Jabeen F, Ali Z, Maharjan A. Assessing Health Impacts of Winter Smog in Lahore for Exposed Occupational Groups. Atmosphere. 2021; 12(11):1532. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos12111532
Chicago/Turabian StyleJabeen, Fatima, Zulfiqar Ali, and Amina Maharjan. 2021. "Assessing Health Impacts of Winter Smog in Lahore for Exposed Occupational Groups" Atmosphere 12, no. 11: 1532. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos12111532
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.