
Association between Ambient Air Pollutants and Pneumonia in Wuhan, China, 2014–2017


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Outpatient Visits for Pneumonia Cases
2.3. Air Pollution and Meteorological Data
2.4. Statistical Analysis
2.5. Statistical Software
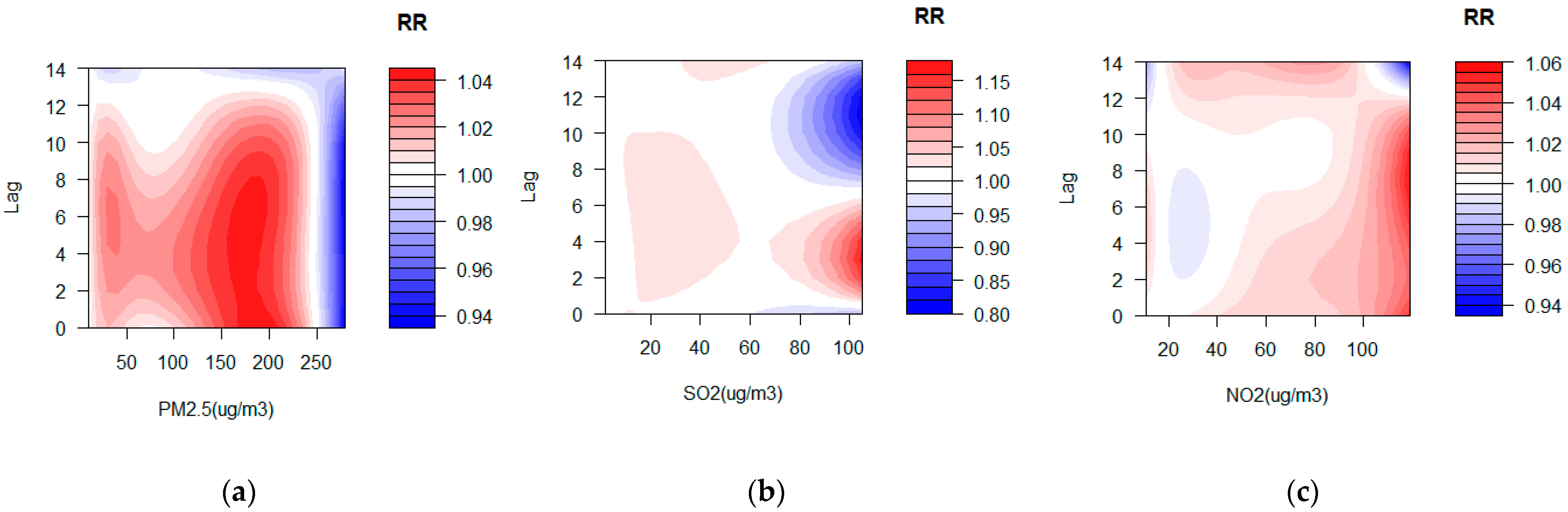
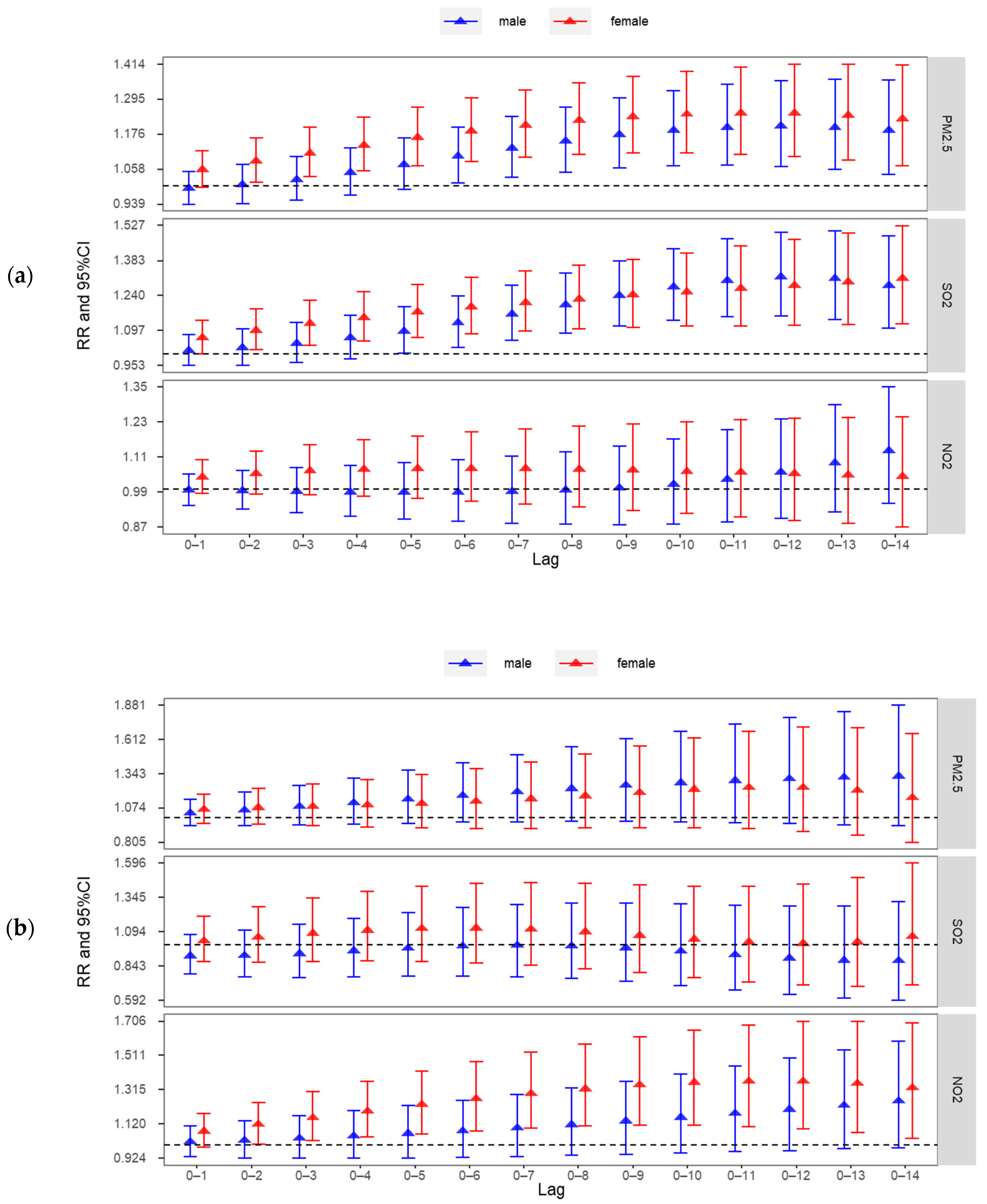
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
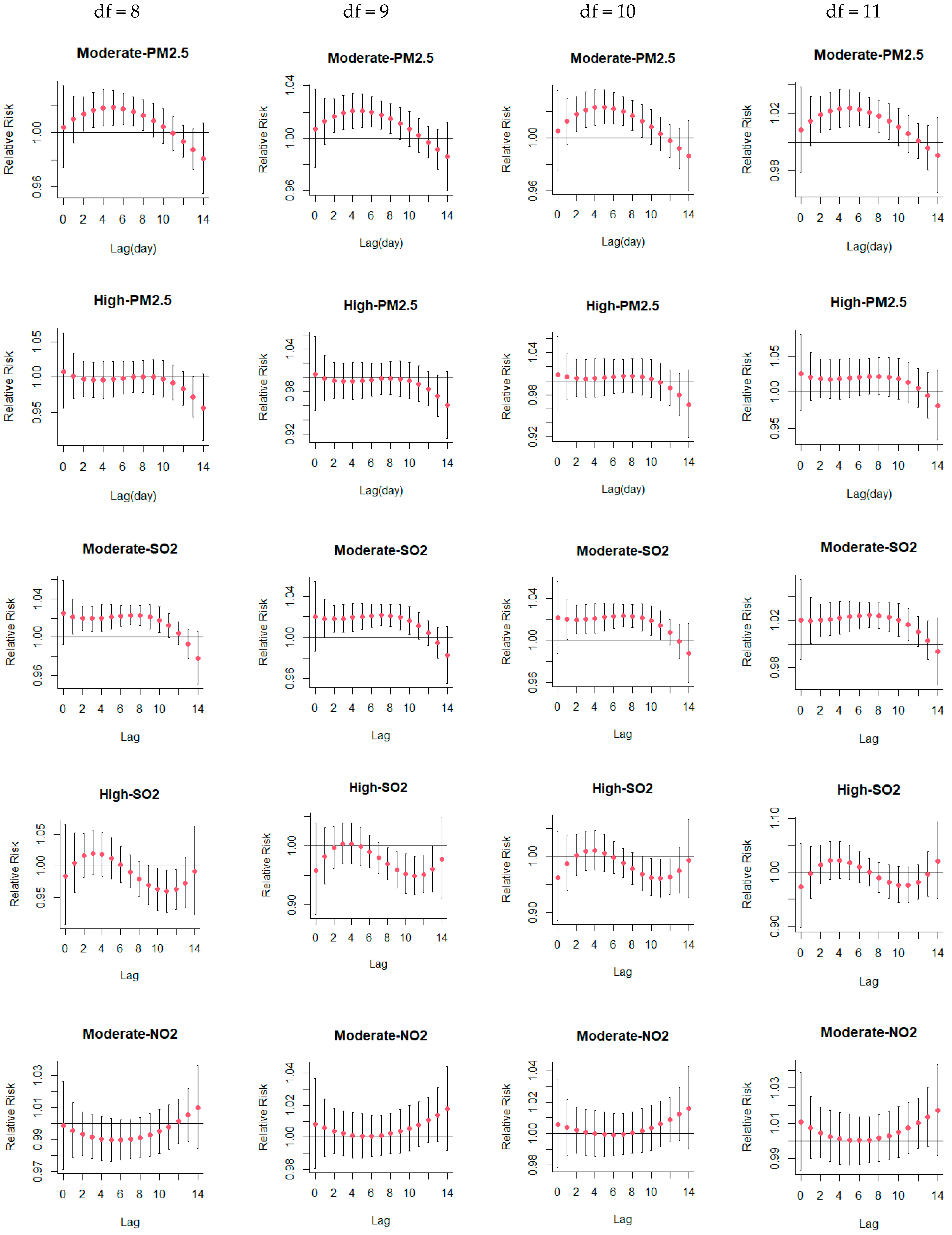
Appendix A. Sensitivity Analysis


References
- Torres, A.; Cilloniz, C.; Niederman, M.S.; Menendez, R.; Chalmers, J.D.; Wunderink, R.G.; van der Poll, T. Pneumonia. Nat. Rev. Dis. Primers 2021, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Quinton, L.J.; Walkey, A.J.; Mizgerd, J.P. Integrative Physiology of Pneumonia. Physiol. Rev. 2018, 98, 1417–1464. [Google Scholar] [CrossRef] [PubMed]
- Lanks, C.W.; Musani, A.I.; Hsia, D.W. Community-acquired Pneumonia and Hospital-acquired Pneumonia. Med. Clin. N. Am. 2019, 103, 487–501. [Google Scholar] [CrossRef] [PubMed]
- Corrales-Medina, V.F.; Musher, D.M.; Shachkina, S.; Chirinos, J.A. Acute pneumonia and the cardiovascular system. Lancet 2013, 381, 496–505. [Google Scholar] [CrossRef]
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 394, 1145–1158. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.J.; Ross Anderson, H.; Ostro, B.; Pandey, K.D.; Krzyzanowski, M.; Kunzli, N.; Gutschmidt, K.; Pope, A.; Romieu, I.; Samet, J.M.; et al. The global burden of disease due to outdoor air pollution. J. Toxicol. Environ. Health A 2005, 68, 1301–1307. [Google Scholar] [CrossRef]
- Zhuang, J.; Bai, H.; Sun, J.; Zhang, T.; Li, J.; Chen, Y.; Zhang, H.; Sun, Q. The association between fine particulate matter and acute lower respiratory infections in Yancheng City, China. Environ. Sci. Pollut. Res. Int. 2021, 28, 61723–61731. [Google Scholar] [CrossRef]
- Slama, A.; Sliwczynski, A.; Woznica, J.; Zdrolik, M.; Wisnicki, B.; Kubajek, J.; Turzanska-Wieczorek, O.; Gozdowski, D.; Wierzba, W.; Franek, E. Impact of air pollution on hospital admissions with a focus on respiratory diseases: A time-series multi-city analysis. Environ. Sci. Pollut. Res. Int. 2019, 26, 16998–17009. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Li, Y.; Niu, A.; Liu, Y.; Su, L.; Song, W.; Liu, J.; Liu, Y.; Li, H. The impact of outdoor air pollutants on outpatient visits for respiratory diseases during 2012–2016 in Jinan, China. Respir. Res. 2018, 19, 246. [Google Scholar] [CrossRef]
- Cai, Y.; Shao, Y.; Wang, C. The association of air pollution with the patients’ visits to the department of respiratory diseases. J. Clin. Med. Res. 2015, 7, 551–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanos, J.K.; Cakmak, S.; Kalkstein, L.S.; Yagouti, A. Association of weather and air pollution interactions on daily mortality in 12 Canadian cities. Air Qual. Atmos. Health 2015, 8, 307–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.; Hu, P.; Chen, R.; Liu, B.; Chen, H.; Hou, J.; Ke, L.; Huang, J.; Ren, H.; Hu, H. Association of long-term exposure to ambient air pollution with the number of tuberculosis cases notified: A time-series study in Hong Kong. Environ. Sci. Pollut. Res. Int. 2022, 29, 21621–21633. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Wang, J.B.; Zhang, Z.Y.; Shen, P.; Zheng, P.W.; Jin, M.J.; Lu, H.C.; Lin, H.B.; Chen, K. Effects of air pollution on hospital visits for pneumonia in children: A two-year analysis from China. Environ. Sci. Pollut. Res. Int. 2018, 25, 10049–10057. [Google Scholar] [CrossRef]
- Neupane, B.; Jerrett, M.; Burnett, R.T.; Marrie, T.; Arain, A.; Loeb, M. Long-term exposure to ambient air pollution and risk of hospitalization with community-acquired pneumonia in older adults. Am. J. Respir. Crit. Care Med. 2010, 181, 47–53. [Google Scholar] [CrossRef]
- Yee, J.; Cho, Y.A.; Yoo, H.J.; Yun, H.; Gwak, H.S. Short-term exposure to air pollution and hospital admission for pneumonia: A systematic review and meta-analysis. Environ. Health 2021, 20, 6. [Google Scholar] [CrossRef]
- Pirozzi, C.S.; Jones, B.E.; VanDerslice, J.A.; Zhang, Y.; Paine, R., 3rd; Dean, N.C. Short-Term Air Pollution and Incident Pneumonia. A Case-Crossover Study. Ann. Am. Thorac. Soc. 2018, 15, 449–459. [Google Scholar] [CrossRef]
- Wu, J.; Wu, Y.; Tian, Y.; Wu, Y.; Wang, M.; Wang, X.; Wang, Z.; Hu, Y. Association between ambient fine particulate matter and adult hospital admissions for pneumonia in Beijing, China. Atmos. Environ. 2020, 231, 117497. [Google Scholar] [CrossRef]
- Cheng, C.Y.; Cheng, S.Y.; Chen, C.C.; Pan, H.Y.; Wu, K.H.; Cheng, F.J. Ambient air pollution is associated with pediatric pneumonia: A time-stratified case-crossover study in an urban area. Environ. Health 2019, 18, 77. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [Green Version]
- Self, W.H.; Williams, D.J.; Zhu, Y.; Ampofo, K.; Pavia, A.T.; Chappell, J.D.; Hymas, W.C.; Stockmann, C.; Bramley, A.M.; Schneider, E.; et al. Respiratory Viral Detection in Children and Adults: Comparing Asymptomatic Controls and Patients With Community-Acquired Pneumonia. J. Infect. Dis. 2016, 213, 584–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Yang, J.; Liu, M.; Sun, X.; Li, T.; Guo, Y.; Hu, K.; Bell, M.L.; Cheng, Q.; Kan, H.; et al. Nonlinear effect of air pollution on adult pneumonia hospital visits in the coastal city of Qingdao, China: A time-series analysis. Environ. Res. 2022, 209, 112754. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.T.; Zhang, H.; Xue, F.Z.; Zhao, L.; Cao, W.C. Associations of air pollutants with pneumonia hospital admissions in Qingdao, China: A prospective cohort study. Environ. Sci. Pollut. Res. Int. 2022, 34981381. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhang, Y.; Zhang, W.; Li, S.; Williams, G.; Marks, G.B.; Jalaludin, B.; Abramson, M.J.; Luo, F.; Yang, D.; et al. Attributable risks of emergency hospital visits due to air pollutants in China: A multi-city study. Environ. Pollut. 2017, 228, 43–49. [Google Scholar] [CrossRef]
- Wang, K.Y.; Chau, T.T. An association between air pollution and daily outpatient visits for respiratory disease in a heavy industry area. PLoS ONE 2013, 8, e75220. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Yan, C.; Li, M.; Zhao, L.; Long, Z.; Fan, Y.; Zhang, Z.; Chen, R.; Huang, Y.; Lu, C.; et al. Short term effects of air pollutants on hospital admissions for respiratory diseases among children: A multi-city time-series study in China. Int. J. Hyg. Environ. Health 2021, 231, 113638. [Google Scholar] [CrossRef]
- Chen, R.; Yin, P.; Meng, X.; Liu, C.; Wang, L.; Xu, X.; Ross, J.A.; Tse, L.A.; Zhao, Z.; Kan, H.; et al. Fine Particulate Air Pollution and Daily Mortality. A Nationwide Analysis in 272 Chinese Cities. Am. J. Respir. Crit. Care Med. 2017, 196, 73–81. [Google Scholar] [CrossRef]
- Tian, Y.; Liu, H.; Wu, Y.; Si, Y.; Li, M.; Wu, Y.; Wang, X.; Wang, M.; Chen, L.; Wei, C.; et al. Ambient particulate matter pollution and adult hospital admissions for pneumonia in urban China: A national time series analysis for 2014 through 2017. PLoS Med. 2019, 16, e1003010. [Google Scholar] [CrossRef] [Green Version]
- Chai, G.; He, H.; Sha, Y.; Zhai, G.; Zong, S. Effect of PM2.5 on daily outpatient visits for respiratory diseases in Lanzhou, China. Sci. Total Environ. 2019, 649, 1563–1572. [Google Scholar] [CrossRef]
- Zhang, F.; Zhang, H.; Wu, C.; Zhang, M.; Feng, H.; Li, D.; Zhu, W. Acute effects of ambient air pollution on clinic visits of college students for upper respiratory tract infection in Wuhan, China. Environ. Sci. Pollut. Res. Int. 2021, 28, 29820–29830. [Google Scholar] [CrossRef]
- Yan, Y.; She, L.; Guo, Y.; Zhao, Y.; Zhang, P.; Xiang, B.; Zeng, J.; Yang, M.; Wang, L. Association between ambient air pollution and mortality from chronic obstructive pulmonary disease in Wuhan, China: A population-based time-series study. Environ. Sci. Pollut. Res. Int. 2021, 28, 33698–33706. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wang, J.; Lu, W. Exposure to nitrogen dioxide and chronic obstructive pulmonary disease (COPD) in adults: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. Int. 2018, 25, 15133–15145. [Google Scholar] [CrossRef] [PubMed]
- Frampton, M.W.; Boscia, J.; Roberts, N.J., Jr.; Azadniv, M.; Torres, A.; Cox, C.; Morrow, P.E.; Nichols, J.; Chalupa, D.; Frasier, L.M. Nitrogen dioxide exposure: Effects on airway and blood cells. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2002, 282, L155–L165. [Google Scholar] [CrossRef] [PubMed]
- Pathmanathan, S.; Krishna, M.T.; Blomberg, A.; Helleday, R.; Kelly, F.J.; Sandström, T.; Holgate, S.T.; Wilson, S.J.; Frew, A.J. Repeated daily exposure to 2 ppm nitrogen dioxide upregulates the expression of IL-5, IL-10, IL-13, and ICAM-1 in the bronchial epithelium of healthy human airways. Occup. Environ. Med. 2003, 60, 892. [Google Scholar] [CrossRef] [Green Version]
- Bai, K.J.; Chuang, K.J.; Chen, J.K.; Tsai, C.Y.; Yang, Y.L.; Chang, C.C.; Chen, T.T.; Lee, C.N.; Feng, P.H.; Chen, K.Y.; et al. Alterations by Air Pollution in Inflammation and Metals in Pleural Effusion of Pneumonia Patients. Int. J. Environ. Res. Public Health 2019, 16, 705. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Hong, Y.; Liu, N. Association of ambient Particulate matter 2.5 with intensive care unit admission due to pneumonia: A distributed lag non-linear model. Sci. Rep. 2017, 7, 8679. [Google Scholar] [CrossRef] [Green Version]
- Lv, C.; Wang, X.; Pang, N.; Wang, L.; Wang, Y.; Xu, T.; Zhang, Y.; Zhou, T.; Li, W. The impact of airborne particulate matter on pediatric hospital admissions for pneumonia among children in Jinan, China: A case-crossover study. J. Air Waste Manag. Assoc. 2017, 67, 669–676. [Google Scholar] [CrossRef]
- Zhang, J.; Ren, D.; Cao, X.; Wang, T.; Geng, X.; Li, X.; Tang, J.; Leng, S.; Wang, H.; Zheng, Y. Ambient air pollutants and hospital visits for pneumonia: A case-crossover study in Qingdao, China. BMC Public Health 2021, 21, 66. [Google Scholar] [CrossRef]
- Tao, Y.; Mi, S.; Zhou, S.; Wang, S.; Xie, X. Air pollution and hospital admissions for respiratory diseases in Lanzhou, China. Environ. Pollut. 2014, 185, 196–201. [Google Scholar] [CrossRef]
- Faustini, A.; Stafoggia, M.; Colais, P.; Berti, G.; Bisanti, L.; Cadum, E.; Cernigliaro, A.; Mallone, S.; Scarnato, C.; Forastiere, F.; et al. Air pollution and multiple acute respiratory outcomes. Eur. Respir. J. 2013, 42, 304–313. [Google Scholar] [CrossRef] [Green Version]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Zheng, P.W.; Wang, J.B.; Zhang, Z.Y.; Shen, P.; Chai, P.F.; Li, D.; Jin, M.J.; Tang, M.L.; Lu, H.C.; Lin, H.B.; et al. Air pollution and hospital visits for acute upper and lower respiratory infections among children in Ningbo, China: A time-series analysis. Environ. Sci. Pollut. Res. Int. 2017, 24, 18860–18869. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Li, X.; Wang, S.; Wang, C.; Huang, F.; Gao, Q.; Wu, L.; Tao, L.; Guo, J.; Wang, W.; et al. Fine Particulate Air Pollution and Hospital Emergency Room Visits for Respiratory Disease in Urban Areas in Beijing, China, in 2013. PLoS ONE 2016, 11, e0153099. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Wang, X.; Fan, J.; Xiao, W.; Wang, Y. Effects of Air Pollution on Hospital Emergency Room Visits for Respiratory Diseases: Urban-Suburban Differences in Eastern China. Int. J. Environ. Res. Public Health 2016, 13, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, H.; Tian, L.W.; Pun, V.C.; Ho, K.F.; Wong, T.W.; Yu, I.T. Coarse particulate matter associated with increased risk of emergency hospital admissions for pneumonia in Hong Kong. Thorax 2014, 69, 1027–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barsky, A.J.; Peekna, H.M.; Borus, J.F. Somatic Symptom Reporting in Women and Men. J. Gen. Intern. Med. 2001, 16, 266–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunzli, N.; Jerrett, M.; Mack, W.J.; Beckerman, B.; LaBree, L.; Gilliland, F.; Thomas, D.; Peters, J.; Hodis, H.N. Ambient air pollution and atherosclerosis in Los Angeles. Environ. Health Perspect. 2005, 113, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Samoli, E.; Aga, E.; Touloumi, G.; Nisiotis, K.; Forsberg, B.; Lefranc, A.; Pekkanen, J.; Wojtyniak, B.; Schindler, C.; Niciu, E.; et al. Short-term effects of nitrogen dioxide on mortality: An analysis within the APHEA project. Eur. Respir. J. 2006, 27, 1129–1138. [Google Scholar] [CrossRef]
- Lv, J.; Chen, W.; Sun, D.; Li, S.; Millwood, I.Y.; Smith, M.; Guo, Y.; Bian, Z.; Yu, C.; Zhou, H.; et al. Gender-specific association between tobacco smoking and central obesity among 0.5 million Chinese people: The China Kadoorie Biobank Study. PLoS ONE 2015, 10, e0124586. [Google Scholar] [CrossRef]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, Sex, Age, and Education as Modifiers of the Effects of Outdoor Air Pollution on Daily Mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef]
- Moshammer, H.; Hutter, H.P.; Hauck, H.; Neuberger, M. Low levels of air pollution induce changes of lung function in a panel of schoolchildren. Eur. Respir. J. 2006, 27, 1138–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Yu, S.; Yan, R.; Zhang, Q.; Li, P.; Wang, L.; Liu, W.; Zheng, X. Characteristics and origins of air pollutants in Wuhan, China, based on observations and hybrid receptor models. J. Air Waste Manag. Assoc. 2017, 67, 739–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Qaness, M.A.A.; Fan, H.; Ewees, A.A.; Yousri, D.; Abd Elaziz, M. Improved ANFIS model for forecasting Wuhan City Air Quality and analysis COVID-19 lockdown impacts on air quality. Environ. Res. 2021, 194, 110607. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, N.L.; Woodhouse, S.; Stieb, D.M.; Brook, J.R. Ambient nitrogen dioxide and distance from a major highway. Sci. Total Environ. 2003, 312, 43–46. [Google Scholar] [CrossRef]
- Simonetti, A.F.; Viasus, D.; Garcia-Vidal, C.; Carratala, J. Management of community-acquired pneumonia in older adults. Ther. Adv. Infect. Dis. 2014, 2, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Ren, M.; Li, N.; Wang, Z.; Liu, Y.; Chen, X.; Chu, Y.; Li, X.; Zhu, Z.; Tian, L.; Xiang, H. The short-term effects of air pollutants on respiratory disease mortality in Wuhan, China: Comparison of time-series and case-crossover analyses. Sci. Rep. 2017, 7, 40482. [Google Scholar] [CrossRef]
- Faverio, P.; Aliberti, S.; Bellelli, G.; Suigo, G.; Lonni, S.; Pesci, A.; Restrepo, M.I. The management of community-acquired pneumonia in the elderly. Eur. J. Intern. Med. 2014, 25, 312–319. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | Mean ± SD | Centiles | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Min | P1 | P25 | P50 | P75 | P99 | Max | |||
| Outpatient visits for pneumonia cases | |||||||||
| All | 133,882 (100%) | 92.00 ± 47.00 | 23.00 | 31.00 | 58.00 | 77.00 | 119.00 | 236.00 | 419.00 |
| Age 0–14 Years | 77,247 (57.70%) | 53.00 ± 32.00 | 4.00 | 10.00 | 29.00 | 40.00 | 61.00 | 142.00 | 247.00 |
| Age 15–64 Years | 33,601 (25.10%) | 23.00 ± 11.00 | 4.00 | 7.00 | 16.00 | 38.00 | 56.00 | 60.00 | 106.00 |
| Age >64 Years | 23,034 (17.20%) | 16.00 ± 10.00 | 1.00 | 3.00 | 10.00 | 44.00 | 70.00 | 48.00 | 113.00 |
| Male | 69,345 (51.80%) | 47.00 ± 25.00 | 10.00 | 14.00 | 30.00 | 21.00 | 27.00 | 123.00 | 238.00 |
| Female | 64,537 (48.20%) | 44.00 ± 23.00 | 9.00 | 13.00 | 28.00 | 14.00 | 19.00 | 112.00 | 214.00 |
| Ambient Pollutants | |||||||||
| PM2.5 (μg/m3) | 1461 | 63.87 ± 43.03 | 5.00 | 9.00 | 33.00 | 54.00 | 82.00 | 229.40 | 287.00 |
| NO2 (μg/m3) | 1461 | 47.50 ± 20.02 | 11.00 | 17.00 | 32.00 | 44.00 | 60.00 | 102.40 | 119.00 |
| SO2 (μg/m3) | 1461 | 17.66 ± 13.84 | 2.00 | 3.00 | 8.00 | 14.00 | 23.00 | 69.00 | 105.00 |
| Meteorological Factors | |||||||||
| Temperature (°C) | 1461 | 17.24 ± 8.83 | −4.32 | 0.41 | 9.55 | 18.33 | 24.79 | 32.50 | 33.98 |
| Relative Humidity (%) | 1461 | 78.81 ± 11.03 | 40.67 | 49.28 | 71.50 | 79.33 | 87.04 | 98.53 | 100.00 |
| Precipitation (mm/h) | 1461 | 0.16 ± 0.55 | 0.00 | 0.00 | 0.00 | 0.00 | 0.05 | 2.25 | 8.00 |
| Wind Velocity (m/s) | 1461 | 1.64 ± 0.89 | 0.30 | 0.43 | 1.00 | 1.43 | 2.10 | 4.42 | 6.52 |
| Lag | Moderate Level (P50) | High Level (P99) | ||||
|---|---|---|---|---|---|---|
| PM2.5 | SO2 | NO2 | PM2.5 | SO2 | NO2 | |
| Single-day lag effects | ||||||
| 0 | 1.006 (0.977–1.036) | 1.020 (0.987–1.054) | 1.011 (0.984–1.039) | 1.026 (0.974–1.081) | 0.972 (0.897–1.053) | 1.023 (0.980–1.068) |
| 1 | 1.013 (0.996–1.030) | 1.020 (1.001–1.039) | 1.007 (0.990–1.025) | 1.021 (0.988–1.055) | 0.997 (0.951–1.046) | 1.023 (0.996–1.050) |
| 2 | 1.018 (1.006–1.031) | 1.020 (1.007–1.033) | 1.005 (0.990–1.019) | 1.019 (0.992–1.046) | 1.013 (0.978–1.050) | 1.022 (1.001–1.044) |
| 3 | 1.021 (1.008–1.034) | 1.021 (1.007–1.034) | 1.003 (0.988–1.017) | 1.018 (0.991–1.045) | 1.021 (0.987–1.056) | 1.022 (1.001–1.043) |
| 4 | 1.022 (1.009–1.036) | 1.022 (1.008–1.036) | 1.001 (0.987–1.016) | 1.018 (0.991–1.046) | 1.021 (0.987–1.057) | 1.022 (1.001–1.043) |
| 5 | 1.022 (1.010–1.035) | 1.023 (1.010–1.036) | 1.000 (0.986–1.015) | 1.019 (0.993–1.047) | 1.017 (0.985–1.050) | 1.021 (1.002–1.042) |
| 6 | 1.021 (1.010–1.032) | 1.024 (1.013–1.035) | 1.000 (0.987–1.014) | 1.021 (0.995–1.046) | 1.009 (0.981–1.037) | 1.021 (1.003–1.039) |
| 7 | 1.019 (1.008–1.029) | 1.024 (1.014–1.034) | 1.001 (0.988–1.014) | 1.022 (0.997–1.047) | 0.999 (0.973–1.026) | 1.020 (1.002–1.038) |
| 8 | 1.016 (1.005–1.026) | 1.024 (1.013–1.035) | 1.001 (0.988–1.015) | 1.022 (0.997–1.048) | 0.989 (0.962–1.017) | 1.019 (1.000–1.038) |
| 9 | 1.012 (1.000–1.024) | 1.022 (1.010–1.035) | 1.003 (0.989–1.017) | 1.021 (0.994–1.048) | 0.981 (0.950–1.013) | 1.017 (0.997–1.038) |
| 10 | 1.008 (0.995–1.021) | 1.020 (1.006–1.034) | 1.005 (0.990–1.019) | 1.018 (0.990–1.047) | 0.976 (0.943–1.010) | 1.015 (0.994–1.037) |
| 11 | 1.004 (0.991–1.016) | 1.016 (1.003–1.029) | 1.007 (0.993–1.022) | 1.013 (0.986–1.041) | 0.975 (0.943–1.009) | 1.013 (0.992–1.034) |
| 12 | 1.000 (0.988–1.012) | 1.010 (0.998–1.023) | 1.010 (0.996–1.024) | 1.006 (0.979–1.033) | 0.981 (0.950–1.014) | 1.010 (0.989–1.030) |
| 13 | 0.996 (0.981–1.011) | 1.003 (0.987–1.019) | 1.013 (0.997–1.030) | 0.995 (0.964–1.027) | 0.995 (0.955–1.037) | 1.006 (0.981–1.031) |
| 14 | 0.992 (0.967–1.018) | 0.993 (0.966–1.022) | 1.017 (0.992–1.043) | 0.981 (0.934–1.031) | 1.019 (0.951–1.093) | 1.001 (0.962–1.042) |
| Cumulative lag effect | ||||||
| 0–1 | 1.020 (0.975–1.067) | 1.040 (0.989–1.094) | 1.018 (0.975–1.064) | 1.048 (0.965–1.138) | 0.969 (0.855–1.099) | 1.046 (0.977–1.119) |
| 0–2 | 1.038 (0.985–1.095) | 1.060 (0.999–1.125) | 1.023 (0.969–1.080) | 1.067 (0.964–1.181) | 0.982 (0.845–1.142) | 1.069 (0.984–1.162) |
| 0–3 | 1.060 (1.001–1.123) | 1.082 (1.015–1.154) | 1.026 (0.964–1.092) | 1.086 (0.967–1.220) | 1.003 (0.849–1.184) | 1.093 (0.995–1.200) |
| 0–4 | 1.084 (1.019–1.152) | 1.106 (1.034–1.183) | 1.027 (0.957–1.102) | 1.106 (0.970–1.260) | 1.024 (0.857–1.225) | 1.116 (1.007–1.238) |
| 0–5 | 1.108 (1.038–1.182) | 1.131 (1.054–1.215) | 1.027 (0.950–1.111) | 1.127 (0.974–1.304) | 1.041 (0.861–1.260) | 1.140 (1.019–1.277) |
| 0–6 | 1.131 (1.056–1.212) | 1.158 (1.074–1.248) | 1.028 (0.943–1.120) | 1.150 (0.979–1.351) | 1.051 (0.859–1.285) | 1.164 (1.031–1.315) |
| 0–7 | 1.152 (1.072–1.239) | 1.186 (1.096–1.283) | 1.028 (0.936–1.129) | 1.175 (0.986–1.401) | 1.050 (0.850–1.297) | 1.187 (1.042–1.352) |
| 0–8 | 1.170 (1.085–1.263) | 1.214 (1.118–1.318) | 1.030 (0.931–1.139) | 1.201 (0.992–1.453) | 1.039 (0.832–1.296) | 1.210 (1.054–1.389) |
| 0–9 | 1.184 (1.093–1.283) | 1.241 (1.138–1.354) | 1.033 (0.927–1.151) | 1.226 (0.997–1.507) | 1.019 (0.807–1.286) | 1.231 (1.063–1.425) |
| 0–10 | 1.193 (1.096–1.299) | 1.266 (1.154–1.389) | 1.038 (0.925–1.165) | 1.248 (1.000–1.559) | 0.994 (0.776–1.273) | 1.249 (1.069–1.460) |
| 0–11 | 1.198 (1.094–1.311) | 1.286 (1.165–1.421) | 1.045 (0.925–1.182) | 1.265 (0.997–1.605) | 0.970 (0.744–1.264) | 1.265 (1.072–1.493) |
| 0–12 | 1.197 (1.088–1.317) | 1.300 (1.169–1.445) | 1.056 (0.928–1.202) | 1.272 (0.987–1.639) | 0.951 (0.718–1.262) | 1.277 (1.072–1.522) |
| 0–13 | 1.192 (1.078–1.318) | 1.304 (1.166–1.458) | 1.070 (0.935–1.225) | 1.266 (0.969–1.654) | 0.947 (0.702–1.276) | 1.285 (1.070–1.543) |
| 0–14 | 1.183 (1.063–1.316) | 1.295 (1.150–1.459) | 1.088 (0.945–1.254) | 1.242 (0.937–1.647) | 0.965 (0.701–1.329) | 1.286 (1.060–1.561) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Liu, S.; Dou, Q.; Huang, Z.; Lv, C.; Liao, J.; Tao, F.; Liu, Y.; Ma, L. Association between Ambient Air Pollutants and Pneumonia in Wuhan, China, 2014–2017. Atmosphere 2022, 13, 578. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos13040578
Zhang H, Liu S, Dou Q, Huang Z, Lv C, Liao J, Tao F, Liu Y, Ma L. Association between Ambient Air Pollutants and Pneumonia in Wuhan, China, 2014–2017. Atmosphere. 2022; 13(4):578. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos13040578
Chicago/Turabian StyleZhang, Huihui, Suyang Liu, Qiujun Dou, Zenghui Huang, Chengcheng Lv, Jingling Liao, Fengxi Tao, Yuehua Liu, and Lu Ma. 2022. "Association between Ambient Air Pollutants and Pneumonia in Wuhan, China, 2014–2017" Atmosphere 13, no. 4: 578. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos13040578