1. Introduction
The health system is supposed to function properly in four determined aspects to accomplish three fundamental objectives of health promotion, having reasonable financial contribution and responsiveness. In addition, concerning the growing challenges of health systems such as resources limitation and increased demand, neglecting variable circumstance and requirements would have detrimental consequences and lead to damaging failures (Coiera and Hovenga, 2007) [
1]. These functions are stewardship, resource generation, financing, and services provision (WHO report, 2000) [
2]. Financing is considered one of the most essential functions of health systems.
Health system financing is the procedure by which revenues are collected from primary and secondary sources, which are accumulated in fund pools and allocated to specific activities of providers (1). Consumers, the government, social insurance, and private health insurance payments constitute four main sources of out-of-pocket payments in health system financing (Markel, 2014) [
3]. In this respect, the objectives of the financing function of the health system are adequate funding, equitable financial access to quality health services, protection from financial costs, and efficiency in resource mobilization allocation and usage. To obtain these objectives, three main functions are identified, including purchasing services, pooling funds, and collecting funds (WHO report, 2000) [
2]. The health-financing system is a highly contextual subject that needs to be addressed exclusively in each country (Moon, 2014; Wang et al., 2016) [
4,
5].
Considering other areas of science in which the MADM-based scenario approach has been demonstrated, the MADM-based scenario approach was implemented to select bicycle chain materials for strategic success in an Indian manufacturing scenario (Singh & Kumar, 2012) [
6]. An MADM-based scenario was applied to select the material alternatives in bicycle manufacturing. Another example of using MADM-based scenario notion takes advantage of implementing the high average of subscribers’ service quality, namely the Quality of Service (QoS), where different radio access technologies are implemented using different handover criteria to link the continuity of the service (Zineb, Ayadi, & Tabbane, 2017) [
7]. Consequently, the MADM-based scenario approach is worked out in different fields and found to be reliable for prioritizing alternatives.
Increasing demand for health services and the increasing costs of health services supplies comprised two main sources for expenditure growth in the health sector that affect drivers and dynamics. The growing burden of disease has been asserted as one of the causes of increasing the demand for health services that stems from the aging population and unhealthy lifestyles. Advanced technologies and innovative strategy have led to rising unit cost of care. Additionally, vested interests and incentive systems have led to a suboptimal allocation of resources (2). Unit cost increment and substandard resource allocation are both sources of expanding the expenditure growth for supplying health services. These specified drivers could potentially be the unsustainability factors in health system financing (Industry agenda, 2012; Ooms et al., 2014) [
8,
9].
There are vital indicators in health financing monitoring and analyzing listed in
Table 1 whose future status can be determined in different scenarios of health financing (WHO report, 2004) [
10]:
The World Business Council for Sustainable Development (WBCSD) acknowledged that the method of managing health systems is unsustainable i.e., the costs that need to be afforded are higher, and on the other side, less deliveries are achieved than expected (NHS report, 2009) [
11]. Sustainable systems are those that perpetuate despite their surrounding changes and the function for their main objectives (Coiera and Hovenga, 2007) [
1]. Health is a vital issue in many nations and is directly related to a sustainable community.
Scenarios can alter the capabilities of a system such as a health system to perceive the nature and effect of the future. Therefore, scenarios can help sense the future and its prerequisites that need to be dealt with (Gnatzy and Moser, 2012; Gille and Houy, 2014; Rhisiart et al., 2015) [
12,
13,
14]. In the general structure of countries, the health structure is remarkably diverse, despite having some relatively comparative aspects. Considerably, Iran is not an exception, setting important strategic plans for upgrading the general health structure of the country.
Speaking of strategic plans, there are two general approaches of using public taxation, called the Boursig approach and Bimsark approach, i.e., social health insurance in which the latter is followed in Iranian policy making. Public budget, social health insurances, the family’s pocket pays, and private insurance are the financial structures for revenue gathering in Iran (Keshavarzian, 2014) [
15].
Concerning the contexts of Iran, strategic planning, futures studies, decision making, and policy making are required to create a holistic picture for managing the future in superior ways. Each of the specialized plans need time to be developed and progressed alongside thoroughly considering the health structure.
In the current situation, the general position of the country is so dynamic and seems to have experienced some improvements compared to the previous decade. It implies an appropriate situation for the country to be developed in different aspects, especially in public health with a sustainable structure. Future scenarios as a framework can be conducive in this procedure and generally can be considered as the backbone to support this idea in the best way. In general, scenarios are qualitative, and there are different ways to evaluate them. It is believed that quantitative evaluations are more accurate in comparison with qualitative structures if quantitative evaluation is possible.
“Multiple attribute decision making (MADM)-based scenarios” is the latest perspective to consider scenarios in a complete quantitative way (Hashemkhani Zolfani et al., 2016a) [
16]. In comparison with other methods and perspectives, this structure is independent and takes future scenarios into account in its structure and methodology, meaning that it enjoys the expert-based structure, which is similar to other decision-making methods. Facing the related future of the policies and strategic decisions is too complicated. So, this approach has an advantage to lead policy makers toward having a better sight on the critical points and topics. In addition, creating a wider picture is something that is not common among approaches and methods, especially toward future scenarios and events. For this reason, the health system of countries appears as a critical and serious topic on which governments are spending time all around the world. Comparably, Iran’s health structure is an evolutionary path through which the development of foresights models importantly seems to be necessary for the country. Finally, coming to the expert-based structure of this methodology, an institution (Institute for Futures Studies in Health) was selected as the pilot for this study.
In this study, probable related future scenarios of health financing will be directed in an “MADM-based scenarios” structure for analyzing the general environment of the future of the health structure of the country in a sustainable way. Two MADM methods, SWARA and WASPAS, will be applied as a suitable hybrid MADM model and a detailed discussion will be presented finally.
2. Literature Review
In this section, the sustainable health structure and current state of the health system in Iran are discussed as two influential issues.
2.1. Sustainable Health
Sustainable development has been defined as “meeting the needs of people here and at the present time, without prejudicing the needs of others elsewhere and in the future” (Pencheon, 2015) [
17].
The primary aspects of sustainable development are economic, social, and environmental. However, sustainable development has been expanded into other dimensions according to the contexts of the studied situation. In the related context of the present study, the governance dimension was introduced as the new dimension. The fundamental issue is the continuous and harmonious interactions of all these dimensions to create the desired balance and construct sustainable systems. Health is critical to achieving these four pillars (Sustainable Development Solutions Network, 2014) [
18].
As claimed by Liaropoulos and Goranitis [
19], economic crises have brought unprecedented attention to the healthcare establishment based on sustainability. For this reason, sustainable healthcare becomes fundamentally pertinent to sustainable financing. Wages decrease due to economic crises and unemployment matters, and accordingly healthcare insurance cover rises with medical costs. To tackle the problem of increasing costs, an MADM-based scenario is applied to prioritize sustainable healthcare criteria and their future impacts to shed lights on future sustainable healthcare financing under sanction circumstances.
To achieve sustainability in a health system, all the functions of the health system should collaborate in a balanced and sustainable form in fulfilling their tasks consistent with sustainability requirements (Smith et al., 2008) [
20]. A sustainable health model can be achieved by provisioning high quality and improved health services, and it can guarantee the perceived safety, improve life quality, enhance well-being, and promote public health. A sustainable health system not only deals with diseases but also with dimensions and determinants of health (Timmers, 2014) [
21].
Health systems are central to the new agenda in which the 13 health targets are proposed to cover most national health concerns. Universally, health coverage achieving access to quality health care is stated in declaration states. Universal health coverage provides several opportunities such as inclusion, equity, financial protection, livelihood generation, a common global vision, and a unified global rallying point. UHC includes health protection, promotion, prevention, treatment, rehabilitation, and palliation. Health is positioned as the major contributor to the other sustainable development goals (SDGs); by overlooking health, many of the other goals would remain inconclusive (Agenda for sustainable development 2015) [
22].
As one of the widespread problems of the millennium in goal development, in the new agenda after the segmentation of countries, health systems are required to provide integrated and fair services considering the costs and resources.
The sustainable development goals are intertwined and indivisible so that progress in one area relies on progress in many other areas as the synergies occur among health, education, nutrition, social protection, and conflict.
Most importantly, the sustainability of a health system is highly dependent on its sustainable financing, as it can ensure a method for financial contributions of prepayment for health care. It aims to reduce the risk share among the population, avoid catastrophic health-care expenditure, and improve the individual’s health status (WHA, 2005) [
23].
2.2. Current State of Health System Financing in Iran
Health is currently generally perceived as a fundamental right, and the urgency of some global health issues has pushed global health policy to the top of the international agenda (Gottret and Schieber, 2000) [
24]. Health financing is a standout amongst the most imperative components in health systems to promote health. Health financing refers to the “function of a health system concerned with the mobilization, accumulation and allocation of money to cover the health needs of the people, individually and collectively, in the health system the purpose of health financing is to make funding available, as well as to set the right financial incentives to providers, to ensure that all individuals have access to effective public health and personal health care” (The World Health Report, 2000) [
25].
Health financing is principal to the capacity of health systems to maintain and improve human welfare. At the extreme, without the necessary funds, no health workers would be employed, no medicines would be accessible, and no health promotion or prevention would occur.
The Iranian health structure system has an egalitarian perspective, although there are so many challenges in between. After the revolution, around 40 years ago, health insurance started covering people, and the government still has been trying to support people in terms of health insurance (Rashidian et al., 2018) [
26]. The Iranian insurance system is a combination of all sectors, both public and private, etc.; however, it is mostly public. Primary care payments mostly are based on subsidy and capitation, while hospital payments are considered according to the general costs and services of physicians (Almaspoor Khangah et al., 2017) [
27]. In Iran, primary health care is financed and delivered predominantly by the government. Secondary and tertiary cares are delivered both publicly and privately (Kavosi et al., 2012) [
28].
Since May 2014, after President Rouhani’s government starting day, his new policies in the government about Ministry of Health and Medical Education (MoHME) followed new strategies and plans in the health structure of the country as a “Health System Transformation Plan” (HSTP) in terms of increasing the equity in different regions of Iran where people are equally treated while categorized in differently economic levels (Olyaeemanesh et al., 2018) [
29].
The main public health insurers are as follows.
The Social Security Organization is one of the largest health insurers in Iran. All the people employed in the formal divisions, except for the government authorities and administration individuals, contribute to the fund and take advantage of this organization.
The Medical Service Insurance Organization provides health insurance for government employees, students, and provincial inhabitants. The rural population, who were not covered by any insurance, became qualified to receive benefits voluntarily in 2000.
The Military Personnel Insurance Organization provides health insurance for military personnel.
The Emdade-Emam Committee provides health insurance for the uninsured poor. Although a small rate of Iranian individuals is not secured by any of the insurance coverage associations, some of them have enlisted in two diverse medical coverage arranges, which are empowered by a small premium (Mehrdad, 2009) [
30].
3. Methodology
To date, various methods have been developed and introduced in MADM; however, the general concept of this research is based on the new future-oriented MADM and MADM-based scenarios, which is presented to make future scenarios quantitative and multi-attribute based, simultaneously (Hashemkhani Zolfani et al., 2016a) [
16]. Each scenario can be considered separately, and each MADM-based scenario is utilized for making decisions about forthcoming situations. This new methodology has been presented to empower new future-based trends in the MADM field such as prospective MADM (Hashemkhani Zolfani et al., 2016b; Hashemkhani Zolfani et al., 2018b; Hashemkhani Zolfani and Masaeli, 2019) [
31,
32,
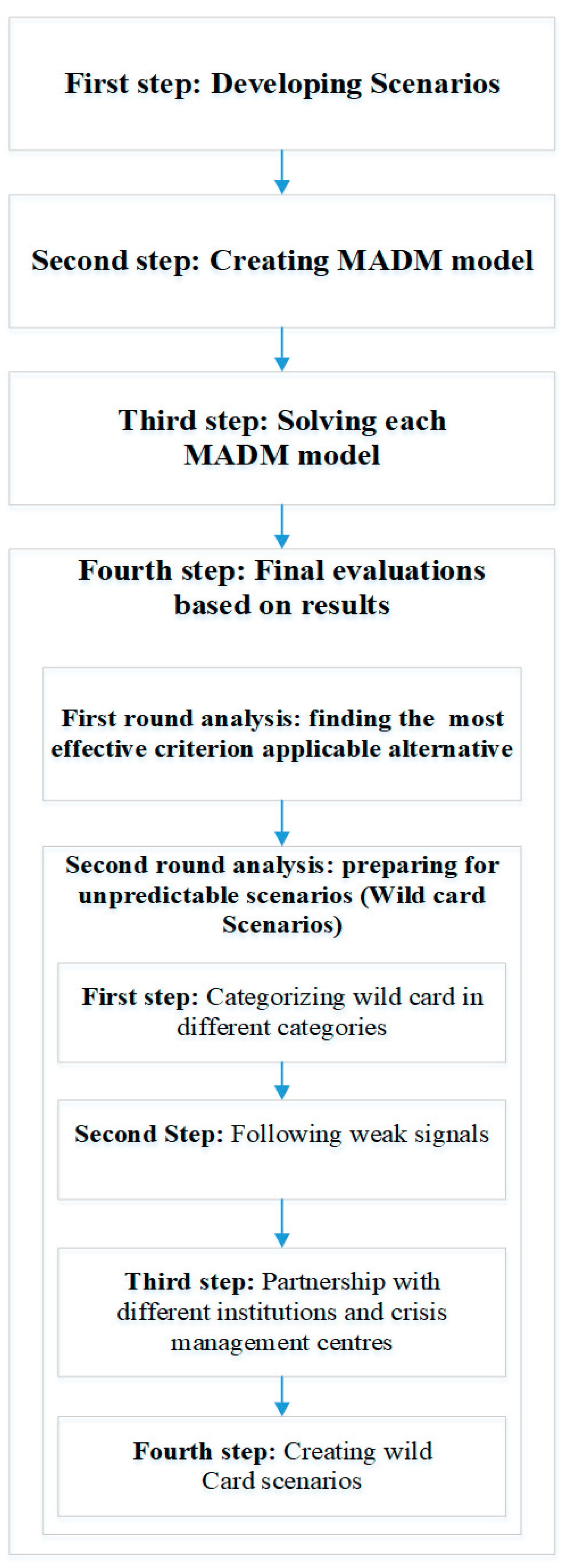
33]. “MADM-based scenarios” are in contrast with scenarios-based MADM. The concept of MADM-based scenarios is not intended to assess the scenarios as, the MADM is the core concept, while in another previous perspective, scenarios are considered to be the core area under study. In this concept, scenarios support presenting a superior model with MADM methods in practice and eventually, a final evaluation can be performed and an ultimate decision can be made.
A foresight comprehensive plan can be completely different in future scenarios. In a foresight strategic policy, pre-planning is considered in all possible scenarios. It can be inferred that future scenarios are similar in most components, although some differences exist among the criteria, alternatives, and relative importance. A final analysis is structured respecting all scenarios and MADM models based on the scenarios. It can be deduced that MADM-based scenarios form a multi-disciplinary perspective comprised of two multi-disciplinary fields, which are futures studies and multiple criteria decision making (MCDM) as a sub-field of Decision Science. The process of the MADM-based scenarios’ concept is illustrated in
Figure 1.
The classic part of “MADM-based scenarios” is structured with classic MADM methods. SWARA-WASPAS as a hybrid model is selected for this study.
In the present study, a policy-based structure is applied in decision making related to selecting criteria, as it is more pertinent to the SWARA method comparing other MADM methods for criteria weighting and evaluating. SWARA-WASPAS is a new fast-growing hybrid model that has been presented in recent years as a powerful hybrid model for solving multi-criteria decision problems (Hashemkhani Zolfani et al., 2013) [
34]. WASPAS itself has both of the advantages of its two classic methods. Considering the importance of this new hybrid MADM model, a review article has been published recently that shows dimensions of the framework from different points of view (Mardani et al., 2017) [
35]. Published studies were identified using SWARA-WASPAS research strategy as listed below:
Vafaeipour et al. [
36] in an assessment of regional priority for the implementation of solar projects.
Bitarafan et al. [
37] in an evaluation of real-time intelligent sensors for the structural health monitoring of bridges.
Aghdaie et al. [
38] in sales branches performance evaluation.
Ghorshi Nezhad et al. [
39] in planning the priority of high-tech industries.
Khodadadi et al. [
40] in evaluating the process of chemical wastewater purification.
Karabašević et al. [
41] for personnel selection.
Yazdani et al. [
42] in material selection.
Mardani et al. [
35] as a systematic review and meta-analysis of SWARA and WASPAS methods.
Ren et al. (2019) [
43] in electric vehicle charging station site selection.
3.1. Step-Wise Weight Assessment Ratio Analysis (SWARA)
SWARA is one of the MADM methods that applies policy-based perspective for criteria weighting and evaluating (Hashemkhani Zolfani and Saparauskas, 2013) [
44]. SWARA is comparable with other MADM methods such as AHP (Saaty 1980) [
45], ANP (Saaty and Vargas 2001) [
46], FARE (Ginevicius, 2011) [
47], BWM (Rezaei, 2015) [
48] (Haghnazar Kouchaksaraei et al., 2015 [
49]; Hashemkhani Zolfani et al., 2015) [
50], rough strength relational DEMATEL (Roy et al., 2018) [
51], and extended SWARA (Hashemkhani Zolfani et al., 2018a) [
52]. The first step in the SWARA method is ranking criteria regarding their priority, which is the policy-based section of this method that can be advantageous for decision making on the top level of policy making [
53]. SWARA is characterized as a friendly structure method that works in a straightforward manner. The procedure of SWARA is based on the below-mentioned steps (Stanujkic et al., 2015) [
54]:
- Step 1
At the first step, all criteria should be ranked according to experts’ viewpoints.
- Step 2
From the second criterion, a comparative importance of the average value should be done as follows: the relative importance of criterion in relation to the previous () criterion.
- Step 3
Determine the coefficient
- Step 4
Determine the recalculated weight
- Step 5
Final step in calculating criteria’ weights
where
denotes the relative weight of criterion
.
3.2. Weighted Aggregated Sum Product Assessment (WASPAS)
WASPAS has been introduced as the one of the state-of-the-art developed MADM methods for evaluating alternatives based on a combination of weighted sum model (WSM) and weighted product model (WPM) (Zavadskas et al., 2012) [
55]. The procedure of WASPAS is presented below (Stojic et al., 2018) [
56]:
- Step 1.
Establish a normalized decision-making matrix:
If the opt value is min
- Step 2.
Calculate the WASPAS weighted and normalized decision-making matrix for the summarizing part:
- Step 3.
Calculate the WASPAS weighted and normalized decision-making matrix for the multiplication part:
- Step 4.
Final calculating for evaluating and prioritizing alternatives:
4. Case Study
The Institute of Futures Studies in Health is in affiliation with Kerman Medical University consisting of five research centers of Modeling in Health, Social Determinants of Health, Health Services Management, Medical Informatics, and the Regional Knowledge Hub, WHO Collaboration Center for HIV Surveillance. The institute delivers consulting services reflecting contemporary topics and issues for future-oriented projects, documents and plans for assistance, research, training, and development deputy of the Health and Medical Education Ministry, and it also cooperates with the Academy of Medical Sciences.
The expertise areas of the institute are Medical informatics, Health services management, Social determinants of health, Modeling in health, HIV surveillance, Data capacity, Data mining, Systematic review, Meta-analysis and meta-synthesis, System dynamics, Futures studies methods, Statistics, and Epidemiology and health philosophy.
5. Future Scenarios
Four possible and probable scenarios are established regarding the experts’ standpoints to demonstrate the future in practice. The general concept has been structured with a foresight perspective as a national plan for the country. Each scenario can be a possible future for the country that can directly affect the health structure.
At the general conference meeting, each scenario was discussed along with its criteria, and final criteria were selected. It is noteworthy that criteria were developed and selected based on each scenario in the future i.e., for each probable future, diverse criteria would be suitable for evaluating the intended situation.
In the procedure of establishing scenarios, finding key criteria and probable important alternatives (strategies), experts cooperated with the director of the research. As mentioned earlier, “The Institute for Futures Studies in Health” is responsible for futures studies regarding the healthcare system of the country. An expert team was selected for this study, and their information is presented in
Table 2.
The final future scenarios based on the experts’ opinions are presented below:
Membership in World Trade Organization (WTO)
Dynamically basic insurance
International joint cooperation
Effective resources management
Futures Scenarios: Definitions, Criteria, and Alternatives
1. Membership in World Trade Organization (WTO)
WTO had more than 162 members by the end of 2015. WTO is involved with Millennium Development Goals and Sustainable Development Goals. Its international economic structure depends on regulations and the structure of the WTO all over the world. Relations, frameworks, and countries’ overseas issues can be partly influenced by the WTO. One of the probable scenarios, which Iran can be confronted with, will be the economic structure after joining the WTO. The economical aspect in each section can evolve differently. The health structure of the country has this opportunity to make a strategic plan for developing a health framework along diverse paths.
Iran is the biggest country among the observer countries, and turning Iran’s situation from observer to permanent membership is not far from reality. It would be easier to access medicine in all aspects such as technologies, and medicine would be cheaper with higher quality as well. International cooperation in the treatment of patients in hospitals and other various aspects can be developed into multi-nationals and completely international. New opportunities would exist in research and technological innovations for the treatment of diseases and exploring new medicines for the country. In the process of setting up a futures exercise, the probable situations and scenarios would turn into realistic ones through strategic plans. Final criteria of this scenario are presented in
Table 3.
In this section, the analysis of alternatives and the selection of the most important ones by experts in a conference meeting are presented. Key alternatives related to the “Membership in World Trade Organization (WTO)” scenario are shown in
Table 4.
2. Dynamic Basic Insurance
In this scenario, insurance companies have the role of a smart shopper by appropriate organizational structure. There is a proper relationship between insurance companies and other organizations involved in the health sector. In dynamic insurance, premiums are collected and calculated sustainably, and both resources and revenue pooling are proper. The structure of health insurance acts properly in terms of quality and quantity. Basic insurance has a good coverage and determines and provides their service package by defined, logical, and smart standards. The level of out-of-pocket payment and catastrophic healthcare expenditure is decreased. Insurance systems monitor the quality of provider’s services and beside the defined and logical mechanisms of their contracts with providers, they also monitor the efficient implementation of the contracts. The position of insurance in the health system is accepted by all its functions. Insurance companies pay providers properly, while the insurance’s choices are limited and the competition among insurances is restricted. Final criteria of the scenario are presented in
Table 5.
For the next scenario, experts made a decision on probable key alternatives for the “Dynamic basic insurance” scenario. The process of this evaluation is structured to just select those alternatives with 100% effectiveness. All alternatives linked to the “Dynamic basic insurance” scenario are shown in
Table 6.
3. International Joint Cooperation
This scenario consists of joint contracts that include the medical education area, educational and research contracts, health technologies, cooperation with international organizations such as the World Health Organization, the design and implementation of the joint projects for health sector reforms, joint graduate students, defining and holding joint training workshops to meet the needs of the same training, increasing foreign investment on technological infrastructure such as hospitals established by an Iranian and foreigner joint force with no border restrictions, defining the benefits of health services free zones such as health settlements or a health island without any visa and passport limitations, health tourism, increasing the quality and diversity of health services, Memorandum of Understanding (MoU) and strategies definition for crisis management, countering and controlling the epidemics and prevalent diseases defined for MOU members, providing opportunities for drawing on the expertise of Iranians living abroad by inviting them to participate in MOU’s implementation, and finally defining the joint projects through which the know-how and know-why knowledge are transferred. As a result, the foreign aid of health system increases. Final criteria of International Joint Cooperation are shown in
Table 7.
Another four alternatives are selected based on experts’ ideas for the “International joint cooperation” scenario, in practice. Alternatives are illustrated in
Table 8.
4. Effective Resources Management
In this scenario, a significant portion of gross domestic product (GDP) is spent on health care. The input resources of the health sector are relatively sustainable. The amount of out-of-pocket payment share to the total health spending is not substantial. Financial data and statistical information on the health system are accessible and integrated. Moreover, the evidence-based philosophy is used by the policy makers. Resource consumption in different parts of the health system is done the most possible ideal way. Controlling the resource consumption is accomplished appropriately. Various groups of stakeholders benefit from the cost effectiveness of the health sector’s advanced technologies, as the most suitable technologies are chosen to be used in health sectors. The relationship between insurance companies, the Ministry of Health, and other health stakeholders is properly established. As a consequence, the community choices of various services increase, which also affects providers’ choices for selecting and delivering the service. It should be kept in mind that during financial crisis in the country, if the state is in charge of financing the health sector, the health sector will confront complications. Final criteria of this scenario are shown in
Table 9.
According to the methodology of MADM-based scenarios, there is no limitation for the numbers of alternatives, criteria, and probable differences. Based on experts’ viewpoints, five key probable alternatives were generated for the “Effective resources management” scenario. “Effective resources management” scenario’s alternatives also are shown in
Table 10.
6. Results
In view of all that has been mentioned so far in the methodology and previous sections, four scenarios are created to show the probable futures. For each scenario, calculations were carried out separately based on a hybrid MADM model (SWARA-WASPAS). The full explanation of the obtained results in each section is explained in
Section 6.1 and
Section 6.2.
6.1. SWARA Results
According to the four scenarios, calculations were performed separately, and each scenario along with its criteria was evaluated based on the SWARA method to prioritize and weigh the criteria. As noted earlier, SWARA is mostly appropriate for the cases that are policy-based rather than for general decision-making structures. Concerning the foresight perspective of the study, a policy and SWARA-based framework was applied for this research. Based on the SWARA methodology and policy-based perspective method, the criteria of each scenario were prioritized based on the experts’ judgments and their importance for the country. The results for each scenario are shown in
Table 11,
Table 12,
Table 13 and
Table 14.
Health services’ quality was selected as the most influential and effective criterion in the first scenario. This criterion also exists in all other scenarios, and it is one of the most effective criteria, undoubtedly.
Justice in health, Level of accountability, and Quality of financial resources management were three new criteria for this scenario, which were not identified as important criteria for the previous scenario. As it can be seen, justice in health was indicated as a vital criterion in this scenario, despite the significance of the quality of health services being considered undeniable since different scenarios have distinct ends.
Quality of human resource management, Cost management (medical equipment), Reinforced social aspects, and Flexibility in management and accountability were justified criteria for the third scenario. Similarly to the previous scenario, the quality of human resource management, which was the key criterion in this scenario, had top priority.
The cost of “Cooperation” and “Level of accessibility (Geographical position)” were other new criteria that were revealed as important criteria only in the fourth scenario. It can be inferred that new criteria in different scenarios are the key criteria of that specific scenario since they are defined respective to their critical situation in the given scenario to increase the accuracy of decision making.
6.2. WASPAS Results
Similarly to the SWARA part, each scenario was evaluated separately. The related alternatives of each scenario were analyzed in this section, and their priorities are shown in
Table 14,
Table 15,
Table 16,
Table 17,
Table 18,
Table 19,
Table 20,
Table 21,
Table 22,
Table 23,
Table 24,
Table 25,
Table 26,
Table 27,
Table 28 and
Table 29. All these evaluations were executed based on WASPAS methodology. The tables of the final ranking are illustrated in the main body of the article, but the calculation parts are presented in
Appendix A (
Table A1).
6.2.1. “Membership in World Trade Organization (WTO)” Scenario
According to the
Table 3, four probable alternatives were selected by experts involved in this research. In this research, future strategies in a special situation were considered as a scenario for the future and as the probable alternatives. Strategies/alternatives of this scenario are: (1) Pharmaceutical Security, (2) Focus of government on research and development (R&D), (3) Empowerment of private sector in both production and technology, and (4) Applying both FDI and equipped new technologies in one structure. The process is shown in
Table 15,
Table 16,
Table 17 and
Table 18.
6.2.2. “Dynamic Basic Insurance” Scenario
As illustrated in
Table 5, four different probable alternatives were selected by the experts of this study. These strategies that are also considered as alternatives in this research are as follows: (1) Hiring international managers, (2) Benchmarking, (3) Supportive governmental policies, and (4) Good governance. The calculations are depicted in
Table 19,
Table 20,
Table 21 and
Table 22.
6.2.3. “International Joint Cooperation” Scenario
In this section, similar to previous scenarios, the selected strategies were evaluated based on WASPAS methodology. The strategies for the dynamic basic insurance scenario include the following subjects: (1) Pharmaceutical security; (2) Supportive governmental policies; (3) Sustainable medical services; and (4) Sustainable human resource management. The results can be seen in
Table 23,
Table 24,
Table 25 and
Table 26.
6.2.4. “Effective Resources Management” Scenario
In this scenario, five strategies were selected as alternatives referring to experts’ opinions. The strategies for the effective resources management scenario are: (1) Benchmarking, (2) Supportive governmental policies, (3) Good governance, (4) Sustainable human resource management, and (5) Re-engineering the process. The final priorities are illustrated in
Table 27,
Table 28,
Table 29 and
Table 30.
7. Discussion
This discussion is prepared in three sections. In the first section, the most effective criterion is addressed, and in the second section, the discovery of the most applicable strategy as an alternative is discussed. The third and last section concentrates on the explanation of the macro monitoring system for the health structure as a comprehensive sustainable health system.
7.1. First Round Analysis: Finding the Most Effective Criterion
According to the methodology, the first round in the discussion is pertinent to the analysis of effective criteria, especially the most effective ones. As it is shown in
Table 31, all 15 criteria and their relative importance (weights) in the different scenarios are presented. Creating
Table 31 prepares a general perspective about criteria and their situations in scenarios.
Considering the critical criteria, the impact of scenarios, their average weights, and their averages based on their priorities are addressed in the second round. As it can be seen, in
Table 32, the mentioned items provide the final analysis of the criteria. A final ranking based on the criteria’s weights and their effectiveness is presented in
Table 32, and the most effective criterion (C
1: Health services’ quality) was identified regarding the expectations.
7.2. First Round Analysis: Finding the Most Applicable Alternative
Similar to the previous section, 11 strategies as alternatives and their priorities in these scenarios are presented in
Table 33, and based on this table, a final evaluation was carried out.
Analyzing and evaluating alternatives is done using different items. Other evaluation methods were utilized for examination, which was beyond this research original methodology. Average in state of max criteria (ASMAC) and Average state of “min” criteria (ASMIC) were added to be checked and examined in this process. A final evaluation of the alternatives is presented in
Table 34. It is noteworthy that these two methods are completely different methods, and no relation exists between them. The final discussion of these two methods is addressed in
Section 8.
The original part of the MADM-based scenarios is the priority based on applicability. Analyzing the priority based on ASMAC and ASMIC was tested for this framework for the first time. The second part was identified as ineffective for two reasons. Firstly, it was not related directly to the original part, and secondly, it was identified as ineffective because of the maximum and minimum criteria. To elaborate more, it was conceived that those alternatives with no minimum criterion can be ranked higher than other alternatives, which are more influential in general.
7.3. Macro Monitoring System
The Institute for Futures Studies in Health of Kerman Medical University has been collaborating as a partner in this research. This institute plays a key role in monitoring weak signals and also preparing scenarios for managing probable crisis in the future. The preparation of Wildcard scenarios has been undertaken by this institute as a concurrent part of the system for directing the general health structure of the country according to macro needs.
7.4. Final Analysis
According to the results, the quality of medical services was identified as the most effective criterion, and sustainable services delivery was recognized as the most applicable alternative. The obtained findings imply that despite the uncertainty of the probable futures, financial sustainability in the health system can be achieved by presenting sustainable and high-quality services delivery.
Sustainable services delivery is affected by three other functions of the health system i.e., stewardship, resource creation, and financing. Thus, to realize the sustainability goals in sustainable service delivery, all these functions need to operate in a sustained manner.
Sustainable medical services delivery was the most applicable alternative for achieving sustainable health financing. It can be deduced that separating a part (a function) of a health system and attempting to make it sustainable does not seem to be pragmatic.
It can be speculated that the economic environment of the health system in three financing layers of international, regional/national, and sectoral (health sector) is interwoven; however, the amount of the effect that can be transformed from the international and regional/national layer to the health financing layer depends on the robustness of the financing mechanisms of the health financing function. For instance, it should be determined how the revenue collection task of the financial system can be performed despite the environmental changes.
Health expenditures are provided from two main channels consisting of the general and private sectors. General expenditures incorporate governmental budget and social security insurance, and private expenditures incorporate out-of-pocket, private insurances and other resources such as donations.
In comparison with other middle and upper-income countries, the governmental share in providing health expenditure is lower in Iran. Two main channels of providing health expenditure are out-of-pocket and governmental payment, which are both affected by other layers of the economic environment. If the health system becomes capable of developing a mechanism of wealth creation such as entrepreneurship based on a national innovation system, moving toward the third generation medical universities, health tourism, etc., this fulfillment will bring about two main results. One of them is the risk reduction as a consequence of the concentration on limited sources and decreasing the dependence on different financing mechanisms. The other result is the lessening of of environmental impacts, which boost the sustainability of the system.
Improving the quality of health services in Iran requires attention to several key factors such as organizing, regulation, financing, payment, and behavioral systems.
Some important factors in organizing are listed as follows: a proper structure for implementing health care programs, determining appropriate structures of quality assessment, providing appropriate definitions of different levels involved in quality promotion, considering the suitable structures for quality-related knowledge share among stakeholders, and defining related appropriate educational and research roles to improve the quality of care.
Defining an appropriate regulatory structure related to quality improvement, the revision of the rules and guidelines associated with different service levels according to the new needs of society (such as chronic diseases), the development of appropriate laws and regulations in the country to produce various types of evidence-based guidelines, and creating a proper understanding about the quality of health legislation are all factors related to the country law and regulation quality.
In regard to the financing factors, the following issues should be considered: defining the health care quality monitoring system of the country and the development of appropriate indicators, considering infrastructural resources of service quality in allocating them in the health sector, creating informational infrastructure related to service quality, providing evidence-based guidelines at different levels of service with the participation of all stakeholders, medical education involvement in training about service qualities concepts and quantitative and qualitative training, a smart selection of models to improve the quality of concepts of stakeholders, motivating and empowering healthcare personnel to provide high-quality services, and ultimately monitoring the quality of inputs such as medicines and medical equipment.
The payment system factors such as creating mechanisms of using quality-based payment methods—and more effectively, the role of insurance in promotion of service quality by strategic purchasing—would enhance the quality of healthcare services.
For the behavioral function, the critical factors that need to be considered are giving feedback related to services quality to providers and society, defining national and local events to appreciate the efforts related to quality improvement, promoting self-assessment processes in organizations providing health services, and institutionalizing moral, social, and cultural values in services delivery to meet the needs of the non-clinical health care community.
8. Methodological Discussion and Contributions
To date, there has been few studies using MADM-based scenarios; hence, this research attempted to add substantially to our understanding of this methodology, in order to demonstrate how this methodology can be applied, and to draw attention to the constructive attributes of this methodology in practice. Additionally, this methodology provides a bright vision for decision makers and policy makers to make more accurate and comprehensive decisions. In this study, two extra evaluation parts were added to this applied methodology. The first one is “Average based on priorities (Min)”, which is influential in evaluating momentous criteria, and the second one is “Estate of alternatives based on ASMAC and ASMIC” which is utilized in the evaluation process of applicable alternatives.
Both extra evaluation parts were presented to be examined in reality and case studies. The results revealed reliable evidence to confirm the validation of “Average based on priorities (Min)”, while no evidence has been attained to support the effective usage of the “Estate of alternatives based on ASMAC and ASMIC” in this specific study. It is surmised that the Average in state of max criteria (ASMAC) and Average state of “min” criteria (ASMIC) were not conducive for finding applicable alternatives due to some limitations and reasons. In the current research, the ranking of alternatives became practically impossible, since alternative 9 did not have a minimum estate. Taken together, these findings suggest that “Average based on priorities (Min)” can be considered as the salient methodology identified as indispensable for finding effective criteria.
9. Conclusions
The current findings add to a growing body of literature on sustainable health financing. In this study, health services’ quality was recognized as the most effective criterion in assessing the different future alternatives. In fact, the promotion of health services’ quality affects different aspects of health system functioning and its enhancement. From the viewpoint of patients, the delivery of quality services is the most paramount aspect of what they receive in a health system. Through the lens of providers, delivering high-quality health services assures their thorough functioning in a health system. From the policy makers’ perspective, delivering health services in a satisfactory quality level implies that the health services are delivered in compliance with standards and regulations; furthermore, it also ensures that the limited health sources are utilized productively. From the health insurance agencies’ outlook, high-quality service delivery can be translated into strategic purchasing for all of the health insurance covered population. At first glance, it may seem that delivering high-quality services will heighten the expenditures. However, after deep contemplation, it can be discerned that delivering high-quality services not only reduces many expenditures incurred by the further reference of patients and the side effects of low-quality health services delivery, it also makes the system well-known as a high quality health care system that is highly committed to its social responsibility besides its other administrative responsibilities, which meets the social pillar of sustainability approach. Therefore, high-quality services delivery can be the joint criterion incorporating the distinctive functions of the health system such as financing, service delivery, and so on.
In the other part of the study, sustainable medical service was determined as the most pertinent and applicable alternative in various health financing scenarios, which signifies that economic, social, and environmental aspects of sustainability are fostered in superior services delivery to individuals. Indeed, sustainable medical services can assure the quality of the services, which was determined as the most effective criterion of health financing for future. In regard to sustainability standards and principles, financing the health system should be possible in every economic, social, and environmental fluctuation influencing the health system such as changes to the oil prices, other probable sanctions of Iran, population aging, and so forth.
Sustainable medical services can guarantee the quality of medical services to establish a sustainable financing in a health system regardless of different probable future scenarios of the health system in Iran. Future research directions in sustainable health and medical services based on the MADM scenario will lead researches to the proper delivery and quality monitoring of medical products under sanction circumstances. For this reason, sustainable development that brings about new rules, regulations, and changes of medical delivery/products with a high quality of service is necessarily needed under sanction. For instance, the wide accessibility of alternative medical products is of interest under sanctioned circumstances based on medical priorities. Moreover, the proper delivery of medical products is guaranteed when alternative medical products are used, and of course, they become economically controlled when sanctions are applied. Future analysis and insight need to be investigated on how potential environmentally friendly medical sources of the sanctioned countries can alter outsourced counterparts to maintain sustainability in a myriad of aspects.

 and
and 
{kind=link}
