Indocyanine Green-Enhanced Colorectal Surgery—between Being Superfluous and Being a Game-Changer

 ,
,
Abstract
:1. Introduction
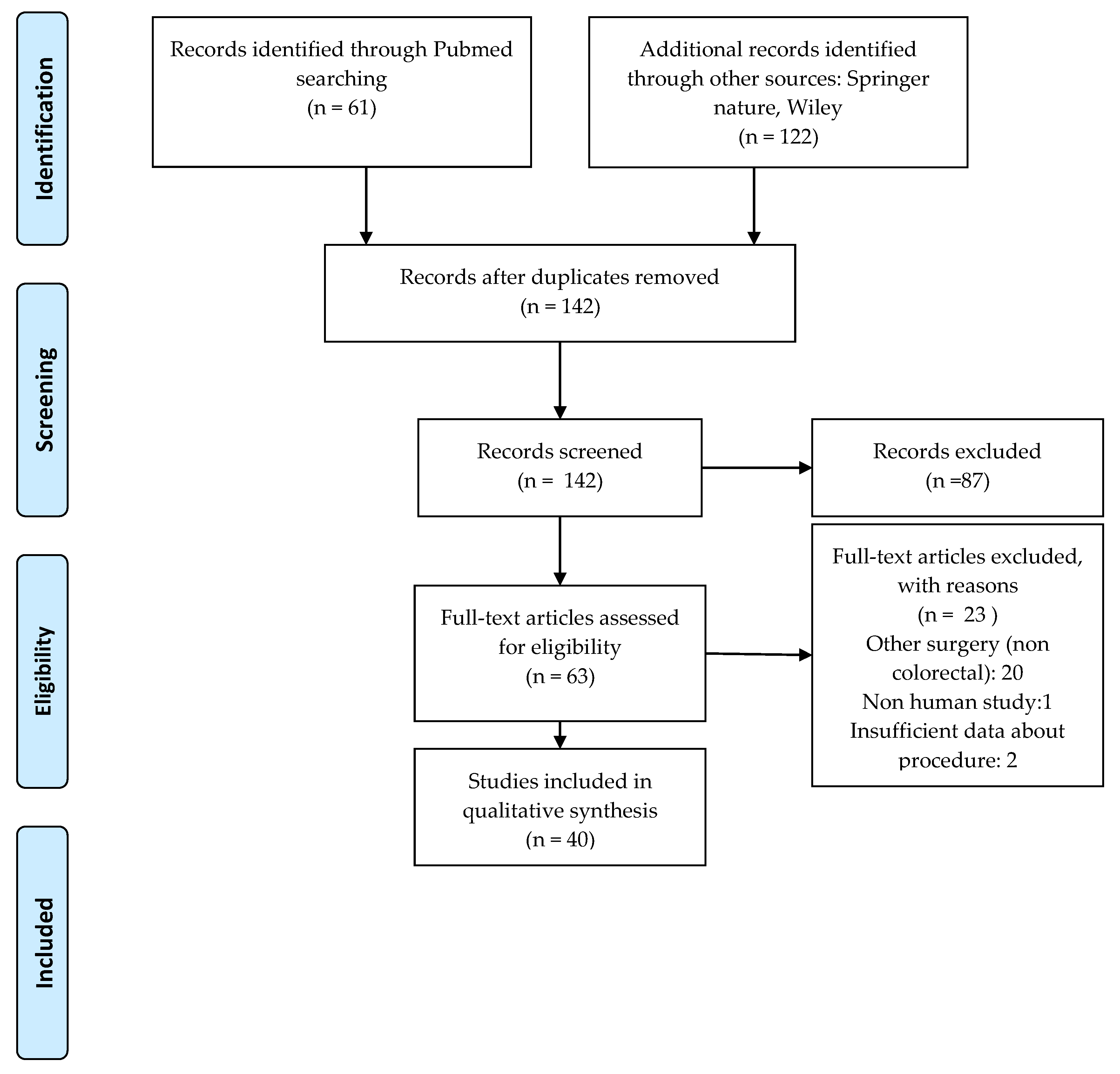
2. Materials and Methods
3. Results
3.1. The Molecule of ICG and the Principle of NIR-Assisted Surgery
3.2. Impact of ICG-Enhanced Surgery on Anastomotic Leak Rates
3.2.1. The Anastomotic Leaks (AL)—A Significant Factor of Outcome in Colorectal Surgery
3.2.2. Study Designs—Comparative Aspects
3.2.3. ICG NIR Fluorescence Assessment: Doses, Devices, Protocols
3.2.4. The Rate of AL with ICG NIR-Enhanced Surgery
3.3. The Usefulness of ICG in Sentinel Lymph Node (SLN) and Lymphatic Basin Identification
3.3.1. ICG NIR Fluorescence in Identifying SLN in Colorectal Cancer Surgery
Study Designs—Comparative Aspects
Technical Aspects of ICG Injection: Dose, Concentration, Technique
Outcomes: Overall Sensitivity and Specificity of ICG Near-Infrared Fluorescence
3.3.2. ICG NIR Fluorescence in Lateral Pelvic Lymph Node Dissection (LPLD) in Rectal Cancer
4. Discussion
4.1. ICG NIR-Enhanced Surgery in Preventing AL: When Should Be It Performed by Routine?
4.2. ICG NIR Enhanced Surgery in SLN: Is It a Game-Changer?
4.2.1. Controversies in the Concept of SLN in Colorectal Cancer
4.2.2. ICG NIR-Assisted Surgery Performance in Detecting SLN
4.2.3. ICG NIR-Assisted Surgery in LPLD
4.3. A Step Forward from Superfluous: Attempts in Standardization and Quantification of ICG NIR-Enhanced Surgery
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Litynski, G.S. Erich Mühe and the Rejection of Laparoscopic Cholecystectomy (1985): A Surgeon Ahead of His Time. JSLS J. Soc. Laparoendosc. Surg. 1999, 2, 341–346. [Google Scholar]
- Raabe, A.; Beck, J.; Gerlach, R.; Zimmermann, M.; Seifert, V. Near-infrared indocyanine green video angiography: A new method for intraoperative assessment of vascular flow. Neurosurgery 2003, 52, 132–139. [Google Scholar] [PubMed]
- Alander, J.T.; Kaartinen, I.; Laakso, A.; Pätilä, T.; Spillmann, T.; Tuchin, V.V.; Venermo, M.; Välisuo, P. A Review of Indocyanine Green Fluorescent Imaging in Surgery. Int. J. Biomed. Imaging 2012, 2012, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Klais, C.M.; Ober, M.; Yannuzzi, L.A. Indocyanine Green Angiography: General Aspects and Interpretation. In Retinal Angiography and Optical Coherence Tomography; Springer Science and Business Media LLC: Berlin, Germany, 2008; pp. 43–59. [Google Scholar]
- Grosek, J.; Tomažič, A. Key clinical applications for indocyanine green fluorescence imaging in minimally invasive colorectal surgery. J. Minimal Access Surg. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Lakowicz, J.R. Principles of Fluorescence Spectroscopy, 2nd ed.; Kluwer Academic/Plenum Publishers: New York, NY, USA; London, UK; Moscow, Russia; Dordrecht, The Netherlands, 1999. [Google Scholar]
- Savopol, T. Curs Master: Elemente de Spectroscopie; Carol Davila University of Medicine and Pharmacy: Bucharest, Romania, 2012; Unpublished work. [Google Scholar]
- Fattahi, A.S.; Tavassoli, A.; Rohbakhshfar, O.; Sadeghi, R.; Abdollahi, A.; Forghani, M.N. Can methylene blue dye be used as an alternative to patent blue dye to find the sentinel lymph node in breast cancer surgery? J. Res. Med Sci. 2014, 19, 918–922. [Google Scholar]
- Mandovra, P.; Kalikar, V.; Patankar, R.V. Real-Time Visualization of Ureters Using Indocyanine Green During Laparoscopic Surgeries: Can We Make Surgery Safer? Surg. Innov. 2019, 26, 464–468. [Google Scholar] [CrossRef]
- Slack, D. Use of Indocyanine Green for Localization and Preservation of Ureters in Robotic-Assisted Colon Surgery. Clin. Surg. J. 2020, 4, 44–46. [Google Scholar]
- Van Manen, L.; Handgraaf, H.J.M.; Diana, M.; Dijkstra, J.; Ishizawa, T.; Vahrmeijer, A.L.; Mieog, J.S.D. A practical guide for the use of indocyanine green and methylene blue in fluorescence-guided abdominal surgery. J. Surg. Oncol. 2018, 118, 283–300. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2018, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Ris, F.; Hompes, R.; Cunningham, C.; Lindsey, I.; Guy, R.; Jones, O.; George, B.; Cahill, R.A.; Mortensen, N. Near-infrared (NIR) perfusion angiography in minimally invasive colorectal surgery. Surg. Endosc. 2014, 28, 2221–2226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudszus, S.; Roesel, C.; Schachtrupp, A.; Höer, J.J. Intraoperative laser fluorescence angiography in colorectal surgery: A noninvasive analysis to reduce the rate of anastomotic leakage. Langenbeck’s Arch. Surg. 2010, 395, 1025–1030. [Google Scholar] [CrossRef]
- Thornton, F.J.; Barbul, A. Healing in the gastrointestinal tract. Surg. Clin. N. Am. 1997, 77, 549–573. [Google Scholar] [CrossRef]
- Lange, M.M.; Buunen, M.; Van De Velde, C.J.H.; Lange, J.F. Level of Arterial Ligation in Rectal Cancer Surgery: Low Tie Preferred over High Tie. A Review. Dis. Colon Rectum 2008, 51, 1139–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohya, H.; Watanabe, J.; Suwa, H.; Suwa, Y.; Ishibe, A.; Masui, H.; Nagahori, K.; Kunisaki, C.; Endo, I. Incidence and risk factors for fluorescence abnormalities on near-infrared imaging using indocyanine green in stapled functional end-to-end anastomosis in laparoscopic colectomy. Int. J. Color. Dis. 2020, 1–8. [Google Scholar] [CrossRef]
- Kin, C.; Vo, H.; Welton, L.; Welton, M. Equivocal Effect of Intraoperative Fluorescence Angiography on Colorectal Anastomotic Leaks. Dis. Colon Rectum 2015, 58, 582–587. [Google Scholar] [CrossRef]
- Sherwinter, D.A.; Gallagher, J.; Donkar, T. Intra-operative transanal near infrared imaging of colorectal anastomotic perfusion: A feasibility study. Color. Dis. 2012, 15, 91–96. [Google Scholar] [CrossRef]
- Kawada, K.; Hasegawa, S.; Wada, T.; Takahashi, R.; Hisamori, S.; Hida, K.; Sakai, Y. Evaluation of intestinal perfusion by ICG fluorescence imaging in laparoscopic colorectal surgery with DST anastomosis. Surg. Endosc. 2016, 31, 1061–1069. [Google Scholar] [CrossRef]
- Somashekhar, S.P.; Reddy, G.R.K.; Deshpande, A.Y.; Ashwin, K.R.; Kumar, R. A prospective study of real-time identification of line of transection in robotic colorectal cancer surgery by ICG. J. Robot. Surg. 2020, 1–6. [Google Scholar] [CrossRef]
- Jafari, M.D.; Lee, K.H.; Halabi, W.J.; Mills, S.D.; Carmichael, J.C.; Stamos, M.J.; Pigazzi, A. The use of indocyanine green fluorescence to assess anastomotic perfusion during robotic assisted laparoscopic rectal surgery. Surg. Endosc. 2013, 27, 3003–3008. [Google Scholar] [CrossRef]
- Gröne, J.; Koch, D.; Kreis, M.E. Impact of intraoperative microperfusion assessment with Pinpoint Perfusion Imaging on surgical management of laparoscopic low rectal and anorectal anastomoses. Color. Dis. 2015, 17, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellan, M.; Spinoglio, G.; Pigazzi, A.; Lagares-Garcia, J.A. The influence of fluorescence imaging on the location of bowel transection during robotic left-sided colorectal surgery. Surg. Endosc. 2014, 28, 1695–1702. [Google Scholar] [CrossRef] [PubMed]
- Boni, L.; Fingerhut, A.; Marzorati, A.; Rausei, S.; Dionigi, G.; Cassinotti, E. Indocyanine green fluorescence angiography during laparoscopic low anterior resection: Results of a case-matched study. Surg. Endosc. 2016, 31, 1836–1840. [Google Scholar] [CrossRef] [PubMed]
- Jafari, M.D.; Wexner, S.D.; Martz, J.E.; McLemore, E.C.; Margolin, D.A.; Sherwinter, D.A.; Lee, S.W.; Senagore, A.J.; Phelan, M.J.; Stamos, M.J. Perfusion Assessment in Laparoscopic Left-Sided/Anterior Resection (PILLAR II): A Multi-Institutional Study. J. Am. Coll. Surg. 2015, 220, 82–92.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Nardi, P.; Elmore, U.; Maggi, G.; Maggiore, R.; Boni, L.; Cassinotti, E.; Fumagalli, U.; Gardani, M.; De Pascale, S.; Parise, P.; et al. Intraoperative angiography with indocyanine green to assess anastomosis perfusion in patients undergoing laparoscopic colorectal resection: Results of a multicenter randomized controlled trial. Surg. Endosc. 2019, 34, 53–60. [Google Scholar] [CrossRef]
- Kim, J.C.; Lee, J.L.J.L.; Yoon, Y.S.Y.S.; Alotaibi, A.M.A.M.; Kim, J. Utility of indocyanine-green fluorescent imaging during robot-assisted sphincter-saving surgery on rectal cancer patients. Int. J. Med. Robot. Comput. Assist. Surg. 2015, 12, 710–717. [Google Scholar] [CrossRef]
- Su, H.; Wu, H.; Bao, M.; Luo, S.; Wang, X.; Zhao, C.; Liu, Q.; Wang, X.; Zhou, Z.; Zhou, H. Indocyanine green fluorescence imaging to assess bowel perfusion during totally laparoscopic surgery for colon cancer. BMC Surg. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Mizrahi, I.; Abu-Gazala, M.; Rickles, A.S.; Fernandez, L.M.; Petrucci, A.; Wolf, J.; Sands, D.R.; Wexner, S.D. Indocyanine green fluorescence angiography during low anterior resection for low rectal cancer: Results of a comparative cohort study. Tech. Coloproctology 2018, 22, 535–540. [Google Scholar] [CrossRef]
- Son, G.M.; Kwon, M.S.; Kim, Y.; Kim, J.; Kim, S.H.; Lee, J.W. Quantitative analysis of colon perfusion pattern using indocyanine green (ICG) angiography in laparoscopic colorectal surgery. Surg. Endosc. 2018, 33, 1640–1649. [Google Scholar] [CrossRef] [Green Version]
- Ogino, T.; Hata, T.; Kawada, J.; Okano, M.; Kim, Y.; Okuyama, M.; Tsujinaka, T. The Risk Factor of Anastomotic Hypoperfusion in Colorectal Surgery. J. Surg. Res. 2019, 244, 265–271. [Google Scholar] [CrossRef]
- Hasegawa, H.; Tsukada, Y.; Wakabayashi, M.; Nomura, S.; Sasaki, T.; Nishizawa, Y.; Ikeda, K.; Akimoto, T.; Ito, M. Impact of intraoperative indocyanine green fluorescence angiography on anastomotic leakage after laparoscopic sphincter-sparing surgery for malignant rectal tumors. Int. J. Color. Dis. 2020, 35, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Tsang, D.Y.-P.; Leung, L.-H.A.; Lau, C.-W.; Tang, C.-N. Indocyanine green fluorescence angiography to evaluate anastomotic perfusion in colorectal surgery. Int. J. Color. Dis. 2020, 35, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Nishigori, N.; Koyama, F.; Nakagawa, T.; Nakamura, S.; Ueda, T.; Inoue, T.; Kawasaki, K.; Obara, S.; Nakamoto, T.; Fujii, H.; et al. Visualization of Lymph/Blood Flow in Laparoscopic Colorectal Cancer Surgery by ICG Fluorescence Imaging (Lap-IGFI). Ann. Surg. Oncol. 2015, 23, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Santi, C.; Casali, L.; Franzini, C.; Rollo, A.; Violi, V. Applications of indocyanine green-enhanced fluorescence in laparoscopic colorectal resections. Updat. Surg. 2018, 71, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, J.; Ishibe, A.; Suwa, Y.; Suwa, H.; Ota, M.; Kunisaki, C.; Endo, I. Indocyanine green fluorescence imaging to reduce the risk of anastomotic leakage in laparoscopic low anterior resection for rectal cancer: A propensity score-matched cohort study. Surg. Endosc. 2019, 34, 202–208. [Google Scholar] [CrossRef]
- Wada, T.; Kawada, K.; Hoshino, N.; Inamoto, S.; Yoshitomi, M.; Hida, K.; Sakai, Y. The effects of intraoperative ICG fluorescence angiography in laparoscopic low anterior resection: A propensity score-matched study. Int. J. Clin. Oncol. 2018, 24, 394–402. [Google Scholar] [CrossRef]
- Guo, J.; Yang, H.; Wang, S.; Cao, Y.; Liu, M.; Xie, F.; Liu, P.; Zhou, B.; Tong, F.; Cheng, L.; et al. Comparison of sentinel lymph node biopsy guided by indocyanine green, blue dye, and their combination in breast cancer patients: A prospective cohort study. World J. Surg. Oncol. 2017, 15, 196. [Google Scholar] [CrossRef] [Green Version]
- Carrara, A.; Motter, M.; Amabile, D.; Pellecchia, L.; Moscatelli, P.; Pertile, R.; Barbareschi, M.; DeCarli, N.L.; Ferrari, M.; Tirone, G. Predictive value of the sentinel lymph node procedure in the staging of non-metastatic colorectal cancer. Int. J. Color. Dis. 2020, 1–8. [Google Scholar] [CrossRef]
- Hirche, C.; Mohr, Z.; Kneif, S.; Doniga, S.; Murawa, D.; Strik, M.; Hünerbein, M. Ultrastaging of colon cancer by sentinel node biopsy using fluorescence navigation with indocyanine green. Int. J. Color. Dis. 2011, 27, 319–324. [Google Scholar] [CrossRef]
- Currie, A.; Brigic, A.; Thomas-Gibson, S.; Suzuki, N.; Moorghen, M.; Jenkins, J.T.; Faiz, O.; Kennedy, R.H. A pilot study to assess near infrared laparoscopy with indocyanine green (ICG) for intraoperative sentinel lymph node mapping in early colon cancer. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 2044–2051. [Google Scholar] [CrossRef]
- Liberale, G.; Vankerckhove, S.; Gomez-Galdon, M.; Donckier, V.; Larsimont, D.; Bourgeois, P. Fluorescence imaging after intraoperative intravenous injection of indocyanine green for detection of lymph node metastases in colorectal cancer. Eur. J. Surg. Oncol. (EJSO) 2015, 41, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Liberale, G.; Vankerckhove, S.; Galdon, M.G.; Larsimont, D.; Ahmed, B.; Bouazza, F.; Moreau, M.; El Nakadi, I.; Donckier, V.; Bourgeois, P.; et al. Sentinel Lymph Node Detection by Blue Dye Versus Indocyanine Green Fluorescence Imaging in Colon Cancer. Anticancer. Res. 2016, 36, 4853–4858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, J.; Ota, M.; Suwa, Y.; Ishibe, A.; Masui, H.; Nagahori, K. Real-Time Indocyanine Green Fluorescence Imaging–Guided Complete Mesocolic Excision in Laparoscopic Flexural Colon Cancer Surgery. Dis. Colon Rectum 2016, 59, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Andersen, H.S.; Bennedsen, A.L.B.; Burgdorf, S.K.; Eriksen, J.R.; Eiholm, S.; Toxværd, A.; Riis, L.B.; Rosenberg, J.; Gögenur, I. In vivo and ex vivo sentinel node mapping does not identify the same lymph nodes in colon cancer. Int. J. Color. Dis. 2017, 32, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Nagata, K.; Endo, S.; Hidaka, E.; Tanaka, J.-I.; Kudo, S.; Shiokawa, A. Laparoscopic sentinel node mapping for colorectal cancer using infrared ray laparoscopy. Anticancer. Res. 2006, 26, 2307–2312. [Google Scholar] [PubMed]
- Kusano, M.; Tajima, Y.; Yamazaki, K.; Kato, M.; Watanabe, M.; Miwa, M. Sentinel lymph node mapping guided by indocyanine green fluorescence imaging: A new method for sentinel lymph node navigation surgery in gastrointestinal cancer. Dig. Surg. 2008, 25, 103–108. [Google Scholar] [CrossRef]
- Cahill, R.A.; Anderson, M.; Wang, L.M.; Lindsey, I.; Cunningham, C.; Mortensen, N.J. Near-infrared (NIR) laparoscopy for intraoperative lymphatic road-mapping and sentinel node identification during definitive surgical resection of early-stage colorectal neoplasia. Surg. Endosc. 2011, 26, 197–204. [Google Scholar] [CrossRef]
- Van Der Pas, M.H.G.M.; Ankersmit, M.; Stockmann, H.B.; Silvis, R.; Van Grieken, N.C.; Bril, H.; Meijerink, W.J. Laparoscopic Sentinel Lymph Node Identification in Patients with Colon Carcinoma Using a Near-Infrared Dye: Description of a New Technique and Feasibility Study. J. Laparoendosc. Adv. Surg. Tech. 2013, 23, 367–371. [Google Scholar] [CrossRef]
- Liberale, G.; Bohlok, A.; Bormans, A.; Bouazza, F.; Gomez-Galdon, M.; El Nakadi, I.; Bourgeois, P.; Donckier, V. Indocyanine green fluorescence imaging for sentinel lymph node detection in colorectal cancer: A systematic review. Eur. J. Surg. Oncol. (EJSO) 2018, 44, 1301–1306. [Google Scholar] [CrossRef]
- Mirnezami, A.; Mirnezami, R.; Chandrakumaran, K.; Sasapu, K.; Sagar, P.; Finan, P. Increased Local Recurrence and Reduced Survival From Colorectal Cancer Following Anastomotic Leak. Ann. Surg. 2011, 253, 890–899. [Google Scholar] [CrossRef]
- Kawahara, H.; Nimura, H.; Watanabe, K.; Kobayashi, T.; Kashiwagi, H.; Yanaga, K. Where Does the First Lateral Pelvic Lymph Node Receive Drainage from? Dig. Surg. 2007, 24, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Noura, S.; Ohue, M.; Seki, Y.; Tanaka, K.; Motoori, M.; Kishi, K.; Miyashiro, I.; Ohigashi, H.; Yano, M.; Ishikawa, O.; et al. Feasibility of a Lateral Region Sentinel Node Biopsy of Lower Rectal Cancer Guided by Indocyanine Green Using a Near-Infrared Camera System. Ann. Surg. Oncol. 2009, 17, 144–151. [Google Scholar] [CrossRef]
- Handgraaf, H.J.M.; Boogerd, L.S.; Verbeek, F.P.; Tummers, Q.R.; Hardwick, J.C.; Baeten, C.I.; Frangioni, J.V.; Van De Velde, C.J.; Vahrmeijer, A.L. Intraoperative fluorescence imaging to localize tumors and sentinel lymph nodes in rectal cancer. Minim. Invasive Ther. Allied Technol. 2015, 25, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.-C.; Tian, Y.-T.; Wang, X.-W.; Zhao, C.-D.; Ma, S.; Jiang, J.; Li, E.-N.; Zhou, H.-T.; Liu, Q.; Liang, J.-W.; et al. Application of indocyanine green-enhanced near-infrared fluorescence-guided imaging in laparoscopic lateral pelvic lymph node dissection for middle-low rectal cancer. World J. Gastroenterol. 2019, 25, 4502–4511. [Google Scholar] [CrossRef] [PubMed]
- Boni, L.; David, G.; Mangano, A.; Dionigi, G.; Rausei, S.; Spampatti, S.; Cassinotti, E.; Fingerhut, A. Clinical applications of indocyanine green (ICG) enhanced fluorescence in laparoscopic surgery. Surg. Endosc. 2014, 29, 2046–2055. [Google Scholar] [CrossRef] [Green Version]
- Blanco-Colino, R.; Espin-Basany, E. Intraoperative use of ICG fluorescence imaging to reduce the risk of anastomotic leakage in colorectal surgery: A systematic review and meta-analysis. Tech. Coloproctology 2017, 22, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Degett, T.H.; Andersen, H.S.; Gögenur, I. Indocyanine green fluorescence angiography for intraoperative assessment of gastrointestinal anastomotic perfusion: A systematic review of clinical trials. Langenbeck’s Arch. Surg. 2016, 401, 767–775. [Google Scholar] [CrossRef]
- Arezzo, A.; Bonino, M.A.; Ris, F.; Boni, L.; Cassinotti, E.; Foo, D.C.C.; Shum, N.F.; Brolese, A.; Ciarleglio, F.; Keller, D.S.; et al. Intraoperative use of fluorescence with indocyanine green reduces anastomotic leak rates in rectal cancer surgery: An individual participant data analysis. Surg. Endosc. 2020, 1–10. [Google Scholar] [CrossRef]
- Impellizzeri, H.G.; Pulvirenti, A.; Inama, M.; Bacchion, M.; Marrano, E.; Creciun, M.; Casaril, A.; Moretto, G. Near-infrared fluorescence angiography for colorectal surgery is associated with a reduction of anastomotic leak rate. Updat. Surg. 2020, 1–8. [Google Scholar] [CrossRef]
- Böckelman, C.; Engelmann, B.E.; Kaprio, T.; Hansen, T.F.; Glimelius, B. Risk of recurrence in patients with colon cancer stage II and III: A systematic review and meta-analysis of recent literature. Acta Oncol. 2014, 54, 5–16. [Google Scholar] [CrossRef]
- Savlovschi, C.; Serban, D.; Andreescu, C.; Dascalu, A.; Pantu, H. Economic analysis of medical management applied for left colostomy. Chirurgia 2013, 108, 666–669. [Google Scholar]
- Savlovschi, C.; Serban, D.; Trotea, T.; Borcan, R.; Dumitrescu, D. Post-surgery morbidity and mortality in colorectal cancer in elderly subjects. Chirurgia 2013, 108, 177–179. [Google Scholar] [PubMed]
- Şavlovschi, C.; Comandaşu, M.; Serban, D. Specifics of diagnosis and treatment in synchronous colorectal cancers (SCC). Chirurgia 2013, 108, 43–45. [Google Scholar] [PubMed]
- Kiss, L.; Kiss, R.; Porr, P.J.; Nica, C.; Bardac, O.; Tănăsescu, C.; Bărbulescu, B.; Bundache, M.; Ilie, S.; Maniu, D.; et al. Pathological evidence in support of total mesorectal excision in the management of rectal cancer. Chirurgia 2011, 106, 347–352. [Google Scholar] [PubMed]
- Scabini, S. Sentinel node biopsy in colorectal cancer: Must we believe it? World J. Gastrointest. Surg. 2010, 2, 6–8. [Google Scholar] [CrossRef]
- Nowak, K.; Karampinis, I.; Gerken, A.L.H. Application of Fluorescent Dyes in Visceral Surgery: State of the Art and Future Perspectives. Visc. Med. 2020, 36, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Emile, S.H.; Elfeki, H.; Shalaby, M.; Sakr, A.; Sileri, P.; Laurberg, S.; Wexner, S.D. Sensitivity and specificity of indocyanine green near-infrared fluorescence imaging in detection of metastatic lymph nodes in colorectal cancer: Systematic review and meta-analysis. J. Surg. Oncol. 2017, 116, 730–740. [Google Scholar] [CrossRef]
- Liberale, G.; Bourgeois, P.; Larsimont, D.; Moreau, M.; Donckier, V.; Ishizawa, T. Indocyanine green fluorescence-guided surgery after IV injection in metastatic colorectal cancer: A systematic review. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 1656–1667. [Google Scholar] [CrossRef]
- Villegas-Tovar, E.; Jimenez-Lillo, J.; Jimenez-Valerio, V.; Diaz-Giron-Gidi, A.; Faes-Petersen, R.; Otero-Piñeiro, A.; De Lacy, F.B.; Martinez-Portilla, R.J.; Lacy, A.M. Performance of Indocyanine green for sentinel lymph node mapping and lymph node metastasis in colorectal cancer: A diagnostic test accuracy meta-analysis. Surg. Endosc. 2019, 34, 1035–1047. [Google Scholar] [CrossRef]
- Boogerd, L.S.F.; Hoogstins, C.E.S.; Schaap, D.P.; Kusters, M.; Handgraaf, H.J.M.; Van Der Valk, M.J.M.; Hilling, D.E.; Holman, F.A.; Peeters, K.C.; Mieog, J.S.D.; et al. Safety and effectiveness of SGM-101, a fluorescent antibody targeting carcinoembryonic antigen, for intraoperative detection of colorectal cancer: A dose-escalation pilot study. Lancet Gastroenterol. Hepatol. 2018, 3, 181–191. [Google Scholar] [CrossRef]
- Gutowski, M.; Framery, B.; Boonstra, M.C.; Garambois, V.; Quenet, F.; Dumas, K.; Scherninski, F.; Cailler, F.; Vahrmeijer, A.L.; Pelegrin, A. SGM-101: An innovative near-infrared dye-antibody conjugate that targets CEA for fluorescence-guided surgery. Surg. Oncol. 2017, 26, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Hoogstins, C.; Burggraaf, J.J.; Koller, M.; Handgraaf, H.; Boogerd, L.; Van Dam, G.; Vahrmeijer, A.; Burggraaf, J. Setting Standards for Reporting and Quantification in Fluorescence-Guided Surgery. Mol. Imaging Boil. 2018, 21, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Urso, A.; Agnus, V.; Barberio, M.; Seeliger, B.; Marchegiani, F.; Charles, A.-L.; Geny, B.; Marescaux, J.; Mutter, D.; Diana, M. Computer-assisted quantification and visualization of bowel perfusion using fluorescence-based enhanced reality in left-sided colonic resections. Surg. Endosc. 2020, 1–11. [Google Scholar] [CrossRef]
- Lütken, C.D.; Achiam, M.P.; Svendsen, M.B.; Boni, L.; Nerup, N. Optimizing quantitative fluorescence angiography for visceral perfusion assessment. Surg. Endosc. 2020. [Google Scholar] [CrossRef]
- Diana, M. Enabling precision digestive surgery with fluorescence imaging. Transl. Gastroenterol. Hepatol. 2017, 2, 97. [Google Scholar] [CrossRef] [Green Version]
- Barth, C.W.; Gibbs, S.L. Fluorescence Image-Guided Surgery—A Perspective on Contrast Agent Development. Proc. SPIE Int. Soc. Opt. Eng. 2020, 11222, 112220J. [Google Scholar] [CrossRef]


{kind=link}
| Study, Year | No. Cases (NIR; Control) | Pathology | Type of Surgery | Fluorescence Assessment | Dose | Decision Change | AL% (NIR; Control) | Image Acquisition Device |
|---|---|---|---|---|---|---|---|---|
| Ris, F.; et al. [13], 2018 | 504 NIR only | B/M colorectal diseases (all locations) | Laparoscopy/open/conversion colorectal surgery | Intraperitoneal | 7.5 mL before and after | 5.8% | 2.4% (none in those with revised surgery) | PINPOINT, Stryker |
| Ohya, H.; et al. [17], 2020 | n = 400 NIR only | Colon/appendiceal cancer (all locations) | Laparoscopic colectomies | Intraperitoneal | 0.25 mg/kg | 2.8% (mostly transverse and left colon anastomosis) | 1% | IMAGE1 S, Karl Storz PINPOINT, Stryker |
| Kin, C.; et al. [18], 2015 | 346 (173;173 historically matched) | M/B colorectal diseases (all locations) | Laparoscopic colorectal surgery | Intraperitoneal | No info | 5% | 7.5% 6.4% | No info |
| Boni, L.; et al. [25], 2017 | n = 107, NIR only | Colorectal cancer, all locations | Laparoscopic right/left hemicolectomy, AR | Intraperitoneal | 0.2 mg/kg before and after | 3.8% | 0.9% (due to stapler related deficiency) | IMAGE1 S, Karl Storz |
| Su, H.; et al. [29], 2020 | 189 (84;105) | Colon cancer, >30 cm anal verge | Totally laparoscopic colic resection | Intraperitoneal | Before and after 7.5 mg (3 mL) | 4.8% | 0% 0% 0% stricture | opto-cam 2100 (Optomedic, Guangdong, China) |
| Ogino, T.; et al. [32], 2018 | 74, NIR only | B/M colorectal diseases (all locations) | Laparoscopy/open colorectal surgery | Extraperitoneal | 5 mg before | 8.1% | 1.4% (1 case, not related to ischemia) | Photodynamic Eye System, Hamamatsu Photonics |
| Tsang, Y.; et al. [34], 2020 | 131 (63;68) | B/M colorectal diseases (all locations) | Laparoscopic/robotic colorectal surgery | Intraperitoneal | 10 mg before | 1.6% | 3.23% 4.35% | Firefly, da Vinci Xi Olympus OTV-S300 CLV-S200-IR (Olympus, Tokyo, Japan) |
| Nishigori, N.; et al. [35], 2016 | 21 NIR only | Colorectal cancer (all locations) | Laparoscopic colorectal surgery | Intraperitoneal | 1–3 mL (2.5 mg/mL) | 16.7% | 0% | D-Light P System/Image 1 SPIES, Karl Stortz; infrared endoscopic camera system, Olympus (Tokyo, Japan) |
| Santi, C.; et al. [36], 2019 | 38, NIR only | Colorectal cancer, all locations | Laparoscopic colic resection | Intraperitoneal | 5 mL (0,3 mg/kg) before | 2.6% | 2.6% (mechanical cause) | IMAGE1S, Karl Storz |
| Sherwinter, D.A.; et al. [19], 2012 | n = 20 NIR only | B/M Rectal diseases | Laparoscopic LAR | Endoscopy, transanal | 1 mL 2.5 mg | N/A 4 cases with hipofluoresce—decision not changed | 10% (managed conservatory)—CT diagnosed | PINPOINT, Novadaq (Canada) |
| Kawada, K.; et al. [20], 2016 | n = 68 NIR only | Left colorectal cancer | Laparoscopic colorectal surgery | Specimen extracted by the umbilical trocar and examined | 5 mg | 26.5% | 4.5% (symptomatic) | PDE-neo system, Hamamatsu Photonics |
| Somerskhar, J.P.; et al. [21], 2020 | n = 50 NIR only | Colorectal cancer | Robotic Sigmoid colectomy, LAR +ileostomy | Intraperitoneal | 3 mL, 2.5 mg/mL | 88% | 0% | FIREFLY, da Vinci |
| Jafari, M.D.; et al. [22], 2013 | n = 38 (16;22) | Rectal cancer | Robotic-assisted AR | Intraperitoneal | 6–8 mg before | 18.75% | 6% 18% | FIREFLY, da Vinci |
| Grone, J.; et al. [23], 2015 | n = 18, ICG only | Rectal cancer | Laparoscopic AR (1 conversion) | Intraperitoneal | 10 mg before and after | 27.8% | 6% (compared to 15% historically, same center) | PINPOINT, Novadaq |
| Hellan, M.; et al. [24], 2014 | n = 40, ICG only | Left colorectal cancer | Robotic-assisted left colorectal surgery | Intraperitoneal | 10 mg ICG | 40% | 5% (with revised anastomosis) | FIREFLY, da Vinci |
| Jafari, M.D.; et al. [26], 2014 | n = 139, NIR only | Left colorectal cancer | Laparoscopy-assisted left colectomy, AR | Intraperitoneal | 3.75-7.5 mg before and after | 8% | 1.4% (no AL in cases with changed decision) | PINPOINT, Novadaq |
| De Nardi, P.; et al. [27], 2020 | n = 240 (118;122) | Left colorectal B/M diseases | Laparoscopic AR, LAR, left colectomy | Intraperitoneal | 0.3 mg/kg before and after | 11% | 5% 9% | IMAGE1 S, Karl Storz |
| Kim, J.C.; et al. [28]. 2016 | 426 (123; 313) | Rectal cancer | Robotic-assisted sphincter-saving operations | Intraperitoneal | 10 mg (before+/- after) | Not applicable (site chosen by NIR) | 0.8% 5.4% | FIREFLY, da Vinci |
| Mizrahi, I.; et al. [30], 2018 | 60 (30;30) | Low rectal cancer, <5 cm anal verge | Laparoscopic LAR | Intraperitoneal | 0.1–0.3 mg/kg | 13.3% | 0% 6.7% | PINPOINT, Novadaq |
| Son, G.M.; et al. [31], 2019 | 86, NIR only | Colorectal cancer | Laparoscopic AR (55) Laparoscopic LAR (31) | Intraperitoneal | 0.25 mg/kg before | Not applicable | 7% good correlation with poor perfusion (TR >0.6) | IMAGE1 S, Karl Storz |
| Hasegawa, S.; et al. [33], 2020 | 852 (143;709) | Rectal cancer | Laparoscopic LAR, ISR | Intraperitoneal | 5 mg before | 17.0% | 2.8% 12.4% | IMAGE1 S, Karl Storz; 1588 AIM and SPY (Stryker), HyperEye (Mizuho Medical) |
| Watanabe, J.; et al. [37], 2020 | 550 (236;314) | Low rectal cancer | Laparoscopic LAR | Intraperitoneal | 0.25mg/kg | 5.7% | 4.7% 10.4% | D-Light P, Karl Storz; 1588 AIM Platform, Stryker |
| Wada, T.; et al. [38], 2019 | 149 (48;101) | Low rectal cancer | Laparoscopic LAR | Specimen exteriorized by the umbilical trocar and examined | 5 mg before | 27.1% | 8.8% 14.7% | PDE-neo system, Hamamatsu Photonics |
| Study, Year | Disease, Stage | No. Cases | ICG Administration | Dose | Fluorescence Evaluation | Detection Rate | Sensitivity (Metastasis in SL/Total Lymph Node Metastasis) |
|---|---|---|---|---|---|---|---|
| Carrara, A.; et al. [40], 2020 | Colon cancer stage I-II, High risk colic polyposis | 95 | Laparoscopic/extraperitoneally | 5 mL (5 mg/mL), sup + inf | Spies-Cam, Karl Storz; Firefly, da Vinci; PDE, Hamamatsu-Photonics | 96.8% | 85.9% |
| Hirsche, C.; et al. [41], 2012 | Colon cancer, T1-3 N0 | 26 | Laparoscopic | 1–4 mL (5mg/mL) sup + inf | IC-View, Pulsion Medical Systems | 96% | 82% |
| Curie, A.; et al. [42], 2017 | Colon cancer T1-2, N0 | 30 | Endoscopic | 1mL in 4 quadrants (5 mg/mL) | NIR Imaging System, Olympus | 90% | 33% |
| Liberale, G.; et al. [43], 2015 | Colon cancer, Tis-T4, N0-2 | 2 | Intraoperatively detected after 15 min + ex vivo | 0.25 mg/kc, i.v. | PDE, Hamamatsu Photonics | N/A | N/A |
| Liberale, G.; et al. [44], 2016 | Colon cancer, Tis-T4, N0-2 | 20 | Ex vivo | 0.5 mL in four sectors (0.5 mg/mL) | PDE, Hamamatsu Photonics | 95% | 43% |
| Watanabe, J.; et al. [45], 2016 | Splenic flexure cancer stage I–II | 31 | Laparoscopic | 1 mL (2.5 mg/mL) in two points | D-Light P, Karl Storz | 100% | 66% |
| Andersen, H.S.; et al. [46], 2017 | Colic cancer T1-3, all cancers suited for laparoscopic surgery | 29 | Endoscopic | 0.5 mL (25 mg ICG + 9 mL sterile water + 1 mL 20% human albumin) inf + sup | SPIES ICG camera with ICG Xenon 300 light source from Karl Storz | 65.5% | 20% |
| Nagata, K.; et al. [47], 2006 | Colon/colorectal junction cancer T1-3, N0-2, all cancers suited for laparoscopic surgery | 48 | Subserosal | 5 mL (5 mg/mL) | Laparoscope, Olympus | 98% | 53.6% |
| Kusano, M.; et al. [48], 2008 | Colorectal cancer | 26 | Submucosal | 2 mL (5 mg/mL) | PDE, Hamamatsu Photonics | 88.5% | 33.3% |
| Cahill, R.A.; et al. [49], 2012 | Colon cancer stages I–III | 18 | Submucosal | 2–3 mL | Laparoscope, Olympus | 94% | 100% |
| Van der Pass, M.H.G.M.; et al. [50], 2013 | Colon cancer stages I–III | 14 | Subserosal | 1 mL (2.5 mg/mL, containing 2% human serum albumin) | Laparoscope, Olympus | 100% | 0% |
| Nishigor, N.; et al. [35], 2016 | Colorectal cancer T1-4 N0-2bM0 | 21 | Submucosal/subserously | 0.2–0.3 mL (2.5 mg/mL) | D-Light P System/Image 1 SPIES, Karl Stortz; laparoscope, Olympus | 69.7% | 45% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alius, C.; Tudor, C.; Badiu, C.D.; Dascalu, A.M.; Smarandache, C.G.; Sabau, A.D.; Tanasescu, C.; Balasescu, S.A.; Serban, D. Indocyanine Green-Enhanced Colorectal Surgery—between Being Superfluous and Being a Game-Changer. Diagnostics 2020, 10, 742. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100742
Alius C, Tudor C, Badiu CD, Dascalu AM, Smarandache CG, Sabau AD, Tanasescu C, Balasescu SA, Serban D. Indocyanine Green-Enhanced Colorectal Surgery—between Being Superfluous and Being a Game-Changer. Diagnostics. 2020; 10(10):742. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100742
Chicago/Turabian StyleAlius, Catalin, Corneliu Tudor, Cristinel Dumitru Badiu, Ana Maria Dascalu, Catalin Gabriel Smarandache, Alexandru Dan Sabau, Ciprian Tanasescu, Simona Andreea Balasescu, and Dragos Serban. 2020. "Indocyanine Green-Enhanced Colorectal Surgery—between Being Superfluous and Being a Game-Changer" Diagnostics 10, no. 10: 742. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100742