Spatial Configuration of Abdominal Aortic Aneurysm Analysis as a Useful Tool for the Estimation of Stent-Graft Migration

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Limitations to the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ryzhakov, P.B.; Soudah, E.; Dialami, N. Computational modeling of the fluid flow and the flexible intimal flap in type B aortic dissection via a monolithic arbitrary Lagrangian/Eulerian fluid-structure interaction model. Int. J. Numer. Methods Biomed. Eng. 2019, 35, e3239. [Google Scholar] [CrossRef] [PubMed]
- Miyake, T.; Morishita, R. Pharmacological treatment of abdominal aortic aneurysm. Cardiovasc. Res. 2009, 83, 436–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindeman, J.H.; Matsumura, J.S. Pharmacologic Management of Aneurysms. Circ. Res. 2019, 124, 631–646. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.O.; Arana, V.T.; Rubbert, C.; Cornelius, J.F.; Fischer, I.; Bostelmann, R.; Mijderwijk, H.-J.; Turowski, B.; Steiger, H.-J.; May, R.; et al. Association between aneurysm hemodynamics and wall enhancement on 3D vessel wall MRI. J. Neurosurg. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Coselli, J.S.; Green, S.Y. A brief history of aortic surgery: Insight into distal aortic repair. J. Thorac. Cardiovasc. Surg. 2013, 145 (Suppl. 3), S123–S125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demanget, N.; Avril, S.; Badel, P.; Orgéas, L.; Geindreau, C.; Albertini, J.-N.; Favre, J.-P. Computational comparison of the bending behavior of aortic stent-grafts. J. Mech. Behav. Biomed. Mater. 2012, 5, 272–282. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, A.; Podgórski, M.; Wozniak, T.; Stefanczyk, L.; Strzelecki, M. Computational Fluid Dynamics as an Engineering Tool for the Reconstruction of Hemodynamics after Carotid Artery Stenosis Operation: A Case Study. Medicina 2018, 54, 42. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, A.; Podgorski, M.; Polanczyk, M.; Veshkina, N.; Zbicinski, I.; Stefanczyk, L.; Neumayer, C. A novel method for describing biomechanical properties of the aortic wall based on the three-dimensional fluid-structure interaction model. Interact. Cardiovasc. Thorac. Surg. 2018, 28, 306–315. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Smith, N.P. The Multi-Scale Modelling of Coronary Blood Flow. Ann. Biomed. Eng. 2012, 40, 2399–2413. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Gao, B.; Gu, K.; Chang, Y.; Xu, J. The Study on Hemodynamic Effect of Varied Support Models of BJUT-II VAD on Coronary Artery. ASAIO J. 2014, 60, 643–651. [Google Scholar] [CrossRef]
- Polanczyk, A.; Podyma, M.; Stefańczyk, L.; Szubert, W.; Zbicinski, I. A 3D model of thrombus formation in a stent-graft after implantation in the abdominal aorta. J. Biomech. 2015, 48, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Tyfa, Z.; Obidowski, D.; Jóźwik, K. Numerical Analysis of the VAD Outflow Cannula Positioning on the Blood Flow in the Patient–Specific Brain Supplying Arteries. Mech. Mech. Eng. 2020, 22, 619–636. [Google Scholar] [CrossRef]
- Polanczyk, A.; Podgórski, M.; Polańczyk, M.; Piechota-Polanczyk, A.; Stefanczyk, L.; Strzelecki, M. A novel vision-based system for quantitative analysis of abdominal aortic aneurysm deformation. Biomed. Eng. Online 2019, 18, 56. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, A.; Wozniak, T.; Strzelecki, M.; Szubert, W.; Stefanczyk, L. Evaluating an algorithm for 3D reconstruction of blood vessels for further simulations of hemodynamic in human artery branches. In Proceedings of the 2016 Signal Processing: Algorithms, Architectures, Arrangements, and Applications (SPA), Poznan, Poland, 21–23 September 2016; pp. 103–107. [Google Scholar] [CrossRef]
- Kociołek, M.; Strzelecki, M.; Klepaczko, A. Functional Kidney Analysis Based on Textured DCE-MRI Images. Adv. Intell. Syst. Comput. 2019, 1011, 38–49. [Google Scholar] [CrossRef]
- Auer, M.; Gasser, T. Reconstruction and Finite Element Mesh Generation of Abdominal Aortic Aneurysms From Computerized Tomography Angiography Data With Minimal User Interactions. IEEE Trans. Med. Imaging 2010, 29, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Fung, G.S.; Lam, S.; Cheng, S.; Chow, K.-W. On stent-graft models in thoracic aortic endovascular repair: A computational investigation of the hemodynamic factors. Comput. Biol. Med. 2008, 38, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Xenos, M.; Rambhia, S.H.; Alemu, Y.; Einav, S.; Labropoulos, N.; Tassiopoulos, A.; Ricotta, J.J.; Bluestein, D. Patient-Based Abdominal Aortic Aneurysm Rupture Risk Prediction with Fluid Structure Interaction Modeling. Ann. Biomed. Eng. 2010, 38, 3323–3337. [Google Scholar] [CrossRef] [PubMed]
- Gundert, T.J.; Marsden, A.L.; Yang, W.; Ladisa, J.F. Optimization of Cardiovascular Stent Design Using Computational Fluid Dynamics. J. Biomech. Eng. 2012, 134, 011002. [Google Scholar] [CrossRef]
- Gijsen, F.J.H.; Van De Vosse, F.; Janssen, J.; Van De Vosse, F.N. The influence of the non-Newtonian properties of blood on the flow in large arteries: Steady flow in a carotid bifurcation model. J. Biomech. 1999, 32, 601–608. [Google Scholar] [CrossRef]
- Hoi, Y.; Meng, H.; Woodward, S.H.; Bendok, B.R.; Hanel, R.A.; Guterman, L.R.; Hopkins, L.N. Effects of arterial geometry on aneurysm growth: Three-dimensional computational fluid dynamics study. J. Neurosurg. 2004, 101, 676–681. [Google Scholar] [CrossRef]
- Chrzanowski, L.; Drozdz, J.; Strzelecki, M.; Kasprzak, J.D. Application of Neural Networks for the Analysis of Intravascular Ultrasound and Histological Aortic Wall Appearance-An In Vitro Tissue Characterization Study. Ultrasound Med. Biol. 2008, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Waite, L.F.; Fine, J. Applied Biofluid Mechanics, 1st ed.; McGraw-Hill Professional: New York, NY, USA, 2007. [Google Scholar]
- Stefanczyk, L.; Grzelak, P.; Podyma, M.; Zbicinski, I. Hemodynamic parameters within aortal stent-grafts vs. Their spatial configuration—A comparison based on computer simulations. Pol. J. Radiol. 2008, 73, 22–26. [Google Scholar]
- Jayendiran, R.; Nour, B.; Ruimi, A. Dacron graft as replacement to dissected aorta: A three-dimensional fluid-structure-interaction analysis. J. Mech. Behav. Biomed. Mater. 2018, 78, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.M.; Murphy, E.; Boyle, F.J. Computational fluid dynamics analysis of balloon-expandable coronary stents: Influence of stent and vessel deformation. Med. Eng. Phys. 2014, 36, 1047–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polanczyk, A.; Piechota-Polanczyk, A.; Stefanczyk, L.; Strzelecki, M. Shape and Enhancement Analysis as a Useful Tool for the Presentation of Blood Hemodynamic Properties in the Area of Aortic Dissection. J. Clin. Med. 2020, 9, 1330. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, A.; Strzelecki, M.; Wozniak, T.; Szubert, W.; Stefanczyk, L. 3D Blood Vessels Reconstruction Based on Segmented CT Data for Further Simulations of Hemodynamic in Human Artery Branches. Found. Comput. Decis. Sci. 2017, 42, 359–371. [Google Scholar] [CrossRef] [Green Version]
- Assi, A.A.N.; Abu Arra, A. Optimization of image quality in pulmonary CT angiography with low dose of contrast material. Pol. J. Med Phys. Eng. 2017, 23, 43–46. [Google Scholar] [CrossRef]
- König, M.; Bültmann, E.; Bode-Schnurbus, L.; Koenen, D.; Mielke, E.; Heuser, L. Image quality in CT perfusion imaging of the brain. Eur. Radiol. 2006, 17, 39–47. [Google Scholar] [CrossRef]
- Polanczyk, A.; Podyma, M.; Trebinski, L.; Chrzastek, J.; Zbicinski, I.; Stefańczyk, L. A Novel Attempt to Standardize Results of CFD Simulations Basing on Spatial Configuration of Aortic Stent-Grafts. PLoS ONE 2016, 11, e0153332. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, A.; Piechota-Polanczyk, A.; Stefańczyk, L. A new approach for the pre-clinical optimization of a spatial configuration of bifurcated endovascular prosthesis placed in abdominal aortic aneurysms. PLoS ONE 2017, 12, e0182717. [Google Scholar] [CrossRef]
- Polanczyk, A.; Podyma, M.; Stefańczyk, L.; Zbicinski, I. Effects of stent-graft geometry and blood hematocrit on hemodynamic in Abdominal Aortic Aneurysm. Chem. Process. Eng. 2012, 33, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, A.; Podgorski, M.; Polanczyk, M.; Piechota-Polanczyk, A.; Neumayer, C.; Stefanczyk, L. A Novel Patient-Specific Human Cardiovascular System Phantom (HCSP) for Reconstructions of Pulsatile Blood Hemodynamic Inside Abdominal Aortic Aneurysm. IEEE Access 2018, 6, 61896–61903. [Google Scholar] [CrossRef]
- Johnston, B.; Johnston, P.; Corney, S.; Kilpatrick, D. Non-Newtonian blood flow in human right coronary arteries: Transient simulations. J. Biomech. 2006, 39, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, A.; Piechota-Polanczyk, A.; Neumayer, C.; Huk, I. CFD Reconstruction of Blood Hemodynamic Based on a Self-made Algorithm in Patients with Acute Type IIIb Aortic Dissection Treated with TEVAR Procedure. In IUTAM Symposium on Recent Advances in Moving Boundary Problems in Mechanics; IUTAM Bookseries(34); Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Polanczyk, A.; Piechota-Polanczyk, A.; Domenig, C.; Nanobachvili, J.; Huk, I.; Neumayer, C. Computational Fluid Dynamic Accuracy in Mimicking Changes in Blood Hemodynamics in Patients with Acute Type IIIb Aortic Dissection Treated with TEVAR. Appl. Sci. 2018, 8, 1309. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, A.; Klinger, M.; Nanobachvili, J.; Huk, I.; Neumayer, C. Artificial Circulatory Model for Analysis of Human and Artificial Vessels. Appl. Sci. 2018, 8, 1017. [Google Scholar] [CrossRef] [Green Version]
- Szmidt, J.; Gałązka, Z.; Rowinski, O.; Nazarewski, S.; Jakimowicz, T.; Pietrasik, K.; Grygiel, K.; Chudzinski, W. Late aneurysm rupture after endovascular abdominal aneurysm repair. Interact. Cardiovasc. Thorac. Surg. 2007, 6, 490–494. [Google Scholar] [CrossRef] [Green Version]
- Pintoux, D.; Chaillou, P.; Azéma, L.; Bizouarn, P.; Costargent, A.; Patra, P.; Gouëffic, Y. Long-Term Influence of Suprarenal or Infrarenal Fixation on Proximal Neck Dilatation and Stentgraft Migration After EVAR. Ann. Vasc. Surg. 2011, 25, 1012–1019. [Google Scholar] [CrossRef]
- Avgerinos, E.D.; Dalainas, I.; Kakisis, J.; Moulakakis, K.; Giannakopoulos, T.; Liapis, C. Endograft Accommodation on the Aortic Bifurcation: An Overview of Anatomical Fixation and Implications for Long-term Stent-Graft Stability. J. Endovasc. Ther. 2011, 18, 462–470. [Google Scholar] [CrossRef]
- Raben, J.S.; Morlacchi, S.; Burzotta, F.; Migliavacca, F.; Vlachos, P.P. Local blood flow patterns in stented coronary bifurcations: An experimental and numerical study. J. Appl. Biomater. Funct. Mater. 2014, 13. [Google Scholar] [CrossRef]
- Yu, C.H.; Kwon, T.-K. Study of parameters for evaluating flow reduction with stents in a sidewall aneurysm phantom model. Bio-Medical Mater. Eng. 2014, 24, 2417–2424. [Google Scholar] [CrossRef] [Green Version]
- Litwinski, R.A.; Donayre, C.E.; Chow, S.L.; Song, T.K.; Kopchok, G.; Walot, I.; White, R.A. The role of aortic neck dilation and elongation in the etiology of stent graft migration after endovascular abdominal aortic aneurysm repair with a passive fixation device. J. Vasc. Surg. 2006, 44, 1176–1181. [Google Scholar] [CrossRef] [Green Version]
- Domanin, M.; Piazzoli, G.; Trimarchi, S.; Vergara, C. Image-Based Displacements Analysis and Computational Blood Dynamics after Endovascular Aneurysm Repair. Ann. Vasc. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rigatelli, G.; Zuin, M.; Dell’Avvocata, F.; Vassilev, D.; Daggubati, R.; Nguyen, T.; Thang, N.V.V.; Foin, N. Evaluation of coronary flow conditions in complex coronary artery bifurcations stenting using computational fluid dynamics: Impact of final proximal optimization technique on different double-stent techniques. Cardiovasc. Revascularization Med. 2017, 18, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Lamooki, S.R.; Tutino, V.M.; Paliwal, N.; Damiano, R.J.; Waqas, M.; Nagesh, S.S.; Rajabzadeh-Oghaz, H.; Vakharia, K.; Siddiqui, A.H.; Meng, H. Evaluation of Two Fast Virtual Stenting Algorithms for Intracranial Aneurysm Flow Diversion. Curr. Neurovascular Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Moulakakis, K.G.; Kakisis, J.; Gonidaki, E.; Lazaris, A.M.; Tsangaris, S.; Geroulakos, G.; Manopoulos, C. Comparison of Fluid Dynamics Variations Between Chimney and Fenestrated Endografts for Pararenal Aneurysms Repair: A Patient Specific Computational Study as Motivation for Clinical Decision-Making. Vasc. Endovasc. Surg. 2019, 53, 572–582. [Google Scholar] [CrossRef]
- Harrison, G.J.; How, T.V.; Poole, R.J.; Brennan, J.A.; Naik, J.B.; Vallabhaneni, S.R.; Fisher, R.K. Closure technique after carotid endarterectomy influences local hemodynamics. J. Vasc. Surg. 2014, 60, 418–427. [Google Scholar] [CrossRef] [Green Version]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
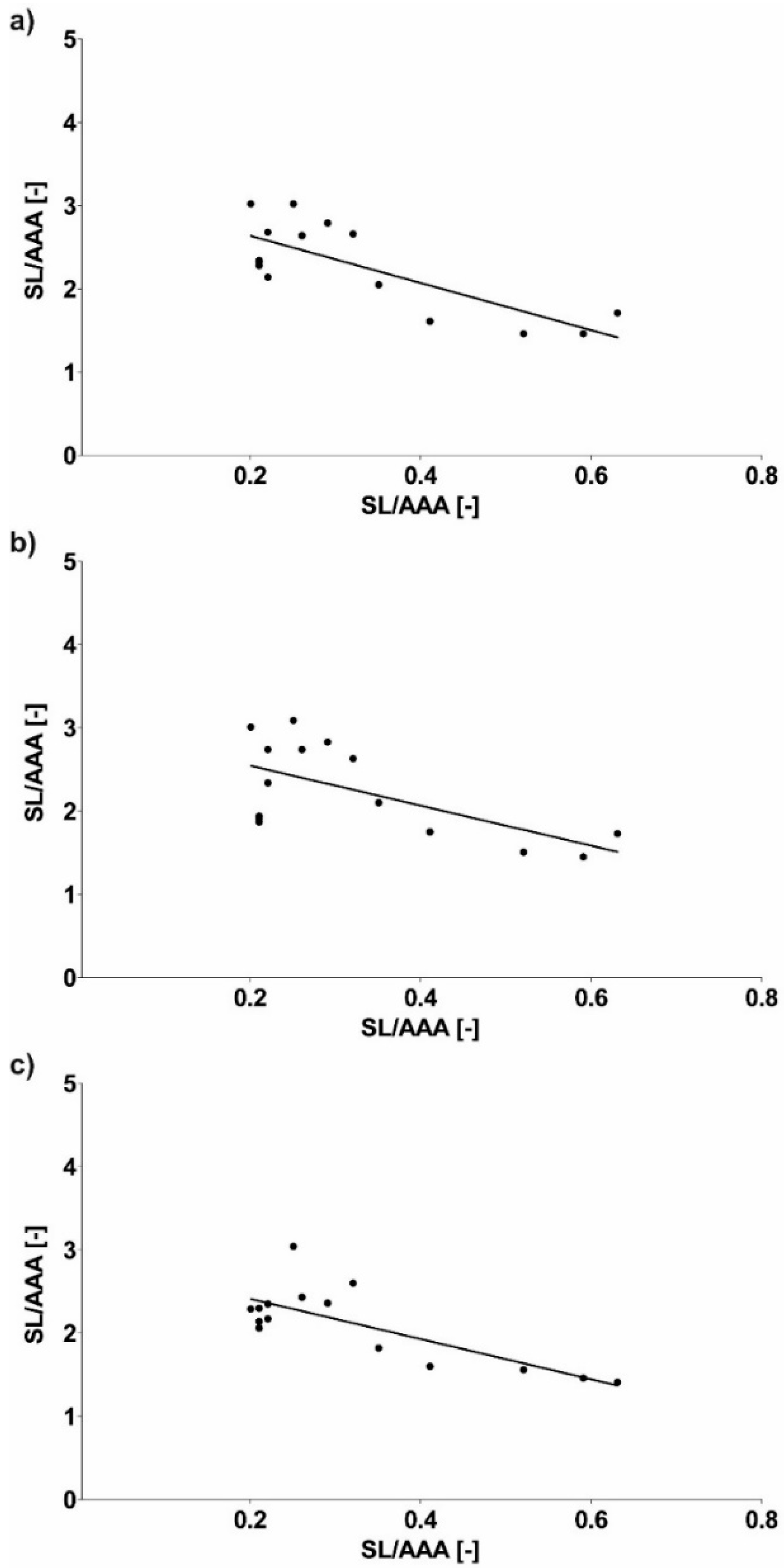
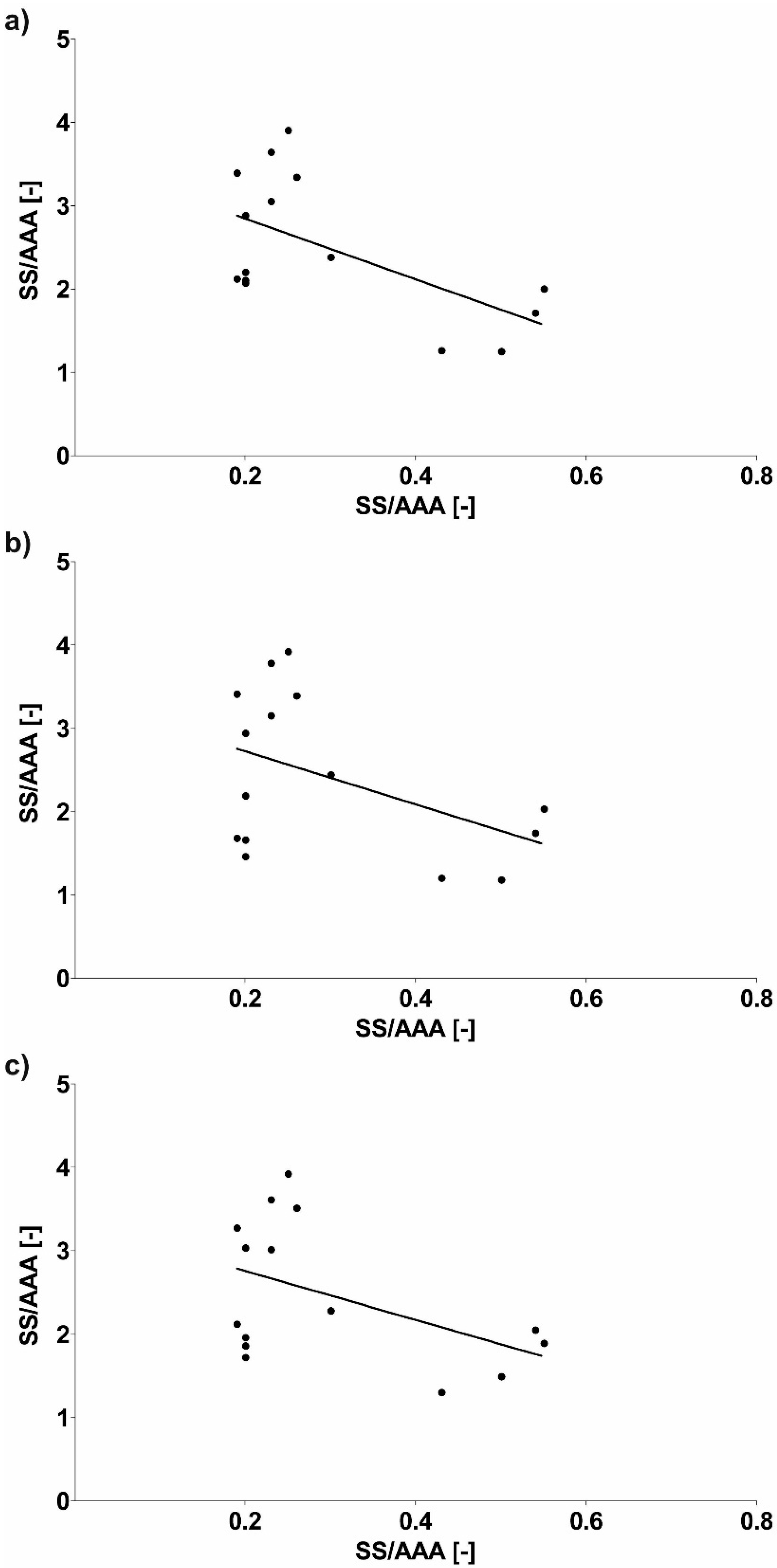
| Type of Stent-Graft | Slope | Y-Intercept |
|---|---|---|
| SL—long stent-graft | −2.835 ± 0.6418 | 3.203 ± 0.2279 |
| −2.405 ± 0.8226 | 3.027 ± 0.2921 | |
| −2.416 ± 0.5628 | 2.894 ± 0.1999 | |
| SS—short stent-graft | −3.643 ± 1.388 | 3.572 ± 0.4514 |
| −3.184 ± 1.735 | 3.360 ± 0.5643 | |
| −2.918 ± 1.529 | 3.338 ± 0.4974 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polanczyk, A.; Piechota-Polanczyk, A.; Stefańczyk, L.; Strzelecki, M. Spatial Configuration of Abdominal Aortic Aneurysm Analysis as a Useful Tool for the Estimation of Stent-Graft Migration. Diagnostics 2020, 10, 737. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100737
Polanczyk A, Piechota-Polanczyk A, Stefańczyk L, Strzelecki M. Spatial Configuration of Abdominal Aortic Aneurysm Analysis as a Useful Tool for the Estimation of Stent-Graft Migration. Diagnostics. 2020; 10(10):737. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100737
Chicago/Turabian StylePolanczyk, Andrzej, Aleksandra Piechota-Polanczyk, Ludomir Stefańczyk, and Michał Strzelecki. 2020. "Spatial Configuration of Abdominal Aortic Aneurysm Analysis as a Useful Tool for the Estimation of Stent-Graft Migration" Diagnostics 10, no. 10: 737. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100737